
Abstract
Assessing the risk for future harm is a crucial task for agencies managing Family Violence (FV) cases. The Integrated Safety Response (ISR) is a multiagency collaboration of such agencies operating in two areas of New Zealand, and one of the first steps in their process is to perform a risk assessment. However, in these assessments, it is unclear whether the factors ISR triage team members select are the basis for their overall risk categorization (low, medium, or high), and if those factors are risk factors (i.e., empirical predictors of outcomes). Therefore, in this study we documented the factors ISR triage teams recorded during their risk assessments for 842 FV cases and examined the relationship of those factors with the risk categories. We then investigated whether those factors and the risk categories were indeed capable of predicting FV-related outcomes (recurrence and physical recurrence). We found most of the triage teams’ recorded factors were associated with the risk categories, but fewer than half of the factors were associated with FV-related outcomes. Moreover, the risk categories predicted FV-related outcomes better than chance, but their predictive ability varied across subgroups, performing poorly for aggressors who were Māori or women, and for non-intimate partner cases. We concluded that the ISR triage teams’ risk assessment protocol may benefit from increased structure and validation.
Agencies responding to Family Violence (FV) cases commonly use risk assessments because they aid practitioner judgments about the likelihood of future harm and can be used to inform their efforts to prevent that harm (Garrington & Boer, 2020; Henning et al., 2021; Robinson & Clancy, 2020; Stanley & Humphreys, 2014). The Integrated Safety Response (ISR) is a multiagency collaboration of organizations responsible for managing FV cases reported to police in two areas of New Zealand (Integrated Safety Response, 2018). Every FV episode reported to New Zealand Police is referred to ISR for further case management, and one of the first actions the ISR takes is to perform a risk assessment. However, it is unclear whether the factors ISR triage team members identify are the basis for the categorical risk level they allocate to cases (low, medium, or high), as well as whether those factors are risk factors (i.e., empirical predictors of criminal outcomes; Bonta & Andrews, 2016). Therefore, in this study we document the factors ISR triage teams recorded for 842 cases and examine the relationship of those factors with the risk categories. We also analyze whether those factors and the risk categories were indeed capable of predicting two FV-related outcomes (recurrence and physical recurrence).
The RNR Model and Risk Assessment by FV Practitioners
Agencies providing FV services often use risk assessments to guide their decision-making (Henning et al., 2021; Robinson & Clancy, 2020; Spivak et al., 2020; Stanley & Humphreys, 2014). In criminal justice settings, risk assessments are designed to predict the likelihood of an individual committing a criminal act in the future (Prins & Reich, 2021). This process improves the ability of law enforcement and other agencies to protect victims and target limited resources at the people who need them most. The risk principle of the Risk Needs Responsivity (RNR) model for correctional treatment states that treatment intensity should be matched to the level of risk offenders pose; with high-risk offenders having the greatest “room for improvement,” thus also receiving the greatest level of intervention (Bonta & Andrews, 2016; Polaschek, 2012). In correctional settings, the RNR principles are commonly used to design and evaluate treatment programs for individual offenders, but the model is also relevant for a wider range of interventions, including family-based interventions (Polaschek, 2016). Translated into the FV context, the risk principle simply indicates that families or whānau 1 with the greatest risk-related needs should be prioritized for effective interventions, and a higher level of service and support (Polaschek, 2016).
Risk assessment instruments are comprised of various risk factors, with the instruments’ ability to predict the criminal outcome being drawn from the statistical association those factors have with that outcome. Importantly, this association is not necessarily causal (Kropp, 2004). Risk factors are understood as measurable characteristics that can be used to predict peoples’ likelihood of engaging in criminal behavior (Bonta & Andrews, 2016; Polaschek, 2012). In addition, victim-focused risk factors can be used to predict peoples’ likelihood of experiencing victimization (Spencer et al., 2019). Many of these characteristics are known as static risk factors, which cannot be changed easily once they have occurred (e.g., age at first offense).
On the other hand, some characteristics used in risk assessments to predict criminal behavior are dynamic risk factors: changeable characteristics of the person or their circumstances (e.g., current substance use; Bonta & Andrews, 2016), with changes in these offending-related needs being followed by changes in the measured criminal outcome (Douglas & Skeem, 2005; Polaschek, 2012). These factors are often psychologically meaningful; they may be causal or act as proxies for the underlying causal mechanisms that lead to criminal behavior (Mann et al., 2010); thus, they are often chosen as targets for change during treatment (Prins et al., 2021).
In line with this idea, a second purpose of risk assessments is to identify information that can be used to inform service provision and case management (Butters et al., 2021; Garrington & Boer, 2020; Kropp, 2008). The responsivity principle from the RNR model states that interventions should be delivered in a way that maximizes people’s ability to engage and benefit from them (Bonta & Andrews, 2016). Agencies play a pivotal role in selecting which interventions families receive (e.g., alcohol or drug rehabilitation, parenting support, financial planning, or nonviolence programs) and providing those interventions in an engaging and accessible manner. The process of assessing risk, which involves reviewing case information, identifying changeable needs that are linked to recurrence, and thinking through future scenarios where harm may occur, serves the dual function of assisting practitioners to plan their response (Butters et al., 2021; Garrington & Boer, 2020; Kropp, 2008).
Types of Risk Assessments
Risk assessment processes differ in the extent to which they are structured. Actuarial instruments are the most structured; they contain a list of risk factors selected for their ability to predict the outcome. These risk factors are scored and combined algorithmically to produce an overall risk score (Geurts et al., 2021). Contrastingly, in unstructured clinical judgment risk assessments, practitioners subjectively evaluate case information and use their expertise in a nontransparent way to identify what they regard as important information, before forming an intuitive impression of the likelihood of future harm (Hilton et al., 2006). Structured Professional Judgment (SPJ) risk assessments sit between these two contrasting methods of assessing risk. SPJ risk assessments typically include empirically derived risk factors, but allow discretion (Hart et al., 2016); practitioners can include information they deem relevant from outside the instrument’s list of risk factors and decide themselves how all the pertinent information (i.e., the identified risk factors) should be weighted to influence the final assessment (Hilton et al., 2006; Kropp, 2004, 2008).
