
Abstract
Homelessness is a public health crisis both nationally, in the United States, and internationally. Nevertheless, due to the hidden vulnerabilities of persons who are without shelter, little is known about their experiences during periods of homelessness. The present research adopts a network approach that conceptualizes how the major risk factors of homelessness interact, namely substance abuse problems, poor mental health, disability, and exposure to physical or sexual violence by an intimate partner. Our analysis draws on a large demographic survey of over 5,000 unsheltered homeless persons conducted in 2017 by the Los Angeles Homeless Services Authority. We estimated a network structure for 12 survey items tapping individual risk using the graphical least absolute shrinkage and selection operator algorithm. We then examined network centrality metrics and implemented a community detection algorithm to detect communities in the network. Our results indicated that mental illness and intimate partner violence (IPV) are central measures that connect all other mental and physical health variables together and that post-traumatic stress disorder and IPV are both highly affected by changes in any part of the network and, in turn, affect changes in other parts of the network. A community detection analysis derived four communities characterized by disability, sexual victimization and health, substance use, and mental health issues. Finally, a directed acyclic graph revealed that drug abuse and physical disability were key drivers of the overall system. We conclude with a discussion of the major implications of our findings and suggest how our results might inform programs aimed at homelessness prevention and intervention.
Keywords
Introduction
A large body of research has focused on the negative life outcomes of homelessness; however, less research has explored the interrelationships among co-occurring risk factors that are likely to perpetuate it. Existing studies focus largely on the structural conditions related to homelessness such as poverty (Ji, 2006), housing shortages and insecurity (Clark et al., 2018; Rollings et al., 2017), unemployment (Burke et al., 2013), and forms of institutional racism and discrimination that prevent upward mobility (Schneider, 2020). Individual factors that may also increase one’s vulnerability to homelessness in complex and interrelated ways have received less attention (Tessler et al., 2001). Moreover, studies that do exist tend to explore interpersonal characteristics related to homelessness such as substance use, mental illness (MI), and physical and/or sexual abuse as discrete and independent factors (Wasil et al., 2020) or as being caused by some underlying latent variable (Barile et al., 2018; Yoder et al., 2008).
Research has demonstrated that the link between homelessness and certain causes and consequences thereof are stronger for men or women conditioned, in part, by gender role socialization. A recent scoping review of the literature concluded that homeless women experience a range of adversities throughout their lives that frequently begin during childhood. Whereas stressful life events contribute to vulnerability to homelessness for both men and women, the number and types of stressful life events experienced by men and women are vastly different. For example, a study conducted by Tessler et al. (2001) found that loss of a job, discharge from an institution, mental health problems, and drug or alcohol problems were contributing factors for homelessness among men. In contradistinction, women reported eviction, interpersonal conflict, and loss of dependency as constituting the main reasons for their perceived pathway into homelessness. A more recent study of 293 men and women experiencing homelessness in Madrid, Spain found that women experiencing homelessness had histories of sexual violence in childhood, sexual abuse in adulthood, and abuse by a spouse or partner whereas men experiencing homelessness were more likely to have indulged in alcohol abuse (AA) and be implicated in the criminal justice system (Rodriguez-Morreno et al., 2021). This conclusion has been supported by other studies such as the one conducted. This body of work suggests that the causal mechanisms underlying homelessness may be different for men and women justifying the need to compare the network structure of homelessness by gender.
These analytical frameworks assume conditional independence between variables once the underlying causal factor (e.g., lack of income) is taken into consideration (Wasil et al., 2020). This assumption is questionable, however. Rather, risk factors associated with being unsheltered—violence exposure, substance abuse, and behavioral health—may be better conceptualized as being constitutive of homelessness rather than a cause or consequence of it (Blanchard et al., 2021; Borsboom & Cramer, 2013; Cramer et al., 2010; Jones et al., 2018). As such, network theory offers a novel methodological approach that may better capture the complexity of homelessness and elucidate the interrelationships undergirding the experiences of homeless persons while simultaneously suggesting directions for effective intervention and prevention.
In this paper, we present a novel network analysis that is uniquely suited to model the complexities of homelessness using a large-scale representative survey conducted in Los Angeles County. Our analysis results in a dynamical system of the multiple characteristics of homelessness including mental health, physical disability (PD), and victimization experiences. When analyzed in conjunction with a directed acyclic graph (DAG), potentially causal mechanisms between the predominant factors of homelessness can reveal patterns describing the underlying relationships between homelessness experiences that may otherwise go undetected. Moreover, a network approach can identify the direction and magnitude of the linkages between different variables and highlight those that are highly central and connected, or not, to the overall network. For example, network theory provides a more nuanced analysis of the multiple, overlapping adverse life events that are commonly experienced by individuals who are homeless, such as intimate partner violence (IPV) and sex trafficking, and how these experiences overlap with other aspects of behavioral health. Further, a network approach will reveal which of several adversities activate other negative experiences captured by the network which may result in the repetitive and ongoing cycle of homelessness for some individuals (Jones et al., 2018; Robinson, 2003). To the best of our knowledge, no study to date has investigated the network structure of multiple co-occurring life stressors and psychopathology in a representative sample of homeless people from a large urban county. Accordingly, this paper aims to (1) estimate, analyze, and assess the network structure of 12 characteristics of homelessness measuring victimization by an intimate partner, substance use disorder, poor mental health, PD, and injury—all of which have been previously identified as either causes or consequences of homelessness; and (2) investigate whether the network structure of those characteristics is invariant (i.e., similar) across genders.
Definition and Prevalence of Homelessness
Homelessness constitutes a major public health crisis in the United States (Donovan & Shinseki, 2013). While definitions of homelessness vary, most federal agencies use the McKinney-Vento Act (P.L. 100-77) to define homelessness as, . . . an individual who lacks a fixed, regular, and adequate nighttime residence; and a person who has a nighttime residence that is (a) a supervised publicly or privately operated shelter designed to provide temporary living accommodations (including welfare hotels, congregate shelters, and transitional housing for the mentally ill); (b) an institution that provides a temporary residence for individuals intended to be institutionalized; or (c) a public or private place not designed for, nor ordinarily used as, a regular sleeping accommodation for human beings (42 U.S.C. § 11302).
While measures of homelessness are imprecise (Brush et al., 2016), an estimated 568,000 people in the United States experienced homelessness in 2019 (U.S. Department of Housing and Urban Development [HUD], 2020). This includes everything from short-term homelessness where someone may be homeless for a single day or short duration to chronic homelessness where they are living on the street or in shelters regularly (HUD, 2020). In Los Angeles County, where the present study was conducted, a reported 66,436 people experienced homelessness in 2020, representing a staggering 12.7% increase from 2019 (Los Angeles Homeless Services Authority [LAHSA], 2020b). The characteristics of unsheltered populations span every demographic, as homelessness crosses age, gender, sexuality, race, ethnicity, and geographic region of the country (National Alliance to End Homelessness, 2000). Yet, national reports tend to indicate a higher prevalence of homelessness among males, persons of color, veterans, and gender non-conforming and transgendered individuals (Kuhn et al., 2020; National Alliance to End Homelessness, 2000; Washington et al., 2010).
Vulnerabilities to Homelessness
Homeless individuals are particularly vulnerable to syndemic health threats due to sociopolitical environmental factors and multiple pathways of risk (Robinson et al., 2016) that exacerbate substance abuse, health problems, HIV risk, and mental health symptoms (Fitzpatrick-Lewis et al., 2011; Kertesz et al., 2009; Larimer et al., 2009). Homeless men and women have higher rates of violence exposure, both as perpetrators and victims, and more contact with the criminal justice system (Goodman et al., 1991; Greenberg & Rosenheck, 2008; Heerde & Hemphill, 2017, 2019; Wong et al., 2016). Homelessness is associated with prolonged gaps in health care access, which may result in unusually high rates of acute and intensive health care services, such as emergency room visits and hospitalizations (Baggett et al., 2010). Finally, homelessness is associated with mortality rates that are three times higher than individuals with some form of housing (McCary & O’Connell, 2005).
