
Abstract
Sexual violence (SV) is a stigmatized form of trauma, yet the stigma experiences of those reporting SV are often assumed rather than explicitly measured. We adapted a measure that quantified three key features of SV stigma across three levels: negative self-image (individual), disclosure concerns (interpersonal), and concerns about public attitudes (structural). We administered this measure to a population-based sample of Swedish young adults (N = 453) who reported a history of either sexual assault (SA) or intimate partner sexual violence (IPSV). Among both groups, 89% endorsed at least one item on the stigma scale. Experiences of SV-related stigma were associated with significantly higher symptoms of generalized anxiety, depression, and posttraumatic stress disorder, with greater perceived need for mental health treatment, and with more shame (measured implicitly via a reaction-time task). Experiences of stigma were negatively associated with symptoms of alcohol misuse. Results suggest that exposure to SV stigma may be a critical, but often overlooked, correlate of post-assault recovery.
Introduction
Sexual violence (SV) is an umbrella term that refers to any act or attempt to obtain a sexual act by violence or coercion and includes behaviors such as rape and sexual assault (SA) (Rutherford et al., 2007). SV can also occur in romantic relationships as one of a constellation of behaviors associated with intimate partner violence (IPV), defined as “any form of physical, sexual, emotional, psychological, and/or verbal abuse between [current or former] partners in an intimate relationships” (Murray et al., 2015, p. 320). Certain groups—including women (Borumandnia et al., 2020) and lesbian, gay, bisexual, and transgender (LGBT) individuals (Chen et al., 2020)—are at heightened risk of experiencing SV in their lifetimes. The relationship between exposure to SV and adverse psychosocial outcomes has been well established (for reviews, see Dworkin et al., 2017; Walsh et al., 2012), and some studies suggest that these consequences may be even more severe for LGBT individuals (Sigurvinsdottir & Ullman, 2016). Compared to other forms of trauma, SV exposure places individuals at especially high risk for a variety of mental health challenges, such as anxiety, depression, posttraumatic stress disorder (PTSD), and substance use disorders (Breslau et al., 1991; Kessler et al, 1999; López-Martínez et al., 2018). A large research tradition has focused on factors that predict the development and maintenance of psychopathology among SV survivors, as well as their treatment utilization and access. These factors include, among others, prior assault history, assault type, assailant type, peritraumatic dissociation, event centrality, and self-blame (Dworkin et al., 2018). Here, we focus on another potentially important risk factor that has received comparatively less attention—namely, stigma.
Stigma, defined as the cooccurrence of labeling, stereotyping, separation, status loss, and discrimination that occurs between groups in a context in which power is exercised (Link & Phelan, 2001), is a well-known determinant of psychosocial distress and poor mental health across multiple stigmatized communities (for reviews, see Hatzenbuehler, 2009; Vigod & Rochon, 2020; Williams et al., 1997). Stigma is a multilevel construct that can be measured at individual, interpersonal, and structural levels (Hatzenbuehler, 2016; Link & Phelan, 2001). Individual-level stigma refers to a person’s cognitive, affective, and behavioral responses to stigma, whereas stigma at the interpersonal level includes discrimination experienced by one person and enacted by another, usually an unstigmatized person (Hatzenbuehler & Pachankis, 2016). Structural stigma has been defined as the “societal-level conditions, cultural norms, and institutional policies and practices that constrain the opportunities, resources and well-being of the stigmatized” (Hatzenbuehler & Link, 2014, p. 2). Structural stigma is measured both objectively, via laws, policies, and institutional practices, and subjectively, via perceptions of structural stigma (e.g., Lattanner et al., 2021). At each level, stigma can be attached to demographic features of a person’s identity (e.g., race, gender, sexual orientation) as well as to conditions that are experienced or acquired throughout the lifespan (e.g., SV, obesity, HIV/AIDS). Like sexism, racism, and homophobia, experiencing stigma related to an acquired condition, such as HIV, results in significant psychological distress and can lead to negative physical and mental health outcomes (Rueda et al., 2016). In the case of SV, stigma may contribute to or exacerbate psychopathology following the experience of SV. Improving our understanding of this type of stigma would not only clarify the challenges faced by survivors working to heal from SV exposure but also potentially help to account for increased incidence and severity of a range of mental health outcomes that exists between individuals who have experienced SV and those who have experienced other forms of trauma (Breslau et al., 1991; Kessler et al, 1999; López-Martínez et al., 2018).