Within SPJ, assessment protocols vary in their procedures and in their predictive validity (Garrington & Boer, 2020; Geurts et al., 2021). Some SPJ risk assessment instruments contain a list of items that are rated (e.g., 0, 1, or 2; absent, somewhat present, or present, respectively; Douglas et al., 2013; Garrington & Boer, 2020; Kropp & Hart, 2015). After completing these ratings, practitioners select a categorical label to communicate the level of risk they think is present in the case (e.g., low, moderate, or high). For research, ratings on SPJ instruments are often summed to produce a total score, and when used this way (i.e., actuarially), their predictive validity is similar to that of actuarial instruments (van der Put et al., 2019). When the risk categories produced using SPJ instruments are used to predict outcomes they tend to have poorer predictive validity than actuarial instruments (e.g., DASH; Richards, 2009; Turner et al., 2019), but this may be in part due to the reduced variance inherent in a three-item scale (e.g., low = 1, medium = 2, or high = 3; Jolliffe Simpson et al., 2021).
Some of the most well-known actuarial or SPJ risk assessment instruments were created to predict reassault, rearrest, or reconviction in intimate partner violence (IPV) cases, and include the Revised Domestic Violence Screening Instrument (Stansfield & Williams, 2014), the Ontario Domestic Assault Risk Assessment (Hilton & Eke, 2017; Hilton et al., 2004), the Spousal Assault Risk Assessment Guide (Kropp & Hart, 2015), and other instruments to predict the risk of intimate partner homicide (e.g., Danger Assessment; Messing et al., 2017). Few validated risk assessment instruments exist for other types of family relationships; a small number have been created for child maltreatment (e.g., California Family Risk Assessment, Dankert & Johnson, 2014; Checklist of Child Safety, van der Put et al., 2016), and some others can be used with all types of FV (e.g., New Zealand Police Dynamic Risk Assessment; Jolliffe Simpson et al., 2021; Victoria Police Screening Assessment for Family Violence Risk; Spivak et al., 2020). In addition to assessing FV risk, some instruments (e.g., SARA; Kropp & Hart, 2015) explicitly inform case management. But despite the availability of these instruments, practitioners often rely on their expertise when assessing risk for FV cases, opting instead to use a less-structured approach (Walklate & Mythen, 2011).
The Integrated Safety Response
Practitioners working in New Zealand’s ISR multiagency crisis response service for FV routinely perform risk assessments based on the SPJ approach. The ISR includes representatives from organizations such as Police, District Health Boards, and nongovernmental FV service providers (e.g., whānau support, nonviolence programs, and women’s refuge). Importantly, Indigenous service providers are partner agencies in the ISR and deliver many of the interventions offered to families. Māori (Indigenous people of New Zealand) are overrepresented in ISR cases, making up around one-fifth of ISR cases but one-tenth of the population in the Canterbury area, and over half of ISR cases but one-fifth of the population in the Waikato area 2 (Dobbs & Eruera, 2014; Mossman et al., 2017). Accordingly, responsiveness to Māori is an important indicator of the ISR’s performance (Mossman et al., 2017).
One of the first steps in the ISR’s process is for a triage team to assess risk for future FV and assign interventions. Triage teams meet daily to discuss recent cases reported in the ISR catchment area, assess the likelihood and severity of future FV, and collaboratively make a risk categorization (low, medium, or high) using a risk assessment guide (see “Method” section and Supplemental Materials; Integrated Safety Response, 2018). During their assessments, the triage teams do not score the items in the risk assessment guide; instead, they freely select risk factors from the guide and from information held by their respective agencies and record the factors they think are most relevant for the case in a free-text field in a centralized database. In essence, they use SPJ to perform an idiographic formulation of what underpins risk for the case in question.
This Study
In this study, we seek to better understand both the process and the predictive validity of the ISR triage teams’ risk assessments. Importantly, triage teams record factors after agreeing upon a risk categorization for a case, introducing the possibility that they may retrospectively justify their categorization, rather than using the factors prospectively to inform their judgment of risk. Put simply, it is unclear whether the factors that triage teams select are the basis for the risk category they allocate. Therefore, we will document the factors triage teams recorded for 842 cases and examine their frequencies and the relationship of those factors with the risk categories the teams assigned.
In addition, because the triage teams can freely select factors, it is unclear whether the factors chosen are risk factors that can be used to predict the likelihood of future FV (Bonta & Andrews, 2016), and the risk categories’ predictive validity has not previously been explored in research. Accordingly, we will examine the association of the factors with FV-related outcomes (recurrence and physical recurrence) and appraise the discriminative ability of the risk categories for those same outcomes. Because FV cases involve heterogeneous aggressors and family relationships, we will explore the risk categories’ discriminative ability for different subgroups of cases according to the relationship of the aggressor to the victim and by aggressor characteristics.
Method
Data Source
This study used archival data sourced from the ISR’s Family Safety System database for a larger study on FV in New Zealand (Jolliffe Simpson et al., 2021). The ISR is a FV multiagency crisis response service including representatives from New Zealand Police, Ara Poutama Aotearoa (Department of Corrections), District Health Boards, Oranga Tamariki (child protection services), Accident Compensation Corporation, and nongovernmental organizations that provide services to families and whānau experiencing FV (Mossman et al., 2017). All FV episodes reported to police are referred to ISR for further triaging, risk assessment, and case management, enabled by information sharing between the organizations involved. A FV episode was defined as an event involving any form of harm to a person who is in, or has been in, a family relationship with the aggressor (Integrated Safety Response, 2019).
