
Abstract
Scholars have recently begun to consider the role of bystander intervention training in countering workplace incivility and bullying. Given the scarce empirical evidence of bystander training outcomes in occupational settings, this study set out to evaluate the effectiveness of a bystander intervention training in a large healthcare organisation, by assessing changes to levels of psychological safety, bystander efficacy, intent and behaviours over time. One hundred and forty employees in a large healthcare organisation in New Zealand attended the training and were asked to complete three surveys, one conducted at baseline, one carried out 2 weeks following the training and the last survey conducted 2 months later. The qualitative and qualitative findings of this study show that the bystander intervention training resulted in significant improvements to bystander attitudes and beliefs, which were ascribed to the quality of training materials, the facilitator and opportunities to role-play bystander intervention strategies. However, the positive bystander beliefs, attitudes and intent to intervene declined in the months following the training. The qualitative findings shed a light on these results and suggest that the participants required support for training transfer in the form of updated and accessible information about negative acts and bystander intervention strategies, leadership support and role modelling of bystander behaviours and civility, and the implementation of accountability systems that ensure the ongoing development of a civility culture.
Workplace incivility and bullying (WI and WB) comprise forms of interpersonal violence that have become pervasive in contemporary organisations (Andersen et al., 2021; Courcy et al., 2019; Hodgins et al., 2014). WI and WB range from micro-aggressions and social ostracism to undermining another’s competence or contributions, insulting, yelling, sending nasty emails and spreading rumours (Lassiter et al., 2021; Schilpzand et al., 2016). These behaviours have been linked to increased absenteeism, turnover and poor performance through their detrimental impact on employee health and wellbeing (Holm et al., 2021; Porath et al., 2015). While the prevalence of incivility and bullying can be ascribed to myriad individual and contextual factors, organisational cultures characterized by low psychological safety, low support and ambiguous social norms promote and sustain these negative workplace acts. For instance, social norms that excuse or fail to check WI and WB eventually give rise to a negative or toxic organisational culture (Durand & Kremp, 2016; Fink-Samnick, 2018; Rosen et al., 2016). Importantly, they can also account for bystander effect, whereby people display low or no intention to intervene when presented with behaviours that signal interpersonal violence.
Bystander intervention training holds the promise to target WI and WB and to transform organisational cultures from toxic to healthy. Bystander intervention describes any situation where witnesses to someone in distress intervene to remedy the situation and to prevent further escalation or harm to the victim (Bennett et al., 2014). Bystander training aims to challenge the belief that inaction is acceptable, to alter individuals’ perceptions of the potential costs associated with intervening, and to increase a sense of competence around their ability to intervene (Banyard, 2008; Moschella & Banyard, 2021). Although predominantly adopted to address serious forms of behavioural misconduct such as sexual assault (e.g. Coker et al., 2011; Kania & Cale, 2021), the underlying principles of bystander intervention training can be usefully applied to different settings, social groups, and behavioural transgressions, including interpersonal violence in organisations. Bystander training participants are invited to challenge existing social norms, understand what constitutes WI and WB, internalise standards of desired conduct, appreciate the benefits of civil workplace behaviours, and feel empowered to act in a bystander situation (Courcy et al., 2019; Hodgins et al., 2014).
Though limited, the extant evidence offers preliminary support for the effectiveness of bystander intervention training to reduce WI and WB (Lassiter et al., 2021; Van Erp et al., 2018). Still, there is need for research that evaluates bystander intervention training relative to contextual barriers to training transfer (e.g. Thompson et al., 2020). This study answers recent calls for more evidence-based bystander training research (e.g. Lassiter et al., 2021) and draws on behavioural change, workplace culture and bystander effect prevention literature to evaluate a bystander intervention program aimed at reducing incivility and bullying in a large healthcare organisation. We rely on 3 surveys, conducted at baseline, 2 weeks following the training and 2 months later, to capture the training reactions, experiences WI and WB in the organisation, and changes to bystander attitudes, beliefs and behaviours among the participants.
