
Abstract
Sexual harassment and violence is a grave public health concern and risk for revictimization increases following initial exposure. Studies of sexual revictimization in military samples are generally limited to women and are focused on rates of posttraumatic stress disorder (PTSD), with no examination of how revictimization relates to interpersonal outcomes, such as relationship or sexual satisfaction. The current study addressed these gaps in a sample of 833 women and 556 men service members/veterans. Self-reported outcomes of PTSD, depression, suicidal ideation, sexual function, and relationship satisfaction were compared across those reporting exposure to sexual harassment and violence before the military only (i.e., pre-military), during the military only (i.e., military sexual harassment and violence [MSV]), before and during the military (i.e., revictimization), and to no exposure. More than half of women (51.14%, n = 426) reported revictimization and only 5.79% (n = 28) of men reported revictimization. Among women, those reporting MSV or revictimization tended to report higher PTSD, depression, and suicidal ideation relative to pre-military sexual violence and no sexual violence exposure. No interpersonal outcomes were significantly different among these sexual violence groups. Among men, revictimization was associated with higher PTSD, depression, and sexual compulsivity. PTSD and depression were also higher among those reporting MSV only. No effects were found for premilitary sexual trauma exposure only or relationship satisfaction for either group. Findings highlight the particularly bothersome nature of MSV, whether it occurred alone or in tandem with premilitary sexual violence. Findings also show unique gender differences across outcomes, suggesting interventions following sexual harassment and violence may differ for men and women.
Keywords
Exposure to military sexual harassment and violence (MSV) is a critical public health concern among service members/veterans (SM/Vs), impacting at least 15.7% of men and women (see review, Wilson and White, 2018). Indeed, experiencing MSV is associated with increased risk for posttraumatic stress disorder (PTSD), depression, substance and alcohol use disorders, as well as suicide (e.g., Blais & Geiser, 2019; Kimerling et al., 2007). Moreover, MSV is positively correlated with greater distress relative to other trauma exposures, including combat (i.e., Blais et al., 2020; Blais & Monteith, 2019). In fact, MSV is associated with more severe distress and impairment relative to sexual violence that occurred before or after military service (Creech & Orchowski, 2016; Himmelfarb et al., 2006), highlighting its complex and lasting nature.
According to several learning models and theories that contextualize the traumatic response (e.g., classical, operant conditioning; see Bisson, 2009; Zayfert, 2011), initial trauma exposure would ostensibly lead to decreased likelihood of subsequent re-exposures due to avoidant coping, trauma over-generalization, or decreased risk taking (Bisson, 2009). However, extant literature shows that exposure to one instance of sexual violence increases risk for subsequent exposures in military samples (e.g., Dichter et al., 2017; Himmelfarb et al., 2006; Schry et al., 2016), making revictimization a probable experience for many. Moreover, while survivors of sexual violence may engage in behaviors that reduce their individual risk (e.g., avoiding situations/locations related to the experience of sexual violence), sexual perpetration persists. For these reasons, re-exposure to trauma was coined “one of the most perplexing of phenomena in the field of traumatic stress” (Zayfert, 2011, p. 9). In military samples, rates of revictimization in convenience samples ranged from 28-71% (e.g., Creech & Orchowski, 2016; Tirone et al., 2020).
Research shows that sexual revictimization is associated with more severe psychological distress and dysfunction relative to a single instance of sexual victimization. For example, studies examining outcomes among SM/Vs reporting a history of sexual revictimization observed higher depression and PTSD severity relative to SM/Vs reporting a single instance of sexual violence (Portnoy et al., 2020; Sadler et al., 2005; Tirone et al., 2020; Zinzow et al., 2008). Additionally, those who endorsed revictimization reported greater use of mental health services (Sadler et al., 2005), potentially underscoring the particularly traumatic nature of revictimization. Civilian literature shows a strong association between revictimization and suicide (Balsam et al., 2011; Chou, 2012), yet few studies have examined this association in military samples. This is surprising given that SM/Vs are more likely than civilians to be exposed to sexual violence and have increased suicide risk more generally (e.g., Watkins et al., 2018). As such, there is a critical need for additional research that explores the association of sexual revictimization and suicide in military samples. In addition to exploring the association of revictimization with PTSD and depression, one of the primary aims of the current study is to examine the association of sexual revictimization and suicide in a sample of men and women SM/Vs.
Few studies have examined interpersonal outcomes associated with sexual revictimization, despite the interpersonal nature of sexual violence. Monteith and colleagues (2019) observed that among men reporting a history of MSV, problems with intimacy and relationship distress were reported. Unfortunately, the study was circumscribed to a small sample of men (n = 18) using a qualitative study design, limiting generalizability to larger samples of men or to women. Notably, recent literature shows that exposure to MSV is associated with poorer relationship satisfaction in women (Blais, 2020) and men (Blais, 2021a) and greater sexual dysfunction and dissatisfaction in women (Blais, 2020) and men (Blais, 2021b). While these latter studies are informative and highlight how MSV is associated with poorer interpersonal outcomes, such studies did not examine whether revictimization was associated with worse interpersonal outcomes relative to single instances of sexual violence. In the current study, we will explore key interpersonal factors such as relationship satisfaction and sexual function with revictimization.
