
Abstract
Intimate partner violence (IPV) adversely affects female reproductive health in various ways. Similarly, it plays a critical role in women’s unintended pregnancy. This study examines the relationship between IPV and unintended pregnancy in Eastern Sub-Saharan Africa (SSA) countries. This study uses data from the nationally representative Demographic and Health Surveys (DHS) in six Eastern African SSA countries. The original sample size was restricted to ever married (or cohabitating) women of reproductive age who completed the survey’s Domestic Violence Module and had a pregnancy in the previous 5 years. Svyset proportion was used to estimate the prevalence and 95% confidence intervals (CI) of the study outcomes and multiple logistic regression was used to compare outcomes of last pregnancy by exposure to lifetime IPV committed by the most recent partner. The prevalence of unintended pregnancy in Eastern SSA was 38% [36.4, 40.34] among married women with high disparity among countries. This prevalence was 45% [42.05, 48.15] and 55% [50.0, 59.87] among women who had experienced any form of IPV and sexual violence, respectively. After adjusting for potential confounding factors, women with a history of sexual violence had a higher risk of unintended pregnancy [AOR: 1.80, 95% CI: 1.39, 2.33] and increased odds of unintended pregnancy for women who had more than five living children [AOR: 4.93, 95% CI: 3.40, 7.15], women who lived in rural residences [AOR: 1.42, 95% CI: 1.07, 1.90], and women who reported they had financial barriers for health care [AOR: 1.36, 95% CI: 1.13, 1.64]. Our findings suggest that IPV, particularly sexual violence, is a key player for higher risk of unintended pregnancy in Eastern SSA countries. This study highlights the need for developing programs and implementation of policies that integrate sexual reproductive health and IPV to reduce unintended pregnancy among married and single women.
Keywords
Introduction
Worldwide, one in three women have experienced gender-based violence (GBV) (WHO, 2013). GBV has been declared a universal public health problem across all contexts, but the distribution differs (Abrahams et al., 2006). GBV includes either/or physical, mental, and sexual health morbidities and increased risk of death, with more than a third of homicides of women attributable to male partners (Stöckl et al., 2013; USAID et al., 2010). GBV is defined as “any act of GBV that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion, or arbitrary deprivation of liberty, whether occurring in public or in private life” (USAID et al., 2010). GBV can be defined depending on the relationship between the perpetrator and victim known as intimate partner violence (IPV) and non-IPV, or by type of the act, such as sexual, physical, or emotional violence (USAID et al., 2010).
The private nature of IPV has made it difficult to quantify its prevalence, understand its associated factors, or address its consequences (Muluneh et al., 2020; WHO, 2013; Yaya & Ghose, 2019). IPV is the most common form of GBV, accounting for 75% to 85% of GBV globally and affects millions of women throughout the world each year (WHO, 2012). Evidence has shown that IPV is most prevalent in resource-limited countries such as Sub-Saharan African (SSA) countries, with wide-ranging disparity in countries (Muluneh et al., 2020). A systematic review conducted in 2020 in SSA countries reported that the infliction of IPV is as high as 44%, which is higher than the global burden of 30% of IPV (Muluneh et al., 2020; WHO, 2013). The same study showed in the sub region analyses that Eastern Africa (42%) including Ethiopia and Uganda were the most affected by all forms of IPV, followed by Western Africa (41.7%) (Muluneh et al., 2020).
The factors associated with IPV in developing countries is attributed to multiple factors (Muluneh et al., 2021a, 2021b; WHO, 2013). Studies showed that the complex interplay between individual, relationship, community, and societal factors increase the chance of IPV among women. Evidence showed that predictors that increase the experiences of IPV include women and men with lower levels of education, increased levels of alcohol consumption by the woman and/or her partner, women with limited decision-making skills, women with a previous history of child abuse, women who have experienced depression, individual and community tolerant attitudes to IPV, unemployed women, low socioeconomic status, and limited food security (Ahinkorah et al., 2020; Muluneh et al., 2021a, 2021b; WHO, 2013).
The effects of IPV range from the individual level to a macro level and harbor socioeconomic and reproductive health impacts (WHO, 2013; World Bank, 2019). However, the effects of IPV are most pronounced in developing countries due to the limited efforts in preventing and rehabilitating women who have experienced IPV (Pallitto et al., 2006; Stöckl et al., 2013). The effect of IPV on women’s health ranges from minor injuries to serious physical, mental, and reproductive health problems and even death (Hindin et al., 2008; Vos et al., 2006). Moreover, victims of IPV are at a higher risk of unwanted and mistimed pregnancies (Lukasse et al., 2015).
Unintended pregnancies occur when no children are wanted and/or are mistimed (when they are not expected) (CDC, 2021). Unintended pregnancies are a universal challenge; 99.1 million unintended pregnancies are reported per year globally, of which one in five (21.6 million) were in Africa (Bearak et al., 2018). Eastern African countries alone account for the biggest prevalence of unintended pregnancies, to the extent of 8.85 million unintended pregnancies per year (CDC, 2021; Purgato et al., 2018). Worldwide, an estimated 44% of pregnancies were unintended in 2010 to 2014 (Bearak et al., 2018). Overall, unintended pregnancy was highest (38%) among women in Eastern SSA countries in comparison to women in SSA (26%) (Ahinkorah et al., 2020). This prevalence of unintended pregnancy in Eastern SSA countries is one of the highest in comparison to studies conducted in many other low and middle-income countries outside of SSA countries, including Bangladesh (30%) (Bishwajit et al., 2017) and Nepal (24.6%) (Acharya et al., 2019). This high prevalence of unintended pregnancies is associated with various sociodemographic and sociocultural situations and many other related factors (CDC, 2021; Lukasse et al., 2015; Purgato et al., 2018). This included not using contraceptives or inconsistent use of contraceptives, lower awareness, low decision making, violence from the husband, and refusal of family planning (FP) measures (Acharya et al., 2019; Ahinkorah et al., 2020; Lukasse et al., 2015; Muluneh et al., 2021a; Purgato et al., 2018). Hence, it is important to address systemic changes that involves dissemination of knowledge and education to all areas of communities and to establish government policy that enables greater access to FP services in rural areas.