Framing the Bystander Effect in Occupational Settings
Organisations rely on their culture and set of established norms and values to signal what constitutes acceptable and non-acceptable behaviour (Fischer et al., 2011). In the absence of clear social interaction norms, employees look to others for guidance and draw cues from their relational encounters in the organisation. When a lack of clear social norms that promote and define the parameters of positive workplace behaviours is accompanied by a weak accountability system that fails to sanction negative acts, there is a greater risk that WI and WB will occur, which over time produces a toxic culture (Schneider et al., 2013). In toxic cultures, there is an unspoken belief that the majority deem incivility and bullying the norm, or even acceptable conduct, rather than exceptional and inappropriate behaviour. Notably, this shared belief dissuades organisational members from intervening on someone’s behalf, reflecting the bystander effect. This effect can be ascribed to the reduced sense of personal responsibility for nurturing a positive social environment, the belief that someone else may be better positioned to intervene, a lack of confidence to intervene when witnessing interpersonal violence and the understanding that the personal costs of intervening outweigh the benefits (Banyard, 2008; Moschella & Banyard, 2021).
Further to established social norms and accountability systems, both the prevalence of WI and WB in organisations and the likelihood of intervening as a bystander are also influenced by leadership role modelling and by existing power structures (Freitas et al., 2019; Porath et al., 2015). Unlike egalitarian cultures that support employee voice (Detert & Treviño, 2010), rigid and hierarchical cultures can exacerbate the bystander effect by discouraging workers from exerting upward influence or standing up to a higher status member of the organisation who engages in WI or WB (Malik et al., 2020). In this instance, bystanders may perceive a lack of organisational support to intervene or deem the personal cost of intervention too high (e.g. they might become the next target of interpersonal violence) (Lassiter et al., 2021; Ortega et al., 2014). Understanding the current bystander climate of an organisation, and designing approaches that promote effective bystander intervention, require knowledge of the psychological mechanisms, social dynamics and work context that underpin the bystander effect. In what follows, we outline the literature on bystander attitudes, beliefs and behaviours in organisations to contextualise the evaluation of a bystander intervention training aimed at reducing WI and WB.
Bystander Intervention Training and Study Aims
The objectives of the bystander intervention training evaluated in this study were to reiterate civility norms, to increase a sense of psychological safety and of bystander efficacy, to change perceptions of the costs and benefits associated with intervening as a bystander (i.e. decisional balance), and to promote intervention behaviours while reducing the observed instances of incivility and bullying. These objectives will be discussed in greater detail next.
Psychological Safety
Psychological safety, defined as the extent to which employees feel accepted and supported by an organisation and its members (Ortega et al., 2014), plays an important role in producing social change in organisations and has been linked to positive organisational cultures. When employees experience psychological safety, they feel at ease to share their thoughts and concerns without fear of negative responses or judgement from others (Chen et al., 2019). At low levels of psychological safety, employees become reluctant to share ideas and voice their worries, which is indicative of a low sense of trust (Nembhard & Edmondson, 2006). The aims of bystander intervention training are precisely to encourage employees to speak up about WI and WB, and to instil a sense that it is safe to do so without negative repercussions. This type of training is the starting point to the development of a collective understanding of what is deemed appropriate or inappropriate conduct at work, which should contribute to a positive social environment and bolster organisational members’ psychological safety over time (Courcy et al., 2019; Lassiter et al., 2021). Hence, the following is expected:
Bystander Efficacy
Self-efficacy reflects the belief in one’s ability to effectively perform tasks and to achieve desirable goals (Bandura, 1997). Self-efficacy stems from the interaction of individual differences with the social context, and can develop as a function of vicarious learning, along with previous experiences of success or achievement. In the context of bystander intervention, efficacy beliefs signal one’s trust in their ability to successfully intervene, enhanced by the availability of clear information about WI and WB, knowledge of intervention strategies, and adequate support (Banyard, 2008; Bennett et al., 2014; Hoxmeier, 2019). Bystander efficacy training is expected to have a positive impact on bystander efficacy beliefs. Bystander training should: (a) raise awareness of the bystander effect and of what constitutes WI and WB through discussion and practical exercises (i.e. information), (b) outline effective bystander intervention approaches (i.e. strategies), (c) offer opportunities to observe exemplary instances of bystander intervention (i.e. vicarious learning) and (d) allow attendees to practice intervention behaviours in a safe environment (i.e. first-hand experience) (Banyard, 2008; Coker et al., 2011). It is therefore expected that bystander intervention training will increase bystander efficacy, and that this sense of efficacy will continue to improve over time as participants are encouraged to practice the behaviours as a team.