Finally, a notable limitation in the extant literature on sexual revictimization among SM/Vs is that samples are typically circumscribed to women (e.g., Himmelfarb et al., 2006; Luterek et al., 2011; Portnoy et al., 2020), despite men experiencing at least comparative distress following MSV exposure (Kimerling et al., 2007; Tannahill et al., 2020), more severe and long-lasting distress (O’Brien et al., 2008; Shipherd et al., 2009), or experiencing fewer treatment gains for MSV-related treatment (Khan et al., 2020). Indeed, no studies that examined outcomes of revictimization specifically of men SM/Vs were identified. In studies that did include men, authors concluded that the rates of reported revictimization were too low to meaningfully analyze (e.g., Luterek et al., 2011). While this might suggest that revictimization is a less severe public health concern in men, the low rate of men reporting revictimization is thought to be a sampling issue or due to lack of reporting. Indeed, there is research and theory for both men and women that each would experience negative outcomes following sexual revictimization. For instance, acceptance of rape myths (Burt, 1980), or false beliefs about rape, are shown to be associated with greater psychological distress following sexual assault (Wilson et al., 2018). Research shows that men are particularly likely to ascribe to such rape myths in both military and civilian samples (e.g., Anderson et al., 1997; Carroll et al., 2016; Chapleau et al., 2008; Walfield, 2018), thereby suggesting a potentially increased risk in men for negative outcomes following sexual violence. Alternatively, women may also experience notable difficulties following sexual revictimization, particularly with interpersonal experiences such as romantic relationship satisfaction or sexual function given the interpersonal nature of MSV coupled with women’s heightened susceptibility for suffering following interpersonal conflict (e.g., Wanic & Kulik, 2011). In the current study, we included a sample of men to examine possible gender differences in outcomes as a function of revictimization.
To summarize, we sought to expand the literature on revictimization in military samples by filling key gaps in our understanding of this phenomenon. Specifically, we expanded the study of individual outcomes by exploring suicidal ideation (in addition to PTSD and depression severity), including a sample of men, and exploring interpersonal outcomes. To build this literature, we explored three groups of sexual harassment and violence survivors: those reporting exposure to sexual harassment and violence before the military only (i.e., pre-military only), those reporting exposure to sexual harassment and violence during the military only (i.e., MSV only), or those reporting exposure to sexual harassment and violence before and during the military (i.e., revictimization). All groups were compared to one another and compared to those reporting no history of sexual violence. We hypothesized that for all outcomes and both genders, revictimization would be associated with poorer outcomes relative to exposure to no sexual violence, pre-military only, or MSV only. Moreover, we hypothesized that MSV would be associated with poorer outcomes relative to no sexual harassment and violence and pre-military exposure only.
Methods
Participants
Data for the current study were extracted from two gender-specific parent studies that assessed MSV, sexual health, and satisfaction in relationships among women (N = 833; (Blais, 2020)) and men SM/Vs in partnered relationships (N = 556; (Blais, 2021)).
Procedure
Both studies had identical methodology and recruited participants through Facebook advertisements and online listservs. Prior to enrolling, participants completed screening questions confirming service in the military, being of ages 18–65, and being partnered at the time of participation. Those who passed screening questions were provided with a Letter of Information and all study questions. Materials were administered through Qualtrics (2020). Those wishing to receive compensation of $15 navigated to a separate page where they could enter identifying information. Identifying information was not linked to study data. Approval for these two studies was granted by the Institutional Review Board at Utah State University. Given the nature of this secondary data analysis, we were unable to compare identical kinds of sexual health concerns and made use of the sexual health measures included in both gender-specific parent surveys.
Measures
Covariates
Covariates of age, marital status, and discharge status were collected through a demographic inventory. Age was measured as a continuous variable. Marital status was coded 1 (married) versus 0 (not married) and discharge status was coded 1 (veteran) versus 0 (active service member). To describe sample composition, variables of race and ethnicity (Black, Native American, Latina, White, and biracial) were also collected and reported in the results section.
History of Sexual (Re)victimization
Sexual victimization was assessed through the combination of two sets of questions that identified MSV and premilitary sexual trauma. For MSV, an adapted version of the Veterans Affairs Military Sexual Trauma Screener (Kimerling et al., 2007) assessed whether participants experienced unwanted sexual harassment (e.g., cornering, pressure for sexual favors) or sexual assault (e.g., unwanted touching, rape). Participants who reported experiencing either type of sexual harassment and/or assault during their military service were coded as experiencing MSV. For premilitary sexual trauma, identical questions were asked through the time period specified that the violence had to occur before military service. Those that reported revictimization endorsed experiencing both MSV and sexual harassment and violence before military service, resulting in four distinct and exclusive groups: those reporting no exposure, those reporting exposure to sexual harassment and violence before the military only (i.e., premilitary only), those reporting exposure to sexual harassment and violence during the military only (i.e., MSV only ), or those reporting exposure to sexual harassment and violence before and during the military (i.e., revictimization).
