
Abstract
While there has been a growth in studies examining sexual violence among sexual minority men, little research attention has been paid to the experience of sexual violence among young sexual minority men (YSMM). In this article we analyze secondary data from the baseline of a pilot randomized control trial with 318 YSMM aged 15 to 24 years in the United States who were in relationships with other males to examine the associations between sexual minority-specific stigma and sociodemographic and relationship characteristics and experiences of intimate partner violence (IPV) and sexual IPV in their relationships. Approximately one-in-five participants reported experiencing any form of IPV and 6% reported sexual IPV in their current relationship. Participants who reported sexual minority-specific familial rejection (Adjusted Odds Rato (aOR) = 2.33, 95% confidence interval [CI] [1.03, 5.26], p < .05), internalized heterosexism (aOR = 3.17, 95% CI [1.45, 6.95], p < .01), and housing insecurity (aOR = 7.22, 95% CI [1.66, 31.34], p < .01) reported higher odds of sexual IPV in their relationship. Study findings point to the role of multiple sexual minority-specific forms of stigma in creating vulnerabilities for the experience of sexual IPV among YSMM, and highlight the need for continued research and interventions that address sexual minority-specific stigma and structural vulnerabilities to guide violence prevention efforts with YSMM.
Introduction
There is now a significant body of research demonstrating that sexual minority adult men (i.e., men who identify as gay, bisexual, or who are attracted to, or who have sex with, other men) experience rates of intimate partner violence (IPV) that are not only comparable to those experienced by heterosexual women, but are significantly higher than those experienced by heterosexual men (Finneran & Stephenson, 2013). To date, only one IPV measure has been developed and validated with sexual minority men (Stephenson & Finneran, 2013); however, studies using measures of IPV originally developed and validated for heterosexual populations have demonstrated high and widely varied rates of IPV among sexual minority men in the United States. For example, one systematic review identified that the estimated prevalence for experiencing IPV among sexual minority men ranged from 12 to 45% for physical IPV (Finneran & Stephenson, 2013). The high levels of IPV experienced by sexual minority men are particularly important given evidence demonstrating a link between IPV and risk for HIV acquisition and transmission (Buller et al., 2014; Edwardset al., 2015; Kalichman et al., 2001; Stults et al., 2015; ).
Despite growing evidence demonstrating the high levels of IPV among sexual minority men and its associations with physical and mental health outcomes (Blosnich & Bossarte, 2009; Buller et al., 2014; Finneran & Stephenson, 2014), there has been a dearth of research that has focused on the experience of IPV among young sexual minority men (YSMM) in their first relationships. The few existing studies focused on experiences of IPV among sexual and gender minority youth has found rates of IPV to range between 10 and 89%, depending on the form of violence (Halpern et al., 2004; Zweig et al., 2013). For example, among a sample of 117 youth who reported exclusively same-sex romantic relationships, Halpern et al. (2004) found that 25% had experienced any psychological or physical IPV, while about 10% had experienced physical IPV from partners. High levels of IPV among sexual minority youth have been further identified in studies showing an estimated 59% experienced psychological IPV (Zweig et al., 2013), 17 to 89% experienced physical IPV (Dank et al., 2014; McLaughlin et al., 2012; Zweig et al., 2013), and 23 to 61% experienced sexual IPV victimization (Dank et al., 2014; Zweig et al., 2013). These rates of IPV appear to continue into young adulthood: compared to heterosexual college students, sexual minority students are at 2 to 3 times higher risk for psychological and physical IPV, and 5 times the risk for sexual IPV by a romantic partner (Porter & Williams, 2011). Evidence has also suggested that sexual minority young adults are also more likely than their heterosexual counterparts to have been in a recent intimate relationship that was emotionally, physically, or sexually abusive (Blosnich & Bossarte, 2009). Analyses of several probability samples have found sexual orientation disparities in IPV among high school students in both recent (Kann et al., 2016; McLaughlin et al., 2012) and lifetime victimization in the United States (Freedner et al., 2002; Reuter et al., 2015). In addition to reports of IPV, compared to heterosexual and cisgender youth, sexual and gender minority adolescents are more likely to experience sexual and physical dating violence (Martin-Storey, 2015). In a study among high school students, boys questioning their sexual identity reported higher rates of physical dating violence compared with bisexual boys and reported higher rates of sexual dating violence when compared to lesbian girls, gay boys, and bisexual boys (Edwards, 2018). A 2014 survey of 7th to 12th grade students in the mid-Atlantic—including 229 lesbian, gay, bisexual (LGB), and 18 transgender youth—showed that LGB youth were more likely than heterosexual youth to experience physical violence (42.8 vs. 29.0%), psychological abuse (59.2 vs. 46.4%), online dating abuse (37.2 vs. 25.7%), and sexual coercion (23.2 vs. 12.3%) from a dating partner (Dank et al., 2014).