Decisional Balance
In the context of bystander intervention, decisional balance pertains to individuals’ appraisals of the pros and cons of intervening, namely their view of the consequences of engaging in bystander behaviour. People with a favourable attitude towards bystander intervention believe that the benefit of intervening outweighs any potential costs, which is indicative of a positive decisional balance. Conversely, when a person focuses on the potential costs of intervening over and above the benefits, this suggests a negative decisional balance, signalling a tendency not to intervene as a bystander. Importantly, when an organisation presents with recurring instances of WI and WB that remain unaddressed, and in which the victims display negative outcomes such as social exclusion, burnout, and decreased performance, the perceived costs of intervening as a bystander are heightened (e.g. Shea et al., 2021). Bystander training is expected to promote a positive decisional balance by highlighting the personal, relational, and organisational advantages of bystander intervention, along with the costs associated with inaction (Jensen & Raver, 2020). Though limited, the literature suggests that a positive decisional balance fosters enduring favourable attitudes toward bystander intervention, and continually reinforces intervention behaviours (Banyard & Moynihan, 2011).
Civility Norms and Negative Acts
Behavioural change in organisations requires that employees perceive the new behaviours as context-appropriate, useful to role performance, and advocated by the organisation through its shared norms and practices. The bystander effect is therefore prevalent in organisations with ambiguous social norms or where negative acts are commonplace, which further reinforce WI and WB (Rosen et al., 2016). Contrarywise, bystander intervention is more likely in organisations where employees are encouraged to identify interpersonal violence and address it as appropriate, that is, organisations with strong civility norms (Shea et al., 2021). The impact of bystander intervention training on the development of strong civility norms remains under-researched and will be examined in this study.
Clear civility norms and expectations around bystander intervention ensure that employees rely on their personal judgement and intervene when they witness WI and WB, as they deem intervention typical and expected in the organisation (Jensen & Raver, 2020). This, in turn, should also contribute to the continuing decline in the number of negative acts in the organisation (Shea et al., 2021). The development of civility norms, knowledge of bystander intervention strategies, awareness of what constitutes WI and WB and progressive decrease in the frequency and severity of negative acts are predicated on the availability of formal training and subsequent support for the enactment of bystander behaviours. Hence, this study will test the impact of bystander intervention training on the perceived civility norms of a work unit, and on the experienced frequency of negative acts in the organisation over time.
Bystander Intervention: Intention and Behaviour
Further to bystander attitudes and beliefs, intention to intervene will be examined by providing employees with scenarios that outline the four intervention strategies described in the training – Direct, Delay, Distract, Delegate (Banyard, 2008) – and ask whether they would apply any of these strategies as bystanders. Each strategy differs in the level of confrontation required, with delay being the least confrontational and direct as the most confrontational. The delay strategy involves checking in with the victim later, rather than addressing the situation immediately following the incident. Delegate entails the involvement of another individual to remedy the situation. Distract is the subtlest strategy and involves the bystander de-escalating a situation by changing the subject. Finally, the direct strategy is characterized by a physical or verbal response to the situation that immediately confronts the perpetrator (Banyard, 2008). In this study, we explored whether training affects participants’ intention to intervene as bystanders across different situations, their choice to intervene given the opportunity, and if bystander intent and behaviours are consistent with levels of psychological safety, bystander efficacy, decisional balance and perceptions of civility norms and negative acts in the organisation.
Method
Participants
This study relied on data from a unit within a large healthcare organisation in New Zealand that undertook a 1-day bystander intervention training. Of the 140 training attendees, 105 completed the pre-training survey, 67 the post-training survey and 39 submitted a complete follow-up survey. It should be noted that only 26 participants completed all the surveys and provided qualitative responses across the timepoints. Across the samples, most of the participants identified as women (64-69%). The participants’ age ranged from 26 to 65 (M = 37). The average tenure within this organisation was 5 years, ranging from less than a year to 37 years. Racioethnic diversity was not captured in this sample to minimise the risk of identification, as there was only small number of ethnic minority employees in the unit. Further, the study was reviewed and approved by the Human Ethics Committees and Māori Advisory Groups from both the researchers’ academic institution and the healthcare organisation where the study was conducted. These steps were taken to ensure that diverse perspectives and expertise informed the adaptation of study materials to the sample, guided culturally sensitive research practices, and that the reporting of findings was conducted in a diversity-responsive manner, in keeping with guidelines to address diversity in interpersonal violence research (Bent-Goodley, 2021).
Procedure
The 1-day bystander intervention training evaluated in this study was trialled within the healthcare division described above and delivered to the 140 employees in 3 groups over the course of a week. The training highlighted common instances of WI and WB, challenged harmful attitudes and beliefs associated with interpersonal violence, and conveyed appropriate social norms and bystander intervention strategies. The training also provided opportunities for open discussion and roleplaying to practice bystander intervention strategies in different workplace scenarios.