PTSD
Symptoms of PTSD were measured through the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013), which research indicates is a measure with good internal consistency, test-retest reliability, and adequate convergent and divergent validity (Blevins et al., 2015). Scores on this 20-item self-report measure range from 0 to 80, with higher scores indicating worse PTSD symptom severity. Responses to the PCL-5 items are based on a five-point Likert scale of 1 (not at all) to 5 (extremely). A sample item includes “In the past month, how much were you been bothered by feeling very upset when something reminded you of the stressful experience?” With the current sample, the PCL-5 showed excellent internal reliability (Cronbach’s α = .97 for the women’s sample and .97 for the men’s sample).
Depression
Symptoms of depression were assessed using the Patient Health Questionnaire-8 (PHQ-8; Kroenke et al., 2009), which research indicates is a valid and reliable screener for depression symptoms (Kroenke et al., 2001). Scores on this 8-item inventory range from 0 to 24, with higher scores indicating more severe depression symptoms. Responses to the PHQ-8 are provided through a Likert scale of 0 (not at all) to 3 (nearly every day). A sample item includes “Over the past two weeks, how often have you been bothered by feeling down, depressed, or hopeless?” The current sample showed adequate internal reliability (Cronbach’s α = .92 for the women’s sample and .91 for the men’s sample).
Suicidal Ideation
Suicidal ideation was measured through the ninth item of the Patient Health Questionnaire-9 (PHQ-9; Kroenke & Spitzer, 2002), which has been shown through previous research to identify veterans with higher suicide risk (Louzon et al., 2016). Scores on this single item range from 0 to 3, with higher scores indicating increased suicidal ideation. Participants report their level of suicidal ideation based on an ordinal scale of 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). The item is stated as follows: “During the past two weeks, how often have you been bothered by thoughts that you would be better off dead or hurting yourself in some way?”
Relationship Satisfaction
Romantic relationship satisfaction was assessed through the Couples Satisfaction Index – 4 (CSI-4; Funk & Rogge, 2007), which previous research reports have adequate convergent validity with other romantic relationship satisfaction assessments (Funk & Rogge, 2007). Scores on this four-item index are summed for a total score that ranges from 0 to 21, with higher scores indicating greater relationship satisfaction. Participants’ responses are based on a Likert scale with varying anchors and that range from 0 (not at all) to 5 (completely) or 0 (extremely unhappy) to 6 (perfect). A CSI-4 sample item includes “How rewarding is your relationship with your partner?” Cronbach’s alphas in the current samples were adequate (Cronbach’s α = .90 for the women’s sample and .86 for the men’s sample).
Sexual Function - Women
Sexual function among women SM/Vs was examined using the Female Sexual Function Index (FSFI; Rosen et al., 2000), which previous research reports have good test-retest reliability, internal consistency, and adequate construct and divergent validity (Rosen et al., 2000). Scores on the 19-item scale range from 2 to 36, with lower scores indicating worse sexual function (e.g., worse desire, lubrication, orgasm, etc.). Participants report their sexual function based on a variable anchor Likert scale of 0–5 or 1–5. An example item from the FSFI includes “Over the past four weeks, how would you rate your level (degree) of sexual desire or interest?” The women’s sample showed adequate internal reliability (Cronbach’s α = .88).
Sexual Satisfaction - Women
Sexual satisfaction was examined with the Sexual Satisfaction Scale for Women (SSS-W; Meston & Trapnell, 2005), which previous research reports have strong internal consistency and validity (Meston & Trapnell, 2005). Scores on the 30-item self-report inventory are summed and scored using an algorithm developed by the scale authors. Scores range from 27.5 to 135, with lower scores indicating worse sexual satisfaction. Responses are scored on a Likert scale from 1 (strongly disagree) to 5 (strongly agree). A sample item from the SSS-W includes “I feel I do not have enough emotional closeness.” With the women’s sample, the SSS-W showed adequate internal reliability, (Cronbach’s α = .84).
Sexual Compulsion - Men
Sexual compulsivity among men SM/Vs was measured using the Sexual Compulsivity Scale (SCS; Kalichman et al., 1994), which reportedly has adequate validity and reliability (Kalichman et al., 1994). The SCS assesses for difficulty controlling sexual thoughts/behaviors through 10-items that are summed for total scores ranging from 10–40, with higher scores indicating greater difficulty with sexual compulsivity. Participants’ responses are scored on a Likert scale from 1 (not at all like me) to 4 (very much like me). A sample item from the SCS includes “I have to struggle to control my sexual thoughts and behavior.” In the current study, the SCS showed adequate internal reliability in the men’s sample (Cronbach’s α = .89).
Erectile Dysfunction - Men
Erectile dysfunction was assessed with the Sexual Health Inventory for Men (SHIM; also known as the International Index of Erectile Dysfunction-5), which measure authors report is a reliable and valid instrument (Rosen et al., 1999). This 5-item self-report measure is summed to create a total score ranging from 1–25, with lower scores indicating greater difficulties with erectile dysfunction. Participants’ responses are scored through a variable anchor Likert scale with item response ranging from 0–5 or 1–5. A SHIM sample item includes “Over the past six months how do you rate your confidence that you could get and keep an erection?” Among men SM/Vs included in the current study, the SHIM had excellent internal reliability (Cronbach’s α = .94).