Thus, it is important to consider unintended pregnancy as a public health issue in Eastern SSA countries (Ahinkorah et al., 2020; WHO, 2013). Recent literature has demonstrated that individual circumstances including socio-demographic factors such as maternal age, level of education of the mother, religion, marital status, parity, termination of pregnancies, and less knowledge of FP methods; household factors including household size, income/wealth status; community factors such as distance from the nearest health facility, residence, and region; are all the main factors associated with unintended pregnancy (Ahinkorah et al., 2020; Ba et al., 2019; Blackstone et al., 2017; Lukasse et al., 2015; Tiruye et al., 2020a, 2020b). Moreover, unintended pregnancies can result from contraceptive failure, not using contraceptives, and/or rape (Tiruye et al., 2020a, 2020b). Hence, it is essential to identify those at risk for unintended pregnancies and provide the services they require to ensure that those women and their families have safe options to consider when faced with unintended pregnancy (Lukasse et al., 2015).
The existing literature has shown the nexus between poor knowledge of reproductive health including low awareness in FP methods and poor reproductive health outcomes such as unintended pregnancy and abortion among young people, mostly in developing countries such as in SSA (Chung et al., 2018; Sarkar et al., 2015). Additionally, reproductive health predictors such as having a first sexual intercourse experience at age 16 or younger, not using contraceptives with a first sexual intercourse experience associated with IPV, harmful health behaviors (i.e., drug use, current smoking), and depression have been found to be positively correlated with unplanned pregnancies (CDC, 2021; Lukasse et al., 2015; Purgato et al., 2018).
Evidence has shown that pregnancy intention is a critical step in the course of maternal and child health outcomes (Ameyaw et al., 2019; Purgato et al., 2018). Unintended pregnancy may affect the behaviors of parenting and the critical support in development of the children (Purgato et al., 2018). Additionally, it is reported that women with no intention of a pregnancy tend to develop unhealthy behaviors such as consuming alcohol, smoking, unnecessary intake of medications, and are less likely to attend antenatal care following pregnancy (Ameyaw et al., 2019; Michau et al., 2015).
Research indicates that IPV is associated with adverse sexual and reproductive health outcomes, including unintended pregnancies (Pallitto et al., 2006). Studies showed that women who had an experience of IPV are at higher risk of not using contraceptives for many reasons possibly due to women being unable to have access to contraceptives and/or health services, and/or living in remote areas, and/or under coercive control (Ameyaw et al., 2019). However, the relationship between IPV and women’s ability to control their fertility including unintended pregnancy (i.e., mistimed or unwanted), has not been adequately explored, especially among women in developing countries, where both unintended pregnancy and IPV are prevalent (Ameyaw et al., 2019; Muluneh et al., 2020; Yakubu & Salisu, 2018). Hence, it is important to understand the relationship between unintended pregnancy and IPV in SSA countries, particularly Eastern African countries. Therefore, this paper aims to answer the following research question: Are women, in SSA countries, who have experienced IPV (physical, sexual, or emotional), more likely to have an unintended pregnancy than women who have not experienced violence from their partners? What are the other factors that increase unintended pregnancy in Eastern SSA countries that need to be considered in women’s health and IPV?
Methodology
Data Source
This study used a pooled data set from the Demographic and Health Surveys (DHS) of six Eastern SSA countries among 33,640 women who were married or living together with their partners (see Table 2 country data). The countries included Burundi (2017), Ethiopia (2016), Kenya (2014), Rwanda (2015), Tanzania (2016), and Uganda (2016) (USAID, 2019). The DHS is a nationally representative survey that is conducted in over 90 low- and middle-income countries globally (USAID, 2019). The DHS surveys used a two-staged stratified cluster sampling technique which makes the survey data nationally representative. An enumeration area (EA) is a specific area in a country, which is generated as the sampling frame. The EAs are mostly generated based on the most recent national census data in the country. In the first stage, urban and rural enumeration sites were selected with probability proportional to EA size and with independent selection in each sampling stratum. In the second stage of selection, a fixed number of households per cluster were selected with an equal probability systematic selection from the newly created household listing. In most instances, the number of selected households per EA ranged from 30 to 40 households/women per rural cluster and from 20 to 25 households/women per urban cluster. The DHS survey population included all women aged 15 to 49 years of age and all men aged 15 to 59 years of age who were either permanent residents of the selected households or eligible visitors (USAID, 2019). Women who were interviewed about their experiences of domestic violence were the main focus of this study.
