
Abstract
Intimate partner violence (IPV) causes substantial physical and psychological trauma. Restrictions introduced in response to the COVID-19 pandemic, including lockdowns and movement restrictions, may exacerbate IPV risk and reduce access to IPV support services. This cross-sectional study examines IPV during COVID-19 restrictions in 30 countries from the International Sexual HeAlth and REproductive Health (I-SHARE) study conducted from July 20th, 2020, to February, 15th, 2021. IPV was a primary outcome measure adapted from a World Health Organization multicountry survey. Mixed-effects modeling was used to determine IPV correlates among participants stratified by cohabitation status. The sample included 23,067 participants from 30 countries. A total of 1,070/15,336 (7.0%) participants stated that they experienced IPV during COVID-19 restrictions. A total of 1,486/15,336 (9.2%) participants stated that they had experienced either physical or sexual partner violence before the restrictions, which then decreased to 1,070 (7.0%) after the restrictions. In general, identifying as a sexual minority and experiencing greater economic vulnerability were associated with higher odds of experiencing IPV during COVID-19 restrictions, which were accentuated among participants who were living with their partners. Greater stringency of COVID-19 restrictions and living in urban or semi-urban areas were associated with lower odds of experiencing IPV in some settings. The I-SHARE data suggest a substantial burden of IPV during COVID-19 restrictions. However, the restrictions were correlated with reduced IPV in some settings. There is a need for investing in specific support systems for survivors of IPV during the implementation of restrictions designed to contain infectious disease outbreaks.
Keywords
Introduction
Intimate partner violence (IPV), defined as behavior from an intimate partner or ex-partner that causes physical, sexual, or psychological harm, is a profound violation of human rights (World Health Organization, 2021). Prior to the COVID-19 pandemic, an article analyzing 366 eligible studies from 161 countries and areas estimated that 27% ([Uncertainty Interval] 23–31%) of ever-partnered women aged 15 to 49 years had experienced physical and/or sexual IPV (Sardinha et al., 2022). There remains a paucity of evidence on men’s experience of IPV; one recent study of IPV in six European cities found that male victimization of psychological aggression ranged from 48.8 to 71.8%, sexual coercion from 5.4 to 8.9%, and physical assault from 8.5 to 9.7% (Costa et al., 2015). Results from a study conducted among university students from 22 countries in Africa, Asia, and the Americas indicated that 15.4% of the men and 17.2% of the women reported physical and/or sexual IPV, with variations between types of IPV (Pengpid & Peltzer, 2016). It remains a serious public health issue, affecting survivors’ mental, physical, and sexual health (Ellsberg et al., 2008).
When countries around the globe began enforcing restrictions to social contact to interrupt transmission of the novel SARS-CoV-2 virus, concerns were raised that many COVID-19 restrictions may inadvertently increase the risk of IPV (Boserup et al., 2020; Bradbury-Jones & Isham, 2020): stay-at-home orders, travel restrictions, and fragmented services may trap IPV survivors in the same accommodation as their perpetrator, with limited access to social support networks or essential services (Boserup et al., 2020; Bradbury-Jones & Isham, 2020; Hall & Tucker, 2020). Stress and anxiety due to the pandemic, as well as economic losses resulting due to the implementation of restrictions, could furthermore compromise coping strategies and serve as triggers for violence (Arenas-Arroyo et al., 2021; Bradbury-Jones & Isham, 2020; Gresham et al., 2021). Conversely, COVID-19 restrictions such as travel bans could forcibly distance survivors from perpetrators of violence if they live separately (Vives-Cases et al., 2021).
In the context of COVID-19, there is no clear, universal definition of what lockdown entails (Haider, Osman, Gadzekpo, Akipede, Asogun, Ansumana, Lessells, Khan, Hamid, et al., 2020). COVID-19 restrictions are heterogeneous and may include stay-at-home orders, geographic containment, limitations on gatherings, and business closures (Haider, Osman, Gadzekpo, Akipede, Asogun, Ansumana, Lessells, Khan, Yeboah-Manu, et al., 2020). While a growing body of literature has examined changes in IPV since the implementation of COVID-19 restrictions in various countries (Agüero, 2021; Arenas-Arroyo et al., 2021; Barbara et al., 2020; Fawole et al., 2021; Gosangi et al., 2021; Gresham et al., 2021), studies that assess the potential impact of the initial restrictions on IPV have had mixed results. Several settings reported an increase in reports of IPV, including police reports and hotline calls (Brink et al., 2021; Nesset et al., 2021). However, other studies have suggested that the restrictions may have decreased or not affected IPV burden (Erausquin et al., 2022; McNeil et al., 2022; O’Hara & Tan, 2022). Some studies suggest that COVID-19 restrictions may have increased disparities in IPV, with subsets of marginalized people having an increased risk (Peitzmeier et al., 2021). Decreases in official IPV reports may have been related to fewer reporting mechanisms, weakened surveillance, and fewer facility-based services (Evans et al., 2020). It is therefore important to better understand the impact of COVID-19 restrictions on IPV to inform future epidemic-related activities.
Current Study
Few studies have examined IPV in a multicountry context. The WHO, UNFPA, and many other organizations have turned to online research in the past 2 years to obtain behavioral data during COVID-19 restrictions (International Centre for Reproductive Health Belgium, 2022; World Health Organisation, 2020). In response to the COVID-19 pandemic, the International Sexual Health and REproductive Health (I-SHARE) multicountry cross-sectional study was established to examine sexual and reproductive health during the restrictions. The I-SHARE study protocol prespecified IPV as one of the primary outcomes (Michielsen et al., 2020). We hypothesized that COVID-19 restrictions would increase the risk of IPV, especially among people cohabiting with partners. Drawing on data from 30 countries, this article addressed the following research questions to determine correlates of intimate partner physical violence, intimate partner sexual coercion, and intimate partner sexual assault during COVID-19 restrictions among those who participated in the I-SHARE survey: This study aims to (1) compare recollected experiences of IPV prior to the restrictions to current IPV experiences during the restrictions in 30 countries and (2) examine correlates of IPV during the restrictions.