Analytic Plan
Demographic Characteristics of Women Service Members/Veterans Based on Mean (SD) or Count (%), N = 819.
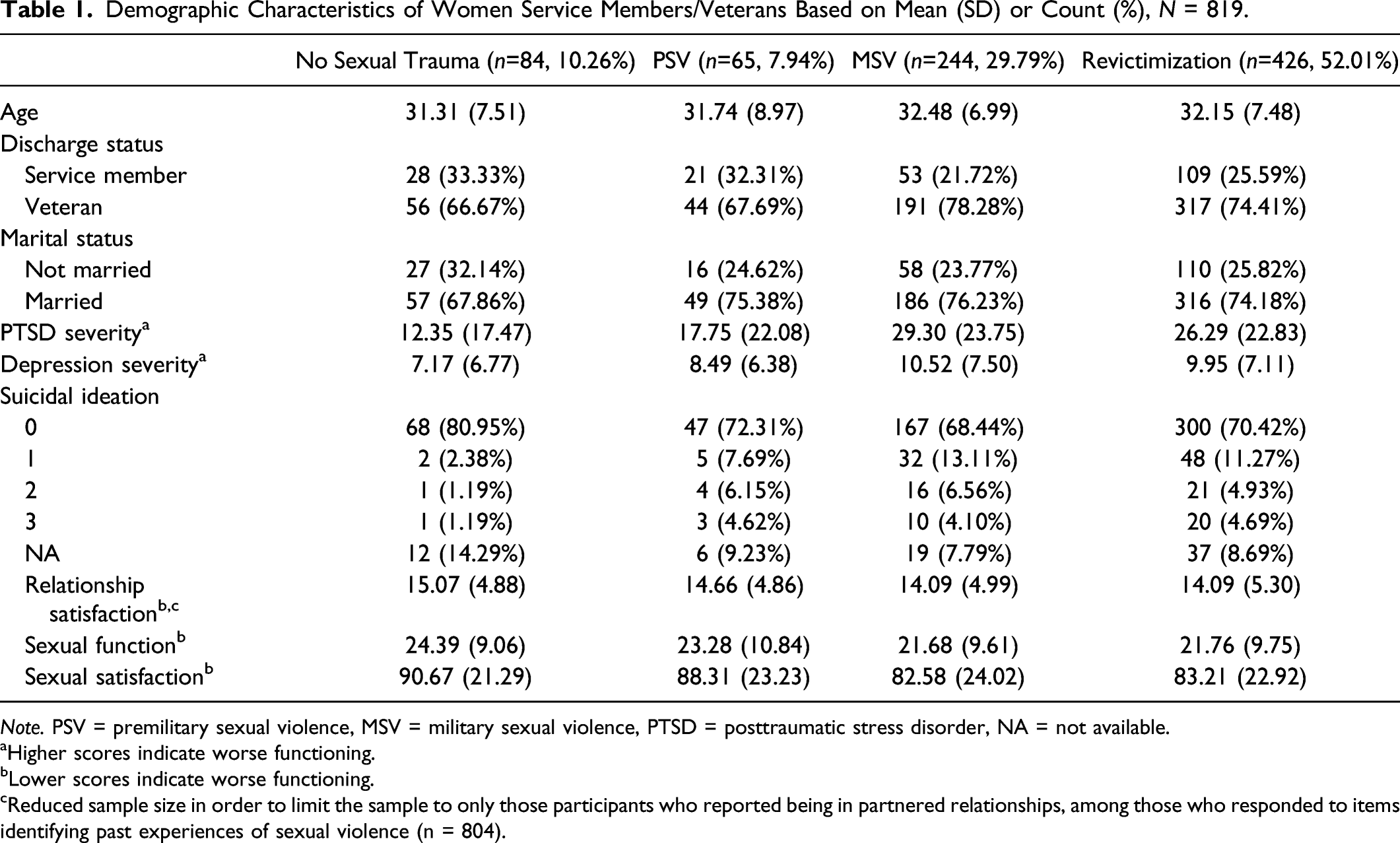
Note. PSV = premilitary sexual violence, MSV = military sexual violence, PTSD = posttraumatic stress disorder, NA = not available.
aHigher scores indicate worse functioning.
bLower scores indicate worse functioning.
cReduced sample size in order to limit the sample to only those participants who reported being in partnered relationships, among those who responded to items identifying past experiences of sexual violence (n = 804).
Demographic Characteristics of Men Service Members/Veterans Based on Mean (SD) or Count (%), N = 484.

Note. PSV = premilitary sexual violence, MSV = military sexual violence, PTSD = posttraumatic stress disorder, NA = not available.
aHigher scores indicate worse functioning.
bLower scores indicate worse functioning.
cReduced sample size in order to limit the sample to only those participants who reported being in partnered relationships, among those who responded to items identifying past experiences of sexual violence (n = 475).