Sexual minority communities experience high rates of sexual violence in their relationships (e.g., forced sex); sexual minority women experience rates of sexual IPV at rates considerably higher than heterosexual women (Balsam et al., 2011; Goodenow et al., 2008; Hughes et al., 2010) and these rates are highest during adolescence (Scheer et al., 2021). Tornello et al. (2014) found that young sexual minority women were 3 to 6 times more likely than heterosexual female youth to experience sexual IPV in their relationships and there is emerging evidence that these disparities may also exist for sexual minority men (Kann et al., 2016; Walters et al., 2013). In a qualitative study with young, partnered sexual minority men from ages 15 to 19 years, Stephenson et al. (2021) found that experiences of sexual IPV were described along with struggles around talking about sexual consent and establishing consent with sexual partners. Participants discussed feeling “uncomfortable” with their own or their partners’ lack of verbal consent during sex and feeling coerced into unwanted sex. However, there has been limited studies focused on understanding the prevalence and potential correlates of sexual IPV among YSMM.
Stigma related to sexual identity—either experienced internally as negative beliefs about being gay or bisexual or attracted to men, or externally as discrimination—has shown to be an important correlate of IPV for adult sexual minority men. The relationship between sexuality-based stigma and IPV has been documented in studies of adult sexual minority men and women (Carvalho et al., 2011) and has been recently shown to predict IPV among sexual minority youth (Stults et al., 2021). Sexuality-related stigma may create lowered self-esteem among sexual minority youth, shaping their perceptions of what should be tolerated in relationships and shaping their beliefs regarding their ability to interrupt cycles of violence (Stults et al., 2021).
The purpose of this article is to explore the correlates of IPV and sexual IPV, including sexual minority-specific stigma, sociodemographic factors, and relationship factors among YSMM. Understanding how YSMM experience IPV in their relationships is vital for the design of interventions that address sexual violence in this underserved and high-risk group.
Methods
Participants and Procedures
Data for the current secondary analysis are taken from an ongoing pilot randomized controlled trial of a relationship-focused HIV prevention intervention (We Prevent) for young, partnered sexual minority men residing in the United States (Gamarel et al., 2019). Recruitment of participants consisted of placing advertisements on social media websites (e.g., Facebook, Instagram, Jack’d). Recruitment advertisements featured photos of young same-sex male couples representing a range of race/ethnicities. People who clicked on the advertisement were then directed to a study screener webpage that provided basic information about the study and participants were asked to complete a brief survey to determine their eligibility. To be eligible, participants needed to be (1) between the ages of 15 and 24 years; (2) identify that they are in an emotional and/or sexual relationship with another man; (3) assigned male on their birth certificate and currently identify as male or transgender man with an intention to have sex with men; (4) report that they have engaged in any sex (oral, anal, vaginal) in their lifetime; (5) meet the age of sexual consent in their state of residence; (6) have access to a personal device with internet access within their home; (7) self-report being HIV negative or unknown serostatus; (8) speak and read English; and (9) be a resident in the United States. Although relationship status was an eligibility criterion, the study did not enroll both members of a dyad. A waiver of parental consent to screen and enroll those under the age of 18 years was approved by the University of North Carolina-Chapel Hill Institutional Review Board: requiring parental consent poses a risk for revealing same-sex behaviors or identities to parents. Participants completed online surveys at baseline, 3, 6, and 9 months. The current analysis uses data from the baseline survey. Enrollment for We Prevent occurred between December 2019 and September 2020. In total, 318 participants enrolled and completed the baseline survey.