Participation in the training evaluation surveys was voluntary and no external incentives were offered. Employees in the unit received an email from the researchers ahead of the training week inviting them to participate in the evaluation study. The employees were informed of the time commitment involved, the voluntary nature of study participation, and that no personal information would be conveyed to the organisation. Participation involved the completion of three online surveys, the first survey before the training (pre-training), the second survey within 2 weeks of training completion (post-training) and the third survey 2 months after the training (follow-up). The post-training survey included both quantitative and qualitative training evaluation questions. The follow-up survey included the same measures as the post-training survey but replaced the training evaluation questions with items that covered intervention behaviours along the direct, delay, distract and delegate strategies covered in the training. Each of the surveys took no longer than 20 minutes to complete. Participant responses to the three surveys were linked through their email addresses and stored on an external server to ensure the organisation had no access to raw data. This identifying information was deleted from the dataset prior to analysis.
Measures
Except for the NAQ, measured on a frequency scale, all items were scored on 5-point Likert scales from 1= strongly agree to 5= strongly disagree.
Psychological safety was measured using an adapted version of Edmondson's (1999) 7-item brief psychological safety scale and measured the participants’ belief that their team would support them and be non-judgemental if they voiced ideas or concerns (α = .85) (Edmondson, 1999). A sample item is ‘Members of this unit/workgroup can bring up problems and tough issues’. In this study, the scale showed good reliability at pre-training (α = .87), post-training (α = .86) and follow-up (α = .87).
Self-efficacy in a situation requiring bystander intervention (i.e. bystander efficacy) was measured using an adapted version of Banyard et al.'s (2007) 14-item Bystander Efficacy scale (α = .82). This scale was adapted from college sexual assault to WI and WB using the training program scenarios for guidance. Following an exploratory factor analysis, 2 bystander efficacy factors emerged. The first factor covered items that reflected confidence to act on WI and WB and it showed good reliability at pre-training (α = .86), post-training (α = .84) and follow-up (α = .80). The second factor included items that reflected speaking up against WI and WB, with reliability ranging from excellent at pre-training (α = .91) to good at post-training (α = .85) and follow-up (α = .81). Sample items include ‘I feel confident doing something if a colleague tries to shift the blame onto another co-worker’ (acting) and ‘I feel confident speaking up at work if my supervisor is unfairly treating another co-worker’ (speaking up).
Cost-benefit attitudes towards bystander intervention were measured using an adapted version of Banyard et al.'s (2007) 11-item decisional balance scale. This scale was originally designed to measure the weight an individual placed on positive or negative outcomes of intervening in a sexual assault context. Items were modified to suit an occupational context. The negative decision balance dimension showed good reliability pre-training (α = .80), post-training (α = .81) and at follow-up (α = .80). The positive decision balance dimension had acceptable reliabilities at pre-training (α = .72), post-training (α = .71) and follow-up (α = .82). An example of a positive decisional balance item is ‘Co-workers will look up to me and admire me if I intervene’, and an example of a negative decisional balance item is ‘Intervening might cost me relationships with my co-workers’.
The perceived civility norms in the organisation were measured using the 4-item Civility Norms Brief questionnaire (α = .81-.85) (Walsh et al., 2012), and the frequency of WI and WB was assessed with the 22-item Negative Acts Frequency questionnaire (NAQ) (α = .91), which included acts directed at the employee (personal) and other negative experiences at work (work) (Einarsen et al., 2009; Malik et al., 2020). A sample item from the civility norms questionnaire is ‘Rude behaviour is not accepted in our unit/workgroup’, and a sample item from the NAQ is ‘You have been humiliated or ridiculed in connection with your work’. The civility norms scale showed excellent reliability in this study pre-training (α = .90), post-training (α = .93) and follow-up (α = .94). Following the removal of items with factor loadings below .4, the NAQ (personal) showed excellent reliability pre-training (α = .94) and follow-up (α = .90), and good reliability post-training (α = .86), while the NAQ (work) showed good reliability pre-training (α = .79), post-training (α = .80) and at follow-up (α =. 86).