Linear, logistic, and ordinal logistic regression models assessed whether no sexual trauma, premilitary sexual trauma, MSV, and revictimization were associated with mental health outcomes, while accounting for covariates. To determine whether these sexual trauma groups significantly differed from one another when considering their association with the mental health outcomes, contrasts were tested for each outcome. These contrasts estimated the differences between all pairs of the four groups (i.e., no sexual trauma, premilitary sexual trauma, MSV, and revictimization). The regression models were carried out separately with the women and men samples, while adjusting for age, marital status, and discharge status. The specific tests conducted for each outcome are described below.
To examine the association of revictimization groups with symptoms of PTSD and depression, two-step hurdle models were used, given the preponderance of zeros found with the PCL-5 (156 [18.72%] responses of zero among women and 56 [14.43%] among men SM/Vs) and PHQ-8 measures (72 [9.70%] responses of zero among women and 34 [9.26%] among men SM/Vs). In the first step, the PCL-5 or PHQ-8 total scores were coded as 0 (for all total scores = 0) and 1 (all total scores ≥1). Logistic regressions estimated the association of each sexual harassment and violence group and the covariates with dichotomous PCL-5 or PHQ-8 outcome variables. In the second step, as is necessary for hurdle models, all individuals with a total score of zero for the PCL-5 or PHQ-8 were removed from the analysis. Then, linear regressions were applied to the remaining observations of the continuous PCL-5 or PHQ-8 outcome variables. Together, the two-steps of the hurdle models provide estimates of the differences between the groups on having any symptoms and on having a higher number of symptoms. Similar methods have been used in other research to handle the preponderance of zeros on outcome measures (e.g., Tannahill et al., 2021). For the continuous outcome measures—relationship satisfaction, sexual function (solely among women), sexual satisfaction (solely among women), sexual compulsivity (solely among men), and erectile dysfunction (solely among men)—linear regression models estimated the differences between the sexual harassment and violence groups. Notably, the outcome of romantic relationship satisfaction was only explored among those who identified as partnered at the time of participation (women: n = 818; men = 499). Finally, ordinal logistic regression models assessed suicidal ideation (four level ordinal dependent variable) among women and men SM/Vs. Specifically, the MASS package in R (Venables & Ripley, 2002) was used to assess how the levels of the PHQ item 9 differed between the groups for both men and women separately.
Both the women and men SM/V datasets had missing data. Of the 833 women SM/Vs, missingness across the outcome measures ranged from 1.6-10.9%. Of the 556 men SM/Vs, missingness across the outcome measures ranged from 20.3-34.0%. To account for missing data, multiple imputation using predictive mean matching was used in all regression analyses (Enders, 2010). The “mice” package in R (van Buuren & Groothuis-Oudshoorn, 2011) was used to create the imputations for the women SM/V and men SM/V data separately. Due to testing multiple comparisons, we accounted for the false discovery rate by adjusting the reported p-values in all analyses (Benjamini & Hochberg, 1995). The R statistical environment was used to conduct all analyses (R Core Team, 2020). Full syntax and output for study analyses can be found at https://osf.io/qvzs2/.
Results
The full sample comprised of 883 women SM/Vs and 556 men SM/Vs. For women SM/Vs, the average age was 32.10 (standard deviation [SD] = 7.44), the majority of the sample was married (n = 614, 73.71%), and discharged from the military (n = 620, 74.43%). The racial and ethnic composition of the women’s sample was majority White (n = 640, 76.83%), with other participants identifying as Black (n = 39, 4.68%), Native American (n = 4, 0.48%), Latina (n = 50, 6.00%), and biracial (n = 80, 9.60%). For men SM/Vs, the average age was 39.05 (SD = 10.70), the majority of the sample was married (n = 384, 69.06%), and discharged from the military (n = 339, 60.97%). The racial and ethnic composition of the men’s sample was White (n = 444, 79.86%), with other participants identifying as Black (n = 23, 4.14%), Native American (n = 14, 2.52%), Latino (n = 33, 5.94%), and biracial (n = 14, 2.52%). Sample characteristics are further described and stratified by history of sexual harassment and violence in Tables 1 and 2. The men’s and women’s samples demonstrated an inverse pattern of reported sexual victimization. That is, more than half the women reported revictimzation and only about 10% reported no victimization (see Table 1) whereas an opposite trend occurred for men: less than 6% of men reported revictimization whereas about 75% reported no victimization (see Table 2). In these tables, the sample size for women SM/Vs reported in Table 1 is 819 and for men SM/Vs reported in Table 2 is 484 due to missing data among responses to sexual harassment and violence items.
Regression Analyses for Women SM/Vs
Mental Health Outcomes Regressed on Types of Sexual Violence Among Women Service Members/Veterans.