Physical or Sexual Abuse
Traumatic life events, particularly physical and sexual abuse (PS) have been documented both prior to and during homelessness. As noted above, while both men and women can experience physical and sexual victimization, they are reported at different rates by gender (Wenzel et al., 2000). Sexual assault, physical abuse, and childhood abuse have been significantly associated with homelessness, particularly among women (Brush et al., 2016; Frencher et al., 2010; Kennedy et al., 2010; Roschelle, 2017; Wenzel, Leake, et al., 2000; Wenzel et al., 2004). In Zugazaga’s (2004) study of homelessness in Central Florida, single homeless women were likely to report experiencing domestic violence (67%). Both single homeless women and homeless women with children were likely to report prior physical violence (46%) and sexual violence (46%) (Zugazaga, 2004). Not all violence occurs prior to homelessness as Stewart et al. (2004) found 83% of homeless youth experienced physical or sexual assault on the street. In addition to directly being the target of violence, in low-income urban areas, witnessing violence in the community may also not be uncommon (Roschelle, 2017). While unsheltered women have been found to experience both sexual assault and IPV at higher rates compared to men (D’Ercole & Struening, 1990; Horan & Beauregard, 2018; Hudson et al., 2010; Nyamathi et al., 2000), homeless men are more likely to report experience of physical violence (Hashima & Finkelhor, 1999; Stewart et al., 2004; Wenzel, Koegel, et al., 2000). Both directly experiencing violence and witnessing violence can increase substance use, MI (e.g., post-traumatic stress disorder [PTSD]), and homelessness (Monnat & Chandler, 2015; Roschelle, 2017; Turner et al., 2017). The negative effects of PS do not exist in a vacuum and intertwine with other vulnerabilities to homelessness such as MI and substance abuse.
Mental Illness and Physical Health Impairments
Individuals who experience homelessness are much more likely to suffer from serious MI (e.g., schizophrenia), chronic medical conditions (e.g., HIV/AIDS), and substance use disorders than the general population (Los Angeles County Department of Public Health [DPH], 2022; National Health Care for the Homeless Council, 2011). The presence of serious physical illness (PI) and severe MI in homeless populations has been estimated to be 3 to 4 times and 10 to 20 times higher compared to the general population, respectively (Susser et al., 1997). Such disorders can influence cognitive ability and result in lower levels of intellectual functioning, literacy, memory, concentration, and attention (Solliday-McRoy et al., 2004). Research suggests that individuals who are vulnerable to homelessness have experienced higher rates (reported up to 65%) of lifetime traumatic brain injury (TBI) (To et al., 2015; Topolovec-Vranic et al., 2012), compared to individuals in the general community (8.5%) (Silver et al., 2001). Previous research has shown as well that homeless people with a history of TBI have an increased risk for a host of adverse physical health outcomes including seizures, as well as mental health and substance abuse disorders (Hwang et al., 2008) and victimization (To et al., 2015; Topolovec-Vranic et al., 2014).
Physical injuries are also likely among homeless individuals. Compared to housed patients with low socioeconomic status, Frencher et al. (2010) reported high rates of unintentional injury among the homeless at a rate of 13% in children, 6% in adults, and 63% in elderly adults. They found homeless individuals to be twice as likely to experience vehicle injuries, burns, and three times as likely to be hospitalized for cold weather/exposure related injuries (Frencher et al., 2010). Not all injuries among this population are unintentional. Among homeless youth, suicide attempts are more common than in housed youth (Whitbeck et al., 2004).
Substance Abuse
Although studies vary, research consistently shows over a third of individuals who are homeless experience alcohol and drug problems (e.g., Gillis et al., 2010) and up to two-thirds have a lifetime history of an alcohol- or drug use disorder (Robertson et al., 1997). According to the U.S. Department of Housing and Urban Development [HUD] (2010), 34.7% of people who were homeless and in shelters chronically abused substances. A study by North et al. (2004) reported that 58% of chronically homeless single women and 84% of single men had a substance use disorder. When it comes to substance abuse, alcohol dependence has been found to be the most common substance use disorder followed by drug dependence (Fazel et al., 2008). For some, drug use may result in homelessness, yet for others homelessness may exacerbate addiction (Neale, 2001). Substance abuse often co-occurs with MI such as depression and anxiety (Ostacher, 2007). As the Substance Abuse and Mental Health Services Administration and Center for Substance Abuse Treatment (2011) reports, approximately 30% of people who are chronically homeless have at least one mental health condition and 50% have co-occurring substance abuse issues. The prevalence of co-occurring substance use and mental disorders in the United States is relatively high (Najt et al., 2011). Individuals with substance use and mental health disorders have been considered some of the most vulnerable to homelessness in our society (Padgett et al., 2011). Those homeless have been documented as having more severe substance use disorders and co-occurring mental health problems (Padgett et al., 2008). In turn, drug abuse (DA) and serious mental disorders are associated with violent victimization (Sells et al., 2003). Furthermore, research indicates that mental health and substance abuse within the homeless population is a contributing factor for incarceration (Greenberg & Rosenheck, 2008; Kushel et al., 2005) and higher use of crisis centers and hospitals (Larimer et al., 2009).
Applying New Analytical Techniques to Vulnerabilities With Homelessness
The above research clearly demonstrates that homeless individuals are at higher risk for a host of negative problems each of which can be either a cause or consequence of homelessness—DA and AA, HIV infection, other sexually transmissible diseases, incarceration, violence, and other problems. These findings are best contextualized by one of the most consistent findings on polyvictimization, namely that individuals, unsheltered and otherwise, who experience one type of adversity typically experience more than one (Anda et al., 2008, 2010; Barboza, 2018; Liu et al., 2020; Radcliff et al., 2019). Further, multiple compared to singular risk exposures lead to poor outcomes that accumulate across several domains including, but not limited to, health, housing, and employment (Anda et al., 2008, 2010; Hardcastle et al., 2018; Nobari & Whaley, 2021). For example, studies have consistently shown that mental health problems, violent physical and sexual victimization, substance use, and PI co-occur with homelessness as causes or consequences (Bearsley-Smith et al., 2008; Heerde et al., 2019). For this reason, to understand homelessness in the United States, one must also explore the co-occurring risk factors that permeate the lives of homeless individuals in ways that elucidate the nature of risk.
Nevertheless, existing research largely views these factors as independent, one-dimensional, or latent rather than as systematic and complex co-occurring vulnerabilities to homelessness and victimization (Blanchard et al., 2021; Wasil et al., 2020). Yet, to understand homelessness is to understand the individual risk factors that shape the pathway to homelessness, including victimization experienced prior to and during homelessness. Recent research in psychology has emphasized the need to examine psychological variables as foundational to a disorder rather than a product of it (Blanchard et al., 2021; Borsboom & Cramer, 2013; Cramer et al., 2010; Jones et al., 2018). For instance, if we suppose that being a victim of violence is a bridge symptom between the manifestation of PTSD and drug use disorder, then someone who is victimized and develops PTSD would be more likely to develop a drug addiction compared to someone who did not. On this basis, therefore, rather than emphasizing any one risk factor, a network analysis will identify the factors characteristic of homelessness and those which tend to sustain it. Additionally, a network analysis is useful for detecting how variables cluster together into communities and identifies the variables that act as bridges that connect the distinct communities constituting the network together. In sum, a network perspective aids in our understanding of the structure of mental and physical health problems in homeless populations by identifying specific causes or consequences of homelessness (e.g., violent victimization) that may fuel each other (e.g., drug use) which can be the basis for targeted and effective prevention and intervention. With that said, the goal of the present study was to investigate the network structure of multiple co-occurring life stressors and psychopathology in a representative sample of homeless people from a large urban county and further to explore differences in network structure across genders. Given past research on co-occurring and cumulative adverse life experiences, we expected to find a densely interconnected network (i.e., strong interrelationships between experiences with victimization, substance use, and mental and physical health problems). In addition, given differences in the factors associated with homelessness among men and women, we expected that experiences of sexual victimization on one hand, and substance use on the other, would be more salient for understanding the underlying network structure of homelessness for women and men, respectively.