Outcome Variables
Unwanted pregnancy was a dependent variable for this study. The DHS surveys on an unintended pregnancy or pregnancy intention were defined as a pregnancy in the past 5 years to when they were last pregnant. It was described as a pregnancy wanted then (intended), later/mistimed (i.e., the pregnancy was wanted but occurred earlier [within 2 years] than expected), not wanted at all/unwanted (USAID, 2019). As such, the pregnancy intention of respondents was categorized as unintended or intended. Women responding that their last pregnancy was “wanted later/mistimed” or “not wanted at all/unwanted” were characterized to have an unintended pregnancy, and those who responded “wanted pregnancy then” were considered to have an intended pregnancy. Unintended pregnancy was coded “1” and intended pregnancy coded “0.”
Explanatory Variables
Experiences of IPV were the main variables for the analysis. IPV was measured by the experience of at least one or more forms of violence such as physical, sexual, or emotional violence. The following were the key questions used to measure IPV in the DHS (USAID, 2019). Physical violence includes seven items whilst emotional and sexual violence includes three questions for each. All the questions were categorical with responses of yes or no. Women were asked whether they had experienced acts of violence within their relationship, perpetrated by their husband/partner. The below questions were categorized as experiencing any violence in their lifetime.
I. Physical violence experience questions included: (1) push you, shake you, or throw something at you? (2) slap you? (3) twist your arm or pull your hair? (4) punch you with his/her fist or with something that could hurt you? (5) kick you, drag you, or beat you up? (6) try to choke you or burn you on purpose? (7) threaten or attack you with a knife, gun, or any other weapon?
II. Sexual violence experience questions included: (1) physically force you to have sexual intercourse with him even when you did not want to? (2) physically force you to perform any other sexual acts you did not want to? (3) force you with threats or in any other way to perform sexual acts you did not want to?
III. Emotional violence experience questions included: (1) say or do something to humiliate you in front of others? (2) threaten to hurt or harm you or someone close to you? (3) insult you or make you feel bad about yourself?
In addition, potential confounding factors related to women (such as age, education, working status, knowledge of FP, occupation, religion, drinking habit), partner’s characteristics (such as age, education, controlling behavior, consumption of alcohol, physical violence, working status), household factors (such as wealth, access to information, and health facility access), and place of residence and other factors that were identified from the literature review (Abrahams et al., 2006; CSA Ethiopia and ICF, 2016; WHO, 2013) were also included in the analysis.
Analysis
All analyses were performed using “SVY” commands in STATA version 16.0 (StataCorp, 2015), which allowed for adjustments for sampling weights in the cluster sampling design. Bivariate and multiple logistic regression analyses were performed. Bivariate analyses were used to check the associations between IPV and unwanted pregnancies and other associated factors. Only factors that were significant in the bivariate analysis were moved to multiple regression analysis. This was followed by conducting multiple logistic regression analysis, a five-stage hierarchical logistic regression that adjusted for clustering and sampling weights. According to this procedure, the effect of distal variables could be determined without incorrect adjustment by other variables that could be mediators of the association of more distal variables (Victora et al., 1997).