Measures
Intimate partner violence
Our two main outcomes of interest were (1) experience (victimization) of any IPV in their current partnership and (2) experience (victimization) of sexual IPV in their current partnership. These constructs were measured using the abbreviated IPV-GBM Scale, adapted from the Conflict Tactics Scale, to assess IPV among GBMSM (Stephenson & Finneran, 2013). Experience of IPV was measured with a 6-item scale that included items of physical IPV (e.g., whether their partner had punched, hit, slapped, kicked, pushed, or shoved them, or other threats of violence or physical intimidation) (sample Cronbach’s α 0.84); emotional IPV (e.g., felt afraid, threatened, isolated, trapped or like you were walking on eggshells within your relationship; insulted, criticized, threatened, or yelled at you in any way) (sample Cronbach’s α 0.76); monitoring and controlling IPV (e.g., prevented you from communicating with or seeing your friends/family/coworkers, or monitored or demanded access to your cell phone, email, social networking sites, finances, or spending) (sample Cronbach’s α 0.81); and sexual IPV (e.g., forced them to do something sexual against their will, pressurized them to have sex without a condom after being asked to use a condom) (sample Cronbach’s α 0.91). Each participant’s responses were dichotomized into “yes” and “no” for all experiences of IPV and the two sexual IPV items.
Sociodemographic, relationship, and behavioral characteristics
Participants reported their age, race, and ethnicity, gender identity, sexual identity, food insecurity, housing status, educational status, relationship length, sexual agreement, and relationship term (e.g., boyfriend, lover, fuck buddy, hook up). Due to small numbers of people of color, race was categorized White, Black, multiracial, and “other” (which included Asian, Native American/Alaskan Native, Native Hawaiian/other Pacific Islander, and other). Sexual identity was categorized as gay, bisexual, and “other” (which included queer, questioning, pansexual, asexual, other). Similarly, most participants identified as cisgender men (assigned male sex at birth and currently identify as male gender) therefore, we created a dichotomous variable such that gender identity was categorized as cisgender men versus transmasculine or nonbinary. Additionally, relationship status was categorized into a dichotomous variable in which more formal terms (boyfriend/lover/husband/partner/significant other) were coded as 1 and more informal terms (fuck buddy/hook up/friends with benefits/we don’t use labels) were coded as 0. Participants were also asked a series of questions about their sexual behaviors in the past 90 days by relationship status. Specifically, participants were asked to report the number of times that they had engaged in different sexual behaviors with or without a condom (e.g., anal insertive, anal receptive) with a main partner or any casual partners. We created two dichotomous variables of any condomless anal insertive or receptive sex with a main partner (Yes/No) or any anal sex with casual partner (Yes/No). Finally, participants completed a 16-item general communication style questionnaire (Kurdek, 1994), designed to assess patterns of behavior during couples’ attempts to resolve disagreements (example items: “focusing on the problem at hand,” “discussing differences constructively”). The scale captures conflict engagement and withdrawal behaviors. Items were mean scored and higher scores indicate more behavioral conflict. The communication scale demonstrated good psychometric properties in our sample (sample α = 0.88).
Sexual minority-specific stigma
Participants completed three measures of sexual minority-specific stigma, specifically internalized heterosexism, discrimination, and sexual minority-specific family rejection. Participants completed the 8-item measure of internalized heterosexism, which was validated with YSMM (Puckett et al., 2017). Items were mean centered where higher scores indicate more internalized heterosexism (example item: “Sometimes I wish I wasn’t gay”). The internalized heterosexism scale demonstrated excellent internal consistency in our sample (sample α = 0.90). Participants completed the 9-item Everyday Discrimination Scale to assess the frequency with which participants experienced various forms of interpersonal mistreatment in their day-to-day lives over the previous 12 months (Williams et al., 1997). The discrimination scale also demonstrated high internal consistency reliability (sample α = 0.92). Discrimination scale items were scored such that higher scores indicated more experiences of everyday discrimination (example item: “Treated with less respect”). Participants completed an 8-item family rejection scale, which was originally developed for sexual minority adolescents (Ryan et al., 2010). These responses were then mean centered using all available data with higher values indicating more family rejection due to one’s sexual minority status (example item: “Says bad things about LGBTQ people in general”; “Taunts or mocks you because an LGBTQ person”). The sexual minority-specific family rejection scale demonstrated good internal consistency in the sample (sample α = 0.85).
