
Abstract
Adverse childhood experiences (ACEs) are a global public health problem, including in low- and middle-income country settings, and are associated with increased risk of intimate partner violence (IPV) during young adulthood. However, current measurement of ACEs may underestimate sequelae of different combinations, or classes, of ACEs and mask class-specific associations with adult exposure to IPV. We used data among ever-partnered young women and men aged 18–24 years from the Cambodia Violence Against Children Survey (Nw = 369; Nm = 298). Participants retrospectively reported on seven ACEs and lifetime physical and/or sexual IPV victimization and perpetration. Latent classes comprised of ACEs were used as predictors of physical and/or sexual IPV perpetration and victimization, controlling for household wealth. Identified latent classes for women were “Low ACEs” (60%), “Community Violence and Physical Abuse” (23%), and “Physical, Sexual and Emotional Abuse” (17%). Latent classes for men were “Low ACEs” (48%) and “Household and Community Violence” (52%). Among women, those in the Physical, Sexual and Emotional Abuse class were more likely to experience and perpetrate physical and/or sexual IPV in their romantic relationships compared to the reference group (Low ACEs). Women in the Community Violence and Physical Abuse class were more likely to perpetrate physical and/or sexual IPV, but not experience IPV, compared to women in the Low ACEs class. Among men, those in the Household and Community Violence class were more likely to perpetrate physical and/or sexual IPV against a partner, compared to men in the Low ACEs class. Overall, patterns of ACEs were differently associated with IPV outcomes among young women and men in Cambodia. National violence prevention efforts might consider how different combinations of childhood experiences shape risk of young adulthood IPV and tailor interventions accordingly to work with youth disproportionately affected by varied combinations of ACEs.
Keywords
Adverse childhood experiences (ACEs) are a global public health problem and contribute to the global burden of disease and disability (Hughes et al., 2017). ACEs refer to potentially traumatic events occurring before age 18 years, such as experiencing violence, abuse or neglect, witnessing violence in the home or community, or other aspects of the child’s environment that undermines their sense of safety and stability (Centers for Disease Control and Prevention, 2019). Experiences of violence during childhood can include emotional, physical, and sexual violence. In the Asia region, 68% of children aged 2–14 years experienced emotional, physical, or sexual abuse in the past year (Hillis et al., 2016). Across the Asia region, children who experience violence are at higher risk of adverse health and behavioral outcomes in adolescence and adulthood (Fang et al., 2015; Fry et al., 2012), including intimate partner violence (IPV) victimization and perpetration (Fulu et al., 2013b, 2013a, 2017). Further, children who experience cumulative ACEs or poly-victimization—in other words, exposure to more than one form of violence or adversity—face higher risk of IPV in adulthood (Chiang et al., 2018). However, current measurement of ACEs may underestimate sequalae of different combinations of ACEs and mask how ACEs are associated with adult exposure to IPV (Clarke et al., 2016; Lanier et al., 2018). Dichotomous or summative measurement of ACEs may conceal patterns of overlap between individual types of experiences (Clarke et al., 2016; Lanier et al., 2018). Various unique or combined experiences of adversity may differentially contribute to IPV risk (Nikulina et al., 2021). To advance research on the measurement and consequences of ACEs, we applied latent class analysis to evaluate whether classes of ACEs are differentially associated with risk of IPV victimization and perpetration among young women and men in Cambodia.
Background
Adverse Childhood Experiences and Intimate Partner Violence in Cambodia
In Cambodia, as elsewhere, children face risk of ACEs during the course of childhood and adolescence. Commonly measured forms of ACEs in Cambodia include experiences of violence (e.g., emotional, physical, or sexual abuse), violent household dysfunction (e.g., witnessing parental IPV), and community violence (e.g., violence by teachers or peers). Nationally-representative survey data show that over half of Cambodian young women and men aged 18–24 years experienced at least one incident of physical abuse in childhood, with the majority of victims (82% females, 86% males) experiencing more than one incident of childhood physical abuse (Ministry of Women’s Affairs, 2014). In Cambodia, young women and girls face greater risk of experiencing sexual violence compared to young men and boys (Stark et al., 2019). Other forms of ACEs are also commonly experienced. For example, among a representative sample of men aged 18–49 years in Cambodia, 71% experienced emotional abuse during childhood, and nearly one in five (19%) witnessed the physical abuse of their mothers by a father or step-father (Fulu, Jewkes, et al., 2013). In qualitative interviews, Cambodian youth described experiences of peer-to-peer bullying and fighting in schools, as well as perpetration of physical violence by teachers as a form of discipline (Ministry of Women’s Affairs, 2014).
Intimate partner violence is also a global public health issue, and IPV incidence is generally highest during early adulthood (Garcia-Moreno et al., 2005). It is well-documented that exposure to ACEs are associated with increased risk of IPV (Fulu et al., 2013, 2017; Thulin et al., 2021). Several theoretical and empirical explanations elucidate the relationship between ACEs and IPV. For example, social learning theory posits that youth exposed to IPV between parents may learn and internalize these relationships dynamics, and replicate them in later adult intimate partnerships (Bandura, 1979; Yount et al., 2016). Further, underlying inequitable gender norms around men’s control in the household may contribute to co-occurring ACEs, such as violence against children and IPV, which may normalize violence within the household and contribute to intergenerational transmission of multiple forms of violence (Miedema & Kyaw, 2022; Namy et al., 2017). Exposure to ACEs during critical child development periods can also lead to stress response dysregulation, which in turn contributes to heightened reactivity to stressors later in life, and may increase risk of IPV (Hammett et al., 2020; Roberts et al., 2011). Multiple factors may also mediate the relationship between ACEs and IPV. ACEs are associated with a host of risk factors for IPV, including substance misuse, mental health problems, and aggressive or delinquent behaviors (Hughes et al., 2017).