Intention to intervene as a bystander was measured using a 12-item scale based on content from the intervention training. Employees rated the likelihood that they would intervene in each situation presented, which mapped onto the strategies conveyed during the training (direct, delay, distract, delegate), and covered situations where the participant was a victim or a witness of WI and WB. The four dimensions that comprise this scale are: intent to intervene as bystander when the manager is the perpetrator (manager), intent to intervene as bystander when a co-worker is the perpetrator (co-worker), intent to act when the individual is the target of incivility (personal) and intent to intervene in situations where the incivility regards hearsay about a colleague (hearsay). Example items include ‘If I overheard gossip about a coworker I would go and confront the people gossiping’, ‘I would distract manager if they were constantly interrupting a colleague’ and ‘If I received a passive aggressive email, I would address it in a direct manner’.
Bystander behaviour was measured qualitatively and quantitatively. In the quantitative portion, participants were asked to report whether an opportunity to intervene had arisen, and if they had intervened using any of the four strategies taught during the training (delay, distract, delegate, direct). This was coded as intervening (yes = 1; no = 0). Participants had the opportunity to provide a qualitative account of the situation (i.e. who was involved, what happened, and how the situation was managed).
Employees were asked to rate six statements regarding the relevance and helpfulness of the training (i.e. training evaluation), which were developed specifically for this study (α = .73). Items included ‘What was taught was valuable to create a safe and healthy workplace culture’. Further to these items, 2 qualitative questions enquired about three positive aspects of the training, and three areas of improvement for subsequent training events.