Methodology
Data were derived from a large Demographic Survey (DS17) of the unsheltered homeless population conducted in 2017 by the LAHSA (2020a). The objective was to collect data on a sample of homeless adults to use in calculating population estimates of homeless adults across continuum of care (CoC) areas and within social planning areas (SPAs) and other geographies contained in the CoC areas across the county. The University of Southern California, the LAHSA, and other service providers collaborated in the design, implementation, and analysis of the survey. First, the researchers identified hot spots to determine the locations of data collection. The hotspot areas excluded the cities of Pasadena, Glendale, and Long Beach. A hotspot was defined as an area with a high concentration of people experiencing unsheltered homelessness compared to what would be expected based on the general population, where individuals may be staying on the street or in vehicles, tents, makeshift shelters, and so forth. Next, a two-stage sampling approach was conducted based on census tracts allocated to SPAs and within SPAs, to strata (defined using information on the homeless population hotspots). A sample of census tracts was selected from both hotspot and non-hotspot locations along with target survey volumes for areas to ensure adequate geographic coverage to meet statistical confidence thresholds. In addition to the sampled census tracts, surveys were conducted at Family Solution Centers and youth at drop-in centers, to target and augment data collection from otherwise underrepresented families and youth. Sample selection probabilities were then used in the computation of sample weights for analysis purposes.
Surveyors canvassed designated sample areas, both hotspots and non-hotspots, and asked individuals presumed to be experiencing unsheltered homelessness if they would be willing to participate in the survey. After providing individuals with a brief explanation of the purpose of the survey and how the information would be used, individuals were provided informed consent; thereafter, surveyors asked two additional questions to determine eligibility, namely where the respondent stayed for the majority of the last 30 days, and where they stayed the previous night. Any individual who reported having stayed in an unsheltered location was eligible to proceed with the full survey. The survey is comprised of over 60 questions that tap demographic characteristics of respondents (e.g., gender, race, age), history of homelessness, past employment and education, as well a variety of mental and physical health conditions. Each survey participant was paid a $5.00 gift card upon survey completion. The survey has high external validity and is considered to be representative of the entire homeless population in Los Angeles County (Leonard, 2018). For more on the survey methodology see https://economicrt.org/wp-content/uploads/2018/08/2017_Methodology.pdf. The dataset used for the present study is freely available and can be downloaded here: https://data.sandiegodata.org/dataset/economicrt-org-demographic-survey/.
Mental and Physical Health
Eligible participants were asked about their physical and mental health and well-being. More specifically, respondents were provided with the following prompt: “Next I’m going to ask you some additional personal questions about you. These questions are about your health and different lived experiences you have had. As a reminder, your answers will be kept confidential. Due to the personal nature of some of the questions, we have a response card for you to tell me the number that corresponds to your answer.” Then, they were asked, “Do you have, have you ever had, or has a healthcare provider ever told you that you have any of the following health conditions?” Response options included (1) Problematic AA, (2) problematic DA, (3) serious and long continuing MI (e.g., schizophrenia), (4) PD, (5) PI (chronic or ongoing), (5) HIV/AIDS-related illness, (7) major depressive disorder (MDD) (chronic or ongoing), (8) PTSD, (9) TBI, and (10) DI. If the responses conformed to none of the above, declined, or don’t know, they were removed from the analysis. Chronic homelessness was defined as being homeless for at least a year continuously or having four episodes of homelessness in the last 3 years that total to 1 year in addition to having a disabling condition.
Violence Victimization
Respondents were also asked whether they have experienced victimization by a domestic or intimate partner, whether they have ever been a victim of a sex crime or whether they were ever sexually trafficked. Possible responses were 1 = Yes and 0 = No. Being the victim of physical and sexual violence was recoded into one variable measuring sexual or physical victimization by an intimate partner.
Demographic Characteristics
Demographic characteristics of respondents were also collected such as age, gender, sexual orientation, homeless status, and race. Information on systems involvement was also collected (i.e., foster care and criminal justice involvement).
Statistical Analysis
The network of 12 physical and mental health indicators among homeless persons was estimated using the binary equivalent of a Pairwise Markov Random Field (Costantini et al., 2015; van Borkulo et al., 2014) called the Ising model (Epskamp & Fried, 2018). In the Ising model, the edge strength represents the predictive ability of each node once all other nodes are controlled. In the network structure, nodes represent behavioral indicators (e.g., HIV+) and undirected edges represent the statistical relationships between them that are estimated from the data. Thicker edges between two nodes indicates a stronger association between them. Nodes connected by positive edges are colored green whereas nodes connected by negative edges are colored red. The edges represent symmetric pathways between nodes representing partial correlation coefficients and estimated as conditional dependence relations. In other words, nodes that remain connected after controlling for all of the other possible associations between nodes are conditionally dependent on one or more nodes in the network. On the other hand, two nodes that lack an edge between them are conditionally independent after controlling for the associations among all other symptoms (Kendler et al., 2018).
Regularization using the least absolute shrinkage and selection operator (LASSO) was used to estimate a sparse network structure using the fewest number of edges necessary to explain the covariance structure and to control the false positive (Type I) error rate. The LASSO procedure combines L1-regularized logistic regression (Ravikumar et al., 2010; Tibshirani, 1996) with model selection based on the extended Bayesian information criteria (EBIC; hyperparameter gamma = .25) which adds a regularizing penalty and “shrinks” false positive relations to zero (Chen & Chen, 2008; Lin et al., 2020). The “tuning parameter” controls the degree to which regularization is applied to the network by minimizing the EBIC thereby selecting the best-fitting regression function (Chen & Chen, 2008). This method controls for spurious connections between nodes and estimates sparser, more interpretable, network models (Costantini et al., 2015; Epskamp & Fried, 2018). The independent variables included in the selected regression function define the nodes that the dependent variable is connected to by edges, which are weighted by the regression parameters.
Centrality Metrics
Centrality indices provide insight into the relative importance of a node in the context of the other nodes in the network (Hevey, 2018). Standardized centrality indices were estimated including strength, expected influence, closeness, and betweenness. Node strength is defined as the sum of the absolute weights of edges connected to any particular node. Similarly, the expected influence is the sum of edge weights, but not the absolute sum, and is more accurate when two nodes are negatively correlated. Node strength and expected influence measure how strongly one node is directly connected to another node. In a weighted network, a node that has high strength centrality has a greater number of edges with high magnitudes (Opsahl et al., 2010). Closeness, on the other hand, measures how strongly a node is indirectly connected whereas betweenness centrality measures how well one node connects to all other nodes.