In Cambodia, IPV is widely prevalent, and, as elsewhere, ACEs are associated with experiences and perpetration of IPV during adulthood (Fulu et al., 2013; Jewkes et al., 2017; Yount & Carrera, 2006). A nationally-representative study found that one in three adult men ever perpetrated physical and/or sexual violence against an intimate female partner (Fulu et al., 2013). Among ever-partnered women, 16% ever experienced physical IPV (Jewkes et al., 2017). Studies from Cambodia demonstrate the predictive role of childhood adversity for violence perpetration and victimization in adulthood. Women who experienced physical, sexual, or emotional abuse during childhood were more likely to experience past-year physical and sexual violence by an intimate partner in adulthood, compared to women who did not experience child abuse and neglect (Jewkes et al., 2017). Among men, child abuse and neglect was associated with an increased risk of perpetrating physical, sexual, or emotional abuse against a female intimate partner (Fulu et al., 2013). Additionally, for both Cambodian women and men, retrospective reports of witnessing physical abuse of their mother by a father or step-father were associated with increased risk of adulthood IPV victimization and perpetration, respectively (Fulu et al., 2013; Yount & Carrera, 2006).
Social factors, such as inequitable gendered norms and practices, may contribute to different development trajectories through adolescence for boys and girls, which in turn may condition risk for different types of adversity during childhood, and have implications for adulthood sequelae. For example, in Cambodia, while young men face increased risk of sexual violence as they age, women’s risk of sexual violence is not age-dependent but rather constant across childhood and adolescence (Stark et al., 2019). This sex-differentiated exposure to childhood violence may be influenced by gendered social scripts. In Cambodia, gendered codes of conduct (chbab proh, for men and chbap srey, for women) inform normative expectations for women and men’s behaviors (Jacobsen, 2012). These codes of conduct have the potential to legitimize gender inequitable norms and expectations related to family dynamics, intimate partnerships, sexuality, and violence (Fulu & Miedema, 2015; Jacobsen, 2012). The traditional code of conduct for women exhorts women to obey their husbands and silently accept any abusive behavior from their husband in order to avoid shaming the family. Conversely, norms around masculinity in Cambodia condone men’s use of aggression when used as a form of social control of women and children (Jacobsen, 2012). The normalization of men’s use of violence in the family reinforces gender hierarchies of power in the family and socializes children into a family structure in which women, alongside children, are subordinate and devalued relative to adult men (Namy et al., 2017). Gendered ideologies of male sexual entitlement further contribute to perpetration of sexual assault and rape against women and children in Cambodia (Fulu et al., 2013; Jacobsen, 2012). Socialization into prevailing gender norms throughout adolescence may contribute to divergent patterns of poly-victimization among boys and girls, and in turn, shape their risk of adversity in adulthood (Barra et al., 2018). However, to date, little evidence exists on sex-differentiated combinations of ACEs and consequences for adult exposure to IPV in Cambodia.
Polyvictimization and Measurement of Adverse Childhood Experiences
Children who are exposed to ACEs are more likely to experience multiple forms of abuse or neglect (Finkelhor et al., 2007; Wolfe, 2018). Multiple ACEs often cluster in context-specific patterns, for example based on type of ACE, risk-level, perpetrator type, or setting (Barboza, 2018; Barra et al., 2018; Clarke et al., 2016; Lanier et al., 2018). However, common ACE measurement approaches, such as cumulative risk scores, may fail to capture context-specific clusters of ACEs and underestimate sequelae of different combinations of ACEs (Barboza, 2018; Clarke et al., 2016; Lanier et al., 2018). To address this limitation, person-centered methods, such as latent class analysis, have been more widely applied in the health sciences to map co-occurrence of different combinations of ACEs (classes) and understand links between ACEs classes and risk of adverse adolescent and health outcomes. Studies indicate different patterning of ACEs across contexts. For example, in Uganda, Clarke et al. (2016) identified three classes of violence among school children characterized by (1) emotional and physical violence by parents, and sexual and emotional violence by non-household members; (2) physical, emotional, and sexual violence by peers but low exposure to violence in the household; and (3) physical violence by teachers and school staff but low probability of all other forms of violence. Among university students in East Asia, researchers identified three classes of ACEs: (1) household violence exposure, (2) household dysfunction, and (3) low exposure to any ACEs (Ho et al., 2020). In the United States, four latent classes of ACEs were identified among a nationally representative sample of youth: (1) child maltreatment; (2) household dysfunction; (3) community violence; and (4) low adversity (Lee et al., 2020). Studies using latent class analytic approaches in high-income countries (HICs) find ACEs class-specific associations with poor child health (Lanier et al., 2018), perpetration of youth violence (Barra et al., 2018; Davis et al., 2019), adult mental disorders (Barboza, 2018; Lee et al., 2020; Merians et al., 2019), adult physical health (Merians et al., 2019), and sexual risk behaviors during adulthood (Barboza, 2018; Willie et al., 2018). While latent class approaches are less commonly applied to research on ACEs in LMICs, existing studies demonstrate class-specific patterns of ACEs associated with mental disorders, poor school attendance and violence perpetration among adolescents and young adults (Clarke et al., 2016; Ho et al., 2020; Li et al., 2021). With respect to IPV, ACEs class membership has been found to be associated with men’s psychological IPV perpetration (Zietz et al., 2020). A study in Tanzania found that men who reported severe and multiple exposure to ACEs were more likely to perpetrate psychological IPV against a female partner compared to men in other ACEs classes, after adjusting for potential confounders (Zietz et al., 2020). To date, we are unaware of existing research in Southeast Asia that estimates latent classes of ACEs and associations with IPV victimization and perpetration among young women and men. However, understanding patterns and consequences of ACEs combinations are critical to inform tailored violence prevention interventions. Targeted interventions may be particularly relevant in low-resource settings, such as Cambodia, where funding for prevention and intervention priorities is limited, despite high prevalence of ACEs and IPV. To fill this gap and inform local violence prevention priorities, we used advanced analytic methods to identify latent classes of retrospectively reported ACEs among young women and men in Cambodia and examined the associations between ACEs class membership and victimization and perpetration of physical and/or sexual IPV in young adulthood.
Methods
Data Set
We used data from the Cambodia Violence Against Children Survey (VACS), a nationally representative, cross-sectional household survey with non-institutionalized children and young adults aged 13–24 years. The VACS estimates baseline prevalence and consequences of emotional, physical, and sexual violence against children, and other ACEs including household dysfunction and community adversity (Chiang et al., 2016). Using a split-sample, multi-stage cluster design, the surveys were administered via face-to-face interviews, and data were collected through household and individual questionnaires (Nguyen et al., 2019). The Cambodia VACS used electronic data collection, where interviewers entered the survey data into CSPro programmed on netbooks. The VACS adapted World Health Organization ethical and safety guidelines on conducting research on violence against women and children, including tailored multi-stage response protocols to support youth who disclose abuse (Nguyen et al., 2019; World Health Organization, 2001).