Despite the potential relevance of exploring SV stigma, much remains to be known about whether (and how) it may influence mental health and treatment-seeking among SV survivors, especially during periods of developmental risk for SV. One of the barriers to this work has been the lack of validated measures of SV stigma. Further, those scales that do exist have a number of important limitations. First, some measures only cover one level of stigma, such as perceptions of rape myth acceptance (RMA) (e.g., Payne et al., 1999). Given the multi-level nature of stigma, scales that capture a single level provide a necessarily limited understanding of the full scope of stigma experiences and responses relevant to SV. Second, newer scales that do assess multiple aspects of SV stigma are calibrated to specific types of trauma, such as IPV (e.g., Crowe et al., 2021), or to specific social contexts, such as the Democratic Republic of Congo (Murray et al., 2018). While important, these scales may not generalize to other forms of SV (e.g., SA, rape, childhood sexual abuse) or to other social contexts. Finally, some scales employ gendered language that implies that everyone who experiences SV is a cisgender-female and that all perpetrators of SV are cisgender-males (e.g., Payne et al., 1999), and thus cannot be used with samples of male and LGBT survivors of SV.
The development of these extant scales highlights a growing recognition of the potential importance of the role of stigma in mental health and treatment-seeking outcomes among survivors of SV. However, researchers have yet to develop a scale for SV stigma that could be administered across SV type and context. Further, existing measures have yet to quantify stigma across all three levels (i.e., individual, interpersonal, and structural) in a single scale. Capturing experiences of SV stigma across stigma levels is critical because members of stigmatized groups typically experience stigma across all three levels (Hatzenbuehler et al., 2013; Hatzenbuehler, 2016). Further, stigma levels are interrelated, such that experiences of stigma at one level may amplify experiences of stigma at another level (Hatzenbuehler, 2016; Link & Phelan, 2001). For example, if a survivor has experienced a negative response to their disclosure of SV, they may internalize that stigmatizing interaction and experience an increase in their negative self-image. Therefore, a more comprehensive approach would be to develop measures that capture SV stigma across all three levels and to test these measures as predictors of post-assault psychopathology and treatment-seeking among survivors. In this investigation, we seek to fill this gap in the literature by adapting a scale from the HIV stigma literature (Berger et al., 2001) to capture SV stigma. This scale captures three constructs relevant to SV stigma: negative self-image (individual level), disclosure concerns (interpersonal level), and concerns about public attitudes (structural level).
A small body of previous work has separately measured each of these constructs to evaluate the association between SV stigma and mental health outcomes. For example, individuals who have experienced SV frequently endorse internalization of these stigma experiences (Gibson & Leitenberg, 2001; Maticka-Tyndale et al., 2020; Quinn et al., 2014). This tendency toward internalization (also known as self-stigma) aligns with current cognitive conceptualizations of trauma exposure, which posit that trauma challenges a person’s “just-world” belief and can negatively bias a survivor’s view of themselves, the people around them, and the world, as the survivor attempts to incorporate the traumatic experience into their life narrative (SAMSHA, 2014). Further, a handful of studies have connected internalized SV stigma to various adverse psychosocial outcomes including avoidance-oriented coping strategies (Gibson & Leitenberg, 2001), disclosure (Maticka-Tyndale et al., 2020), and general psychological distress (Quinn et al., 2014). Despite these important contributions, few studies have explored a direct relationship between internalized SV stigma and symptoms of psychopathology. One investigation has observed a positive association between self-stigma and PTSD symptom severity (Deitz et al., 2015). However, some of the items from the self-stigma measure employed in this investigation conflate SV stigma itself with an outcome associated with stigma (i.e., shame).