Methods
Study Development
Survey development was a collaborative effort among research teams in 30 countries whereby potential items were proposed and discussed for inclusion in the survey. The WHO IPV scale was suggested for inclusion because it is a widely used scale and has been used in many diverse settings. A short form of the items included in the WHO IPV scale was selected. Respondents were assured that they could leave these items blank. Each country was required to include details of country-specific organizations and IPV resources at the end of the survey. In each country, the in-country lead organized translation into relevant local languages, field testing, and ethical approval. Field testing included providing the survey instrument in print form to at least 10 individuals who provided feedback on translation and sensitive topics. Further field testing in digital form among 5 to 10 volunteers per country was conducted to iteratively examine errors in skip logic function. Each country survey had one to three rounds of field testing. More details are found in Michielsen et al. (2020).
Participants and Procedures
Participants from each country were recruited through an online survey link that was distributed through local, regional, and national networks chosen by the in-country research lead, including email listservs, sexual and reproductive health networks, and social media groups. Twenty-three countries used convenience sampling (Australia, Canada, Colombia, China, Czech Republic, Egypt, France, Germany, Italy, Latvia, Panama, Portugal, Luxembourg, Mexico, Malaysia, Moldova, Mozambique, Nigeria, Singapore, South Africa, Spain, Uruguay, United States), six used online panels with participants selected based on age, ethnicity, gender, and location (Sweden, Botswana, Uganda, Lebanon, Kenya, Argentina), and two used population-representative sampling (Denmark, Czech Republic). The survey took approximately 15 to 20 minutes to complete. Open Data Kit software (version 1.16) was used to collect data from participants on personal devices.
Inclusion criteria for the survey were to be a minimum of 18 years or older (19–49 years old in Sweden), a current resident in the country where the survey was being conducted, and able to provide an online informed consent. Participant safety was also considered in the consent process and given the sensitive nature of questions asked, participants were allowed to withdraw from the survey at any point and leave out items that they did not wish to answer. No identifiable information was collected. In addition to country-specific IPV resources at the end of the survey, some countries provided warnings, social support, and IPV services as part of the informed consent process.
Data for each country were only accessible by in-country leads who made final decisions regarding data use. Data sharing agreements were signed among participating country institutions for multicountry analyses. Ethical approvals were obtained from each country’s ethical review committee before the study launch. Ethical approval was obtained from Ghent University (BC-07988) and the University of North Carolina at Chapel Hill (295989) for secondary data analysis from multiple countries. Researchers from each country were invited to join working groups focused on analyzing multicountry data: this article is the main paper from the IPV working group. Survey data were collected only if they met the following criteria: institutional review board approved, description of sampling methodology provided, and field tested. The survey instrument included sections on sociodemographic characteristics, adherence to COVID-19 restrictions (e.g., physical distancing), couple and family relationships, sexual behaviors, access to contraceptives, access to maternal healthcare, abortion, IPV, and HIV/STI testing. The full survey instrument has been published (Michielsen et al., 2020).
Measures: Dependent Variables
Six items were used to measure IPV, adapted from the WHO multicountry survey on women’s health and domestic violence against women (Supplementary Data 1) (Heise & Hossain, 2017). This article reports on three of these items measuring physical and sexual IPV. The first item related to physical violence, including being slapped, hit, pushed, kicked, choked, or had something thrown at them by an intimate partner. Two items related to sexual violence, including being forced to have sex when they did not want to, which we subsequently referred to as intimate partner sexual assault (Bagwell-Gray et al., 2015), and made to have sex because they were afraid of what their partner would do if they didn’t have sex (subsequently referred to as intimate partner sexual coercion) (Bagwell-Gray et al., 2015). We focused on physical and sexual IPV to facilitate comparison with other studies (Bagwell-Gray et al., 2015; Devries et al., 2013; García-Moreno et al., 2013) and because these are associated with greater morbidity and mortality (Devries et al., 2013; García-Moreno et al., 2013). Given the cross-sectional nature of the study, participants were asked about IPV experiences during the three months prior to COVID-19 restrictions and since the introduction of the restrictions. Answer options included the following: no; yes, once; yes, multiple times; and no partner.
Measures: Independent Variables and Covariates
Individual-level variables included sociodemographic characteristics such as sex assigned at birth, age, sexual orientation, highest educational attainment, and subjective income levels, perceived changes to one’s economic situation as a result of COVID-19, having children at home, living arrangements with partners, and area of residence. These survey items were based on a WHO sexual and reproductive health survey (Kpokiri et al., 2021).
In terms of country-level variables, the stringency of lockdown index from the Oxford COVID-19 Government Response Tracker was included as a quantitative measurement of lockdown stringency ranging from 1, least stringent, to 100, most stringent. Each country’s maximum stringency measure was included (Hale et al., 2020). The gender inequality index was also used as a measure of country-level gender inequality (United Nations Development Programme, 2021).
Data Analysis
Sociodemographic characteristics were summarized using descriptive statistics and cross-tabulated with responses to the physical and sexual violence items (Table 1). We also examined IPV stratified by geography, using low- and lower middle-income countries (LMICs), upper-middle income countries (UMICs), and high-income countries (HICs) based on World Bank categories (Hamadeh et al., 2021). The self-reported proportion of participants experiencing IPV prior to the introduction of restrictions was compared to the proportion of participants experiencing IPV during the restrictions (Table 2). Subsequently, bivariate and multivariable analysis of sociodemographic and relevant variables chosen a priori was undertaken for each country using adaptive Gauss–Hermite quadrature (AGHQ; Bolker et al., 2009). The model was subsequently run using random effects and including country-level variables. Given past evidence for varying dynamics based on cohabiting status (Tan et al., 2021), stratified analyses were conducted according to whether participants lived with their partner during COVID-19 restrictions. The proportion of participants reporting IPV during COVID-19 restrictions was examined. Sensitivity analyses were conducted using the same models while excluding data from countries with fewer than 200 participants (Supplemental Tables 1 to 4b). Stata 16.0 (StataCorp, College Station, TX, USA) was used for primary analyses and MLwiN 2.34 (University of Bristol, Bristol, UK) was used for sensitivity analyses.