The Cambodia VACS was implemented in 2013, led by the Cambodia Ministry of Women’s Affairs with coordination support from UNICEF Cambodia and technical assistance from the Cambodia National Institute of Statistics, Ministry of Planning and the U.S. Centers for Disease Control and Prevention’s Division of Violence Prevention (Ministry of Women’s Affairs, 2014). The sampling frame was generated by the National Institute of Statistics for the Cambodian national population census in 2013. Villages within communes were selected based on probability proportional to size. Enumeration areas served as the primary sampling unit and were stratified by sex so that boys and girls were not interviewed in the same enumeration area. Interviews were completed in private locations to protect the privacy and confidentiality of participants. Verbal consent/assent was obtained from each participant. In households where the selected participant was younger than 18 years, consent was first obtained from the parent or caregiver followed by assent from the participant. Individual response rates were 93.7% and 92.1% for girls/young women and boys/young men, respectively. A total of 1121 girls and young women and 1255 boys and young men completed the survey. To measure completed exposure to ACEs, and distinguish between childhood and young adulthood adversity, we restricted our analytic sample to ever-partnered young women (N f = 369) and young men (N m = 298) aged 18–24 years.
Latent Class Manifest Variables
For latent class analysis, we generated seven dichotomous ACEs variables from 18 survey items on childhood adversity before age 18 years. Multi-item manifest ACEs variables were generated due to low prevalence (e.g., <.5%) of some survey items, particularly sexual and severe physical abuse. ACEs items were similar to those included in the Adverse Childhood Experiences International Questionnaire (ACE-IQ) (World Health organization, 2018), although not all items from the ACE-IQ were included in the Cambodia VACS. Physical abuse by parents/caregivers was coded yes if participants reported that a parent or other adult relative ever (1) punched, kicked, whipped, or beaten them; (2) choked, smothered, tried to drown them, or burned them intentionally; or (3) used or threatened them with a knife or other weapon. Physical abuse by community members was coded yes if participants experienced any of the above by a member of their community including teachers, police, religious or community leaders, friends, classmates, or strangers. Emotional abuse by a parent or caregiver was coded yes if a participant’s parent or someone like a parent ever told them that (1) they were not loved or did not deserve to be loved; said they wished they had never been born or were dead; (3) or ever ridiculed them or put them down (for example say that they were stupid or useless). Sexual violence was coded as yes if respondents responded affirmatively to experiencing any contact or non-contact sexual violence. Contact sexual violence included sexual touching without permission, attempted sexual intercourse, physically forced sexual intercourse, and pressured sexual intercourse. Non-contact sexual violence included becoming upset by being spoken to in a sexual way or writing sexual things about them; being forced to watch sex photos or videos against their will; or being forced to be in a sex photo or video against their will. Death of either/both parent(s) was coded yes if participants reported the death of either their mother or father or both before age 18 years. Witnessing physical violence in the home was coded yes if participants reported seeing an adult hurt or scare another adult by slapping, punching, or kicking them; or using or threatening to use a knife, gun, stick, rock, or other similar weapon. Witnessing violence in the community was coded yes if participants reported seeing anyone physically hurt or scare someone else in their community before age 18 years. For purposes of comparison with latent class membership, we generated a single dichotomous measure of exposure to any ACE and a continuous cumulative risk score that summed exposure to all ACE manifest variables (range = 0–7).
Outcome Measures and Covariates
For both females and males, adulthood exposure to physical and/or sexual IPV victimization was measured by a dichotomous variable of whether a participant had ever experienced physical and/or sexual IPV by a romantic partner/husband (for young women)/wife (for young men). Indicators of physical IPV included whether a romantic partner ever: slapped or pushed; punched, kicked, whipped, or beat the participant; choked, smothered, tried to drown, or burned the participant intentionally; or used or threatened the participant with a knife or other weapon. Sexual IPV victimization was measured by four indicators of sexual abuse by a romantic partner: unwanted sexual touching, attempted forced sex, physically forced sex, and pressured into sexual intercourse when they did not want it. Participants were coded as experiencing physical and/or sexual IPV victimization if they responded yes to any of the above survey items and experienced the violence after age 18 years. Young adult perpetration of physical and/or sexual IPV was measured by a dichotomous variable of whether participants had ever perpetrated at least one form of physical or sexual IPV against a romantic partner/husband (for females)/wives (for males), and a measure of IPV perpetration frequency. Physical IPV items included the following behaviors against a current or previous partner: slapped or pushed; punched, kicked, whipped, or beat with an object; choked, smothered, tried to down or intentionally burned or scalded; or used or threatened to use a knife or other weapon. Sexual IPV perpetration was measured by a single item: whether participants had ever forced a current or previous partner to have sexual intercourse or perform other sex acts when they did not want to. Physical and sexual IPV perpetration were combined into a single variable due to low prevalence of sexual IPV perpetration among both young women and young men. Participants were coded as perpetrating physical and/or sexual IPV if they responded “once,” “few,” or “many” times to any of the five items. We also calculated frequency perpetration scores among all ever-partnered participants. Higher scores indicated greater frequency of perpetration. We controlled for household wealth quintile (categorical). Wealth quintiles were constructed based on the DHS Wealth Index measurement approach. This approach uses principal components analysis of household survey items related to country-specific indicators of household wealth to generate a wealth score for each household. Household survey items include, for example, source of drinking water, type of toilet facilities, material of floor, walls and roof, source of cooking fuel and household possessions (Rutstein, n.d.).
Analytic Design
We estimated weighted prevalence of descriptive characteristics, ACEs, and IPV indicators among ever-partnered young women (N f = 369) and young men (N m = 298). To identify latent classes of ACEs for young women and men, and evaluate associations between latent classes and IPV outcomes, we implemented a three-step analysis using BCH weights in Mplus, and accounting for the complex survey design of the Cambodia VACS (Asparouhov & Muthén, 2021; Muthén & Muthén, 1998–2017). We first estimated the latent class measurement model by fitting ACEs manifest variables to sequential models ranging from two to six possible latent classes (Muthén & Muthén, 1998–2017). Model identification was tested with 1000 sets of random starting values. Model fit was compared using Akaike’s information criterion (AIC), Bayesian information criterion (BIC), Lo-Mendell-Rubin test, the entropy value, and model interpretability (Collins & Lanza, 2010; Lo et al., 2001). To aid model selection, we evaluated the relationship between individual indicator variables and the latent variable, as well as item-response probabilities to assess homogeneity and latent class separation (Collins & Lanza, 2010). High homogeneity signals that class membership aligned with a common observed response pattern. In other words, all participants in a class had the same or similar responses across ACE’s indicators. A high degree of latent class separation indicated that a particular response pattern was characteristic of a single latent class only.