Clustering Physical and Mental Health Symptoms
We investigated the community structure of our resulting network to explore mutual influences among indicators within and across different clusters. The walktrap algorithm was used to determine whether the 12 items of physical and mental health could be reliably detected as separate communities (i.e., to identify clusters of items in the network; Reichardt & Bornholdt, 2008; Yang et al., 2016). The walktrap algorithm is based on the principle that adjacent nodes tend to belong to the same community (Yang et al., 2016) and is considered one of the most reliable forms of community detection (Gates et al., 2016; Pons & Latapy, 2005). With this procedure, each symptom can be part of only one community. To ensure the stability of the community structure, we simulated this process 1,000 times and extracted the number of communities with the highest frequency. The modularity ratio (also known as the Q-index) was utilized to evaluate the goodness-of-fit of the communities by comparing the density of edges within a community to the density of edges outside a community (Blondel et al., 2008). Modularity ranges from 0 to 1 with higher values indicating the number of within-community edges is larger than expected at random, and therefore represent a strong community structure (Newman & Girvan, 2004).
Network Stability
We investigated the accuracy and stability of the network model using several bootstrapping procedures to test for the accuracy of edge weight rankings (from strongest to weakest) and the stability of the centrality statistics (Epskamp et al., 2017). These tests (a) reveal how accurately the connections are estimated by constructing a 95% confidence interval (CI) around them, and (b) show how stable centrality is estimated via the centrality-stability coefficient. The bootstrapped difference test was used to determine the accuracy of the edge weights. It computes the 95% CIs around the edge weights and calculates whether edges differ significantly from each other (Epskamp et al., 2018). If the CI crosses zero it suggests the edge weights are not statistically different from one another. The subsetting bootstrap method was used to determine centrality estimate stability (Epskamp et al., 2018) by dropping cases and re-estimating the networks. Centrality values are considered stable if there is a high correlation between rank order of these estimates in the original network and a network in which many cases have been dropped. The centrality stability coefficient (CS-coefficient) indicates whether this was the case; CS-coefficients should be at least above 0.25 and preferably above 0.5 to be interpreted as stable (Epskamp et al., 2018).
Network Invariance Across Gender
The Network Comparison Test (NCT) was used to detect differences in the network across gender (i.e., invariance). This procedure tests the following hypotheses (1) that males and females have the same network structure; (2) that the level of overall connectivity is the same among males and females; and (3) that the edge strength between nodes is not significantly different for males and females.
Directed Acyclic Graph
The DAG is a Bayesian network approach that provides information about both the strength and the direction of connections in a network, that is, regarding how the indicators may be causally related (i.e., potentially causal mechanisms). The DAG models a network in which edges are directed and noncircular. The DAG network estimation process was completed by bootstrapping the Bayesian hill-climbing function hc in the R package bnlearn (Scutari & Denis, 2014) and creating an average of the 50,000 bootstrapped networks. The hc algorithm repeatedly creates new models of the network and then tests the accuracy of the resulting models’ directional effects by their goodness-of-fit to the observed data. We verified the network stability by accepting only the edges that appeared in a specified proportion of the models (49.8%), based on the optimal significance threshold for inclusion (Scutari & Nagarajan, 2013).
Network estimation of the responses to the mental and behavioral health items was conducted using the function IsingFit available in R (Kossakowski et al., 2016). The resulting object stores the estimated network in the form of a weight adjacency matrix as well as thresholds of the different nodes that represent the slopes of the regression equations of predicting a particular node (see Table 1, last column). The Fruchterman-Reingold algorithm available in the qgraph package in R (Fruchterman & Reingold, 1991) was used to visualize the network (using option = “spring”) (Epskamp et al., 2012). The Fruchterman-Reingold algorithm (Fruchterman & Reingold, 1991) iteratively computes the optimal layout so that symptoms with stronger and/or more connections are placed closer to each other; central nodes often end up in the center of the graph, nodes with low centrality in the periphery. The regularized partial correlation network was estimated using the IsingFit (van Borkulo et al., 2014) package in the R programming environment which includes LASSO estimation with EBIC (“elasso”). The graphical visualizations of the binary network were generated using the R package qgraph (Epskamp et al., 2012) and the robustness of the network was assessed using the R-package bootnet (Epskamp et al., 2018). Finally, we used the library NetworkComparisonTest in R to test the invariance of the network across gender.
Characteristics of the Unsheltered Homeless Population by Gender.
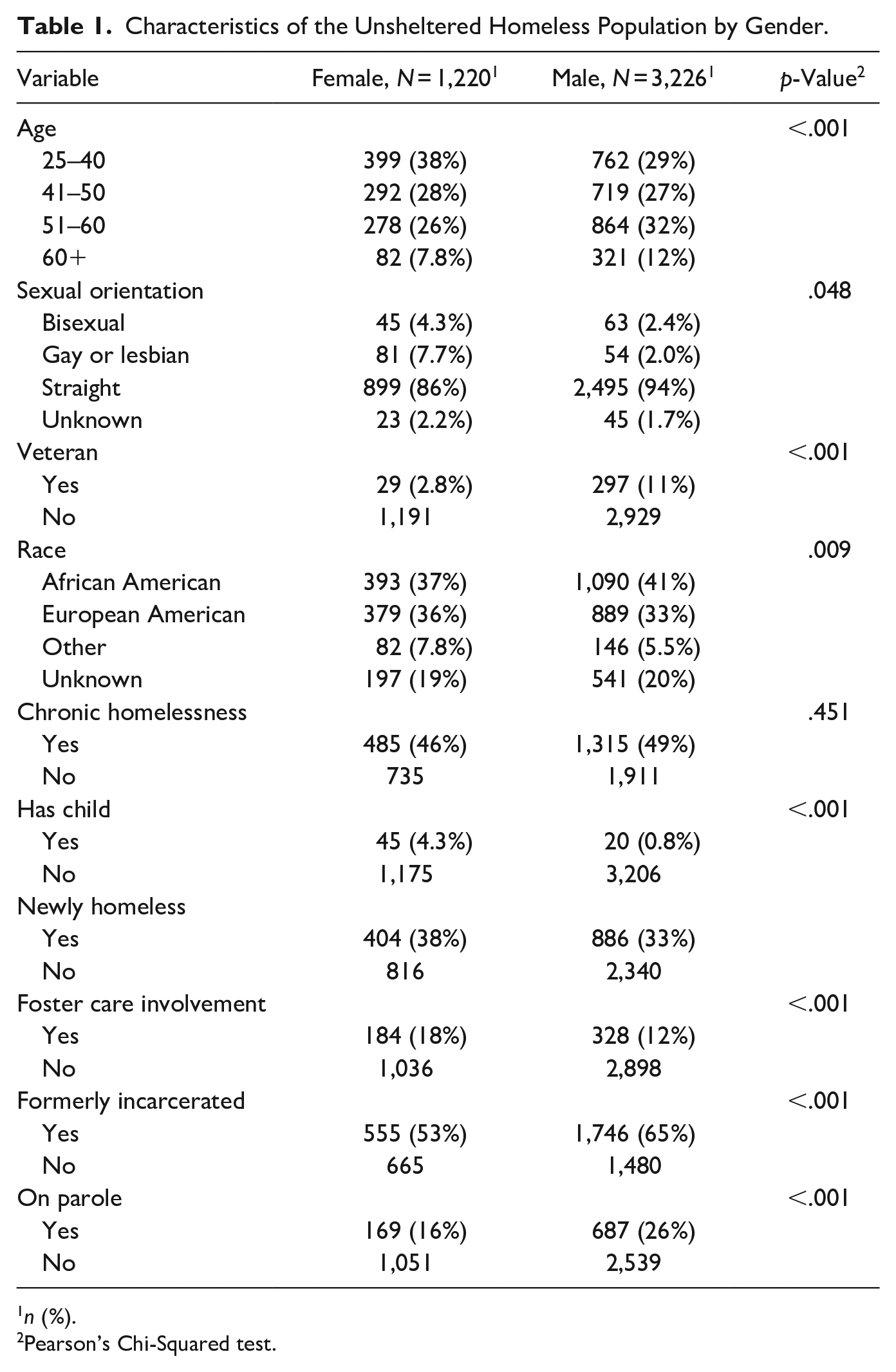
n (%).