Note. PSV = premilitary sexual violence, MSV = military sexual violence, PTSD = posttraumatic stress disorder. Covariates of age, discharge status, and marital status adjusted for in all regressions. Outcomes were tested in separate regressions. Unstandardized betas reported for models with outcomes that are continuous, including PTSD severity, depression severity, relationship satisfaction, sexual function, and sexual satisfaction. Odds ratios are provided for models with outcomes that are dichotomous, including PTSD symptoms and depression symptoms. Odds ratios are provided for the models with suicide ideation as the outcome as this was tested with an ordinal logistic regression. Bolded estimates indicate significant associations with outcomes based on p < .05. For PTSD severity and depression severity, the sample sizes are smaller as these were tested with hurdle models where responses of zero were removed. For relationship satisfaction, the sample size was reduced in order to limit the sample to only those participants who reported being in partnered relationships.
aHigher scores indicate worse functioning.
bLower scores indicate worse functioning.
cFor relationship satisfaction, the sample size was reduced in order to limit the sample to only those participants who reported being in partnered relationships (n=818). d,ep<.001. fp=.002. gp=.016. hp=.047. ip=.047. jp=.021. kp=.030. l,mp=.005.
PTSD
For the first step of the PTSD hurdle models, where we examined differences among those with no symptoms versus any symptoms, MSV and revictimization (premilitary sexual trauma + MSV) relative to no sexual trauma were associated with presence of PTSD symptoms among women SM/Vs. MSV and revictimization relative to premilitary sexual trauma were each significantly associated with presence of PTSD symptoms. For the second step of the hurdle models, where we examined symptom severity among those reporting at least some symptoms, MSV and revictimization relative to no sexual trauma were each significantly associated with higher PTSD symptoms. No other comparisons were significant between sexual trauma groups on the presence of PTSD symptoms and PTSD severity.
Depression
For the first step of the hurdle model, where we examined differences among those with no symptoms versus any symptoms, only revictimization relative to no sexual trauma was significantly associated with presence of one or more depression symptoms. For the second step of the hurdle model, where we examined symptom severity among those reporting at least some symptoms, MSV relative to no sexual trauma was associated with higher depression symptoms. No other associations were significant between sexual trauma groups on the presence of depression symptoms and depression severity.
Suicidal Ideation
For suicidal ideation, MSV and revictimization relative to no sexual trauma were associated with suicidal ideation among women SM/Vs. No other comparisons were significant between sexual trauma groups on suicidal ideation.
Relationship Satisfaction and Sexual health
There were no significant associations between sexual trauma groups and relationship satisfaction, sexual function, and sexual satisfaction.
Regression Analyses for Men SM/Vs
Mental Health Outcomes Regressed on Types of Sexual Violence Among Men Service Members/Veterans.

Note. PSV = premilitary sexual violence, MSV = military sexual violence, PTSD = posttraumatic stress disorder. Covariates of age, discharge status, and marital status adjusted for in all regressions. Outcomes were tested in separate regressions. Unstandardized betas reported for models with outcomes that are continuous, including PTSD severity, depression severity, relationship satisfaction, sexual function, and sexual satisfaction. Odds ratios are provided for models with outcomes that are dichotomous, including PTSD symptoms and depression symptoms. Odds ratios are provided for the models with suicide ideation as the outcome as this was tested with an ordinal logistic regression. Bolded estimates indicate significant associations with outcomes based on p < .05. For PTSD severity and depression severity, the sample sizes are smaller as these were tested with hurdle models where responses of zero were removed. For relationship satisfaction, the sample size was reduced in order to limit the sample to only those participants who reported being in partnered relationships.
aHigher scores indicate worse functioning.
bLower scores indicate worse functioning.
cFor relationship satisfaction, the sample size was reduced in order to limit the sample to only those participants who reported being in partnered relationships (n=499). dp=.024. ep=.010. f,g,hp=.043. ip<.001. jp=.043. kp<.001. lp=.043.
PTSD
For the first step of the hurdle models, where we examined differences among those with no symptoms versus any symptoms, there were no significant associations between sexual trauma groups and presence of PTSD symptoms among men SM/Vs. Conversely, the second step of the hurdle model, where we examined symptom severity among those reporting at least some symptoms, MSV and revictimization in comparison to no sexual trauma were significantly associated with higher PTSD symptom severity. No other sexual trauma group comparisons were significantly associated with the presence of PTSD symptoms or PTSD severity.
Depression
For the first step of the hurdle models, where we examined differences among those with no symptoms versus any symptoms, there were no significant associations between sexual trauma group and presence of depression symptoms. In the second step of the hurdle model, where we examined symptom severity among those reporting at least some symptoms, MSV and revictimization relative to no sexual trauma were associated with higher depression severity. No other comparisons examining sexual trauma groups on the presence of depression symptoms and depression severity were significant among men SM/Vs.
Suicidal Ideation
For suicidal ideation as the outcome, revictimization relative to no sexual trauma was associated with suicidal ideation. No other sexual trauma group comparisons were associated with suicidal ideation.
Relationship Satisfaction and Sexual health
For relationship satisfaction, there were no significant associations between sexual trauma groups with relationship satisfaction. For sexual compulsivity among men SM/Vs, revictimization relative to no sexual trauma was associated with increased sexual compulsivity. Additionally, revictimization relative to premilitary sexual trauma was associated with higher sexual compulsivity. Finally, revictimization compared to MSV was significantly associated with increased sexual compulsivity among men SM/Vs. For erectile dysfunction, MSV relative to no sexual trauma was associated with worse erectile dysfunction among men SM/Vs. No other trauma comparisons were significantly associated with erectile dysfunction. Estimates for covariates across all regressions can be received by contacting the corresponding author of this paper.