We then estimated associations between latent classes with three distal outcomes (IPV victimization, IPV perpetration, and frequency of IPV perpetration). The BCH approach assigns participants to latent classes based on posterior probabilities and generates weights to account for classification error (Asparouhov & Muthén, 2021; Nylund-Gibson et al., 2019). We regressed each outcome on the modally assigned latent class membership, adjusting for wealth quantile.
For comparison purposes, we also estimated the associations between two standard measures of ACEs (a summative score and a dichotomous variable, 0 vs. any ACE) with all three IPV outcomes. All analyses were stratified by sex. We estimated descriptive statistics using Stata/SE 16 (StataCorp, 2019). We used Mplus 8.5 for all other analyses (Muthén & Muthén, 1998–2017).
Results
Prevalence of Adverse Childhood Experiences
Weighted Percentages of Demographic Characteristics, Adverse Childhood Experiences (ACEs) and Intimate Partner Violence (IPV) Among Ever-Partnered Young Women and Men Aged 18–24 years, Cambodia Violence against Children Survey, 2013.

Prevalence of Intimate Partner Violence
Among women, 13% experienced physical and/or sexual IPV. Among men, 7% experienced physical and/or sexual IPV (Table 1). Women reported higher prevalence of perpetrating physical and/or sexual IPV, with nearly one in three (30%) women perpetrating physical and/or sexual IPV compared to 17% of men.
Latent Class Analysis
Summary Information for Selecting Number of Latent Classes of Adverse Childhood Experiences (ACEs) Among Ever-Partnered Women and Men Aged 18–24 years, Cambodia Violence against Children Survey, 2013.

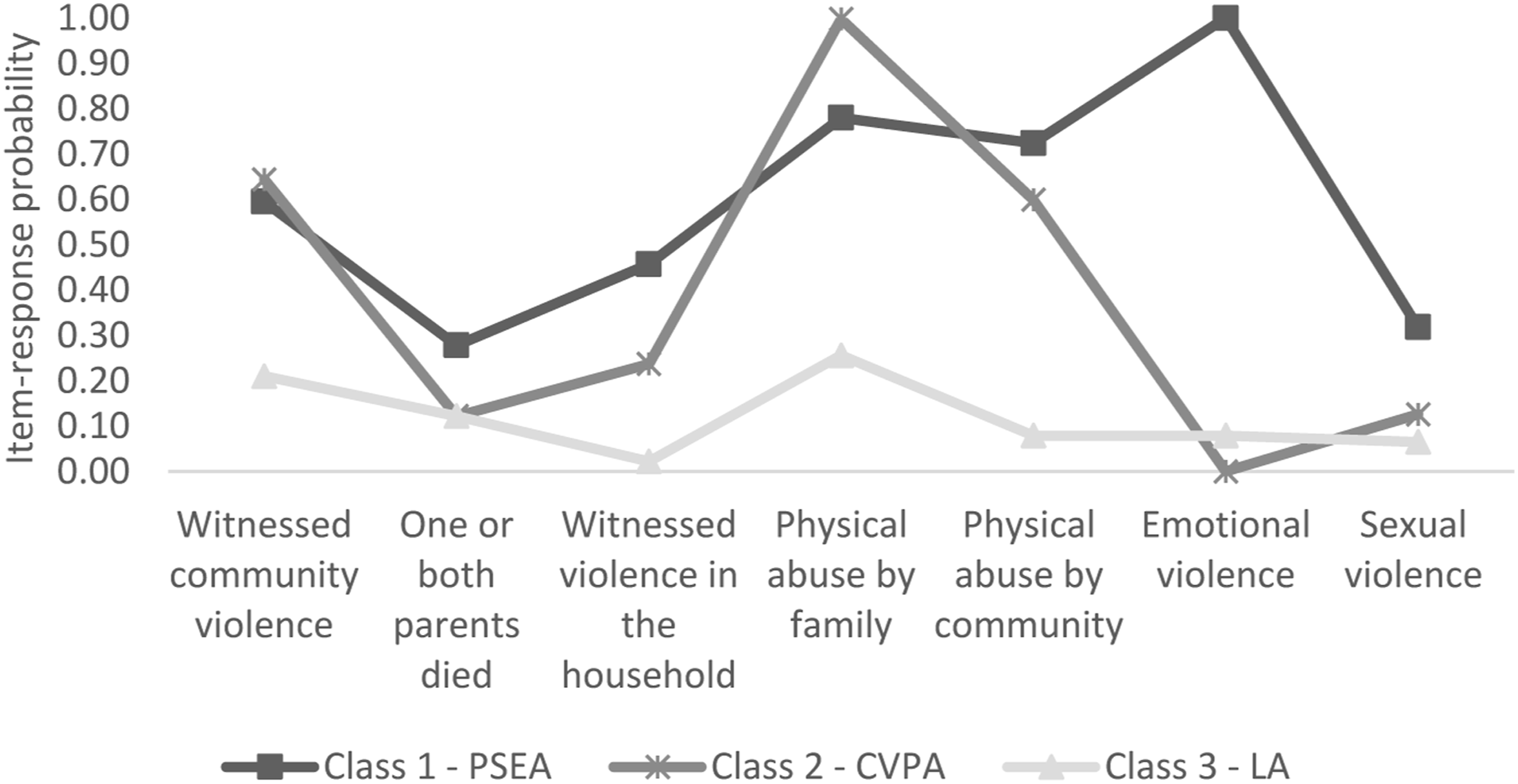
Latent class profiles for 3-class model of adverse childhood experiences (ACEs) among ever-partnered young women. Note. Abbreviations: PSEA = physical, sexual, and emotional abuse; CVPA = community violence and physical abuse; LA = low ACEs.