Sociodemographic Characteristics of the Sample and Cross-Tabulation of Sociodemographics With Responses to Sexual and Physical Violence Questions During the COVID-19 Restrictions.
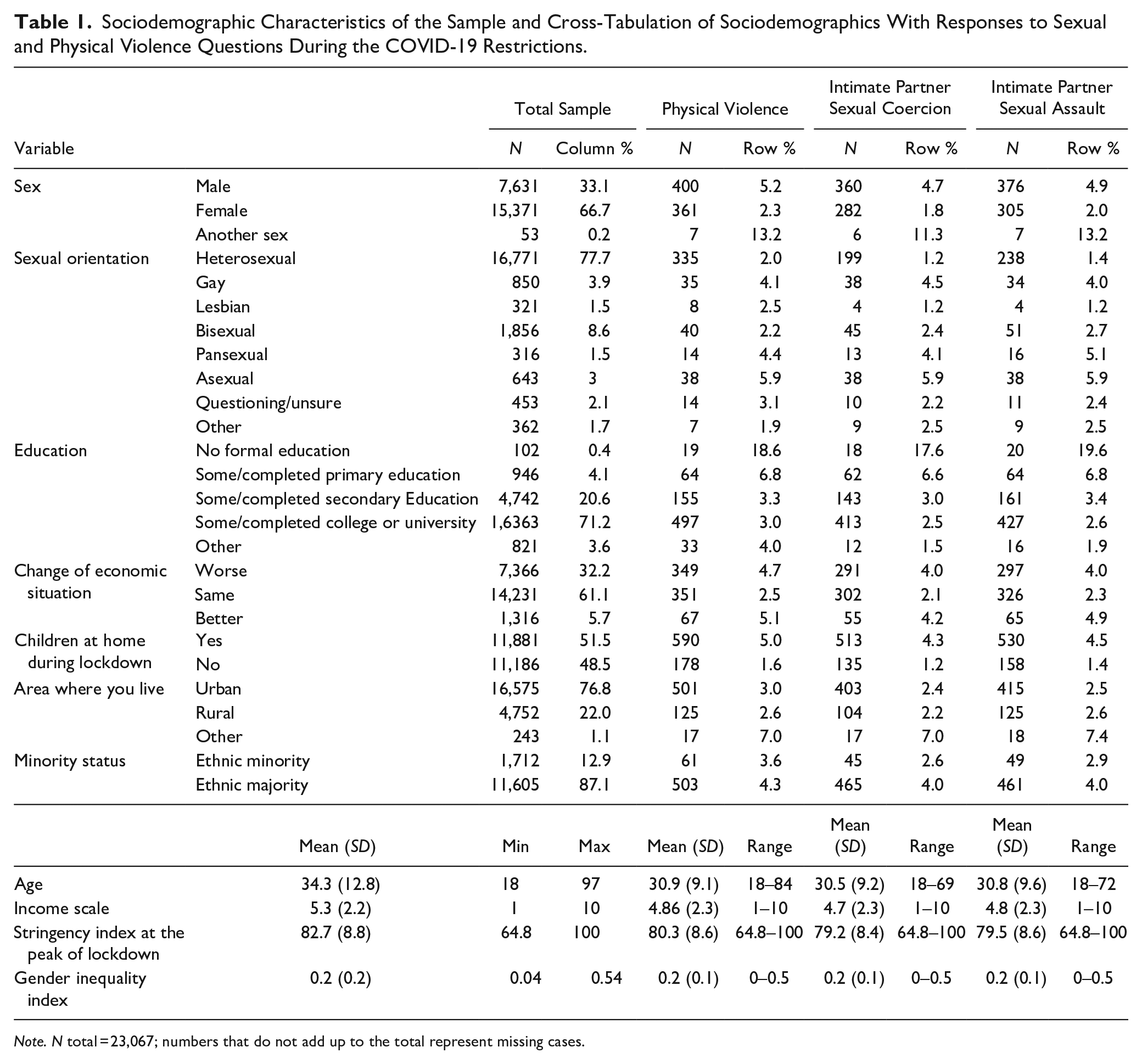
Note. N total = 23,067; numbers that do not add up to the total represent missing cases.
Descriptive Statistics of Physical, Sexual, and Composite Violence Pre-COVID and During COVID-19 Restrictions.

Note. N total = 23,067; numbers that do not add up to the total represent missing cases.
Given the relatively small number of respondents reporting IPV in this sample, a composite IPV variable was created where a participant answered yes to experiencing any one of the three physical or sexual violence items. A composite sexual violence variable was also created where a participant answered yes to either of the sexual violence items. The sexual violence items were also analyzed separately because there are important differences and other IPV research has differentiated these constructs as unique subtypes of sexual violence (Bagwell-Gray et al., 2015; Bouffard & Goodson, 2017). Intimate partner sexual coercion is more common and may be less likely to be recognized by legal systems (Bagwell-Gray et al., 2015; Bouffard & Goodson, 2017).