Data Analysis
Descriptive statistics were calculated for all variables in the bivariate analyses, which included examining the distribution of scale scores with appropriate tests for normality. We then fit a series of independent samples t-tests and χ2s to examine whether there were bivariate differences in sociodemographic, relationship, and sexual minority-specific stigma variables by the reporting of sexual IPV and any IPV. Finally, we fit two multivariable logistic regression models to assess whether sociodemographic, relationship, and sexual minority-specific stigma factors were associated with the reporting of sexual IPV or any IPV, controlling for significant covariates identified in the bivariate analyses. Levels of data missingness were very low (<5%) and did not vary by demographic or behavioral characteristics. Statistical analysis was conducted using SPSS.
Results
Descriptive Characteristics of the Sample
Table 1 presents the characteristics of the sample and bivariate comparisons by sexual IPV and any IPV. Overall, 6.9% (n = 22) reported experiencing sexual IPV and 20.1% (n = 64) reported any experience of IPV. Participants ranged in age from 15 to 25 years (M = 20.50, SD = 2.37). Most of the sample identified as White (70.4%), cisgender male (74.5%), and gay (72.2%). In total, 28.9% reported food insecurity in the past 3 months, 7.2% reported some form of housing instability in the past 30 days, and nearly two-thirds were currently in school. Participants varied in terms of relationship length where 31.1% had been in the relationship for less than 3 months, 26.7% for 4 to 11 months, and 42.1% for 1 year or more. The majority of participants reported that they had a monogamous sexual agreement (53.8%) or an open sexual agreement (35.0%). Participants reported a range of relationship terms with “boyfriend” being the most commonly endorsed one by over half of the participants. Regarding sexual behavior, 84.1% reported anal sex with their current partner with over half reporting condomless anal sex (51.6%) and less than one-third reported having anal sex with other partners (30.6%).
Sociodemographic and Relationship Characteristics of Sexual and Any IPV for the Sample of Young, Gay, Bisexual, and Other Men Who Have Sex With Men (N = 318).

Note. MP = main partner; CAS = condomless anal sex; IPV = intimate partner violence.
p < .05. *p < .01. ***p < .001.
Bivariate Differences by IPV Experiences
A greater proportion of participants who reported housing instability reported sexual IPV, χ2(1) = 14.15, p < .001, and any IPV, χ2(1) = 20.43, p < .001. A higher proportion of those who reported any anal sex with their current partner reported sexual IPV, χ2(1) = 5.26, p < .05. Those who had experienced sexual IPV and any IPV reported higher negative communication compared to those who did not report IPV, sexual IPV, t(315) = 3.15, p < .01; any IPV, t(316) = 6.29, p < .001. Regarding sexual minority-specific stigma, those who reported sexual IPV and any IPV reported higher internalized heterosexism compared to those who did not report IPV, sexual IPV, t(316) = 4.55, p < .001; any IPV, t(316) = 3.93, p < .001. Those who reported sexual IPV and any IPV also had higher sexual minority-specific family rejection scores compared to those who did not report any IPV, sexual IPV, t(316) = 2.74, p < .05; any IPV, t(316) = 2.24, p < .05.