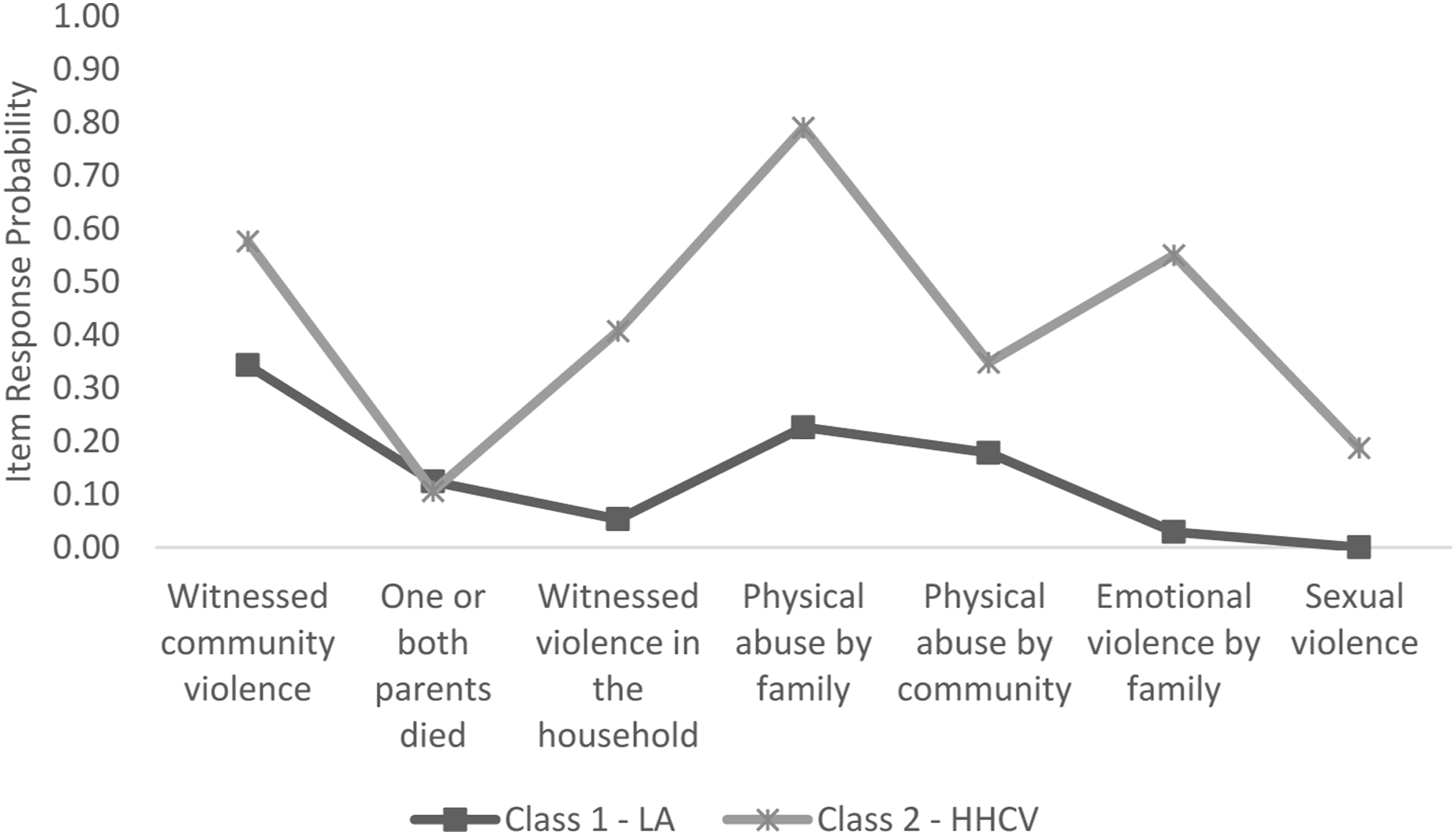
Latent class profiles for 2-class model of adverse childhood experiences (ACEs) among ever-partnered young men. Note. Abbreviations: LA = Low ACEs; HHCV = Household and community violence.
Classification Probabilities for the Most Likely Latent Class Membership (Column) by Latent Class (Row).

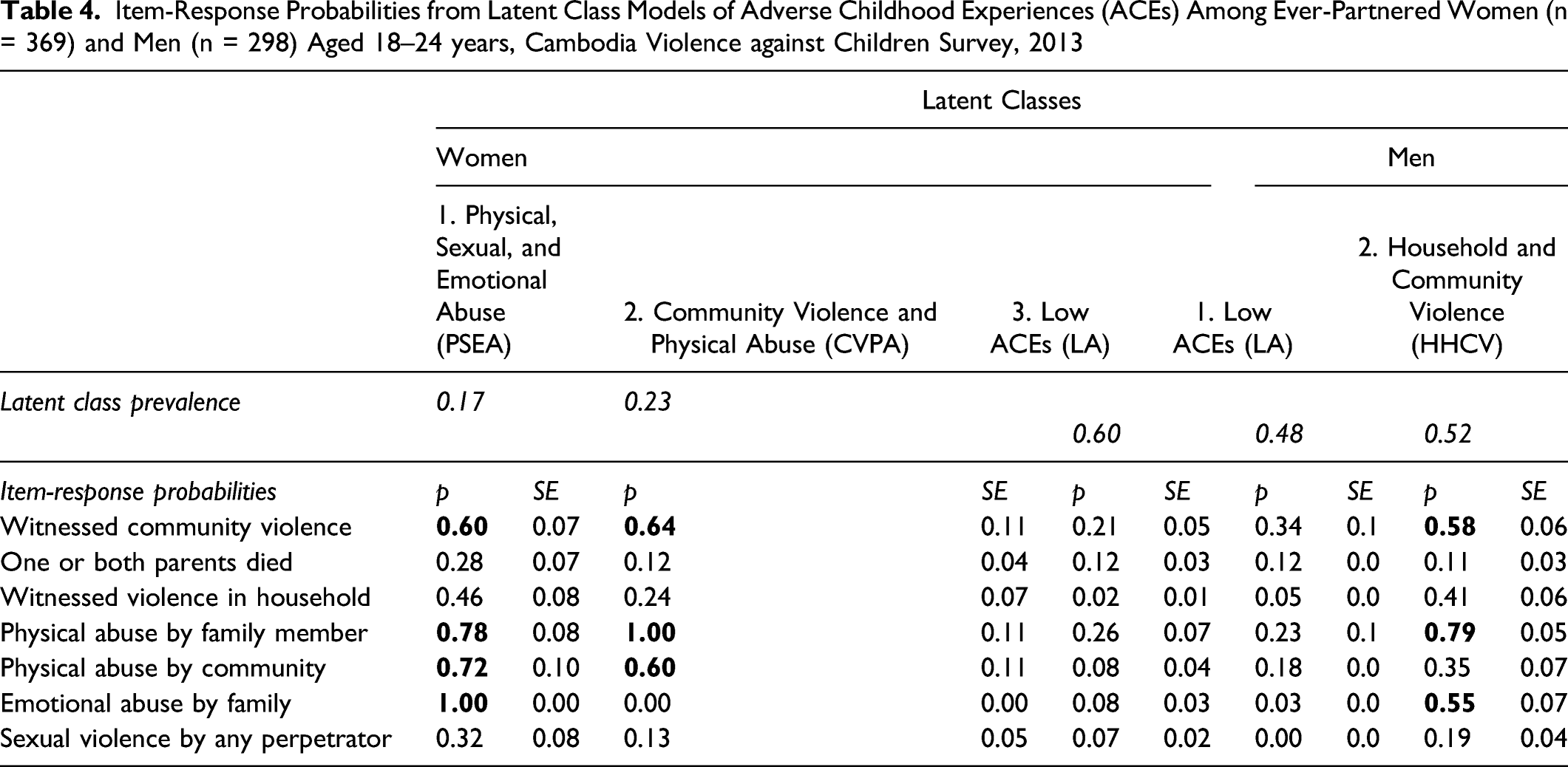
Item-Response Probabilities from Latent Class Models of Adverse Childhood Experiences (ACEs) Among Ever-Partnered Women (n = 369) and Men (n = 298) Aged 18–24 years, Cambodia Violence against Children Survey, 2013
Latent Classes with Intimate Partner Violence Outcomes
Among women, those in the PSEA and CVPA classes demonstrated increased odds of IPV outcomes in young adult relationships compared to women in the LA class (Figures 3 and 4). Among all classes, women in the PSEA class experienced the highest odds of IPV outcomes. Women in the PSEA class had 3.85 times greater odds of experiencing physical and/or sexual IPV victimization compared to women in the LA class (95% CI: 1.80, 8.22). Women in the PSEA and CVPA classes had 4.85 and 3.31 greater odds, respectively, of perpetrating physical and/or sexual IPV against an intimate partner in young adulthood (95% CI: 2.61, 9.02; 95% CI: 1.67, 6.56; respectively). Both classes also had greater odds than the reference class (LA) to experience higher frequency of IPV perpetration in their young adult relationships. Probability of intimate partner violence victimization or perpetration by adverse childhood experiences (ACEs) class membership. Note. Abbreviations: PSEA = physical, sexual, and emotional abuse; CVPA = community violence and physical abuse; HHCV = household and community violence; LA = low ACEs. Mean level of intimate partner violence perpetration frequency by adverse childhood experiences (ACEs) class membership. Note. Abbreviations: PSEA = Physical, sexual, and emotional abuse; CVPA = Community violence and physical abuse; HHCV = household and community violence; LA = low ACEs.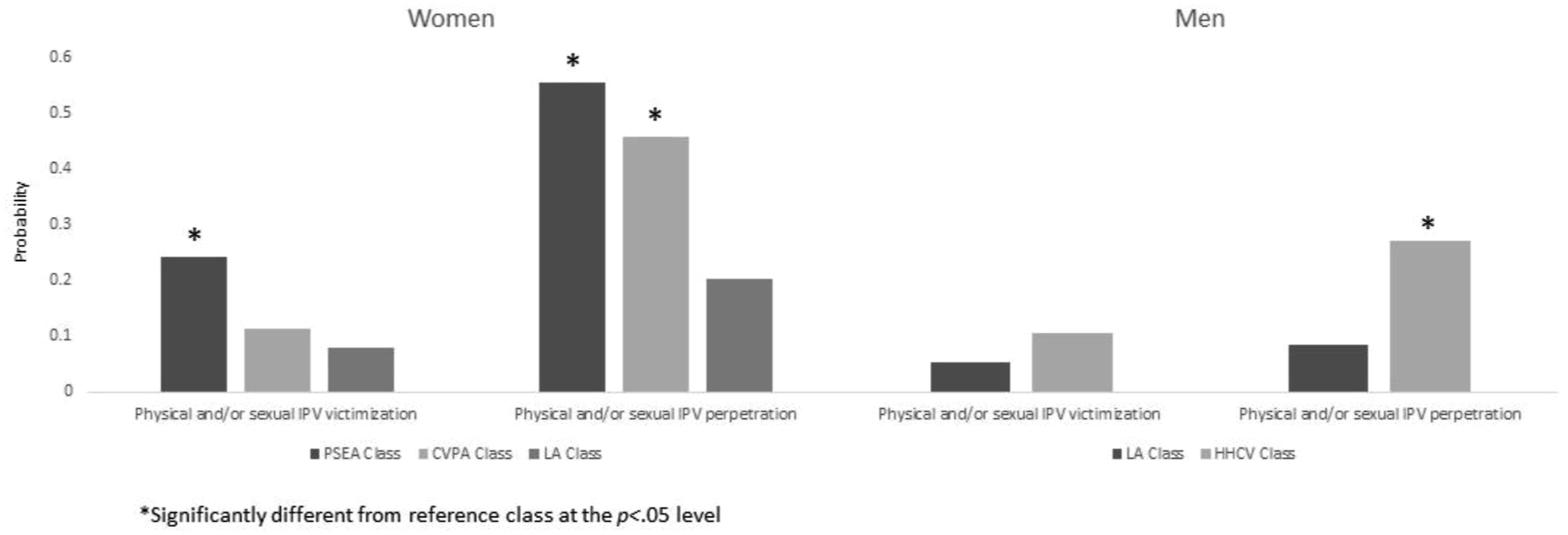