Pearson’s Chi-Squared test.
Results
Table 1 shows the demographic characteristics of the sample by gender. The majority of the 4,446 respondents were male—almost three in four homeless respondents, or 71.2%. As shown by the table, statistically significant differences were observed across all indicators except respondent’s race. Homeless females tended to be slightly younger and more likely to identify as members of the LGBQ community compared to males, on average. Males were significantly more likely to report being a veteran and to more likely to be involved in the criminal justice system compared to females; however, females reported higher levels of foster care systems involvement. Females reported being homeless for shorter periods of time (i.e., newly homeless) whereas males were significantly more likely to report being homeless for three or more years (i.e., chronic homelessness). The threshold of a variable represents the autonomous disposition to be present. As shown in Table 2, all threshold values are negative which indicates a disposition for all variables to be absent. Nevertheless, relative to other symptoms, PS has the highest threshold (−1.615) and therefore the highest probability of being endorsed by the homeless men and women in the sample. On the other hand, the variable “HIV positive” has the lowest threshold (−4.272) and was therefore least likely to be endorsed by respondents, consistent with its overall prevalence.
Characteristics of Persons Experiencing Homelessness From the Los Angeles Homeless Services Authority (2017) n = 5,807.

Descriptive statistics of the 12 network variables are presented in Table 2. As shown from Table 2, about one in three respondents reported both being physically or sexually abused by an intimate partner (0.316) and having ever been diagnosed with a MI (0.332). About one in four homeless persons reported having ever been diagnosed with MDD with similar numbers reporting a substance use disorder. On the other hand, very few respondents reported ever being HIV positive (0.019) or having had a TBI (0.054). The Spearman correlation coefficient between pairs of variables is shown in Figure 1. As shown by Figure 1, the highest observed correlations were found for DA and AA (r = .47), being a victim of physical or sexual abuse and sex trafficking (r = .35), and a lifetime diagnosis of PTSD and MDD (r = .29).
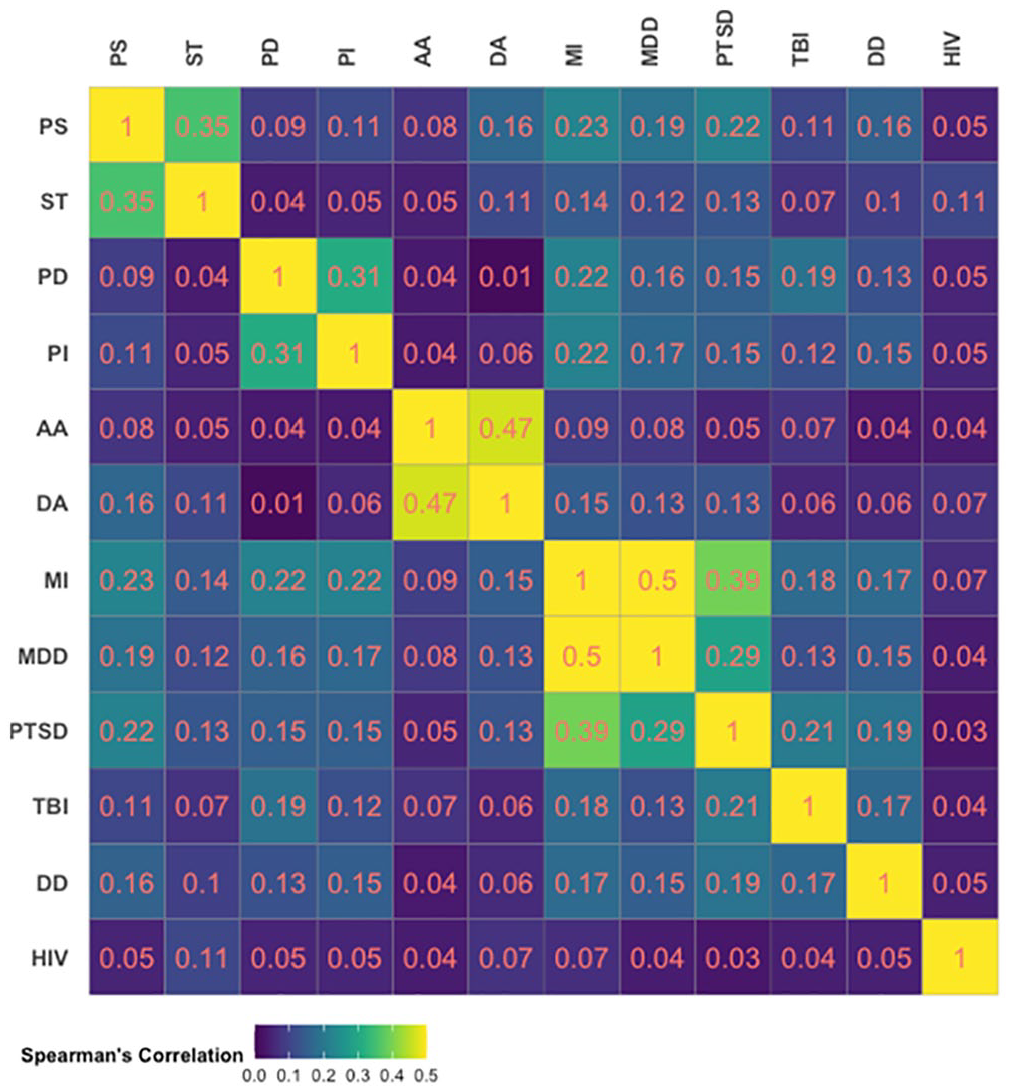
Spearman’s correlation.
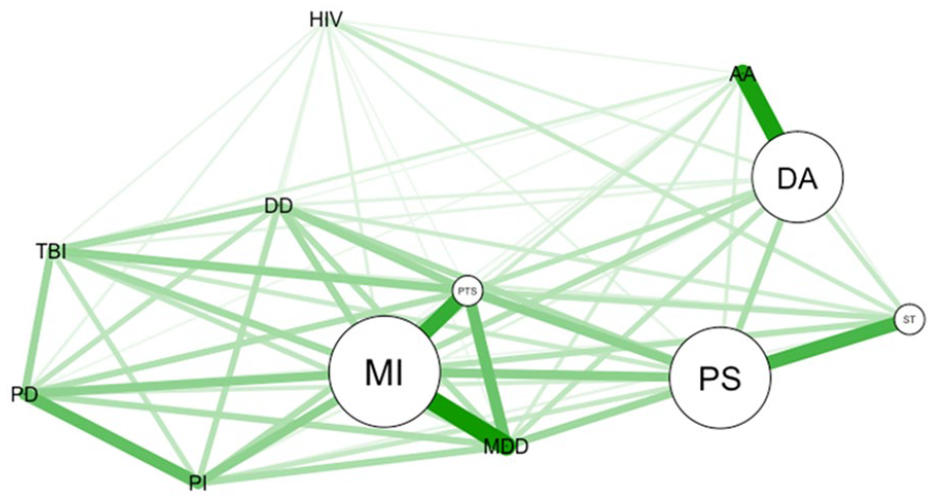
To prevent topological overlap (two highly correlated variables that measure the same thing), the correlation matrix of network nodes was first assessed as being positive definite (i.e., not linear combinations of other nodes). The goldbricker function in the R package networktools was used to compare dependent, overlapping correlations for pairs of items that were highly deemed highly correlated (r > .50) with 0.25 as the significance proportion and a significance level of 0.01 (Hittner et al., 2003; Levinson et al., 2018). Since less than 25% of correlations were significantly different, this method suggested that no reductions were necessary. The network in Figure 2a shows the association network (i.e., zero order correlations) between the physical and mental health variables. Positive (negative) associations are in green (red). Surprisingly, the edge between PD and DA is colored red indicating that the two variables are negatively related; however, all other associations are positive as indicated by the green edges between nodes. The thickness of the edges shows that some variables are very highly connected such as physical injury and PD, AA and DA, being victim of sex trafficking and PS, major depression and MI, whereas others have weaker relationships (e.g., PTSD and sex trafficking, DA and MDD). The graphical LASSO network is shown in Figure 2b. Unlike Figure 2a the edges in the graphical LASSO network represent regularized partial correlations between variables. The largest edge weights are between MDD and MI, DA and AA, and PI and PD. Figure 3 shows the results of the community detection walktrap algorithm applied to the network variables that clusters them into multiple related component parts. The results identified four clustering of nodes that are more highly interconnected among themselves than they are with nodes in other clusters that were labeled as: (1) sexual (covering PS, being victim of sex trafficking and being HIV+); (2) disability (covering physical injury, PD, DD, and TBI); (3) substance (covering drug and AA); and (4) mental health (covering MDD, PTSD, and MI/schizophrenia).