Procedure
New Zealand Police extracted the dataset containing information about each FV episode reported in November and December 2018 in Waikato and Canterbury from the Family Safety System database. We coded the risk factors recorded in ISR case notes for episodes reported in the 2-week period between 1 and 14 November, 2018, which covered 842 cases. We also coded FV-related recurrence outcomes using criteria (see below) from information in the archive about episodes reported in the 24 weeks following the index episode where the index aggressor was again recorded as an aggressor or mutual participant 3 (i.e., was not the reported victim).
Risk Factors
Triage teams assessed each case and made a risk categorization (low, medium, or high) assisted by a risk assessment guide (Integrated Safety Response, 2018). The guide included 46 risk factors relating to the victim, aggressor, relationship, children or young people, and practice considerations (see supplemental materials; Integrated Safety Response, 2018). The ISR risk assessment guide is based on risk factors and lethality indicators drawn from the international research literature, but it has not yet been validated or evaluated. Triage teams did not score items per se; instead, team members identified relevant risk factors from the information held by their respective agencies and shared that information to guide group decision-making. After a triage team agreed on a risk category, they recorded the risk factors present in the case in a free-text field and used those risk factors to form a case management plan. Although it is likely that the triage teams prioritized some risk factors over others, it was not possible for us to establish risk factors’ weights from the recorded information, but only their presence. It is the presence of these risk factors that we focus on in the present study.
We initially developed a coding scheme to organize the risk factors listed in the free-text field in the Family Safety System database into 74 dichotomous variables. As expected, many of these variables came from the risk assessment guide; but some recorded factors were not listed in the guide, and we coded these as well. We then removed the variable any mention of child because it overlapped two other variables (vulnerable child and non-biological child). The first author coded the presence or absence of each risk factor for all cases, and to examine inter-rater reliability a postgraduate student with experience in both FV practice and the Family Safety System independently coded 199 cases (23.5% of the sample). We calculated intraclass correlation coefficients and used guidelines from Koo and Li (2015) to interpret them: <.50 = poor, .50–.74 = moderate, .75–.89 = good, and .90–1.0 = excellent. Of the 73 risk factors we examined, 10 had perfect agreement, 21 had excellent agreement, 24 had good agreement, 11 had moderate agreement, and 2 had poor agreement (see supplemental materials for the intraclass correlations). A further five variables were low in frequency and absent in all cases coded for inter-rater reliability, but we left them, because infrequent variables still have the potential to be good risk predictors, and to avoid artificially reducing the heterogeneity of the risk factors. We therefore chose to retain all variables except those with poor agreement, leaving 71 variables for analysis.
FV-Related Outcomes
We recorded two FV-related outcomes. Recurrence was a binary indicator defined as any subsequent FV-related call for police service within 24 weeks after the index episode, where the index aggressor was an aggressor or mutual participant (i.e., not the victim). Physical recurrence was a binary indicator for whether physical harm was recorded in the police report for any episode reported during the 24 weeks following the index episode.
Analytic Plan
We conducted analyses in R (R Core Team, 2013) and in IBM SPSS Statistics v. 27. We used descriptive statistics and cross-tabulations to describe the sample and identify statistically significant associations between demographic characteristics and the ISR triage teams’ risk categories. Next, we used descriptive statistics and cross-tabulations to identify associations between the recorded factors and risk categories.
To discern whether the factors were risk factors (i.e., empirically associated with the FV-related outcomes), we analyzed their associations with recurrence and physical recurrence with point biserial correlations. Then we calculated the area under the receiver operating characteristics curve (AUC) for the risk categories predicting recurrence or physical recurrence over the following 24 weeks. AUC statistics communicate the probability that a randomly selected person with a given outcome (i.e., recurrence or physical recurrence) would have a higher risk classification than a randomly selected person without that outcome. AUCs can range from 0 to 1; values near .5 indicate discriminative ability similar to chance, and values closer to 1 indicate better accuracy (Helmus & Babchishin, 2016). The AUC is one of many statistics used to evaluate predictive accuracy and has several advantages, including being relatively resilient to the base rate of the outcome, and being nonparametric (thus appropriate for ordinal categories; Helmus & Babchishin, 2016). We repeated the AUC analyses for different subgroups of cases according to the relationship of the aggressor to the victim and by aggressor characteristics.
Results
The average age of aggressors was about 33 years with a small proportion being under 18 years old (n = 67, 8.0%), whereas the average age of victims was about 35 years and a similarly small proportion of victims were under 18 years old (n = 55, 6.5%). Around three-quarters of aggressors were men, and around three-quarters of victims were women. Most aggressors and victims were Māori or New Zealand European. Aggressors were most commonly the current partners of victims (half of the sample) followed by former partners, parents, siblings, or other family members. Almost 60% of cases in the sample were in the Waikato region, with the remainder in Canterbury.
Table 1 shows that over half of the cases were classified by an ISR triage team as being at medium risk of future FV outcomes, a third were low risk, and a small proportion were classified as high risk (6.7%). The final two columns of the table show χ2 statistics for the relationship between demographic variables and the risk categories, with statistically significant associations at α = .05 present for almost all variables. For example, one in three aggressors were women in the low-risk category, and this proportion became smaller in the higher risk categories. The proportion of victims who were men followed a similar pattern.
Descriptive Statistics for the Sample Overall (N = 842) and by ISR Risk Category.