Since both bivariate and multivariate analysis returned high odds ratios and confidence intervals for the pre-COVID violence variable, which can be common in multilevel modeling (Ensoy et al., 2015; Ju et al., 2020), Firth logistic regression was explored which returned smaller odds ratios (between 4 and 6) for experiencing violence during COVID-19 if a participant had experienced violence before COVID-19 restrictions. The mixed-effects models were then rerun using penalized quasi-likelihood (PQL) and Bayes estimation (Supplemental Tables 7 and 8) (Benedetti et al., 2014; Bolker et al., 2009; Breslow & Clayton, 1993; Ju et al., 2020). Given that there were few differences in the results between these and the AGHQ models, the AGHQ models were retained. We furthermore ran the models without the pre-COVID variable (Supplemental Table 6).
Results
Among all participants, 15,336/16,329 (93.9%) answered questions about physical and sexual violence. Of the 15,336 participants who answered the questions about experiencing physical and sexual violence, the majority identified as female (68.4%), heterosexual (81.7%), and had at least some college or university education (72.5%). The average age of participants was 35.3 years (SD = 12.5). The majority experienced no economic change during the pandemic (63%) and were living with a partner (63.2%). These participants did not differ considerably from the total sample (Table 1).
Prior to COVID-19 restrictions, 7% of participants in HICs reported experiences of physical and sexual violence, compared to 13% in UMICs and 14% in LMICs. A total of 4.9, 10.5, and 12.5% of participants reported experiencing physical and sexual violence during COVID-19 restrictions in HICs, UMICs, and LMICs, respectively (Table 3). The proportion of participants who experienced physical and sexual violence before COVID-19 restrictions was higher than the proportion of participants who experienced physical violence and sexual violence during COVID-19 restrictions across all three indicators. Physical violence was experienced by 6.3% of participants before COVID-19 restrictions and by 5.0% during COVID-19 restrictions. Intimate partner sexual assault was experienced by 5.7% before COVID-19 restrictions and 4.5% during COVID-19 restrictions. Intimate partner sexual coercion was experienced by 5.0% before COVID-19 restrictions and 4.2% during COVID-19 restrictions (Table 2). Participants who had experienced any type of violence prior to the introduction of the COVID-19 restrictions had higher odds of experiencing violence during COVID-19 restrictions (Tables 4 and 5).
Descriptive Statistics of Composite Violence by World Bank Country Income Level.
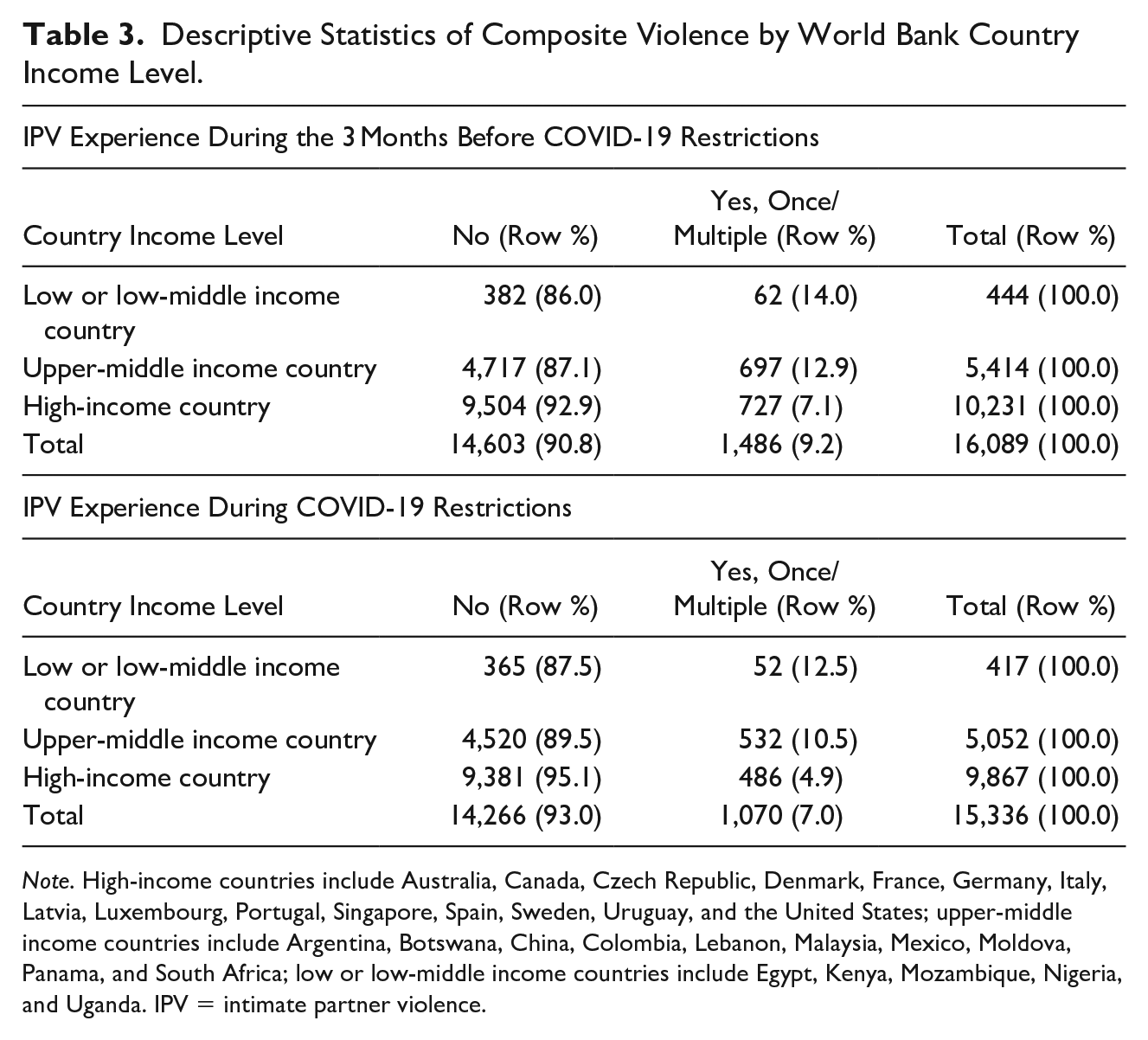
Note. High-income countries include Australia, Canada, Czech Republic, Denmark, France, Germany, Italy, Latvia, Luxembourg, Portugal, Singapore, Spain, Sweden, Uruguay, and the United States; upper-middle income countries include Argentina, Botswana, China, Colombia, Lebanon, Malaysia, Mexico, Moldova, Panama, and South Africa; low or low-middle income countries include Egypt, Kenya, Mozambique, Nigeria, and Uganda. IPV = intimate partner violence.