Partial correlation network and LASSO regularization. Regularized partial correlation network of 12 mental and physical health indicators. Connections between symptoms depict conservative estimates of partial correlations. The spring layout places nodes that are more related closer together. (a) Partial correlation network and (b) LASSO regularization.

Community detection analysis. Results of the community detection analysis performed on the network. The three identified communities depict symptoms that more strongly inter-correlate with each other.
Network Centrality
The centrality plots in Figure 4 provide information on the inter-connectedness of variables. Centrality indices, which measure the importance of each node to the network, are presented as standardized z-scores plotted along the x-axis. Centrality is defined as the sum of the absolute values of retained connections for each symptom with all other symptoms. A central node is one that has several strong connections compared to more peripheral nodes that have little to no connections or connections with weak edge strength. As shown by Figure 4, MI, PTSD, and drug use disorder had the highest strength centrality meaning that they have strong connections to other nodes and serve as the “bridges” connecting the other communities of nodes. Practically speaking, this means that when either MI, post-traumatic stress, or drug use disorder is present, the other nodes in the network are activated. Closeness centrality quantifies the node’s relationship to all other nodes in the network by considering the indirect connections from that node (Hevey, 2018) and measures the extent to which information from a given node can reach other nodes quickly (Wasserman & Faust, 1994). Our analysis revealed that PTSD, IPV victimization, and MI have the highest closeness centrality meaning they are closer to all other nodes in the network. The betweenness metric provides information on how important a node is in the average pathway between other pairs of nodes (Hevey, 2018). As shown by Figures 4 and 5, MI and PS by a spouse or intimate partner had the highest betweenness centrality. Node strength, closeness, and betweenness centralities demonstrated an excellent stability (CS-coefficient = 0.75, 0.67, 0.75, respectively). Network stability measures are found in the Supplemental Figures S1 to S3.
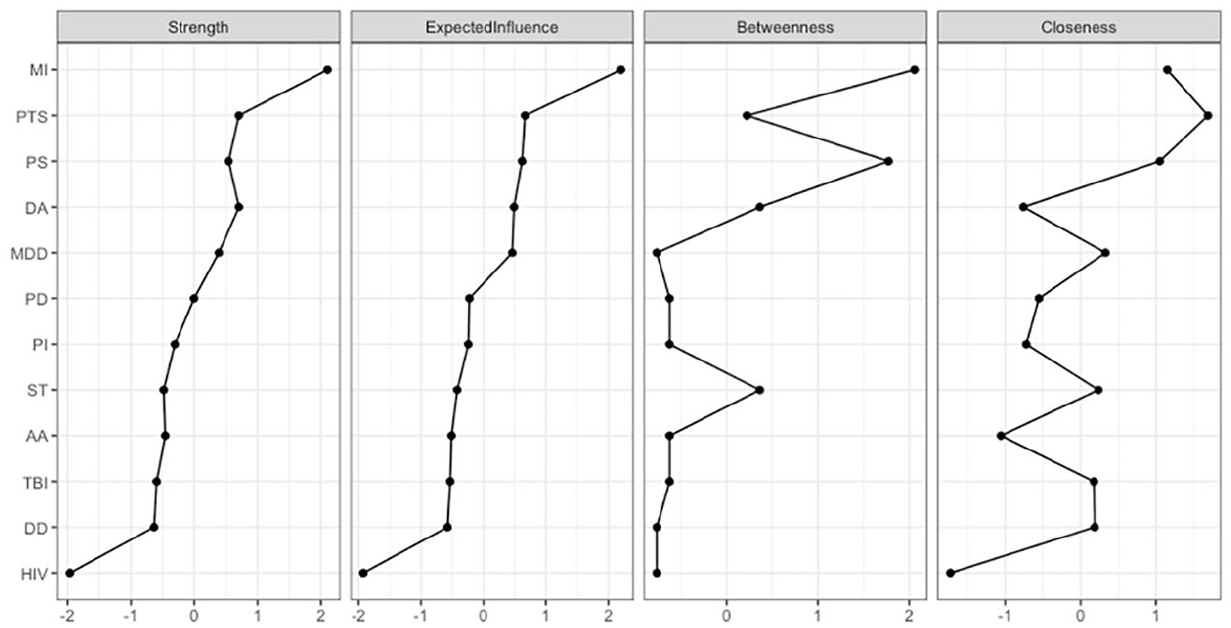
Centrality metrics. Standardized centrality estimates and expected influence of the network of the Sexual, Mental Illness, Physical Illness and Abuse diagnoses. Centrality refers to the sum of all absolute connections of each symptom with all other symptoms. Please refer to Table 1 for symptom shortcodes.
Betweenness centrality.
The network structures of females (left panel; n = 1,220) and males (n = 3,226) (see Figure 6). Estimation was performed with IsingFit and λ = 0.25. The NCT indicated that overall connectivity was the same, however multiple edges differed significantly, across samples. In other words, the network invariance tests did not uncover a significant difference in network structure across gender (see Table 3). However, two edge tests showed significant differences (p < .05) for the nodes representing IPV victimization (PS) and AA, and PS and DD. Consequently, these particular edges were found to differ significantly between males and females.

(a, b) Network structure by gender.
Results of Invariance Tests of Network Structure Across Gender.