In the first stage (Model 1), physical violence, sexual violence, and emotional violence factors were examined. In the second-stage model (Model 2), Model 1 was added to women’s demographic circumstances to examine factors associated with unwanted pregnancy. Similar statistical procedures conducted in Model 2 were carried out in Model 3 and Model 4 that were partners’ factors and household factors/community and barriers to health care factors, respectively, to determine factors associated with unwanted pregnancies. The final model (Model 5) includes the explanatory variables and potential confounding factors (as described in Table 1 for details). The odds ratios and their 95% CI’s were obtained from the adjusted multiple logistics model. The aim of this modeling strategy reported in this paper was to allow a comparison of the influence of each of the different sets of potential confounding factors on the relationship between IPV and unintended pregnancy.
Potential Covariates Used for Hierarchical Survey Logistic Regression Model 1 to 5.
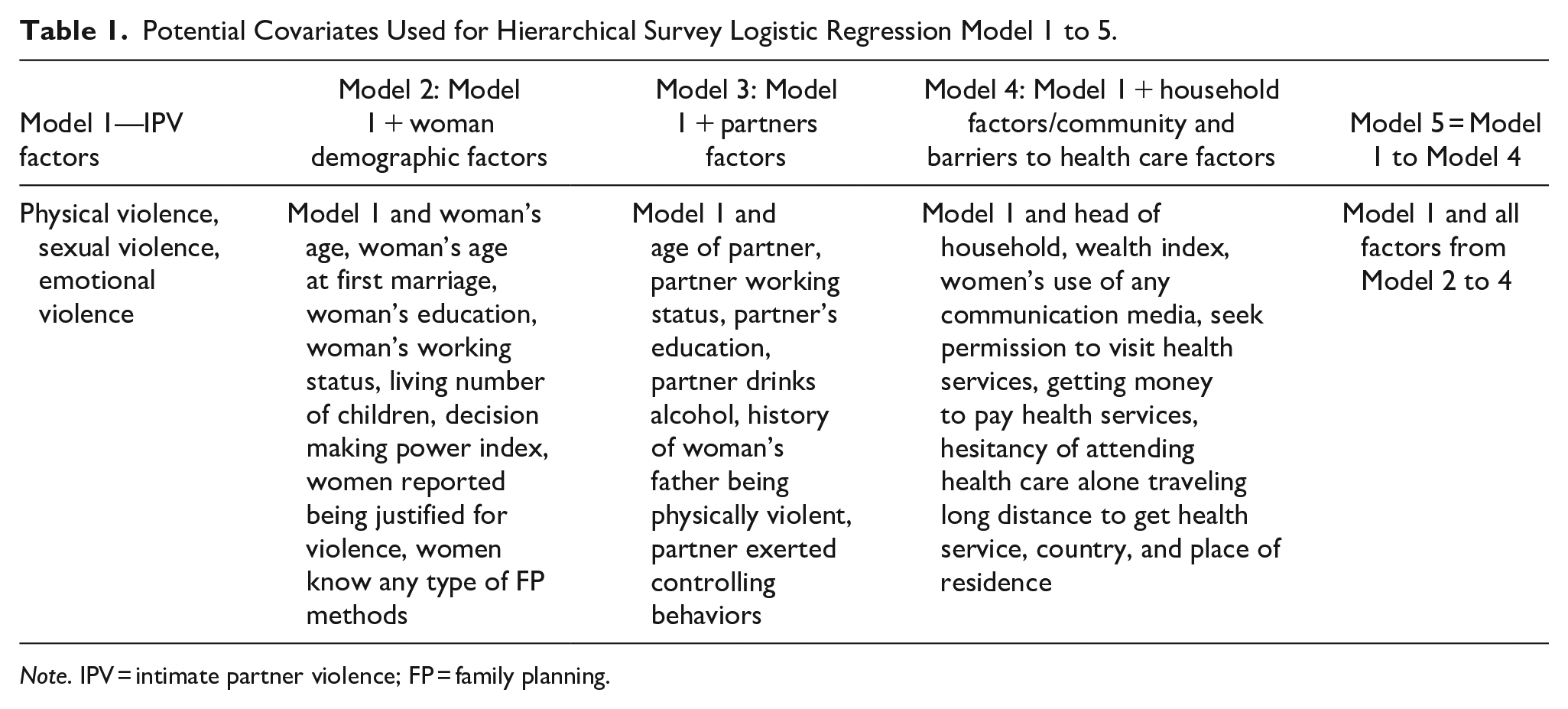
Note. IPV = intimate partner violence; FP = family planning.
Ethical Statement
The research design, including the content of all the survey questionnaires of the domestic violence in DHS, was reviewed by the United States Department of Health and Human Services’ regulations and approved by both the ICF Institutional Review Board and Eastern Sub-Saharan African countries’ Review Boards. We obtained approval from Measure DHS to download and use these datasets for this study. All methods (use of data) were performed in compliance with the Declarations of Helsinki. In the datasets used in our study, all identifier information was removed, and no personal identity was compromised.
Results
Descriptive Results
Figure 1 depicts the prevalence of unintended pregnancies in Eastern SSA; the results revealed that 38% [36.4, 40.34] of the pregnancies were unintended pregnancies. The unintended pregnancies were reported highest (44%) in Uganda followed by Burundi (42%) and lowest in Ethiopia (30%).
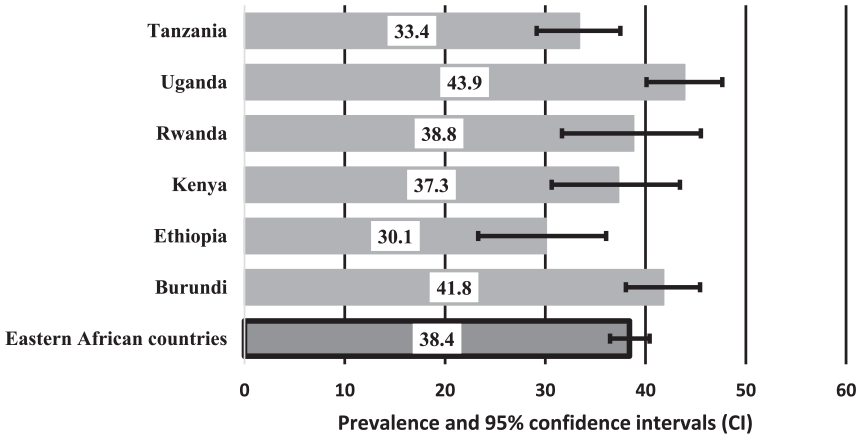
Prevalence and 95% confidence intervals of unintended pregnancy in Eastern Sub-Saharan African countries.
The Prevalence and 95% CI of IPV (Physical, Sexual, or Emotional Violence)
In Eastern SSA, almost half (48%) of women have experienced at least one form of IPV from their partners. The prevalence varies by country, where Uganda (56%) and Burundi (50%) and Tanzania (49.5%) were the top three countries with the highest proportion of women who reported IPV. By type of violence, physical violence (36.5%) was the most frequently reported, followed by emotional violence (32%), while sexual violence was the least reported (17.5%) type of violence. The highest prevalence of sexual violence was reported in Burundi (25.4%) and Uganda (23%) among married women of reproductive age. Ugandan women experienced the highest emotional violence (41%) followed by Tanzanian women (36%) (see Figure 2).