Much of the work investigating the association between SV stigma and mental health outcomes has focused on interpersonal responses to SA disclosure. These findings have been mixed and are often moderated by interpersonal reactions to the disclosure. In general, SA disclosure has been associated with less severe trauma symptomatology (Orchowski et al., 2013). A positive response to disclosure can increase future support seeking (Ullman & Peter-Hagene, 2014), feelings of control over recovery, and perceptions of support from members of the community (Jonzon & Lindblad, 2004). Negative social reactions, on the other hand, have been associated with psychological distress (Littleton, 2010), abuse of alcohol (Ullman & Peter-Hagene, 2014), depression (Orchowski et al., 2013), and PTSD symptoms (Ullman & Filipas, 2001; Ullman et al., 2007). For sexual minority individuals who experience sexual minority stigma in addition to SV stigma, SV disclosure can be especially risky due to concerns about further sexual minority discrimination as well as peer rejection due to SV stigma that sometimes exists within the LGBT community (Binion & Gray, 2020; Jackson et al., 2017). Concerns about SV disclosure have been connected to reduced treatment-seeking for both mental and physical health services (Gruenfeld et al., 2017; Vranda et al., 2018). Taken together, the disclosure literature suggests that one important way that SV stigma is communicated to survivors is through negative or unsupportive responses to SV disclosure.
Yet, SV disclosure is only one specific instance in which survivors of SV may encounter stigma. Additional work has explored whether perceptions of public attitudes, such as peers’ acceptance of rape myths, known as RMA, are associated with post-SV mental health outcomes. For instance, Paul et al. (2009) found that college students who had experienced SA tended to overestimate the level of RMA among their peers, and that greater estimations of peer RMA predicted increased PTSD symptom severity. These findings suggest that survivors may harbor a high degree of concern about public attitudes towards SV, and that these concerns may exacerbate negative mental health outcomes. Notably, these concerns may originate from survivors’ exposure to negative portrayals of people who have experienced SV in the news, social media, politics, as well as laws and policies. So although survivors overestimated their peers’ acceptance of rape myths in the Paul et al. (2009) investigation, those estimates may be reflective of survivors’ accurate perceptions of a stigmatizing structural environment, though this hypothesis awaits empirical investigation.
Current Study
In this investigation, we adapted a scale to measure individuals’ multi-level experiences with SV exposure. We embedded the new scale into an ongoing population-based longitudinal study of young adults in Sweden. Young adulthood is an age range during which individuals are at particularly elevated risk of experiencing SV, making SV stigma an especially relevant consideration for this group (Breiding et al., 2011). We tested three hypotheses. First, among participants who have experienced SV, we predicted that those who report greater levels of SV stigma would exhibit more symptoms of anxiety, depression, PTSD, and problematic alcohol use.
Our second hypothesis was that those reporting greater levels of SV stigma would index higher levels of shame—an affective outcome that is frequently examined in the SV literature (e.g., Finkelhor & Browne, 1985)—which was operationalized via a behavioral (i.e., reaction time) task. We chose to incorporate an outcome that can be measured behaviorally to circumvent two drawbacks associated with self-report measures. The first is the risk of confounding that can occur when both stigma and stigma-related outcomes of interest (e.g., symptoms of psychopathology) are both measured using self-report. In such cases, it is possible that a person’s experience of their psychopathology symptoms may modulate their reporting of stigma burden, making it difficult to determine causality (Meyer, 2003). Incorporating a novel behavioral task ensured that we had a multi-modal assessment of study outcomes, thereby addressing the limitations of same-source bias (Diez Roux, 2007). A second drawback of self-report measurement approaches applies to the quantification of shame specifically. When quantifying shame via self-report, it is possible that social desirability biases may lead to underreporting. Consequently, shame may be difficult to capture via self-report due to the nature of shame itself (Pachankis et al., in press). Incorporating a behavioral measure of shame circumvents this difficulty.
Third, we predicted that participants who report more SV stigma would report greater perceived treatment need in order to manage their elevated psychopathology symptoms. Furthermore, prior research has shown that internalized stigma among IPV survivors (Overstreet et al., 2017) and among survivors of military sexual trauma (Andresen & Blais, 2019) is associated with lower disclosure. As such, we additionally hypothesized that, despite greater reported treatment need, those who report greater SV stigma burden would also report less actual treatment use, as compared to those reporting lower levels of SV stigma.