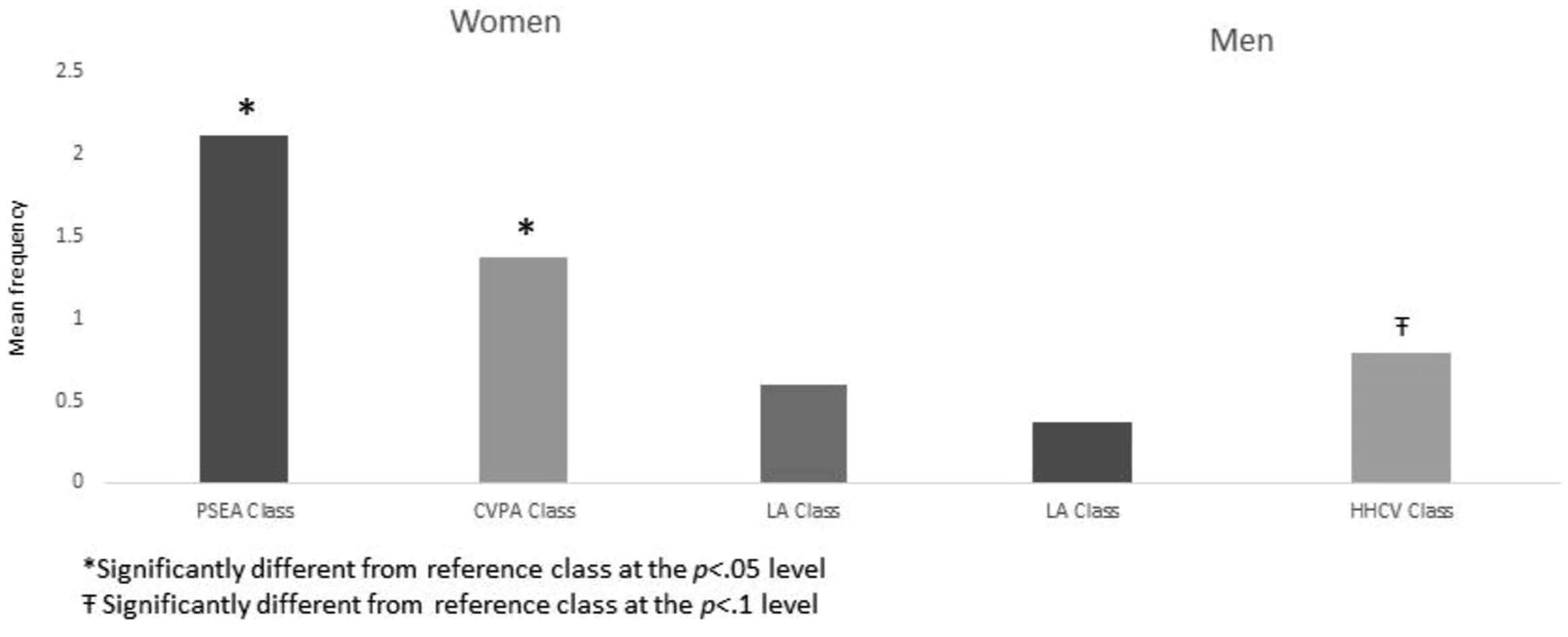
Among men, we found no significant differences between ACEs classes with respect to physical and/or sexual IPV victimization. However, those in the HHCV class had greater odds of perpetrating physical and/or sexual IPV against a partner, compared to men in the LA class (aOR = 3.73, 95% CI: 1.44, 9.68). Men in the HHCV class also had marginally higher odds of perpetrating IPV at greater average frequency compared to the LA class (β = 0.45, 95% CI: 1.02, 2.38), although the results were significant only at the 0.10 level (Figures 3 and 4).
Standard Adverse Childhood Experiences measures with Intimate Partner Violence outcomes
Associations between Adverse Childhood Experiences (ACEs) Latent Class Membership and Intimate Partner Violence (IPV) Victimization, Perpetration, and Perpetration Frequency among Ever-Partnered Young Women (n = 362) and men (n = 298) in Cambodia.

Note. All models adjusted for wealth categories. Bold = significant at the p < 0.05 level. Abbreviations: LA = low ACEs; CVPA = community violence and physical abuse; PSEA = physical, sexual and emotional abuse; HHCV = household and community violence.
Discussion
In this study examining classes of ACEs and IPV among a nationally representative sample of young Cambodian women and men, we found distinct classes of ACEs, and these ACEs classes showed variation in associations with IPV risk during young adulthood. We identified three classes of ACEs for women and two classes of ACEs for men. For both women and men, community-based ACEs (e.g., witnessing community violence or experiencing physical abuse by a community member) were high across the sample and tended to co-occur with elevated probability of other forms of ACEs. The relevance of community-based ACEs across latent classes aligns with studies demonstrating high levels of community violence in Cambodia, and