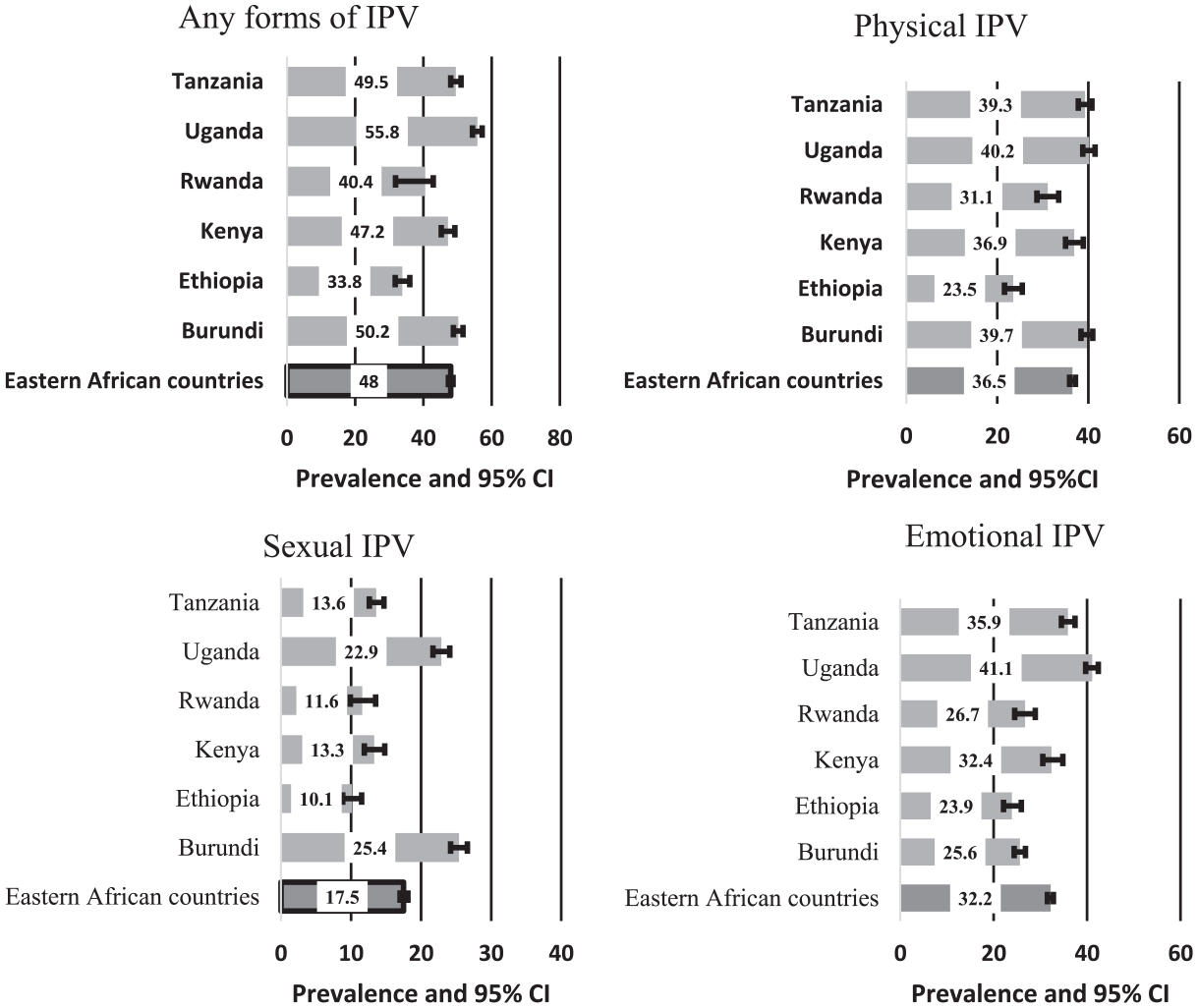
Prevalence and 95% confidence intervals of intimate partner violence (IPV) (any forms of IPV, physical, sexual, or emotional form of IPV).
The Association Between Unintended Pregnancies and Various Variables
The study analyzed a weighted sample of 30,715 married or cohabiting women in six Eastern SSA countries. Table 2 presents the different characteristics of variables weighted and unweighted frequencies.
The Study Population Characteristics, Prevalence, and Unadjusted Odds Ratios (UOR) and Their 95% Confidence Intervals (CIs) of Unintended Pregnancy, N* = 30,715.
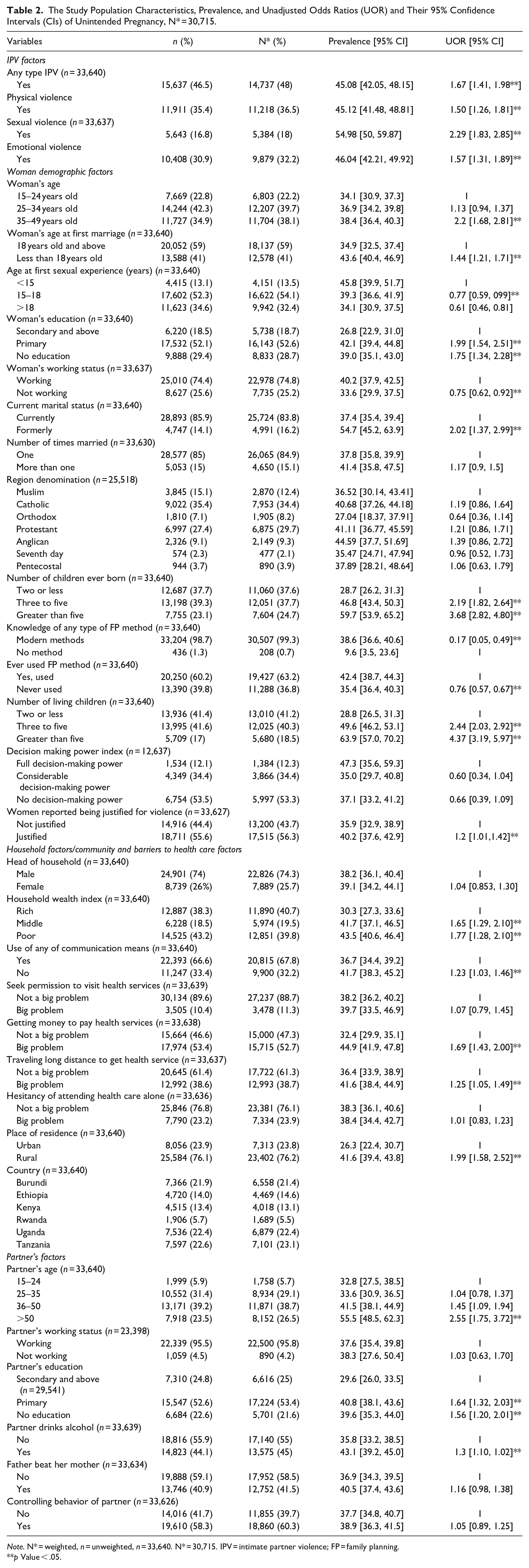
Note. N* = weighted, n = unweighted, n = 33,640. N* = 30,715. IPV = intimate partner violence; FP = family planning.