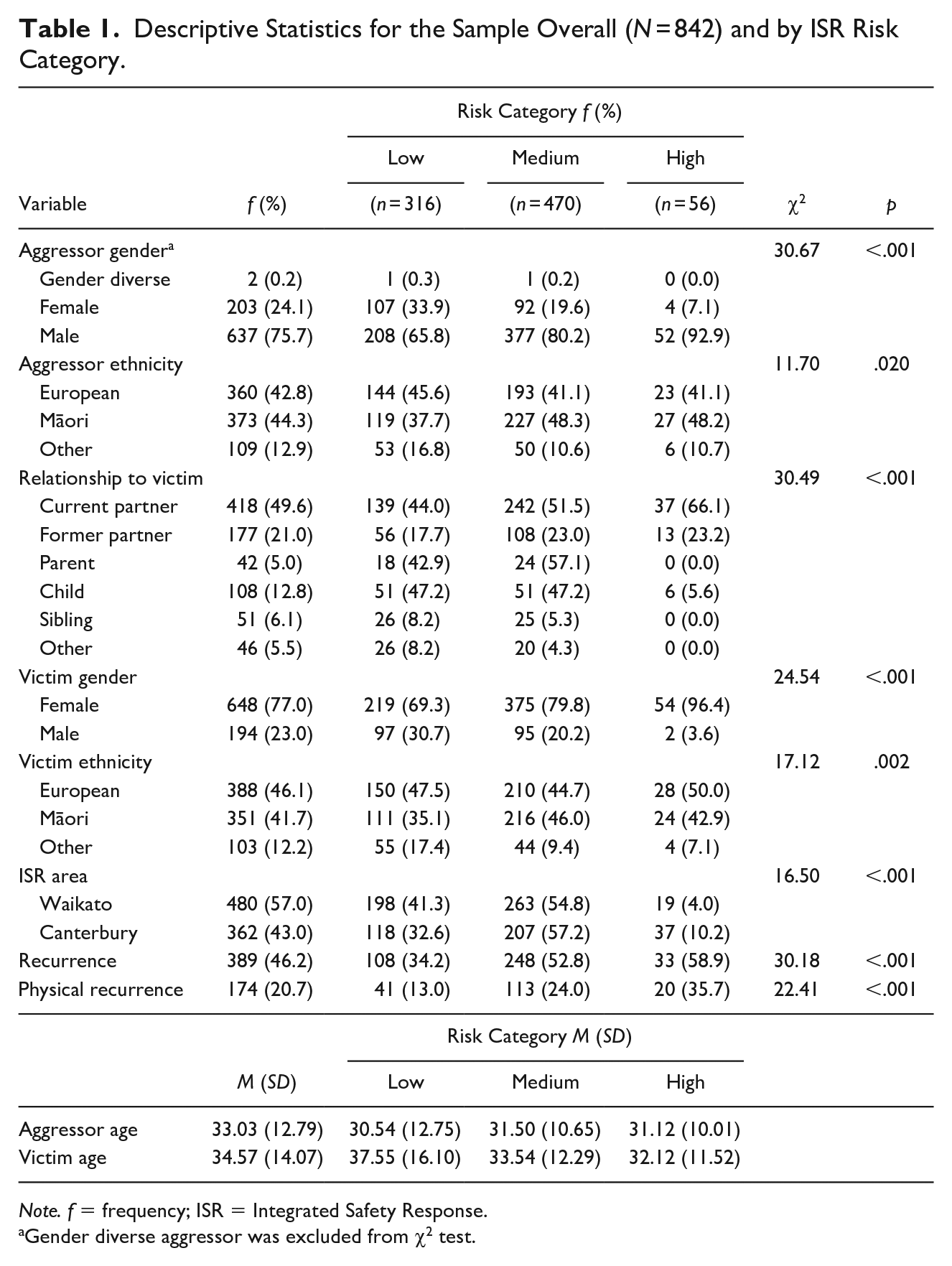
Note. f = frequency; ISR = Integrated Safety Response.
Gender diverse aggressor was excluded from χ2 test.
There was also an association between the risk categories and ethnicity, whereby a greater proportion of aggressors who were Māori were in the medium- and high-risk categories, a greater proportion of victims who were Māori were in the medium-risk category, and a greater proportion of victims who were European were in the high-risk category, compared with other ethnicities. Cases in the high-risk category almost exclusively involved IPV, and other family relationships were overrepresented in the low-risk category. A greater proportion of cases in the Canterbury region had higher risk categorizations than in Waikato.
Finally, Table 1 shows the proportion of cases with recurrence or physical recurrence in the 24 weeks following the index episode. Overall, almost half of cases had a recurrence reported to police during this period, with one in five cases experiencing a recurrence in which the aggressor physically harmed the victim. The proportion of cases with recurrence and physical recurrence differed by risk category, with those proportions increasing as the risk category increased.
Table 2 shows the 71 factors coded from the triage teams’ risk assessments, which we organized inductively, based on the sections in the ISR risk assessment guide (see Supplemental Materials; Integrated Safety Response, 2018). Unsurprisingly, the most common factors recorded were types of harm in the index episode: verbal abuse (43.2%), physical harm (31.2%), followed by aggressor FV/criminal history (27.4%). Of note, many other factors were low in frequency, with only 14 factors being present in more than 15% of cases. On an average, there were 6.51 factors present in each case (range = 1–23, SD = 3.50).
ISR Factor Frequency by ISR Risk Category.