Multivariable Analyses of IPV Experience
Results of the two multivariable logistic regression models are presented in Table 2. Participants who were unstably housed reported increased odds of any sexual IPV (aOR = 7.22, 95% confidence interval [CI] [1.66, 31.34], p < .01). Participants who had been in a relationship for 3 months or less (aOR = 0.17, 95% CI [0.04, 0.80], p < .05) had reduced odds of experiencing sexual IPV compared to those who had been in a relationship for 1 year or longer. Participants who used formal relationship terms had reduced odds of sexual IPV (aOR = 0.23, 95% CI [0.07, 0.78], p < .05) compared to those who used informal terms. In terms of sexual minority-specific stigma, greater internalized heterosexism (aOR = 3.17, 95% CI [1.45, 6.95], p < .01) and sexual minority-specific family rejection (aOR = 2.33, 95% CI [1.03, 5.26], p < .05) were each associated with increased odds of sexual IPV. Model 2 presents the results predicting any IPV. Similar to sexual IPV, reporting unstable housing was associated with increased odds of any IPV (aOR = 6.06, 95% CI [1.92, 19.08], p < .01). Higher negative communication scores were associated with increased odds of any IPV (aOR = 4.67, 95% CI [2.35, 9.26], p < .001). Finally, sexual minority-specific family rejection was associated with increased odds of reporting any IPV (aOR = 1.10, 95% CI [1.01, 2.10], p < .05).
Multivariable Logistic Regression Models of Sexual and Any IPV for the Sample of Young, Gay, Bisexual, and Other Men Who Have Sex With Men (N = 318).
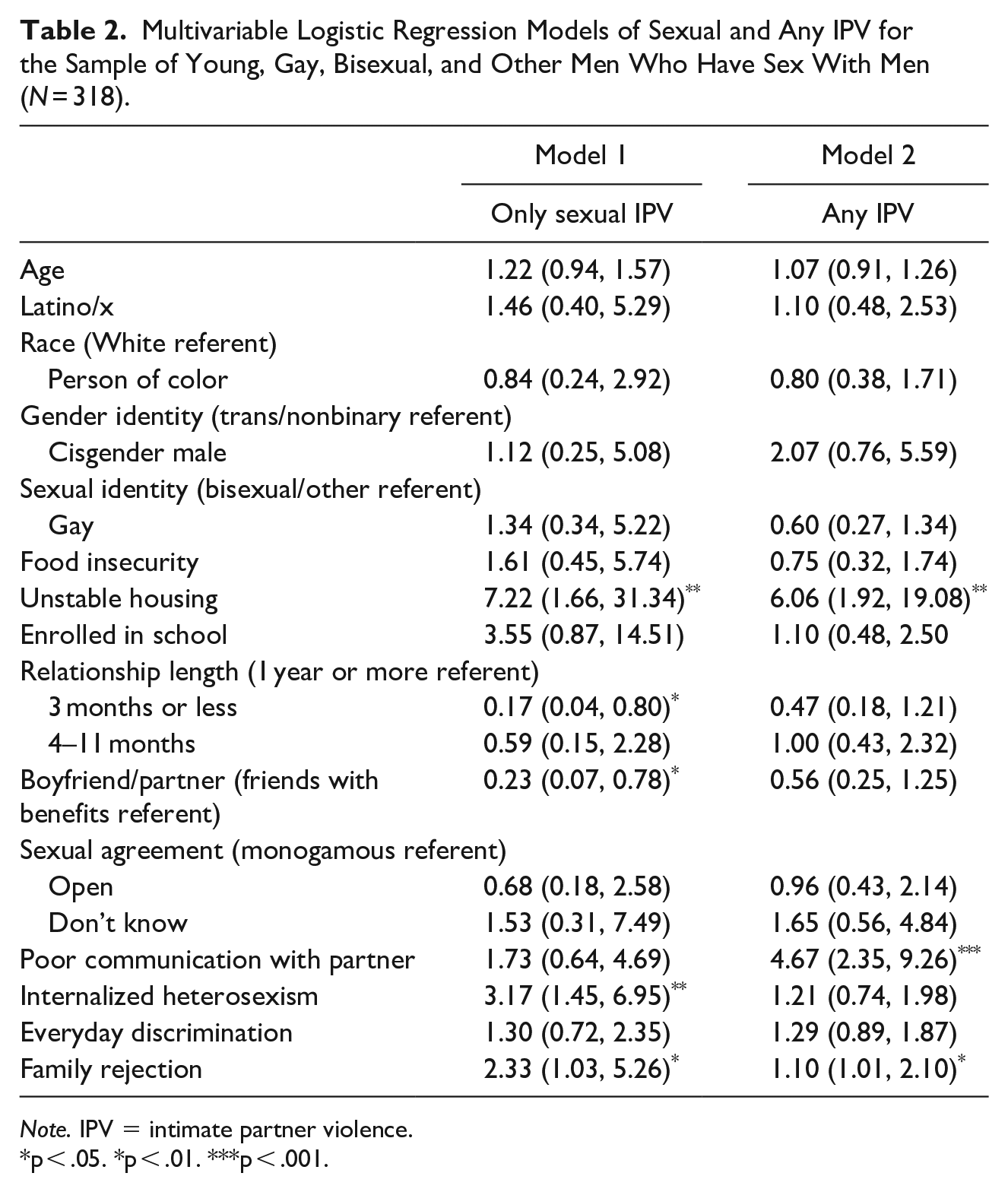
Note. IPV = intimate partner violence.