Binomial Logistic Regression Coefficients Predicting Experience of Composite Violence Among Participants in the I-SHARE Study, 2020 to 2021 (Partner Lived With Them).
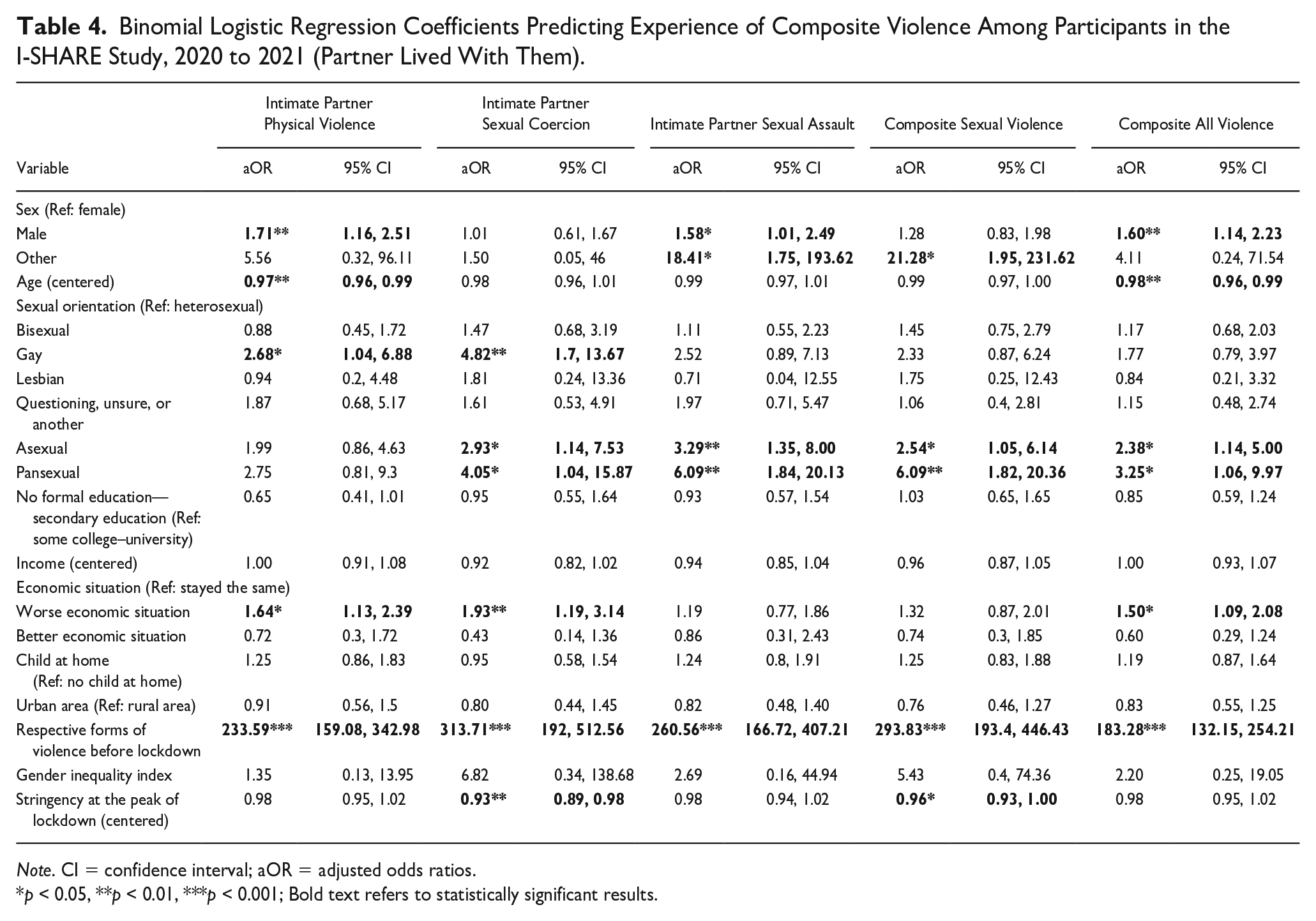
Note. CI = confidence interval; aOR = adjusted odds ratios.
p < 0.05, **p < 0.01, ***p < 0.001; Bold text refers to statistically significant results.
Binomial Logistic Regression Coefficients Predicting Experience of Composite Violence Among Participants in the I-SHARE Study, 2020 to 2021 (Partner not Living With Them).