supports evidence-based efforts to consider community violence as an ACE category (Lee et al., 2020) and complementary prevention priority alongside existing IPV prevention efforts (Thulin et al., 2021). Between the two higher ACEs classes among women, exposure to emotional abuse by family members and exposure to sexual violence distinguished the PSEA from the CVPA class. The PSEA class for women and the HHCV class for men had similar latent class profiles, characterized by high probability of household physical and emotional abuse, community violence and relative probability of sexual violence exposure. These results suggest that some underlying latent classes of ACEs may be similar for young women and men in Cambodia. However, women in the PSEA class had higher probability of physical abuse by community members, sexual violence, and death of one or both parents compared to men in the HHCV class. Between these two classes, young women’s greater probability of experiencing physical abuse by community members and sexual violence compared to young men may reflect the influence of normative environments (e.g., community norms that control women’s movements and sexualize women’s bodies) on women’s experiences of childhood adversity (Jacobsen, 2012). Further research on the determinants of ACEs latent class membership in Cambodia—and elsewhere—is needed.
Notably, even among women and men with low probabilities for any ACEs (LA class), participants had a moderate probability of witnessing community violence and experiencing physical abuse by family members. These results signal the regularity of these two ACEs across youth experiences, which is consistent with studies demonstrating the normative use of child corporal punishment and prevalence of community violence in Cambodia (Nho & Seng, 2017; Yi et al., 2013). The results of this latent class analysis provide support for conceptualizing and measuring ACEs as sex-differentiated classifications in Cambodia.