p < .05. *p < .01. ***p < .001.
Discussion
Our study explored the correlates of IPV and specifically sexual IPV among a sample of young, partnered sexual minority men in the United States. Approximately one-in-five participants reported a recent experience of any form of IPV in their current relationship, and although less frequently reported, [a not insignificant] 6% of participants reported a recent experience of sexual violence in their current relationship. In multivariable models, sexual minority-specific stigma and structural vulnerabilities, specifically unstable housing, was associated with higher likelihood of experiencing IPV in this sample of YSMM in relationships. These findings extend prior literature with sexual minority women (Balsam et al., 2011; Goodenow et al., 2008; Hughes et al., 2010) but also underscore the necessity of accounting for the unique social and developmental context that contribute to experiences of IPV among YSMM.
Although our analyses indicated that both increased sexual minority-specific and family rejection were each independently associated with increased IPV and sexual IPV, family rejection and housing instability may be synergistic (Durso & Gates, 2012). That is, rejection from families of origin may lead to the experience of housing instability for sexual minority youth. Evidence suggests that many sexual minority youth report parental disapproval of their sexual orientation as the main reason for their homelessness (Durso & Gates, 2012). The associations between housing instability and an increased risk of violence have been well documented among heterosexual women. For example, a study of 3619 women in California found women reporting IPV were four times more likely to also report housing instability (Pavao et al., 2007), and approximately one-in-four homeless women cite IPV as a major contributor to their homelessness (Jasinski et al., 2005). The combination of familial rejection and housing instability may put YSMM at risk for IPV, increasing their dependency on abusive partners, limiting their options to leave abusive relationships, and diminishing their ability to negotiate or control the circumstances around sex. The experiences of familial rejection and homelessness may also adversely impact self-esteem and the sense of future self among YSMM. Being rejected from families of origin and the potential trauma associated with homelessness may lead to reductions in resiliency and self-esteem among YSMM, increasing their susceptibility to IPV and reducing their ability to remove themselves from abusive relationships.
YSMM who reported increased levels of internalized heterosexism also reported increased odds of sexual IPV, an association that has been identified among adult sexual minority men (Stephenson & Finneran, 2017). Heterosexist discrimination and sexual orientation concealment have been identified as correlates of perpetration of IPV (Edwards & Sylaska, 2013; Lewis et al., 2017). The negative health outcomes associated with experiencing sexual minority-specific stigma (e.g., mental health and substance use) are known to be linked to increased risk of IPV perpetration and victimization, and therefore, it seems reasonable that the experience of sexual minority-specific stigma may also lead to increases in IPV through creating tension, poor communication, lowered self-esteem, and the adoption of maladaptive behaviors in relationships. Previous studies suggest experiences of sexual minority-specific stigma can evoke feelings of anxiety, shame, and victimization, resulting in self-devaluation (Kubicek et al., 2015). It is possible that chronic victimization and self-devaluation resulting from sexual minority-specific stigma—in this case high levels of internalized heterosexism—could predispose YSMM to experiences of sexual IPV. For example, internalized heterosexism has been linked to poor relationship quality (Frost & Meyer, 2009) and a decrease in couples’ beliefs in their ability to adequately communicate and make joint decisions (Stachowski & Stephenson, 2015). Heterosexism may produce added stress on the relationships of YSMM (Kubicek et al., 2015); thus, future research is warranted to identify the pathways through which sexual minority-specific stigma is associated with experiences of IPV.