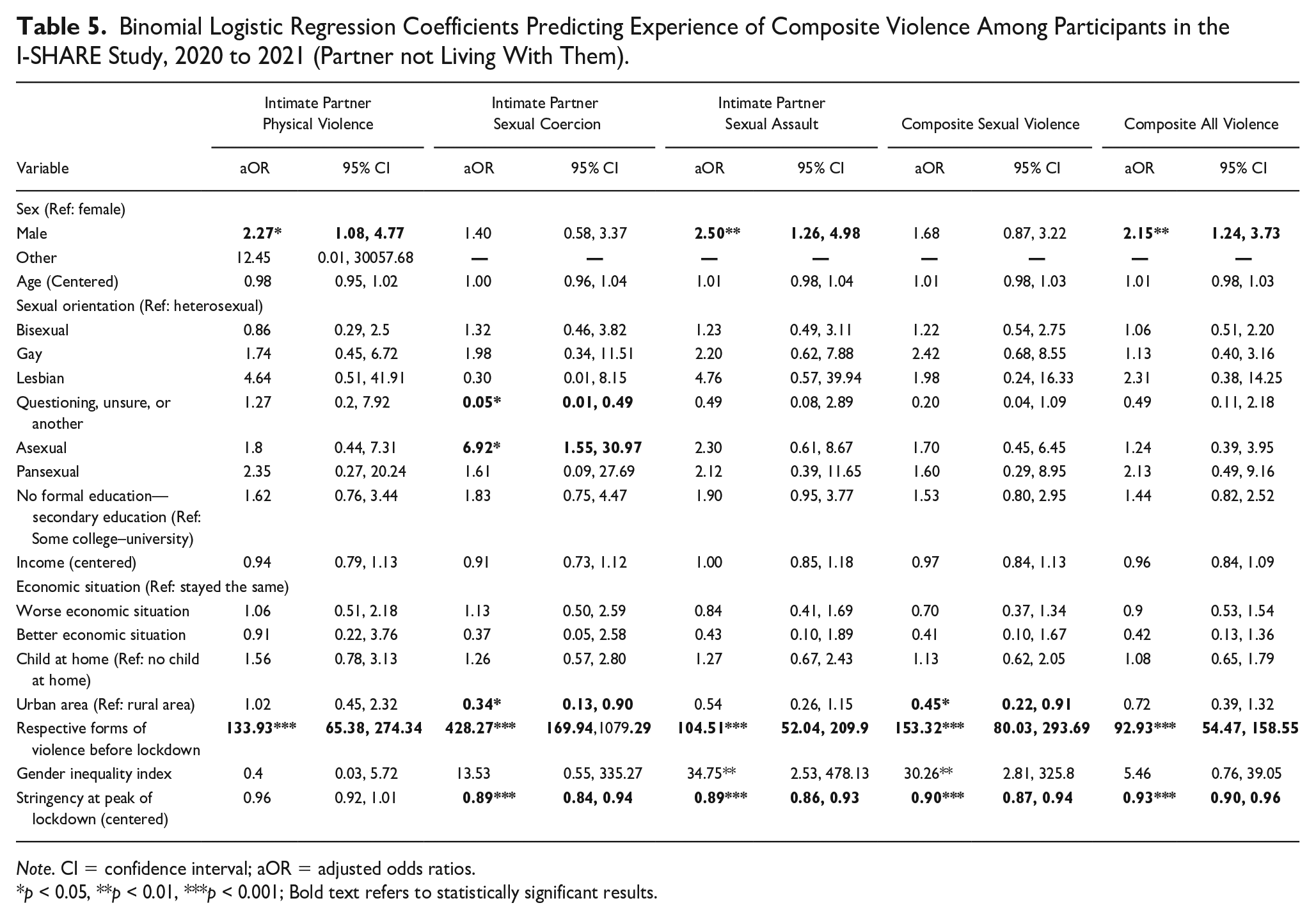
Note. CI = confidence interval; aOR = adjusted odds ratios.
p < 0.05, **p < 0.01, ***p < 0.001; Bold text refers to statistically significant results.
The analysis suggested several correlates of physical IPV. Among participants living with their partners, there were higher odds of experiencing violence during COVID-19 restrictions for participants who were male at birth (aOR = 1.71, 95% CI [1.16, 2.51]) compared to those who were assigned female at birth. Participants who identified as gay had higher odds of experiencing physical violence (aOR = 2.68, 95% CI [1.04, 6.88]) compared to those who identified as heterosexual. There were also higher odds of experiencing physical partner violence for those who stated their economic situation had worsened during COVID-19 restrictions (aOR = 1.64, 95% CI [1.13, 2.39]) compared to those who experienced no change or an improvement in their economic situation during the pandemic. Among participants who were not living with their partners and were male at birth, there were higher odds of experiencing such violence during COVID-19 restrictions (aOR = 2.27, 95% CI [1.08, 4.77]).
Regarding intimate partner sexual coercion, among participants living with their partners, there were higher odds of experiencing violence during the COVID-19 restrictions for those who identified as gay (aOR = 4.82, 95% CI [1.70, 13.67]), asexual (aOR = 2.93, 95% CI [1.14, 7.53]), or pansexual (aOR = 4.05, 95% CI [1.04, 15.87]), relative to those who identified as heterosexual. There were also higher odds of experiencing intimate partner sexual coercion for those who stated their economic situation had worsened during COVID-19 restrictions (aOR = 1.93, 95% CI [1.19, 3.14]) compared to those who experienced no change or an improvement in their economic situation. There were slightly lower odds of experiencing such violence during COVID-19 restrictions for those who were residing in countries with a higher stringency index score (aOR = 0.93, 95% CI [0.89, 0.98]). Among participants who were not living with their partners, there were higher odds of experiencing such violence during the COVID-19 restrictions for participants who identified as asexual (aOR = 6.92, 95% CI [1.55, 30.97]), but lower odds for those who identified as questioning, unsure, or another (aOR = 0.05, 95% CI [0.01, 0.49]), relative to those who identified as heterosexual. There were also lower odds of experiencing such violence for participants residing in urban and semi-urban areas (aOR = 0.34, 95% CI [0.13, 0.90]) compared to those in rural or semirural areas, as well as for those residing in countries with a higher stringency index score (aOR = 0.89, 95% CI [0.84, 0.94]).