Discussion
The purpose of the current study was to examine individual and interpersonal outcomes associated with exposure to sexual harassment and violence in a sample of men and women SM/Vs. Namely, we sought to broaden the literature by comparing premilitary, MSV, and sexual revictimization with PTSD, depression, suicidal ideation, relationship satisfaction, and sexual health characteristics. Our findings showed that different categories of sexual victimization had unique associations with individual and interpersonal outcomes and gender differences in these associations were observed.
Prior literature on revictimization in SM/Vs was largely circumscribed to describing risks for PTSD relative to single exposures or no exposures (Portnoy et al., 2020; Sadler et al., 2005; Tirone et al., 2020; Zinzow et al., 2008). Similar to previous findings, revictimization and MSV in the current study were associated with higher PTSD severity for both men and women when compared to no exposure to sexual harassment and violence. Revictimization and MSV were also associated with the presence of any PTSD symptoms relative to no exposure or premilitary exposure in women, but this latter effect was not observed in men. This is consistent with previous research showing that women with history of MSV were at greater risk for the presence of PTSD symptoms relative to men (Tannahill et al., 2021). For both men and women, there were no differences in the presence of PTSD symptoms among those reporting MSV versus revictimization. Such findings may suggest that revictimization and MSV could be distinguished from premilitary exposure in women, but this distinction does not seem to exist in men.
Fewer effects were observed for depression. Revictimization was associated with the presence of depression symptoms relative to no exposure in women, but this effect was not observed in men. Women with exposure to MSV reported more severe depression relative to those reporting no exposure, while men with MSV and revictimization reported higher depression than those reporting no exposure. Such findings suggest that for both men and women, exposure to premilitary sexual trauma does not confer greater risk for depression.
This is the first quantitative study to our knowledge to examine sexual revictimization and suicide risk in a military population. Among women, exposure to MSV and revictimization were associated with higher suicidal ideation relative to no exposure. Interestingly, there were no differences between sexual harassment and violence exposure groups, suggesting that MSV and revictimization exert that same level of risk for suicidal ideation. Among men, compared to no exposure to sexual harassment and violence, only revictimization was associated with suicidal ideation. Such findings highlight the particularly devastating association of MSV with suicidal ideation. That is, for both men and women, exposure to MSV, whether alone or in tandem with premilitary sexual harassment and violence, was associated with higher suicidal ideation. These findings suggest that it is important to screen for suicidal ideation when treating those reporting a history of MSV. As revictimization did not confer a greater risk for suicidal ideation in the current sample, uniform screening (as compared to enhanced screening among those reporting exposure to revictimization) may be adequate to identify those at risk for having thoughts of ending one’s life. As noted by Kimerling et al. (2016), including preventative measures for MSV will be an important element of suicide prevention strategies, and including exposure to MSV into predictive models of suicide is critical.
The relationship of varying exposures to sexual harassment violence and interpersonal outcomes, which included relationship satisfaction, sexual function and satisfaction in women, and sexual compulsivity and erectile dysfunction in men, included key gender differences such that unique associations were observed for men but not women. This may be due to factors particularly salient to the male gender, such as male gender role expectations and avoidant coping. Indeed, societal male gender norms suggest that men should be emotionally tough and self-reliant (Levant & Richmond, 2007). However, after experiencing a traumatic event such as sexual victimization, emotional toughness is associated with negative mental health outcomes (e.g., Jakupcak et al., 2014; Morrison, 2012). The literature suggests that men tend to cope with the psychological effects of MSV with avoidance methods, such as the use of substance (Monteith, Brownstone, et al., 2019; Monteith, Gerber, et al., 2019), which is shown to be negatively associated with overall sexual function (Kumsar et al., 2016; Peugh & Belenko, 2001). This may explain the current study’s findings of men’s worse sexual outcomes after sexual victimization. At the same time, measures assessing sexual function among men and women were markedly different, precluding us from making thorough comparisons.
Contrary to hypotheses, premilitary sexual harassment and violence, MSV, or revictimization were not associated with poorer relationship satisfaction for men or women. Given the interpersonal nature of sexual harassment and violence, it was hypothesized that it would negatively impact intimate relationships, such as satisfaction with one’s partner. Previous research examining the association of MSV and relationship satisfaction observed that the association was indirect, through the effects of higher sexual dysfunction and lower sexual satisfaction in women (Blais, 2020) and higher sexual compulsion in men (Blais, 2021b). Thus, it is possible that although not observed in the current study, the impact of sexual harassment and violence and relationship satisfaction shown in the literature is best explained by other, indirect factors. At the same time, prior research shows that it is more severe forms of sexual violence that is associated with poorer interpersonal outcomes. The current study included both harassment and assault exposures, and the inclusion of harassment may have weakened any association. Future research could explore whether severity is a critical component of this association.