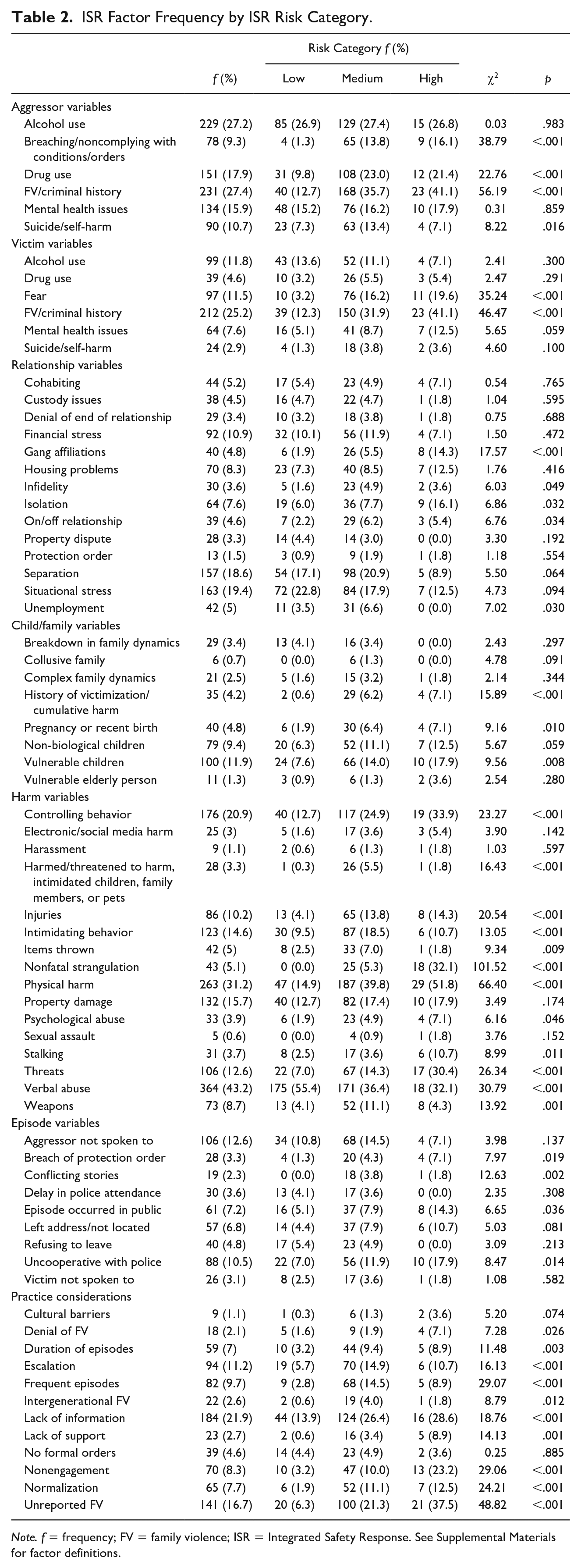
Note. f = frequency; FV = family violence; ISR = Integrated Safety Response. See Supplemental Materials for factor definitions.
The final two columns of Table 2 show χ2 statistics for the relationship between the presence of each factor and the risk categories. More than half of the χ2 statistics were statistically significant at α = .05, indicating that most of the factors appeared in different proportions across the three risk categories, with the overall trend being that factors were more commonly present in higher risk cases compared with low-risk cases. These χ2 statistics should be interpreted with caution because there is a high chance of false positive results given the large number tests conducted, and we include them simply to illustrate the overall pattern of results.
Table 3 shows relatively few of the factors triage teams recorded were associated with recurrence or physical recurrence. In order from largest to smallest associations, frequent episodes, financial stress, housing problems, nonengagement, aggressor drug use, controlling behavior, escalation, items thrown, victim FV or criminal history, victim mental health issues, and victim drug use were positively associated with recurrence. On the other hand, injuries, physical harm, and aggressor alcohol use were negatively associated with recurrence. Frequent episodes, financial stress, denial of FV, episode occurred in public, items thrown, on/off relationship, housing problems, escalation, lack of information, nonengagement, normalization, unemployment, and victim suicide or self-harm were positively associated with physical recurrence, whereas aggressor alcohol use and custody issues were negatively associated with physical recurrence.
Point Biserial Correlations Between the ISR Factors and Recurrence and Physical Recurrence.
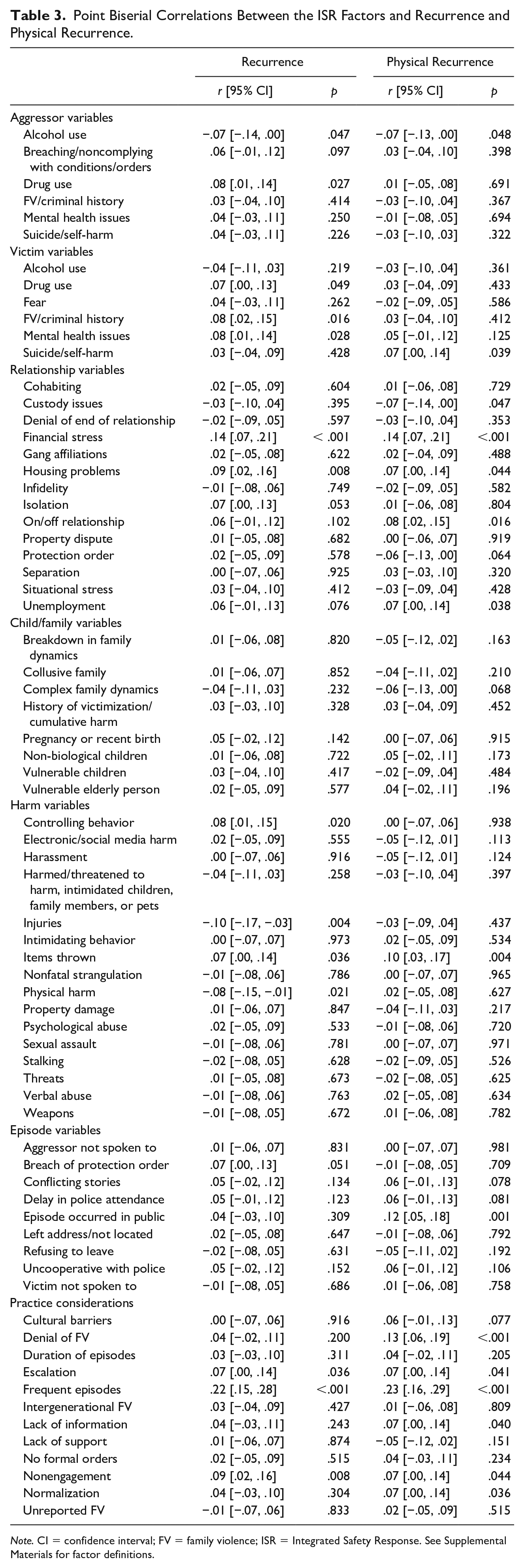
Note. CI = confidence interval; FV = family violence; ISR = Integrated Safety Response. See Supplemental Materials for factor definitions.