Interestingly, YSMM who referred to their partners in more formal terms (i.e., boyfriend) and those who were in relationships for less than 3 months reported lower odds of IPV (although the lower odds of IPV in shorter relationships may reflect less time for IPV to have occurred). Reporting a more formal relationship term may signal either greater levels of positive communication—with formal relationship terms agreed upon through communicating—or greater levels of trust and commitment within these relationships. Higher levels of positive relationship qualities have been shown to be associated with lower levels of IPV among adult sexual minority men (Finneran & Stephenson, 2014) (Stephenson et al., 2013). Lower levels of sexual IPV among those early in their relationships—less than 3 months—may represent a “honeymoon” period in a relationship, in which levels of love and intimacy are highest. Alternatively, a large portion of the data collection occurred during the COVID-19 pandemic, and it may be that many YSMM may not have been able to spend time with their partners, and those in very early relationships may have had limited contact, and therefore limited opportunities for IPV to occur.
Limitations
The study findings should be interpreted within the context of several limitations. It is plausible that experiences and forms of IPV may be underreported, which necessitates future research to better understand and explicitly address experiences of IPV among YSMM. In particular, Stephenson et al. (2021) found that YSMM often struggled with defining sexual IPV, and thus participants may be misreporting or underreporting IPV based on their definitions of what constitutes sexual violence. Participants were recruited online using convenience sampling methods, which has important implications for generalizability. We most likely were not able to reach youth experiencing significant structural vulnerabilities (e.g., homelessness, incarceration). Recall bias may have shaped the reporting of relationship details. Most importantly, only one member of the dyad completed the survey, which is standard practice when collecting data on IPV to protect the safety of the participant; however, this precluded a dyadic understanding of how relationship contexts shape the risk for IPV among YSMM. The large confidence intervals around some estimates—particularly for housing instability—underscore the need for data from larger samples of YSMM to fully explore these issues. The sample was also predominantly White cisgender men; therefore, research is warranted with more racially and ethnically diverse samples, as well as young gender minority men, to understand how intersecting identities shape the risk for IPV.
Conclusions
Results from this study demonstrate high levels of IPV, in particular sexual IPV, among YSMM in their current relationships and demonstrate an urgent need for interventions that address the multiple factors that make YSMM vulnerable to IPV. Negative experiences associated with sexual identity—including familial rejection, homelessness, and internalized heterosexism—may place YSMM at greater risk of sexual IPV. The results point to two potential areas for intervention efforts. First, family-based interventions are needed to reduce familial rejection of sexual minority youth (Huebner et al., 2013) and may have the potential to also lead to reductions in IPV. Thus, future research attention is needed to explore the potential for family-based strategies as violence reduction interventions. Second, culturally appropriate services are needed to meet the specific needs of sexual minority youth. Previous studies have highlighted that sexual minority individuals, particularly youth, experience multiple economic and administrative barriers in accessing violence prevention and treatment services (i.e., domestic abuse shelters) (Calton et al., 2016; Ford et al., 2013). Calton et al. (2016) note that in addition to the need to create culturally appropriate and accessible violence-related services for sexual minorities, there is a need to make these barriers visible and to ensure that violence and barriers to existing services continue to be in the scientific discourse. Our study findings offer preliminary insights regarding the correlates of sexual IPV among a large sample of YSMM and highlight the need for continuing to examine these issues with larger and more diverse samples of YSMM.
Footnotes
Acknowledgements
The authors would like to thank the young men who participated in this study; and staff members Matthew Rosso, Kristina Felder Claude, Ramona Rai, and Elizabeth Adam for their contributions to this study. The authors are also grateful to Dr. Sonia Lee for her support of this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by a grant from the National Institutes of Health (U19HD89881).