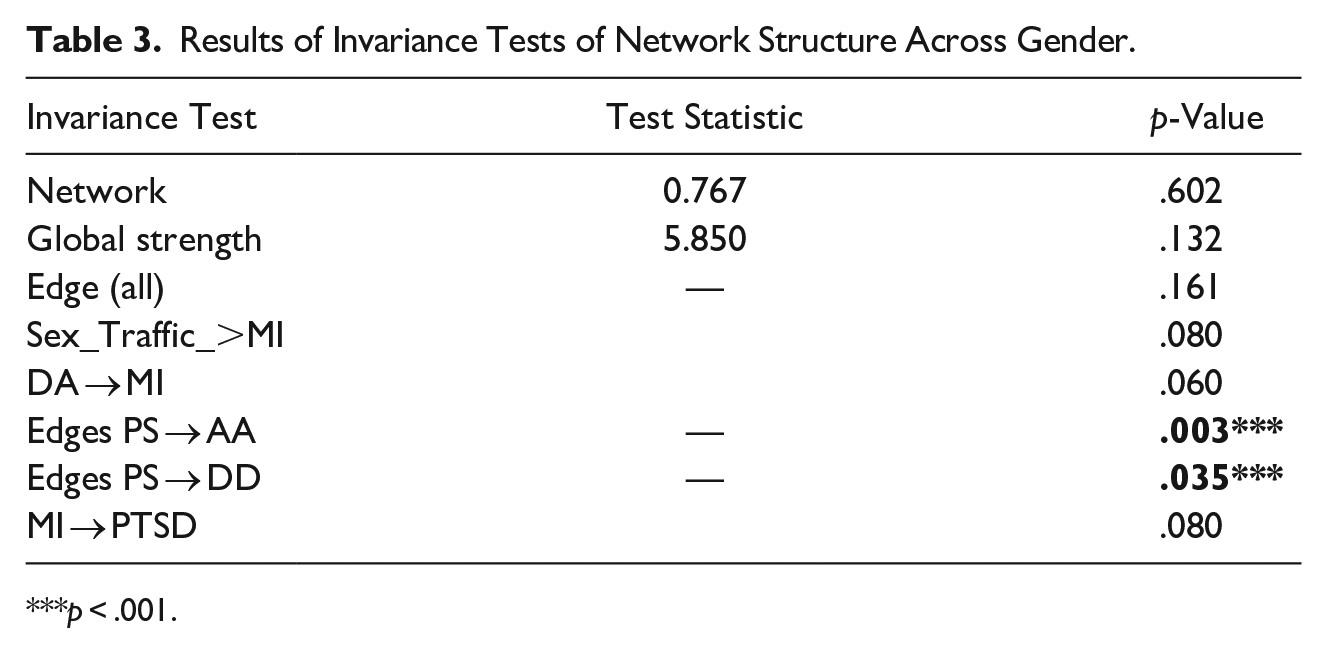
p < .001.
Figure 7 depicts the DAG arising from the averaging of the 50,000 bootstrapped networks whereby edge thickness signifies confidence that direction of prediction (and potential causality) flows in the direction depicted in the graph. As shown by the figure, a history of drug use and PD emerged as the most prominent nodes that directly predict a history of MI. In addition to MI, being physically disabled directly predicts physical injury. On the other hand, in addition to MI, drug use disorder is directly associated with PTSD, alcohol use, being physically or sexually abused, and being HIV positive. Being HIV positive along with having a TBI are downstream problems that depend on the presence of other factors in the network.

Dyadic acyclic graph indicating potentially causal mechanisms of behavioral and physical health and violent victimization among N = 5,266 homeless persons from the 2017 Los Angeles Homeless Services Authority Demographic Survey.
Discussion
The current study represents the first network analysis of the most common physical and mental health issues affecting the functioning and well-being of over 4,000 homeless persons living in Los Angeles County, California. Our network analysis provides strong evidence that the relationship between homelessness and mental and behavioral health is complex, consistent with previous studies suggesting that both are causes and consequences of homelessness (National Coalition for the Homeless, 2009). Our findings contribute to the current body of literature on homelessness by demonstrating (1) the centrality of MI and IPV in connecting all other mental and physical health variables together; (2) that PTSD and IPV are both highly affected by changes in any part of the network and can, in turn, affect changes in other parts of the network; (3) that the 12 behavioral health variables cluster into four communities characterized by disability, outcomes related to sexual behaviors, substance use and mental health issues; (4) the role of DA and PD as potentially causal mechanisms that drive the overall system; and (5) that the homelessness network structure is the same for males and females. The implications for each of these findings is discussed further below.
Our partial correlations network allowed us to assess the connections between each pair of variables considering the effect of all the other variables included in the network. This analysis showed that lifetime diagnosis of a MI, physical or sexual victimization by an intimate partner, and PTSD were the nodes with the highest centrality closeness and strength and, thus, the nodes most strongly connected to the other nodes in the network. In network theory, the activation of a node may cause the development of the connected nodes; we found that MI, IPV, and PTSD are central nodes that can affect changes in other parts of the network quickly due to its high closeness with other nodes and hence when present place individuals at higher risk for further mental and physical health problems and violent victimization. Our results in this regard are consistent with previous research showing that PTSD is a key mechanism leading to both homelessness and substance use even after controlling for lifetime experiences of victimization. As well, MI and IPV play important roles in explaining the relationship between nodes such as substance abuse and physical injury.
We found that MI, PTSD, and IPV had the highest betweenness centrality. Betweenness centrality is a measure of the extent to which a particular behavior lies between other behaviors in the network, with higher betweenness indicating that the specific behavior frequently connects other behaviors (Lowery et al., 2021). Practically speaking, this means that PTSD may mediate the relation between PD and MI on the one hand and MDD, DD, and TBI on the other. While the network analysis does not suggest a direction for this relationship, the DAG model suggested that PD may be a key driver of the overall system. Taken together, these findings are consistent with previous research showing that cognitive impairment, which is more characteristic of homeless persons compared to the general population (Spence et al., 2004; Stone et al., 2019), is highly associated with acquired brain injury and DD and can co-occur with severe MI (Roy et al., 2020). Similar to other studies, our results suggest that cognitive deficits and physical disabilities can be a risk factor for chronic homelessness (Stone et al., 2019). One implication is that providing financial assistance for disability is critical for preventing homelessness and/or helping an individual out of a state of homelessness (Evans et al., 2016). As well, health education and outreach programs that highlight the importance of both mental and physical health will facilitate a better understanding of the prevalence of these disabling, often co-occurring conditions among the homeless and is relevant for disability policy, as well as program and system planning (Roy et al., 2020). Our results also highlight the importance of untreated PTSD symptomology in influencing violent victimization risk and DDs. In sum, given their key role in linking other nodes together in the system, MI, PTSD, and IPV should be the focal point for homelessness prevention and intervention (Jones et al., 2018).
Our DAG model also pointed to the importance of DA as an important causal mechanism that drives the overall network. However, even when homeless individuals are motivated to address substance abuse problems, access to the variety of services they need to succeed in finding stable housing are not available. Taken together, our results reinforce the importance of integrating services to address the serious and complex health challenges faced among homeless persons. Until recently, few services have addressed the needs of substance abusing homeless persons who were not motivated to address their substance use. In addition, successful integration of substance abuse treatment, permanent stable housing, and related services such as mental health has been notably lacking. Our results suggest that people experiencing homelessness should have access to expanded behavioral health services including substance use disorder treatment as well as behavioral health services. It is worth noting behavioral and mental health service provision is most effective when integrated with housing services to provide a more comprehensive platform for service delivery (United States Interagency Council on Homelessness, 2018). Regarding physical and sexual violence, we note that our only significant finding regarding gender differences was in the association between victimization and mental health. This finding is consistent with other studies finding gender differences in the reasons for homelessness being related to interpersonal conflict and lack of support thereby reinforcing that different intervention strategies may be required for men and women. Organizations providing services to homeless individuals in general, and women in particular, who have experienced physical or sexual violence must acknowledge and address the impact of trauma through the provision of trauma-informed care. Research conducted by Hopper et al. (2010) shows that the best practices for providing wrap-around services to meaningfully address and treat the consequences of trauma among homeless persons include (1) incorporating and understanding the behavioral adaptations to trauma, (2) emphasizing physical and emotional safety procedures, (3) rebuilding a sense of efficacy and control, and (4) developing coping skills that are focused on the future and that utilize skill-building to increase resiliency.