p Value < .05.
Table 2 shows the relationships of various women and household characteristics with unintended pregnancy in Eastern SSA countries. The results have revealed that unintended pregnancy is associated with various forms of IPV. The highest prevalence of unintended pregnancy was found amongst women that experienced sexual violence 55% [50, 59.87] in comparison to women who had no experiences of sexual violence (p < .001). Additionally, unintended pregnancies were positively associated with increased age of women, increased age at marriage, and younger age of first sexual intercourse experience, working women, women with lower rates of literacy, and larger number of current living children (p < .001). Moreover, higher prevalence of unintended pregnancy was associated with household characteristics including lower wealth index (p < .001), no access to any means of communication medias, and amongst women who justify physical violence against the wife (p < .05). For instance, the prevalence of unintended pregnancy differs depending on the number of women’s living children. The proportion of unintended pregnancies amongst women who have five or above children was higher by 35% in comparison to women who have up to two children. Similarly, unintended pregnancy was highly prevalent amongst women in a poor wealth category in comparison with a wealthy family. In contrast, based on this study, being married more than once, being of any religious denomination, being male or female head of household and decision-making status were some of the factors that were not associated with unintended pregnancy.
The prevalence of unintended pregnancy varied depending on the partner’s socioeconomic status and access to health care. Unintended pregnancy occurred most often amongst women who have illiterate partners, women whose partners were older and drank alcohol (p < .001). Similarly, unintended pregnancy was highly prevalent amongst women who have barriers to access health care due to long distances to travel and lack of money for treatment. Moreover, women who reside in rural residences had a 15% higher chance of an unintended pregnancy in comparison to women residing in an urban residence in Eastern SSA countries (see Table 3).
Multiple Logistic Regression Analysis of Adjusted Odds Ratio (AOR) of Intimate Partner Violence (IPV), for Individual, Household, and Partner’s Variables and Associated Factors of Unintended Pregnancy Amongst Married Women of 15 to 49 years of Age in East Africa Countries.
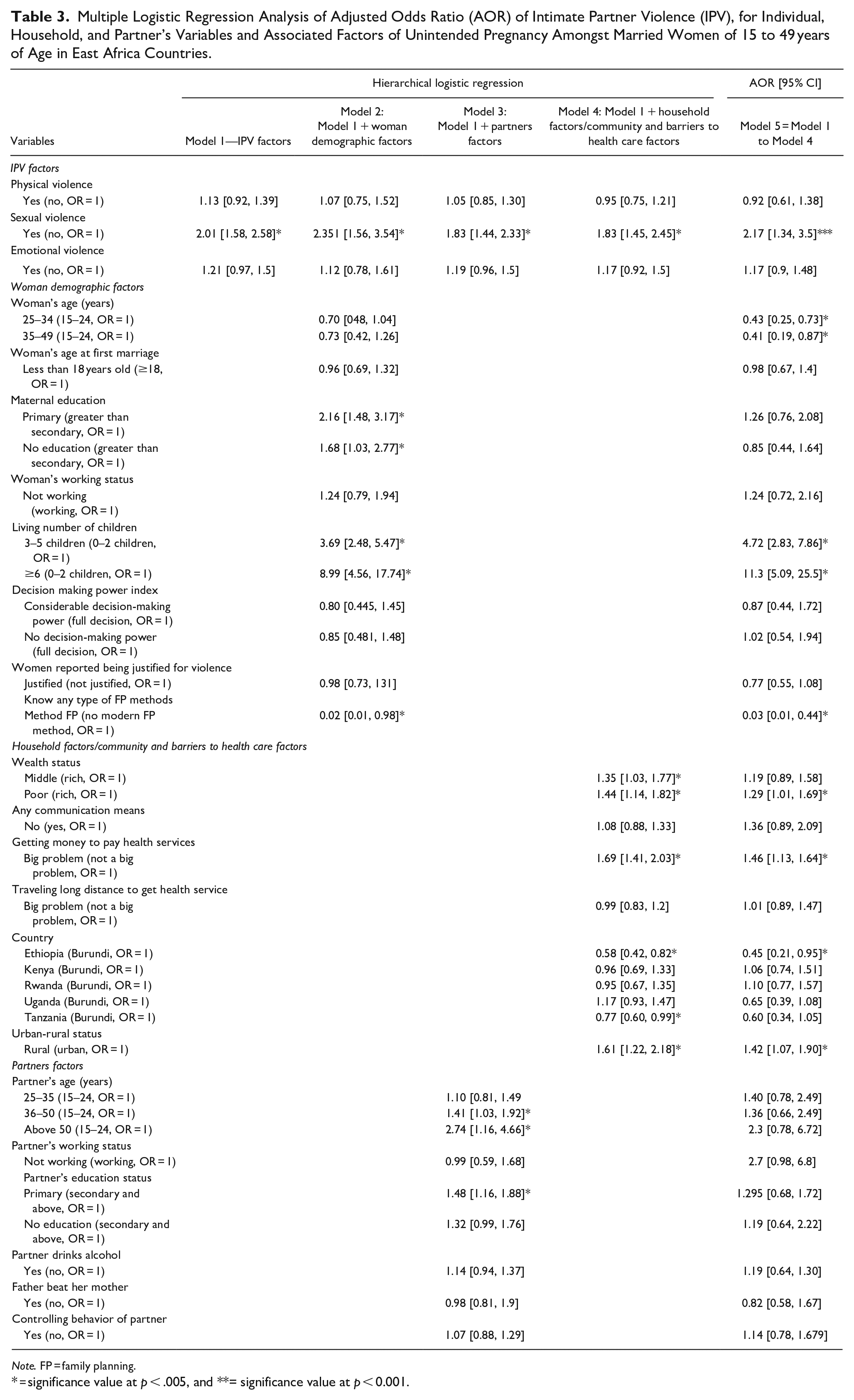
Note. FP = family planning.