Data Analysis
All quantitative data was analysed using Jamovi (1.6.1). Exploratory factor analyses were conducted on all measures at each time point to examine their factor structure and support the creation of composite variables (Howard, 2016). Paired samples t-tests were run to test the hypotheses concerning mean differences between pre-training and post-training assessments, and between post-training and follow-up for assessments. Independent t-tests provided a comparison of the variables of interest between participants who intervened as bystanders and participants who elected not to intervene. Finally, a thematic analysis was carried out according to guidelines laid out by Braun and Clarke (2006). The purpose of this analysis was to identify strengths and areas of improvement of the bystander intervention training and to contextualise the participants’ quantitative responses.
Results
Quantitative Analysis
Preliminary Analyses
Independent samples t-tests and correlation analyses were conducted to check for gender and age effects across the variables of interest. The analyses revealed that there were no significant gender differences with respect to the bystander beliefs and attitudes, negative acts and bystander efficacy variables tested. Similarly, there were no significant correlations between these variables and age.
Pre-Training Versus Post-Training
Paired t-Tests of Pre-Training and Post-Training Assessments.

Note. N = 64; * = p < 0.05 ** = p < 0.01.
Post-Training Versus Follow-Up
Paired t-Tests of Post-Training and Follow-Up Assessments.
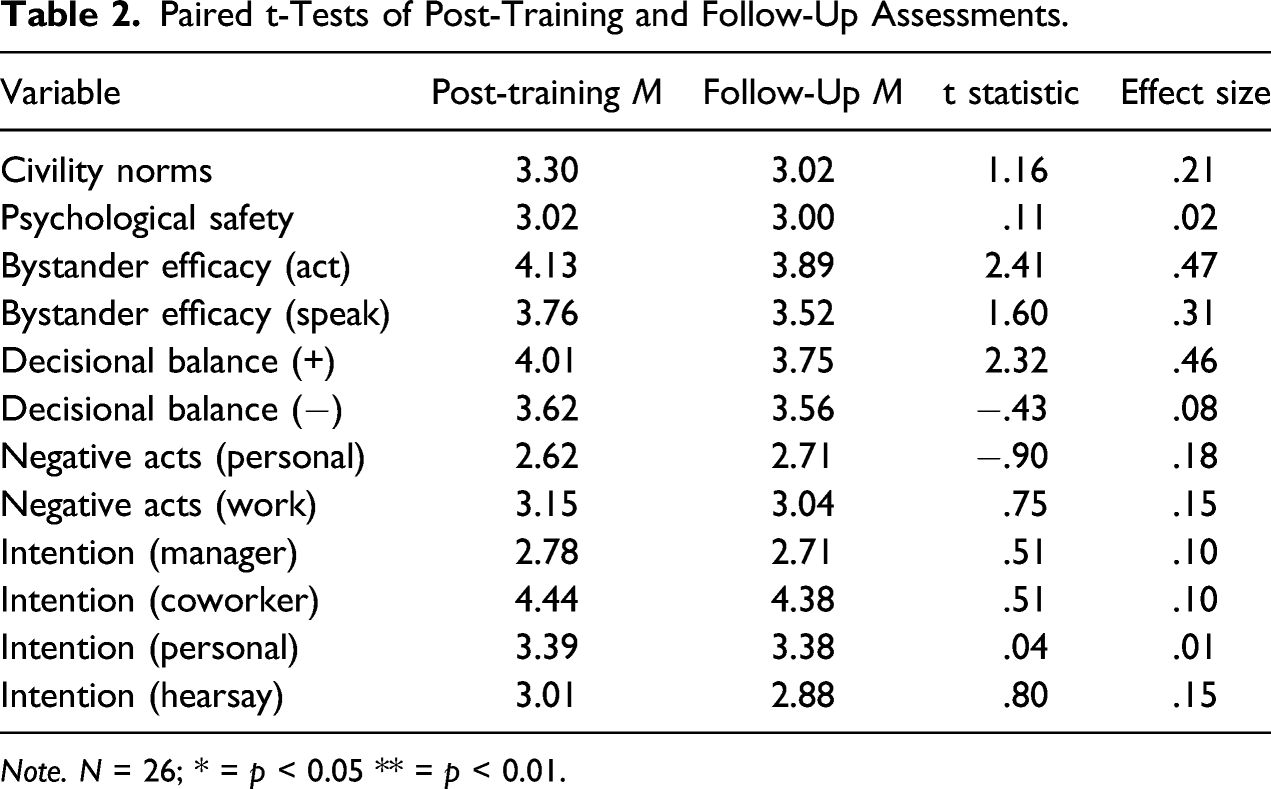
Note. N = 26; * = p < 0.05 ** = p < 0.01.
Bystander Behaviours
Independent t-Tests for Training Participants Who Had the Opportunity to Intervene at Follow-Up.
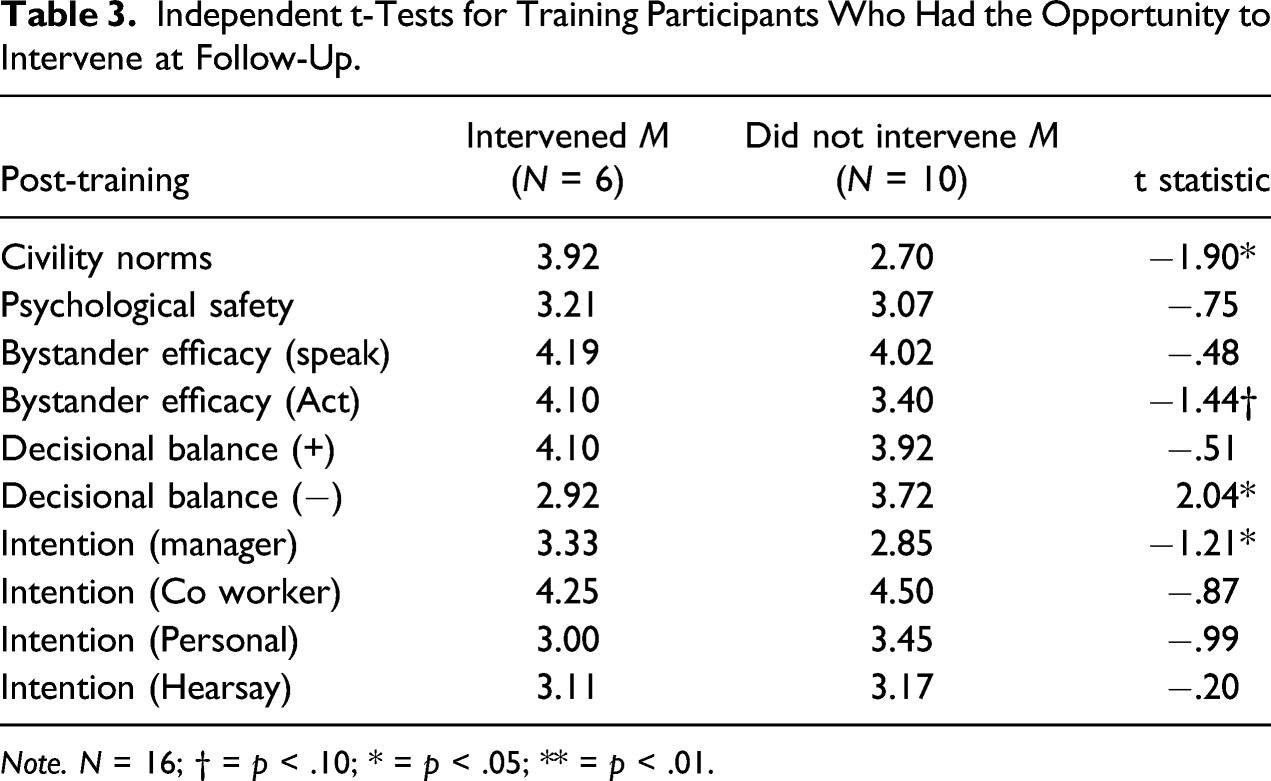
Note. N = 16; † = p < .10; * = p < .05; ** = p < .01.