Regarding intimate partner sexual assault, the model indicated that among participants living with their partner, there were higher odds of experiencing sexual violence during COVID-19 restrictions for those who were male at birth (aOR = 1.58, 95% CI [1.01, 2.49]) or of other sex (aOR = 18.41, 95% CI [1.75, 193.62]), people who identified as asexual (aOR = 3.29, 95% CI [1.35, 8.00]), and people who identified as pansexual (aOR = 6.09, 95% CI [1.84, 20.13]). Among participants who were not living with their partners and who were male at birth, there were higher odds of experiencing such violence during COVID-19 restrictions (aOR = 2.50, 95% CI [1.26, 4.98]). There were also lower odds of experiencing such violence for participants residing in countries with a higher stringency index score (aOR = 0.89, 95% CI [0.86, 0.93]).
Our sensitivity analyses suggest that our main findings were robust when we disaggregated data based on sampling strategy, study population, and geographic region (Erausquin et al., 2022). Data from mixed-effects models using PQL and Bayes estimation were similar to those from the the primary analyses. There were few differences in results between these and the AGHQ models. The AGHQ models were retained and are additionally presented without adjustment for pre-COVID violence (Supplemental Tables 6 and 7). Overall, adjusting for pre-COVID violence attenuated the estimates for factors that would have predisposed individuals to any form of IPV regardless of COVID-19, including having children at home, and measures of socioeconomic status such as years of schooling and subjective income levels. Our findings with adjusted pre-COVID violence therefore robustly capture the factors that exacerbated violence during COVID-19 restrictions.
Discussion
This study examined IPV during COVID-19 restrictions in 30 countries using data from online surveys. The data suggest a substantial burden of IPV during COVID-19 restrictions. However, many people perceived their experience of IPV to be less common during COVID-19 restrictions compared to their experience before COVID-19. Additionally, more stringent COVID-19 restrictions were associated with less intimate partner sexual coercion. This study expands the literature by including analyses of country-level predictors such as stringency of COVID-19 restrictions and organizing a large multicountry survey in which IPV was a primary outcome. This study also highlights the potential for online methods to supplement and enrich emergency response research. While many in-person methods were restricted, behavioral research was able to adapt to diverse COVID-19 settings.
The analysis suggests a modest decrease in the proportion of participants reporting IPV during COVID-19 restrictions compared to those reporting during the 3 months prior to the restrictions. Current evidence regarding the impact of COVID-19 restrictions on IPV is mixed. A substantial number of studies indicate increased rates of IPV or IPV-related assistance seeking during COVID-19 restrictions (Agüero, 2021; Fawole et al., 2021; Gosangi et al., 2021; Rhodes et al., 2020) while a smaller number of studies found decreased rates (Barbara et al., 2020; Gosangi et al., 2021; Ravindran & Shah, 2020). Increase in assistanceseeking and calls to helplines may be due to an increase in severity of IPV rather than increased rates, as well as greater willingness of survivors to seek help when they are confined at home (Stripe, 2020). Decrease in violence may be due to lockdowns curtailing the need to use violence as a control mechanism within a relationship (Arenas-Arroyo et al., 2021) or forcibly separating survivors from perpetrators (Vives-Cases et al., 2021).
This study found higher odds of physical violence for those whose economic situation worsened as a result of COVID-19 restrictions. This is consistent with other researches on COVID-19, poverty, and IPV risk (Arenas-Arroyo et al., 2020; Das, et al., 2021; Fawole et al., 2021; Gresham et al., 2021; Perez-Vincent et al., 2020). Lockdowns have caused widespread economic problems which can generate stress and impact both IPV victimization and perpetration (Perez-Vincent et al., 2020). OneCOVID-19 study found that IPV occurred when both partners experienced economic stress during the restrictions (Arenas-Arroyo et al., 2020). Similarly, other COVID-19 studies in the U.S., Nigeria, and India have also found that anxiety about finances or economic stress to be associated with IPV risk (Das et al., 2021; Fawole et al., 2021; Gresham et al., 2021). This underlines the importance of public sector’s financial support in response to pandemics.
When examining country-level factors, residents of countries with more stringent COVID-19 restrictions had slightly lower odds of experiencing intimate partner sexual coercion. This finding contrasts with trends observed in single-country studies from India and Argentina (Perez-Vincent et al., 2020; Ravindran & Shah, 2020). More stringent COVID-19 restrictions may have inadvertently protected participants from some forms of sexual violence. This may be due to enforced distance between survivors and perpetrators.
This study found that sexual minorities had higher odds of experiencing physical and sexual violence during COVID-19 restrictions. These findings are consistent with other studies of physical and sexual violence among sexual minorities during the restrictions (Stephenson et al., 2021; Swiatlo et al., 2020). Previous studies have suggested that the restrictions increased stress and stigmatization among sexual minorities (Gibb et al., 2020). Sexual minority stress may exacerbate IPV risk during the restrictions. Minority stress related to stigmatization and homonegativity has well-known links to adverse health outcomes (DiPlacido, 1998; Salerno et al., 2020). In some settings, sexual minorities have been blamed for worsening the COVID-19 pandemic or targeted by punitive COVID-19 laws and regulations (Gibb et al., 2020; Salerno et al., 2020). This may further marginalize a subpopulation already at heightened risk of IPV.
This study has several limitations. First, there was heterogeneity in sampling methods, including convenience samples, online panels, and population-representative samples. Nevertheless, several strategies were undertaken to improve the comparability of our results for participants across varying samples and country contexts. We adopted a multilevel modeling approach which allowed us to account for country-level attributes. This allowed us to better estimate standard errors and capture differences in countries. Furthermore, while convenience sampling was used in many countries, we also had several countries that used population-representative sampling or online panels, which allowed us to stratify our main findings based on sampling methodology that showed similar findings between groups (Erausquin et al., 2022). We also conducted sensitivity analyses (see supplementary materials) where countries with less than 200 participants were removed from analyses. Finally, we ensured that our analyses adjusted for measures of pre-COVID IPV (i.e., self-reported experiences of IPV among participants prior to COVID-19). To address these potential limitations, further details on our sensitivity analyses were added in our supplementary materials without including these pre-COVID IPV measures.