= significance value at p < .005, and **= significance value at p < 0.001.
Multiple Logistic Regression Results
Table 3 shows the analysis of multiple logistic regressions, showing unintended pregnancy increased amongst women who experienced sexual violence, those who had greater than five living children, those who did not know usage of FP methods, women who lived in rural residences, and women less wealthy with restricted access to health care (p < .001). For instance, women who experienced sexual violence were two times more likely [AOR: 2.17, 95% CI: 1.34, 3.5] to have an unwanted pregnancy in comparison to those who had never experienced sexual violence (p < .001). Similarly, the chance of unintended pregnancy was four [AOR: 4.72, 95% CI: 2.73, 7.86] and 11 times [AOR: 11.3, 95% CI: 5.09, 25.5] among women who had three to five and more than or equal to six living children, respectively in comparison to women who had up to two living children (p < .001). In addition, women who lived in rural residences had a higher chance of unintended pregnancy than women residing in urban residences in Eastern SSA countries.
Discussion
This study showed there was a strong relationship between violence against women and unintended pregnancy. The analysis showed the risk of unintended pregnancy increased amongst women who had an experience of IPV, with as high as 45% of women having an unintended pregnancy. Most interestingly, the highest proportion of unintended pregnancy (55%) was reported amongst women facing sexual violence. Overall, irrespective of education, economic status, employment, access to health care facilities, or any other partner’s factors, women with a history of sexual violence were twice as likely to have an unintended pregnancy in Eastern SSA. Similarly, the findings of other studies resonate with our results, showing that women who experienced violent sexual experiences had higher rates of unintended pregnancy (Acharya et al., 2019; Ahinkorah et al., 2020; Lukasse et al., 2015; Raihana et al., 2012; Zakar et al., 2016).
This unintended pregnancy and sexual violence may be related to many factors in Eastern SSA countries. Firstly, it may be related to male dominance, particularly in decision making about sexual practices and accessing health care, especially contraceptives (Acharya et al., 2019; Muluneh et al., 2021c; WHO, 2013). As a result, those women experiencing IPV tend to have less negotiation power with decisions about their fertility (Hasselmann & Reichenheim, 2006). One of the clear relationships is coercion by husbands to engage in unprotected sexual intercourse (Miller et al., 2014; Samankasikorn et al., 2019). Hence, abusive partners may dominate women economically and emotionally, which may reduce women’s inability to make decisions about their pregnancies (Hasselmann & Reichenheim, 2006; WHO, 2013). However, our results differ from this evidence and did not show a significant association between IPV and low decision-making and controlling behavior of the male partner. This example of women’s disempowerment may be due to low wealth index and lack of access to health services. Therefore, even though low decision-making and controlling behaviors were not significant in our study, the financial situation and economic disempowerment issues are indirectly related to these factors.
Secondly, SSA countries have a deep-rooted cultural system with patriarchal societies that are common and this directly or indirectly works to endorse a male-dominated social order and family structure, often resulting in men exercising power and control over women in several ways, as demonstrated by IPV (Hasselmann & Reichenheim, 2006). As a result, society reduces the chances for women to access contraceptives freely. Similarly, our study showed that controlling behaviors from a male partner within relationships are related to an unequal social balance between genders and diminish economic independence for women.
Thirdly, this high prevalence of unintended pregnancy among women who have experienced sexual violence may be related to women’s characteristics. Women living in Eastern SSA are less educated, have less knowledge about FP, and have reduced power status for various reasons including fear, stigma, and divorce and limited financial resources in comparison to their male partner (Miller et al., 2014; Samankasikorn et al., 2019). This is an example of structural sexism and gender inequality that prevents women having the same opportunities as their male counterparts. For women, physical health problems are associated with greater exposure to structural sexism which aligns with logical expectations given their disadvantaged social position (Homan, 2019). These women are less likely to seek help at health facilities for usage of contraceptives (Blackstone et al., 2017; Yaya & Ghose, 2019). This increases the risk of unintended pregnancy as reported in various studies (Miller et al., 2014; Samankasikorn et al., 2019). Lastly, in these regions, health care services, including FP and counseling, are scarce and relatively inaccessible for women.