Qualitative Analysis
Positive Aspects and Areas of Improvement of the Bystander Intervention Training.

Despite the generally positive views of the bystander training, the respondents identified several areas of improvement. Over half of the participants considered that guidelines for bystander intervention, including intervention strategies, points of contact and other relevant information conveyed during the training, should be made available and reiterated organisation wide. In addition, the participants wanted to gain greater experience with upward bystander intervention, as speaking up or acting when a senior leader is the perpetrator of WI or WB was viewed as a significant challenge in the organisation. About 30% of the participants remarked on the need for support to transfer training. This suggests that lack of support may partly explain the decline across bystander attitudes and behavioural intent between post-training and follow-up assessments. The participants noted that curbing WI and WB and developing a bystander intervention culture requires ongoing organisational and leadership support. Moreover, some of the respondents hoped to see more members of the senior leadership team in attendance to strengthen civility norms and develop bystander behaviours. Regarding the latter, a participant commented: ‘the people in this room didn’t need training, they have impeccable behaviour. It’s management that needs targeting’. Together, these results highlight significant leadership and cultural barriers that may undermine the effectiveness of bystander intervention training.
Discussion
Drawing on bystander intervention and behavioural change literature, this study examined the effects of bystander intervention training on bystander attitudes, intent and experiences of WI and WB in a large unit of a healthcare organisation. As predicted, our respondents reported improvements in their sense of psychological safety, bystander efficacy, perceived advantages of intervening as a bystander and intent to intervene right after the training (Banyard, 2008). Combined with the qualitative data that showed overwhelmingly positive appraisals of the training content, environment and trainer, these results substantiate the literature on training reactions, which links favourable post-training reactions to improvements in attitudes and emotional states (Aguinis & Kraiger, 2009; Shea et al., 2021).
On the other hand, the perceived costs of intervening as a bystander remained unaffected after the training. Overall, the findings reveal a contrast between improvements to proximal factors such as bystander efficacy, psychological safety and clarity of civility norms, and the unchanging perceptions of bystander intervention costs in the organisation. The results signal the importance of assisting bystander intervention through leadership support and role modelling, and communications that clarify what constitutes WI and WB, along with the benefits of eliminating interpersonal violence at work (Courcy et al., 2019; Lassiter et al., 2021). Combined with robust accountability systems, supportive leadership and communications are essential to reduce WI and WB, and to develop a healthy organisational culture (Choi & Park, 2019; Willis et al., 2016).
Contrary to our predictions and to research highlighting the increasing benefits of bystander intervention training (e.g. Amar et al., 2012), there was no significant improvement to bystander attitudes and efficacy in the months that followed the training. In effect, there was a decline across many of these indicators between post-training and follow-up measurements. These findings can be partially explained by the fact that the training was not accompanied by other organisation-wide changes to reaffirm civility norms and encourage bystander intervention. The participants foresaw barriers to the enactment of bystander behaviours (i.e. training transfer barriers) in the conspicuous absence of senior leaders from the training sessions, and in the paucity of other organisational initiatives aimed at addressing WI and WB. Poor alignment between training and the broader organisational environment and leadership constitutes a significant barrier to training transfer (Blume et al., 2010; Eid & Quinn, 2017), one that may explain the deterioration in positive bystander attitudes and beliefs among our participants in the months following the training (Shea et al., 2021). Further to these contextual barriers, levels of bystander efficacy and intention to intervene may have also been undermined by the lack of readily accessible policy and materials that specify bystander strategies and negative acts, and by the limited opportunities for practice following the training session, both of which were noted as weaknesses of the training in the qualitative statements. Limited access to information that reiterates situations where bystander intervention is appropriate, and guidelines on how to intervene, have been noted by other researchers as significant hurdles to intervention (Kania & Cale, 2021; Moschella & Banyard, 2021), and arguably played a part in the decline of bystander attitudes and efficacy beliefs among our participants.