Method
Study Design
Data were gathered as part of an ongoing longitudinal investigation, the Pathways to Longitudinally Understanding Stress (PLUS) study. The PLUS cohort is a longitudinal cohort study developed to evaluate psychosocial mechanisms that explain mental health disparities between LGBT and cisgender-heterosexual young adults in Sweden. Participation in the PLUS study was not based on exposure to the constructs of interest (SV, SV stigma) in this investigation. All participants in the PLUS cohort received survey items inquiring about experiences of SV, and those who endorsed a history of SV subsequently received the Sexual Violence-Related Stigma Scale (SVRSS).
Participants in the PLUS study were recruited among respondents to the Swedish National Public Health Survey (SNPHS), a regularly disseminated cross-sectional survey legislated by the Public Health Agency of Sweden and administered by Statistics Sweden. In 2015, 2016, and 2018, nationally representative randomly selected samples were invited using information from the Swedish Total Population Register that contains personal identification and address information of all individuals living in Sweden. By using the comprehensive population register, the sampling frame for the SNPHS includes all individuals living in Sweden at the time of the study. SNPHS participants are invited to complete the questionnaire, which covers health outcomes, health behaviors, and contextual exposures. In the 2015, 2016, and 2018 data collections, one question regarding self-identification of sexual orientation identity was included: “What is your sexual orientation?” with the Swedish-language equivalent of the response categories: “heterosexual,” “bisexual,” “homosexual” (the commonly accepted term in Sweden), “not sure,” and “other.” Most participants (96%) responded to this item.
To create the PLUS cohort, we selected all 2,943 young adult participants (ages 18–34) who reported identifying as non-heterosexual in the 2015, 2016, and 2018 SNPHS. We then selected a random sample of 2,943 heterosexual participants ages 18 to 34 to create our comparison group. A total of 2,222 (37.8%) sexual minority and heterosexual participants provided consent and completed the Wave 1 survey assessment (October 2019). At Wave 2 (October 2020), 1,395 (62.8% of the Wave 1 participants) completed all assessments and, of those, 1,081 (77.5% of the Wave 2 participants) completed the Wave 3 assessments (October 2021). The final analytic sample included participants who were retained at Wave 3.
Respondents completed online batteries of self-report and behavioral measures of internalizing psychopathology, treatment utilization, and experiences with stigma. Although the PLUS database is longitudinal, our analyses of study outcomes were performed on cross-sectional data from Wave 3 because the SV questionnaire was only administered at this time point.
Measures
Sexual Violence
History of SV exposure was measured via self-report. Participants were asked about lifetime experiences of SA using three items from the Kaiser Family Foundation (2015). Questions assessed history of sexual contact by physical force, sexual contact when unable to provide consent, and sexual contact by threat of force or physical harm using three binary (yes/no) questions. Participants who answered yes to at least one of these questions were coded as having a lifetime history of SA.
Additionally, to identify past-year intimate partner sexual violence (IPSV), participants were asked about ongoing SV within romantic relationships using the following question: “During the past 12 months, how many times did someone you were in a relationship with or dating force you to do sexual things that you did not want to do?” Response options included “I did not go out with anyone in the past 12 months,” “0 times,” “1 time,” “2 or 3 times,” “4 or 5 times,” and “6 or more times.” Participants who endorsed at least one experience of IPSV at either Wave 2 or Wave 3 were coded as having an experience of recent IPSV (yes/no).
Sexual Violence-Related Stigma
The SVRSS, which was developed for this study, is a nine-item scale adapted from the well-validated HIV Stigma Scale originally developed by Berger et al. (2001) and abbreviated by Reinius et al. (2017). We chose to adapt the HIV Stigma Scale for several reasons. The first is that SV and HIV share similarities across multiple stigma dimensions, including origin, aesthetics, concealability, disruptiveness, and course (Pachankis et al., 2018). SV and HIV are both experienced or acquired conditions typically originating from a sexual interaction with another person. People who have experienced SV and HIV may be considered “dirty” or “tainted” by the experience (Delker et al., 2020; Reinius et al., 2017), despite both stigmas being partially concealable in nature. Further, both conditions are life course persistent once experienced or acquired, even if resulting physical and mental health symptoms decline over time, and they can disrupt interpersonal relationships after disclosure. Recognizing the overlap between HIV and SV stigma, other researchers in the SV field have also made adaptations to the long version of the HIV Stigma Scale (Eckstein, 2016). However, this adapted measure has only been used with participants who have experienced IPV and has not been examined in connection with the mental health outcomes (anxiety, depression, PTSD, and alcohol misuse) reported in this investigation. The second reason we chose to adapt the HIV Stigma Scale is that the measure allows for assessment of stigma at all three levels (i.e., individual, interpersonal, and structural) within a single scale. Finally, both the 15-item and 40-item versions of the HIV Stigma Scale predict a range of mental health, physical health, and treatment-seeking outcomes among people living with HIV/AIDS (Felker-Kantor et al., 2019; Hojilla et al., 2021; Okawa et al., 2018). Given the strong foundation provided by the HIV Stigma Scale, we adapted this measure to reflect perceived individual-, interpersonal-, and structural-level stigma experiences of people who have experienced SV.