Importantly, all variables in the network were highly interconnected and causally dependent. Methodologically, this finding reinforces the utility of network analysis over other factor and latent class analysis which assume conditional independence between indicators. Substantively, our results reinforce the need for interventions that focus specifically on the potentially causal factors driving the overall network. In this regard, the most important factors revealed by the DAG were DA, MI, and PD. These nodes were directly related to problematic outcomes such as lifetime diagnoses of PTSD, which was in turn directly related to experiencing physical or sexual abuse and major depression. Our results indicate a very strong relationship between histories of poor mental health and substance abuse, indicating that providing individuals with trauma-informed care will similarly address the psychosocial sequalae of domestic and interpersonal violence exposure, which will additionally create a higher success in job retention, housing stability, and healthcare. From a policy perspective, our results suggest that the provision of trauma-informed, wraparound services is critical to treat and address the complexity of psychosocial problems experienced by homeless individuals. In this regard, our research is consistent with recommendations of Hopper et al. (2010) who concluded that providing trauma-informed services can produce better behavioral health outcomes, improve housing stability, and decrease crisis-based services for people who are homeless.
Limitations
Despite the novelty of the current study it is not without limitations. First, all measures are based on self-report and hence susceptible to reporting bias. Our measures are limited to presence or absence of behavioral and mental health/victimization over the course of one’s lifetime. Therefore, it is impossible to ascertain the time period in which the respondent experienced the risk factor under consideration. Whereas our DAG analysis provides interpretable and logic estimates of potential causality, we note that our analysis is based on cross-sectional data and hence we cannot make definitive causal connections between indicators. We decided to limit the focus of our study to physical and behavioral health issues and therefore omitted institutional contact as a potential cause or consequence of homelessness (e.g., foster care, criminal justice system). Systems involvement is a critical context for homeless persons that deserves special consideration particularly given the criminalization of homelessness and the disproportionate involvement of some youth in these systems (e.g., youth of color; Boyd, 2021, LGBTQ youth; Mountz & Capous-Desyllas, 2020). Future studies should use similar methods as presented here to explore causes and consequences of homelessness by including institutionalization such as criminal justice and child welfare involvement. Despite these limitations, large-scale studies conducted on homeless persons are rare due to the hidden nature of the population and hence our study represents an important contribution to the literature. These limitations underscore the dearth of data on homelessness that currently exists and reinforces the need to continue to pursue innovative ways to collect and analyze data in order to understand the interrelationship and dependency of factors that have exacerbated catastrophic levels of homelessness in Los Angeles County and in other cities across the United States.
Conclusion
Homelessness is a complex and multifaceted phenomenon that is caused by more than financial instability alone. Addressing the multidimensional nature of homelessness requires holistic and comprehensive preventive approaches that acknowledge the interrelated mental and physical health needs of individuals in areas of high demand (see Figure 8). Programs designed to assist individuals and families experiencing homelessness must be trauma-informed to help them overcome their experiences of victimization and mental and physical health issues in the context of limited resources, diminishing social support networks, and addiction issues.
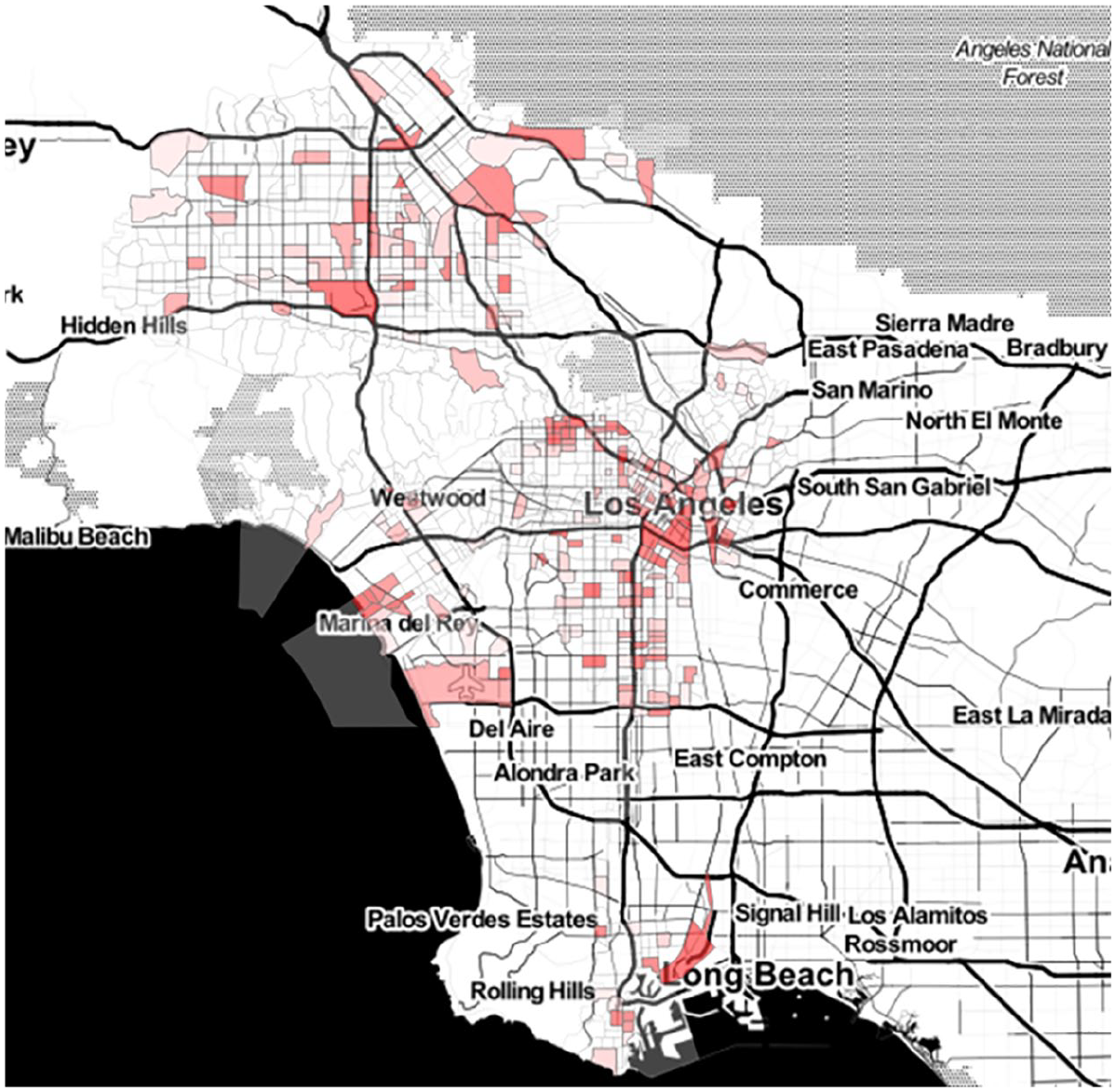
Census tracts where homeless respondents were interviewed.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605221127222 – Supplemental material for A Network Analysis of the Relationship Between Mental and Physical Health in Unsheltered Homeless Persons in Los Angeles County
Supplemental material, sj-docx-1-jiv-10.1177_08862605221127222 for A Network Analysis of the Relationship Between Mental and Physical Health in Unsheltered Homeless Persons in Los Angeles County by Gia Elise Barboza-Salerno, Anna Kosloski, Henriikka Weir, Dywane Thompson and Alexey Bukreyev in Journal of Interpersonal Violence
Footnotes
Authors’ Note
Gia Elise Barboza-Salerno is now affiliated to Colleges of Public Health and Social Work, The Ohio State University, Columbus, OH, USA.
Dywane Thompson is now affiliated to School of Criminology and Criminal Justice, University of South Carolina, Columbia, South Carolina, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.