In most Eastern SSA countries such as Ethiopia, contraceptives are freely available in most public health facilities (Tiruye et al., 2020c; WHO, 2013). Even so, this study found that other factors associated with unintended pregnancy were higher among women who have five or more living children, those who had less knowledge of FP methods, women who lived in rural residences, and women who had financial constraints for treatment of health care (p < .001). For example, women who have a large number of living children had a higher risk of unintended pregnancies than women with fewer children. One possible justification is that women who already have numerous children have never used contraceptives due to a lack of knowledge about using contraceptives and financial constraints (Miller et al., 2014; WHO, 2013).
This study has shown the high disparity amongst women experiencing unintended pregnancy living in rural and urban areas. Women living in urban areas were less likely to be exposed to unintended pregnancy than women who lived in rural settings. This finding may be attributed to women residing in urban areas having greater accessibility to FP, and a better awareness about the benefits of FP to prevent unintended pregnancy. Moreover, legal practices and social protection are relatively better in urban settings in comparison to women living in a rural setting (WHO, 2013). The community acceptance for male dominance in urban settings is relatively lower in comparison to women in rural areas and women are more empowered in urban residences (Muluneh et al., 2021a, 2021b; UNICEF, 2015), subsequently contributing to the reduction of unintended pregnancies. This finding is consistent with a study conducted in India that demonstrated a higher experience of unintended pregnancy was found among women living in rural India in comparison to women living in urban settings (Sarder et al., 2021). Similarly, a study conducted in Ethiopia showed women in rural settings experienced higher unintended pregnancies (Tiruye et al., 2020a).
In summary, it is important to consider and to distinguish that widespread education is primarily targeted to individuals through various education systems such as school and program levels, when greater structural changes (such as increased access to FP in rural areas, education systems at the regional level, human resources arrangements for responses to gender equality) may be more effective in eradicating and reducing IPV. Addressing all these levels will promote the education of equity. In addition, the education system needs to be strongly integrated with the social fabric of the legal system. Educating the legal system needs to be supported by the legal enforcement system. Moreover, most Eastern African countries contain many laws in place at all levels of the legal system that guarantee equal rights and prohibit most forms of GBV, including female genital mutilation, child marriage, most forms of rape, and some IPV. However, for many reasons, including the often-discordant levels of the formal and informal legal systems, the general culture of acceptance of IPV, the poor training of law enforcers and judges, and the lack of institutional support behind the enforcement of the law and the policies are widely ineffective at preventing this violence against women (van Eerdewijk et al., 2018).
Strength and Limitations of the Study
This study’s strengths include using standard measurement tools from DHS measures and large data sets from six Eastern SSA countries to assess factors related to women experiencing unwanted pregnancies. It also used a rigorous analysis to identify the effects of IPV on unintended pregnancy. However, this study does not show any causality of effects due to its nature of being a cross-sectional design study. Additionally, this study is only limited to DHS questionnaires and lacks some characteristics related to refugees, internally displaced people, and people who have traveled from other parts of the country, where unwanted pregnancies may be underreported.
Conclusion and Implications
In conclusion, this study provides a strong relationship on the impact of IPV on unintended pregnancy. It is central to understanding the burden of IPV in Eastern SSA countries and closing the gaps in reducing unintended pregnancies amongst women who are married or in a relationship/union. Hence, sexual violence is a key factor for the increased prevalence of unintended pregnancy in Eastern SSA countries. Therefore, it is critical to reduce the occurrences of IPV to reduce unintended pregnancies, mistimed, or unwanted pregnancies. Additionally, unintended pregnancies are strongly related to the larger number of living children, lower knowledge of FP and financial barriers and rural residence. Therefore, this study informs policies and interventions to address these target groups of the population. To reduce unwanted pregnancy, it is important to provide public health and human rights approaches to scale up prevention of unwanted pregnancy and sexual violence. This includes strengthening relationship skills such as comprehensive sexual education among partners, empowering women, enhancing health service access including FP, and encouraging women to use contraceptives. In addition, widespread education to transform attitudes, beliefs, and norms in the community to reduce unintended pregnancy is urgently needed. In addition, male engagement is an important key means to address IPV and reduce male dominance. Moreover, enhancing FP accessibility and usability, particularly in rural communities will be important to reduce unintended pregnancies. As evidenced in the literature, there are legislative and policy frameworks that exist to address violence against women. However, there are substantial gaps in enforcement of the policy translation, policy literacy, and its enforcement that might limit capacity and implementation of local legal structures. Engaging various stakeholders including the government in SSA countries is key to addressing women experiencing unwanted pregnancies in IPV relationships.
In accordance with the findings, interventions that seek to enact sustainable change should target the root causes of IPV, including power inequalities, and involve all communities including men, women, and adolescents. According to various reviews, there is a limited number of GBV programs (McCrory & McNally, 2013), hence there is a need for more programs to address gender inequality, women’s empowerment, and social norms with interventions targeted at both men and women. Hence, future research needs to focus on analyzing the policy framework and practice at various levels and how IPV is understood, practised, and resisted in local contexts and program responses. Interventions should focus on integrating, mainstreaming, and coordinating for various sector offices in SSA countries to ensure national data systems are able to document and monitor patterns of IPV and prevention of violence against women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.