The SVRSS was given only to respondents who indicated that they had at least one lifetime experience of SA or had experienced IPSV during the past 24 months. The scale was designed to quantify three key features of SV stigma across three levels: negative self-image (individual), disclosure concerns (interpersonal), and concerns about public attitudes (structural). Negative self-image was assessed with items such as, “I feel like I am not as good as others because I experienced sexual violence.” Disclosure concerns were assessed with items such as, “Telling someone I’ve experienced sexual violence is risky,” and concerns about public attitudes were assessed with items such as, “Most people feel a person who has experienced sexual violence is dirty.” The full scale is provided in Table 2. The scale was internally reliable in our sample of individuals who experienced SV (Cronbach’s alpha = .86).
We predicted that items in our scale would reflect latent factors associated with their respective subscales, as well as a higher-order latent factor of SV stigma. Accordingly, we conducted a higher-order confirmatory factor analysis of the SVRSS (Appendix 1). Factor loadings in our model are standardized. Results of the higher-order confirmatory factor analysis (CFA) indicate strong loading (0.74 or greater) for each of our items onto their respective subscales (i.e., individual, interpersonal, and structural), in addition to strong loadings (0.80 or greater) of each of our subscales onto the higher-order factor of SV stigma. These results provide evidence of construct validity of the SVRSS across stigma levels.
Outcomes
We examined four mental health outcomes using sum scores from the following validated scales. Generalized anxiety disorder was measured with the Generalized Anxiety Disorder-7 scale (GAD-7; Spitzer et al., 2006), a seven-item screening tool used to assess the presence and severity of symptoms of generalized anxiety disorder (Cronbach’s alpha = .88). Depression was measured with the Center for Epidemiologic Studies-Depression Scale-20 (CES-D-20), a 20-item scale that is a reliable and valid measure of depressive symptoms (Radloff, 1977; Cronbach’s alpha = .78). Symptoms of PTSD were assessed using the Five-Item Primary Care Screen for PTSD (Prins et al., 2016), which was designed to identify individuals with probable PTSD. Individuals who endorse a lifetime history of trauma are asked to respond to 5 yes/no items addressing the presence of common PTSD symptoms (Cronbach’s alpha = .78). Alcohol misuse was measured using the three-item Alcohol Use Disorders Identification Test-Concise (AUDIT-C; Bradley et al., 2003), which is a shortened version of the 10-item AUDIT instrument. The AUDIT-C identifies individuals who are hazardous drinkers or have active alcohol use disorders (Cronbach’s alpha = .66).
We included a behavioral measure of shame using a modified form of the Self-Referent Encoding Task (SRET) adapted by Pachankis et al. (in press). The SRET is an online task that includes 11 positive (e.g., “talented,” “terrific”) and 11 negative (e.g., “boring,” “selfish”) adjectives. Participants were exposed to each word twice, and always just one word at a time. Participants complete 44 trials in which either a positive or negative word is displayed on a computer screen along with a question asking them to select “yes” or “no” to one of two questions (“Like me?” and “Has an E?). “Like Me?” represents a self-referential judgement and “Has an E?” represents an objective judgement of the content of the word. To compute a behavioral measure of shame, Pachankis et al. (in press) calculated a ratio of reaction time for endorsing the word “ashamed” as self-referential or the reversed reaction time to not endorsing the word “ashamed” as self-referential, to the reaction time for endorsing (or not endorsing) the word “proud” as self-referential. The variable was log-transformed before it was entered into the analyses.