Next, we examined the predictive validity of the ISR triage teams’ risk categories. Table 4 shows that overall, the risk categories predicted recurrence and physical recurrence within the 6-month follow-up period better than chance, but the AUCs were small in magnitude (Rice & Harris, 2005). Table 4 also shows that the risk categories predicted recurrence or physical recurrence for all IPV cases, and for cases between current partners, as well as for aggressors who were male, aged above 18 years, or European. Further, the risk categories predicted recurrence for cases between former partners, and when aggressors were aged below 18 years, and predicted physical recurrence for cases where parents were aggressors toward their children. No other AUCs were statistically significant.
AUCs for the ISR Risk Categories Predicting Recurrence and Physical Recurrence, by Aggressor–Victim Relationship, Aggressor Characteristics, and ISR Area.
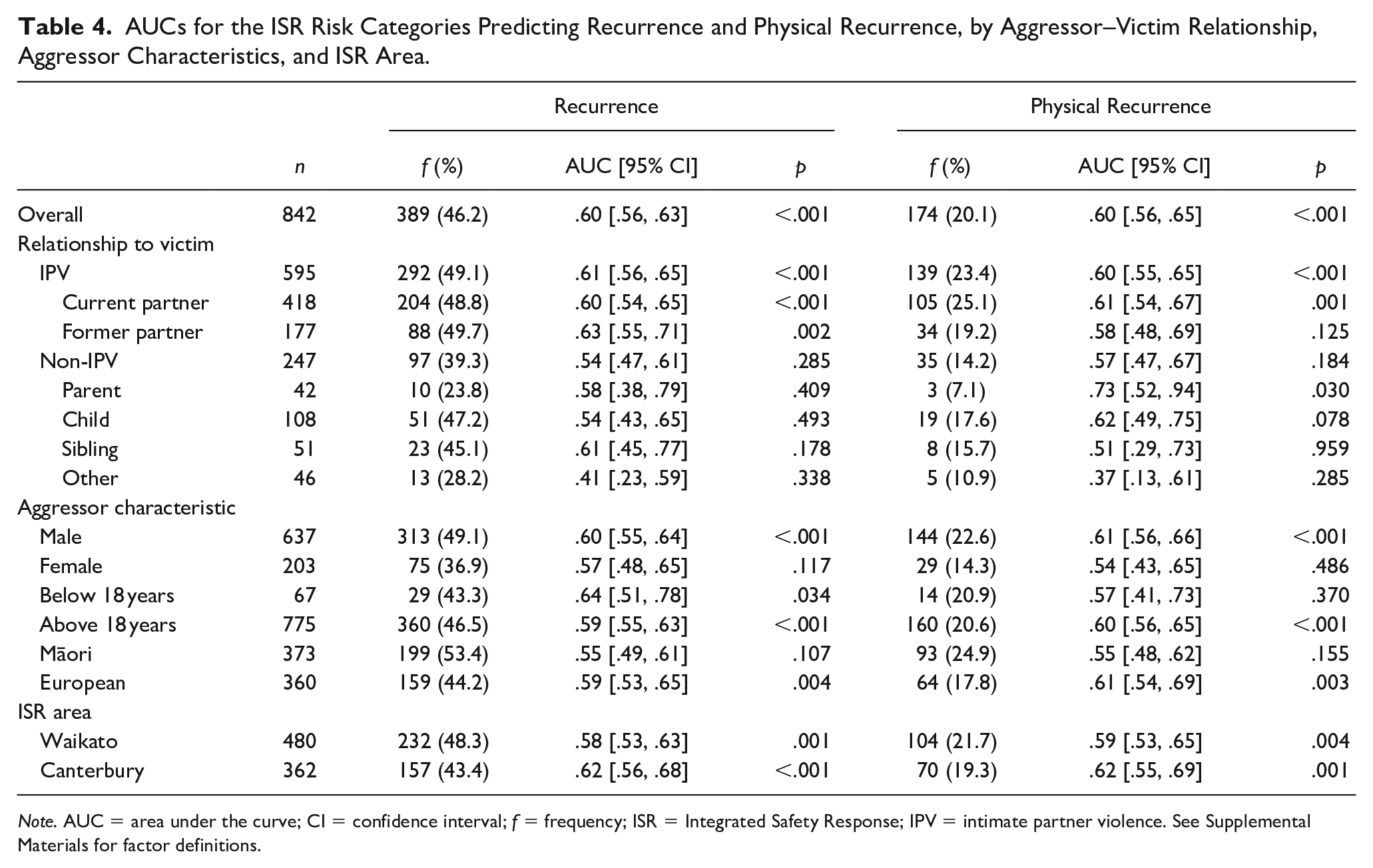
Note. AUC = area under the curve; CI = confidence interval; f = frequency; ISR = Integrated Safety Response; IPV = intimate partner violence. See Supplemental Materials for factor definitions.