Second, online surveys have an inherent selection bias because only willing individuals with internet access participate. At the same time, we used the following strategies to decrease potential bias: population-based sampling strategies and online panels to compare with convenience samples; piloting and tailoring the online surveys to facilitate local implementation; leveraging relationships with national and global organizations to enhance recruitment; and prespecifying analyses plans (Hlatshwako et al., 2021). Third, response bias may have impacted the results. IPV underreporting is common and survivors who were living with their perpetrators may have been unable to report IPV (Arenas-Arroyo et al., 2021). This article’s survey instrument used established methods and each survey provided a list of local IPV resources. Fourth, this study focused on cross-sectional data collected from July 2020 to February 2021. As a result, the longitudinal effects of COVID-19 restrictions on IPV were not captured. Fifth, retrospective self-reports were used which instructed participants to indicate the frequency of a certain behavior during the 3 months before COVID-19. However, these assessments are an important source of data in the context of IPV where clinical ascertainment of outcomes is often not possible. Sixth, many adolescents experience IPV (World Health Organization, 2021) but this study focused only on adults. Finally, since there was absence of relevant national or local data from all study settings involved in this survey, we were not able to comparatively establish the representative accuracy of our respective samples.
This study has implications for policy, practice, and research. From a COVID-19 policy perspective, stringent lockdowns may have protected some individuals from experiencing some types of sexual violence. Nevertheless, such restrictions have potentially placed individuals such as sexual minorities, and those who had experienced worse economic situations, at a greater risk of IPV. Policy makers may consider ensuring that services are made available to such populations at a greater risk of IPV. From a practice perspective, our findings indicated a substantial burden of IPV experienced during COVID-19, and therefore recommend telepsychiatry and psychology services be strengthened and reoriented toward IPV detection, prevention, and responses. Further research and action are needed to ensure the safety of people who experience IPV during COVID-19. Specifically, more research is needed to understand how new work/home arrangements may impact IPV risk.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605221141865 – Supplemental material for Intimate Partner Violence During COVID-19 Restrictions: A Study of 30 Countries From the I-SHARE Consortium
Supplemental material, sj-docx-1-jiv-10.1177_08862605221141865 for Intimate Partner Violence During COVID-19 Restrictions: A Study of 30 Countries From the I-SHARE Consortium by Linda Campbell, Rayner K. J. Tan, Maximiliane Uhlich, Joel M. Francis, Kristen Mark, Naomi Miall, Stefano Eleuteri, Amanda Gabster, Simukai Shamu, Leona Plášilová, Elizabeth Kemigisha, Adesola Olumide, Priya Kosana, Felipe Hurtado-Murillo, Elin C. Larsson, Amanda Cleeve, Soraya Calvo González, Gabriela Perrotta, Victoria Fernández Albamonte, Lucía Blanco, Johanna Schröder, Adedamola Adebayo, Jacqueline Hendriks, Hanna Saltis, Michael Marks, Dan Wu, Chelsea Morroni, Tammary Esho, Peer Briken, Takhona Grace Hlatshwako, Rebecca Ryan, Nik Daliana Nik Farid, Raquel Gomez Bravo, Sarah Van de Velde and Joseph D Tucker in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We want to acknowledge the following I-SHARE members for their contributions to this article: Kristien Michielsen, Vinicius Jobim Fischer, Amr Abdelhamed, Noor Ani Ahmad, Juliana Anderson, Nicholás Brunet, Sharyn Burns, Leonardo Chavane, Juan Carlos Rivillas, Fiorella Farje De la Torre, José de Jesús González- Salazar, Gert Martin Hald, Devon Hensel, Corina Iliadi-Tulbure, Olena Ivanova, Anna Kågesten, Kateřina Klapilová, Lucia Knight, Dorie Kogut, Eneyi Kpokiri, Gunta Lazdane, Alejandra Lopez-Gomez, Ismael Maatouk, Filippo Maria Nimbi, Caroline Moreau, Rocio Murad Rivera, Viola Nilah Nyakato, Pedro Nobre, Caitlin Alsandria O’Hara, Shania Pande, Emilie Peeters, Carles Pericas, Lore Remmerie, Juan Rivillas, Eusebio Rubio-Aurioles, Osama Shaeer, Jenna Marie Strizzi, Kun Tang, Inês M. Tavares, Jennifer Toller Erausquin, Sonam Shah, Eline Van Damme, Wah Yun Low, and Wei-Hong Zhang. A full list of I-SHARE consortium members can be found on the I-SHARE website. We would like to thank the Academic Network for Sexual and Reproductive Health and Rights Policy, Social Entrepreneurship to Spur Health, the London School of Hygiene and Tropical Medicine Sexually Transmitted Research Interest Group, and the University of North Carolina at Chapel Hill Institute for Global Health and Infectious Diseases.
Author Contributions
LC and JT conceptualized the study and wrote the first draft of the manuscript. LC, RT, MU, JF, KM, and NM were on the data analysis subgroup and organized main analyses and sensitivity analyses. SE, AG, SS, LP, EK, AO, FH, EL, AC, SG, GP, VA, LB, JS, JH, TE, PB, and RB were all leading respective in-country surveys. MM coled the digital subgroup and assisted with survey programming and data management. PK, TH, and LC helped to clean data and program the survey instrument. HS assisted with survey implementation. SD helped with multilevel modeling and data analysis. All authors critically revised the article for important intellectual content and approved the final version. All authors had full access to all of the data and had final responsibility for the decision to submit for publication.
Data Sharing
The survey protocol and final survey instrument are available. Requests for data access must follow the rules outlined in the I-SHARE data sharing agreement. Data code can be made available upon request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: JT received support from the US NIH (NIAID K24AI143471, UH3HD096929). The funder played no role in study design, the methods of collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.