Among men, revictimization was associated with higher sexual compulsivity when compared to no exposure to sexual harassment and violence, exposure to premilitary sexual harassment and violence, and exposure to MSV. However, there were no differences observed in sexual compulsivity between those reporting no sexual harassment and violence exposure, premilitary sexual trauma, and MSV. Such findings may suggest that sexual compulsivity is more likely to be problematic among those with more experiences of sexual violence across the lifespan or during different identities in life (e.g., civilian vs. service member). From a prevention of sexual compulsivity perspective, our findings suggest that measures should be taken among those reporting exposure to sexual harassment and violence during their military and premilitary lifetime, such as providing information related to experiences one might have following sexual harassment and violence. To be most efficient and accurate, screenings for sexual compulsivity may specifically target those reporting revictimization. Unfortunately, many clinics treating SM/Vs for sexual harassment and violence do not screen for sexual health issues, despite evidence showing that sexual health problems are associated with increased risk for suicide after adjusting for key mental health characteristics (e.g., depression severity; Blais et al., 2018). As causes of sexual compulsivity have yet to be firmly established (e.g., Coleman et al., 2018; Fong, 2006), it is a challenge to understand the best intervention for those who report revictimization. As scientists, we may best contribute to this line of inquiry by conducting additional studies to better understand correlates of sexual compulsivity. Unlike sexual compulsivity, erectile dysfunction had a unique association with sexual harassment and violence exposure. Contrary to hypotheses, revictimization was not associated with the greatest risk. However, MSV was associated with higher erectile dysfunction relative to no exposure; premilitary sexual harassment and violence was unrelated to erectile dysfunction. Though these results are preliminary and are based on a non-clinical convenience sample, such results may suggest that it is not non-military or cumulative exposures that are most difficult for erectile challenges, but exposures that occurred during military service.
Unfortunately, research is limited on possible gender differences associated with risk for sexual revictimization in military populations. Furthermore, the extant literature in this area is mixed as to which gender confers greater risk for revictimization. For instance, in a study of 3106 veterans, results showed that childhood sexual assault significantly increased risk for MSV in both men (OR = 3.08) and women (OR = 2.25), but adolescent sexual assault only predicted increased MSV risk in men (OR = 8.67) but not women (OR = 1.73; Schry et al., 2016). In another study of veterans, the association between MSV and intimate partner sexual violence was stronger amongst women than men (Relyea et al., 2020). Finally, one study showed that while women veterans were 10.9 times more likely than men veterans to report any history of sexual assault, the subgroups of those with history of sexual assault in both genders seemed to have similar risks of revictimization, with women at a 65% revictimization rate and men at a 52% revictimization rate (Zinzow et al., 2008). However, the genders were not compared statistically, so it is unclear if there is a significant difference in revictimization risk between genders. Taken altogether, it is unclear if there are gender differences associated with risk for sexual revictimization in military populations, or if the gender differences in patterns of victimization seen in the current study are due to risk for sexual victimization more broadly. Additional research in this area would strengthen this line of inquiry.
While not a primary aim of the current study, our samples demonstrated an inverse pattern of sexual harassment and victimization among men and women. That is, more than half of the women reported revictimization and only slightly more than 10% reported no victimization. The opposite trend occurred for men: over 76% reported no victimization and slightly less than 6% reported revictimization. This is consistent with prior research in military populations showing that women are at greater risk for sexual victimization relative to men (e.g., Kimerling et al., 2007; 2010; Wilson et al., 2018). Further, research shows that history of sexual victimization increases risk for revictimization (see review, Classen et al., 2005), which may explain the larger cell sizes in the revictimization group for women compared to men in the current study.
The current study has limitations. Data collection was based on a cross-sectional study design and was conducted on convenience samples of men and women; generalizability is limited and causal conclusions cannot be drawn. Notably, both samples were comprised of participants who were most likely to identify as white, and in the case of the male sample, heterosexual. The homogeneity of our samples should be cautiously interpreted. Coupled with the reviewed literature, which also included samples that were predominantly white and heterosexual, there is a clear need for additional research on the various minority groups found in our military, including those that identify as non-white, non-heterosexual, or gender non-conforming. Information on sexual orientation of romantic relationships or whether spouses were also part of the military were not queried. Information on the duration of time that has passed since exposure to sexual harassment and violence was not collected, nor were the cumulative number of exposures across the lifespan calculated. The level of missingness among the men SM/V sample (20.3–34.0%) should be taken into account when considering these result. Though the study assessed sexual health variables across genders, the measures used were not consistent across the men’s and women’s studies. That is, we did not measure sexual satisfaction among men nor did we examine sexual compulsivity in women. Future research in this area that used more similar measures across genders would extend these findings. Finally, information on participants’ substance use was not examined.
In summation, findings from the current study highlight the particularly bothersome nature of MSV, whether it occurred alone or in tandem with premilitary sexual harassment and violence. Moreover, our findings highlight key gender differences such that women’s dysfunction was largely circumscribed to individual outcomes whereas men’s dysfunction included both individual and interpersonal outcomes. Though sexual harassment and violence is considered an interpersonal trauma, type of sexual victimization was not related to relationship satisfaction among those who identified as partnered. This information may aid in detection and treatment planning, and interventions would be well-poised if they screened for revictimization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided to the first author from Division 19 (Society for Military Psychology) of the American Psychological Association and the Emma Eccles Jones College of Education and Human Services of Utah State University.