Notably, the risk categories were no better than chance at predicting recurrence or physical recurrence for aggressors who were women or Māori, and for non-IPV cases, particularly cases between siblings or people with other types of familial relationships. We speculated that one reason why the risk categories performed better for IPV cases than non-IPV cases was because IPV cases may be more likely to recur with the same victim than non-IPV cases, meaning the victim-related factors recorded in assessments remain relevant. Indeed, of the 292 IPV cases with a recurrence, 266 (91.1%) of the first recurrences recorded were again IPV episodes, with most of those (87.7%) involving the same victim as the index episode. In contrast, of the 97 non-IPV cases with a recurrence, 76 (81.4%) were again non-IPV episodes, but with only 47 (48.5%) involving the same victim.
Discussion
In this study we sought to better understand both the process and the predictive validity of the ISR triage teams’ risk assessments. To fulfill this aim we first documented the factors triage teams listed during their risk assessments and examined the proportions of those factors across the risk categories the triage teams assigned. Overall, most of the 71 factors were associated with the risk categories, with many factors being more common among higher risk cases than low-risk cases. This result may suggest the factors triage teams record are the basis for their risk categorizations, but because factors were recorded after the categorization, it could also suggest that teams retrospectively assign a greater number of risk factors to cases in higher risk categories.
We then examined the association between these factors and two outcomes—recurrence and physical recurrence—to discern whether the identified factors can be used to predict the likelihood of future FV (Bonta & Andrews, 2016). We found that frequent episodes, financial stress, items thrown, housing problems, escalation, and nonengagement were risk factors for recurrence and physical recurrence, suggesting they may be particularly important. For example, when these factors co-occur, they may indicate a particularly volatile family environment in need of intervention to prevent further harm. Moreover, for recurrence, aggressor and victim drug use, victim FV or criminal history, victim mental health issues and controlling behavior were significant predictors. There were also several significant predictors for physical recurrence: denial of FV, on/off relationship, unemployment, lack of information, normalization, and episode occurred in public. But overall, fewer than half of the factors triage teams recorded were associated with recurrence or physical recurrence, in line with previous research showing that many of the items in risk assessment instruments did not predict violence (Coid et al., 2011). The findings from this study also support other research suggesting that specific outcomes may have distinct risk factors (Capaldi et al., 2019; Robinson et al., 2018).
Some of the factors triage teams recorded had negative associations with recurrence or physical recurrence, suggesting they could be protective factors or act as proxies for other mechanisms that prevented recurrence (Eisenberg et al., 2022). For physical recurrence, there were several factors with negative associations, including injuries and physical harm, which seem counterintuitive here. We speculate that their presence in the index episode may have led to ISR agencies to prioritize these cases for interventions that prevented recurrence. In addition, one of the possibilities for why aggressor alcohol use was negatively associated with physical recurrence may be that it was a situational factor that helped to precipitate the index episode and was not a stable characteristic of the aggressor (whereas chronic substance use is a well-established risk factor for FV; Capaldi et al., 2019; Timshel et al., 2017). Furthermore, the factor custody issues was a unique protective factor for physical recurrence, with one explanation being that this factor is commonly present in cases where reported episodes are limited to verbal disagreements over parenting arrangements.
Many of the factors recorded in the triage teams’ assessments may add value to those assessments by highlighting barriers to responsivity and assisting practitioners to deliver interventions in ways that maximize engagement and behavior change (Bonta & Andrews, 2016, Polaschek, 2012, 2016), in addition to (or rather than) contributing to the assessments’ ability to predict recurrence (Butters et al., 2021; Kropp, 2008). For example, nonengagement could indicate a family or whānau has not engaged with FV services in the past, causing practitioners to consider alternative ways to foster that engagement. Some factors that may also measure responsivity (e.g., unreported FV, lack of support) were more common in cases with higher risk categorizations, perhaps due to concerns about managing those cases successfully; high-risk cases tend to be more difficult to manage (Tomkins, 2020).
Finally, we examined the discriminative ability of the ISR triage teams’ risk categories and found they predicted recurrence or physical recurrence better than chance with small effect sizes (Rice & Harris, 2005). These AUCs were comparable to the average predictive ability of risk categorizations made using SPJ risk assessment instruments reported in an international meta-analysis of instruments used to predict IPV (mean AUC of .58; van der Put et al., 2019). However, when we investigated the predictive ability of the risk categories for different subgroups based on aggressor–victim relationship and aggressor characteristics, we found that they performed poorly for aggressors who were Māori, or women, and for non-IPV cases. This result echoes previous research on the predictive validity of New Zealand Police’s FV risk assessment instruments, which also performed poorly for women, Māori and non-IPV cases of FV (Jolliffe Simpson et al., 2021).
The finding that the risk categories performed more poorly for non-IPV cases than IPV cases was not surprising. By far the most dominant and widely researched form of FV is physical IPV within heterosexual adult couples, with women as the primary victims; this was also the most common type of FV in our sample. While coding factors, we noticed the triage teams’ assessments were geared toward identifying risk factors for IPV. The risk assessment guide exemplifies this, with an entire section devoted to “relationship risks” (Integrated Safety Response, 2018). Indeed, some of the risk factors that triage teams recorded only applied to IPV (e.g., infidelity, on/off relationship). This characteristic of the assessments is not necessarily bad; but it suggests that research should test existing risk factors’ predictive validity for non-IPV types of FV and answer the question of whether those cases should be assessed using procedures created for IPV cases. Moreover, different types of FV tend to co-occur (Chan et al., 2021); there are additional challenges inherent in assessing risk and responding to families experiencing both IPV and violence against other family members, compared with families experiencing IPV or non-IPV.