Classes of ACEs for women and men were significantly associated with increased risk of IPV victimization and perpetration in their young adult relationships. Women and men with high probability of multiple household level ACEs, such as witnessing violence or experiencing physical or emotional abuse by a family member, had elevated odds of exposure to IPV as young adults. As the PSEA and HHCV classes for women and men, respectively, showed the greatest odds of IPV outcomes in young adulthood, these results may signal the salience of emotional abuse and sexual violence to women and men’s risk of adversity in their adult intimate relationships in this context. Comparison with models using traditional ACEs measurement approaches suggest that latent classes may provide more nuanced understanding of the sequelae of ACEs combinations than more commonly used measures (Lanier et al., 2018). Thus, replication of the latent class approach can advance research on patterns and sequelae of ACEs in LMICs.
Women’s experiences of physical and/or sexual IPV perpetration were higher than those of men, which is counter to other studies comparing women and men’s perpetration of IPV in LMICs (Swedo et al., 2019). Women’s experiences of physical and/or sexual IPV victimization were also higher than those of men. With respect to IPV perpetration, we caution against direct comparison between women and men’s prevalence estimates. Despite national advocacy efforts, violence against women is prevalent and normalized in Cambodia (Fulu & Miedema, 2015; Jacobsen, 2012; Yount & Carrera, 2006). The Cambodia VACS questionnaire items do not provide contextual information on women’s use of aggression against a male partner, nor do they collect dyadic data to ascertain whether women’s perpetration of IPV is unidirectional, bidirectional, or mutual. However, in other LMICs, women’s physical aggression against a partner is often applied as self-defense or reactive against men’s perpetration of violence (Garcia-Moreno et al., 2005). Women tend to perpetrate less physically aggressive forms of IPV (e.g., pushing, slapping, kicking) even while they are at risk of exposure to more severe forms of IPV by male partners (e.g., choking, slamming into a wall, coercive control, or sexual violence) (Hardesty & Ogolsky, 2020; Swan et al., 2012). In Southeast Asia, over half of female homicides are perpetrated by intimate partners (59%) compared to less than 1% for male homicides (Stöckl et al., 2013). Finally, studies underscore how interpretation and consequences of violence itself are gendered: women’s violence against men tends to be construed as less threatening than men’s violence against women, and women experience disproportionately greater consequences (e.g., injuries, depression, anxiety, and post-traumatic stress) (Caldwell et al., 2012). For these reasons, we interpret these results among women as indicative of associations between ACEs classes and intra-couple conflict within early adult partnerships, rather than direct comparison of women’s and men’s perpetration of physical and/or sexual IPV.
Together, our results have several implications for violence prevention efforts in Cambodia. Latent class profiles on ACEs suggest that youth in Cambodia face distinct typologies of poly-victimization, even while exposures to physical abuse in the household and community violence exposure are universally moderate to high. Tailored interventions with youth disproportionately affected by high levels of household and community violence may be particularly effective at preventing reoccurrence of violence across life stages. For example, adaptation and implementation of interventions shown to be effective in preventing emotional abuse and sexual violence among children and adolescents may be particularly relevant for boys and girls in high ACEs exposure classes in Cambodia. Culturally relevant adaptations of effective violence prevention interventions and strategies may reduce emotional abuse and sexual violence by building social-emotional, conflict management, and healthy communication skills (Basile et al., 2016; Niolon et al., 2017; World Health Organization, 2016). Given the high probability of community violence across latent classes, practitioners, and policy makers may consider prioritizing community-based violence prevention and reduction strategies to decrease child exposure to violence in their neighborhoods and villages. For example, the INSPIRE Framework, coordinated by the World Health Organization and Centers for Disease Control and Prevention, lists community mobilization programs as an effective strategy to shift community norms and attitudes around violence, and increase community intervention and response to violence (World Health Organization, 2016). Similarly, implementation of culturally-appropriate interventions to promote positive parenting and guardianship may reduce the prevalence of physical violence, including corporal punishment, in the home (Nho & Seng, 2017; World Health Organization, 2016). In one Cambodian study, mother and child participation in early childhood education programs was indirectly associated with reductions in harsh parenting practices via mother’s agency suggesting that ACEs prevention efforts might also have cross-generational effects on both child abuse and mother’s empowerment (Grace, 2019). Future research is needed to explore factors that predict class membership to identify entry points for ACEs prevention and distinguish unique risk factors for children in classes with high exposure to multiple forms of childhood adversity (Clarke et al., 2016).
Limitations
This study has several limitations. ACEs items were retrospectively reported by young Cambodian women and men. Due to small sample size, we were unable to disaggregate all ACEs by the perpetrator or location. For example, our measure of sexual violence includes sexual violence by any perpetrator before age 18 years. Studies in other LMICs find distinct patterning of ACEs classes by types of perpetrators (Clarke et al., 2016). Further, we were limited in our measurement of ACEs based on available measures in the data set. Future research in Cambodia could explore latent classes of expanded ACEs distinguished by location (e.g., school, home, community) or perpetrator (e.g., mother, father, teacher, peer), and inclusive of other types of ACEs (e.g., peer bullying and violence by teachers) which could further assist in identifying violence prevention priorities. Measurement of IPV did not distinguish between heterosexual or same-sex intimate partnerships. Further research is needed on how patterns of IPV and associations with ACEs may vary between heterosexual and sexual minority couples. Finally, the Cambodia VACs did not include information on frequency of IPV victimization and we were unable to assess the relationship between ACEs classes and how often women and men experienced physical and/or sexual IPV victimization. However, in general we are unaware of other studies examining latent classes of childhood adversity and their relationships with both adult IPV victimization and perpetration in Cambodia, or other LMICs. The present study advances our understanding of ACEs poly-victimization and sequelae of ACEs among youth in Cambodia.
Conclusion
Young women and men in Cambodia experience distinct combinations of ACEs in childhood, which in turn are differentially associated with physical and/or sexual IPV risk in young adulthood. Identification of previously unobserved sub-groups of childhood adversity can help tailor intervention strategies and prevention strategies to improve overall child health and wellbeing, and interrupt risk of violence in adult intimate relationships. We encourage further application of these latent class analytic approaches to understand contextual patterning of ACEs and risk with adulthood adversity in other LMICs. Evaluation of latent class membership characteristics may be useful to identify strategic populations for prevention interventions and improve efforts to identify and implement contextually appropriate violence prevention strategies.
Footnotes
Acknowledgments
The authors gratefully acknowledge Dr. Allison Tracy for consultation on distal outcome analyses and the two anonymous reviewers who provided feedback. The findings and conclusions in this manuscript are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.