Finally, while the study’s sample size constrains our ability to confidently draw inferences about the relationship between post-training outcomes and bystander behaviours, the findings suggest a relationship between bystander attitudes, intentions and subsequent behaviours. In this study, the participants who witnessed WI and WB and elected to intervene as bystanders also reported significantly more positive views of civility norms in the team, higher bystander efficacy, greater intent to intervene when a manager is the perpetrator, and lower perceptions of bystander intervention costs in the post-training assessment, compared to participants who chose not to intervene. While these differences may in part be the upshot of contextual factors, including position in the organisation and severity of the negative acts, they provide encouraging support for the effectiveness of bystander intervention training on the backdrop of a strong civility culture.
Limitations and Directions for Research and Practice
Though common in longitudinal studies conducted in applied settings, the considerable participation dropout across the pre-training, post-training and follow-up surveys reduced the study’s statistical power, and consequently our ability to confidently establish training effects over time. In addition, the relatively short timeframe between post-training and follow-up assessments (2 months) may be insufficient to allow for attitudinal and behavioural changes, which are best captured over a 6 or even 12-month period (Hill et al., 2016; Kania & Cale, 2021). It should also be noted that this study was carried out at the beginning of the healthcare organisation’s cultural journey. Hence, greater separation between post-training and follow-up assessments, along with improved communications and an incentive scheme to secure participation across the timepoints, might have allowed us to observe changes to bystander attitudes and behaviours, and to the organisation’s civility culture (Willis et al., 2016).
The self-report nature of our data renders our study susceptible to response biases (e.g. social desirability, recall of negative acts), to survey fatigue from repeated measurement, and to common-method bias. Despite assurance that the survey responses would be kept confidential, levels of trust in managers and the organisation may have influenced the trainees’ willingness to complete evaluation surveys, and the extent to which they provided socially desirable responses (Lines et al., 2005). One way to mitigate or account for these effects in future bystander intervention training evaluations is to include measures of trust in leadership and organisational support.
Another limitation of the study concerns sampling. The bystander training and respective evaluation surveys were conducted within a single work unit, one that is gender-diverse yet not as ethnically diverse as other parts of the organisation, which restricted our ability to conduct group analyses at this level. Additional research is needed to ascertain the role of diverse representation on bystander attitudes and behaviours, and the unique experiences of WI and WB across employee groups. Further to this, the participants’ job roles require them to interact with employees from other units, essentially placing them in different micro-cultures of civility following the training where they likely encountered varying levels of WI and WB, and barriers to bystander intervention (Baldwin & Ford, 1998). Given these constraints, and in line with the qualitative remarks urging senior leadership participation in, and support for, bystander intervention training, we contend that large organisations should roll out bystander training across units and involve senior leaders in the first instance to ensure alignment.
As a final note, the bystander intervention training and evaluation surveys were conducted during the Covid-19 pandemic, which has been particularly straining on healthcare professionals. Further to the greater incidence of negative acts and decline in helping behaviours that characterise high stress work environments (Penney & Spector, 2005), pandemic constraints may explain the significant participation dropout across the surveys, along with unchanged frequency of negative acts at work despite the positive reactions to training and intent to intervene as a bystander. Moreover, while the participants remarked on training’s relevance and usefulness, which are important conditions for transfer (Eid & Quinn, 2017), their engagement with the evaluation surveys may have been deemed a low priority relative to the ongoing pandemic challenges.
Conclusion
This study evaluated a bystander intervention training program by assessing changes to healthcare workers’ sense of psychological safety, bystander efficacy, perceptions of negative acts, and bystander intentions and behaviours over time. The findings from this study extend the research on bystander intervention and interpersonal violence at work. Specifically, the results suggest that while well-delivered training prompts positive attitudes and beliefs about bystander intervention and can motivate workers to foster a civility culture, bystander training effectiveness is contingent on visible leadership support and organisation-wide changes to its culture, practices, and accountability systems. The notion that context can act as a barrier to, or an enabler of bystander training effectiveness has been echoed in recent research (e.g. Kania & Cale, 2021; Shea et al., 2021; Thompson et al., 2020; Van Erp et al., 2018). Our study supports these assertions and indicates that bystander training reactions and effectiveness are contingent on the extent to which leaders are involved in the training and role model civility in the organisation, information about incivility, bullying and bystander intervention strategies is available, and participants have opportunities to practice bystander behaviours with appropriate support.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.