That the risk categories performed more poorly when aggressors were women or Māori may be grounds for concern. This result is also unsurprising given most research on risk assessment for FV focuses on men who commit IPV, and there is less research validating risk assessment instruments for women (van der Put et al., 2019). Moreover, there is a lack of research about culturally specific risk factors (Ashford et al., 2022; Mallory et al., 2016), and few instruments have been validated for specific cultural contexts (e.g., Chan, 2012). The poor performance for Māori is especially problematic when considering the ISR’s special commitment to being responsive to Māori communities and including Indigenous service providers (Mossman et al., 2017). However, because we could not account for the level, type, or effectiveness of interventions received after the index episode, it is also possible that interventions were sufficiently effective for these groups to statistically decouple the risk categorizations from the outcomes we measured. Therefore, we need to understand more about what interventions families and whānau receive, and how those services are provided, including whether provision adheres to the RNR principles of effective correctional treatment (Mossman et al., 2017). This examination will enable us to more clearly understand how the triage teams’ assessments inform responses for different groups of people experiencing FV and the extent to which those responses moderate the relationship between the risk categories and recurrence.
Limitations
A clear limitation of this study is how risk factors were recorded. Triage teams freely listed the risk factors they considered relevant to each case, rather than systematically scoring the presence or absence of risk factors from the risk assessment guide. Our observations of the triage team meetings around the time these data were collected and they suggested that most risk factors mentioned in oral discussion by triage team members were recorded in the free-text field in the Family Safety System database; but the teams did not systematically work through and acknowledge or discard each of the risk factors included in the guide. As a result, assessments may not have captured the full range of risk factors present for each case. Because the triage teams typically recorded risk factors after determining the risk category for the case, they may have retrospectively chosen risk factors to justify their categorization. While there was an association between the risk categories and many of the factors, we could not rule out this alternative explanation. This characteristic of their risk assessment process suggests the triage teams’ risk assessment process is relatively unstructured, even though they have a guide that is intended to impose some structure.
In addition, the ISR’s recording procedure meant that to generate data for research we coded the risk factors for each case from a string of text, adding a layer of interpretation and potentially introducing further error that we sought to minimize by measuring inter-rater reliability. Because the triage teams did not score items but simply noted their presence, we also could not infer items’ weightings. Many SPJ risk assessment instruments (e.g., HCR-20; Douglas et al., 2013; SARA; Kropp & Hart, 2015) allow practitioners to weight items (usually from 0 to 2), indicating the degree to which they are relevant and present for the case in question. Some research shows risk factors indicating the potential for serious harm such as weapons, injuries, escalation, and fear may be weighted more strongly by practitioners when they assess risk, compared with other risk factors like custody issues, unemployment, and non-biological children (Perez Trujillo & Ross, 2008; Robinson & Howarth, 2012; Robinson et al., 2018). This weighting of factors is an important aspect of risk assessments that we could not investigate here. Increased structure in the ISR’s risk assessment protocol such as requiring triage teams to formally identify risk factors from the risk assessment guide before their categorization may increase transparency of their decision-making and ensure risk factors are used as the basis for risk categorizations. Moreover, greater transparency would enable formal validation of the triage teams’ risk assessments and may help identify which factors triage teams consider most strongly in their assessments.
We also could not account for interventions following the index episode that may have prevented FV recurrence, and thus moderated the association between the categorizations and recurrence. For example, a high-risk family could engage intensively with effective services and reduce their level of risk substantially. By contrast, a family at medium risk may not be offered or engage with any services. As a result, the initially high-risk family may now be at lower risk than the medium-risk family, weakening the relationship between the pre-intervention risk category and FV outcomes. The ISR was developed to coordinate interventions delivered to families experiencing FV and all cases are assigned at least one intervention (Integrated Safety Response, 2019), although not all families engage with what is offered. Thus, further research that accounts for the number, intensity, and effectiveness of those interventions is necessary before we can fairly evaluate the triage teams’ risk categorizations.
Implications
The results of this research indicate that the ISR triage teams’ risk assessment protocol may benefit from increased structure and validation. We were not able to investigate the predictive validity of the guide created for triage teams’ assessments because it was not used systematically. Therefore, encouraging practitioners to complete the guide may help in improving their assessments, by (a) helping them to systematically consider the presence of all risk factors in the guide, rather than just those that come to mind; (b) creating data that can be used to validate the risk factors more rigorously than what was possible here; and (c) producing weightings that indicate which factors contributed most strongly to their risk categorization. This information would lend itself to the systematic identification of a subset of risk factors associated with recurrence, and an optimal algorithm for combining those factors thus, creating an improved model to guide ISR triage teams’ decision-making.
Conclusion
In this study we documented and examined the ISR triage teams’ factors and risk categorizations for 842 cases, to better understand both the process and the predictive validity of the teams’ risk assessments. Taken together, the results indicate ISR triage teams consider a wide array of factors when assessing risk in a relatively unstructured way. Moreover, many of the factors triage teams recorded were not associated with recurrence or physical recurrence, and the risk categories’ predictive validity varied across subgroups, performing particularly poorly when aggressors were Māori, or women, and for non-IPV cases. Therefore, the triage teams’ risk assessment protocol may benefit from increased structure and validation. Future research should also measure the interventions cases are allocated and engage with, to find whether those interventions mitigate risk for the recurrence of FV.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605221147069 – Supplemental material for Unpacking Multiagency Structured Professional Judgment Risk Assessments for Family Violence
Supplemental material, sj-docx-1-jiv-10.1177_08862605221147069 for Unpacking Multiagency Structured Professional Judgment Risk Assessments for Family Violence by Apriel D. Jolliffe Simpson, Chaitanya Joshi and Devon L. L. Polaschek in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We would like to thank Josephine Ryan, the Integrated Safety Response, and New Zealand Police for supplying the data for this article. We also acknowledge the University of Waikato and the William Georgetti Scholarship for the financial support provided to the first author.
Authors’ Note
Chaitanya Joshi was affiliated with the School of Computing and Mathematical Sciences at the University of Waikato at the time of the research and is currently affiliated with Department of Statistics at the University of Auckland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Notes
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.