Participants were also asked questions about their use of mental healthcare services. Treatment need was assessed for the past 12 months using the following question: “Was there ever a time during the past 12 months when you felt that you might need to see a professional because of problems with your emotions, nerves, or your use of alcohol or drugs?” Response options were yes/no. Treatment use (yes/no) was also assessed for the past 12 months. Participants were asked, “In the last 12 months, did you go to see any of the professionals on this list for problems with your emotions, nerves, or your use of alcohol or drugs?” and indicated which provider they saw from a list of options. Participants could also indicate that “I did not see a professional in the last 12 months.”
Covariates
We controlled for participant age, sex assigned at birth, and sexual orientation, as each of these variables has been independently linked to psychopathology outcomes and treatment utilization (Cochran et al., 2003; Kessler et al., 2005). Additionally, we controlled for relationship status because individuals experiencing SV in intimate partner violent relationships may have different rates of mental health and treatment-seeking based on whether they are still in a relationship with a violent partner. For models focused on treatment outcomes, we additionally controlled for symptoms of generalized anxiety, depression, alcohol misuse, and PTSD to determine whether associations were independent of the level of psychopathology endorsed by the participant.
Statistical Analysis
Analyses were conducted in R (Version 4.1.1; R Core Team, 2021). We fit separate models for each of our outcomes of interest.
Our mental health outcomes were assessed using scales with Likert-item response variables, so we fit beta regression models to account for the bounded nature of the data (i.e., a participant cannot score above a certain threshold on symptoms scales, and therefore responses are not truly continuous) using the betareg package (Cribari-Neto & Zeileis, 2010). For the SRET scale, in which scores were normally distributed values between −1 and 1, we fit a simple linear model using the stats package, which is included in base R (R Core Team, 2021). For binary outcomes (treatment need and treatment use), we fit logistic regression models, also using the stats package. Statistical significance was set at p < .05, and two-tailed significance tests were used.
We did not use survey weights in this analysis because the betareg package, which was necessary to analyze our mental health outcome variables, cannot currently accommodate complex survey weights. However, as a sensitivity analysis, we re-ran the results for the mental health outcome variables using a GLM framework accounting for the complex survey design. These results were identical in magnitude and direction to those reported below, indicating that our findings generalize to the population of Swedish young adults ages 18 to 35.
Results
Demographic Characteristics
A total of 1,356 participants completed the PLUS survey at Wave 3. Participants included in our analysis indicated that they had experienced at least one incident of SA or IPSV in their lifetimes, which resulted in a total of 453 participants (33.4%). Of these participants, 46.0% identified as heterosexual, 8.13% as lesbian or gay, 39.1% as bisexual, 2.32% as unsure of their sexuality, and 4.41% as “something else.” The average age of our sample was 27.9 (SD = 4.92). The majority of our sample was assigned female at birth (87.9%) and identified as cisgender (96.5%), with 2.64% identifying as genderqueer, 0.66% identifying as trans men, and one participant (0.23%) identifying with a different gender identity. In terms of education, 4.6% had no high school degree, 39.7% had a high school diploma or GED, 5.3% had some college or an associate’s degree, 9% had a 4-year university degree, and 41% had completed part or all of a graduate degree program.
The PLUS study enrolls ethnic minority and non-minority participants by using a sampling frame that is reflective of the Swedish general population. Swedish demographic analyses do not contain data regarding North American-specific races (e.g., African American, Native American) and official statistics on Hispanic ethnicity do not exist according to Statistics Sweden, the Swedish government agency responsible for producing official statistics. Participants were asked if they identify as a member of an ethnic minority group in Sweden. Within this sample, 7.5% of participants identified as a member of an ethnic minority group and 24.9% indicated that they were born in a country other than Sweden. Further demographic characteristics can be found in Table 1.
Sample Characteristics.

The majority of participants (89%) endorsed at least one item on the SVRSS (for item-level data, see Table 2). The average sum score for our scale was 7.79 (SD = 6.27; range 0–27), indicating moderate levels of SV stigma exposure.
Item Level Means, Standard Deviations, and % Endorsement for Sexual Violence-Related Stigma Scale.

Each item is a Likert scale with a range of 0 to 3, range for total score is 0 to 27.
Note. SV = sexual violence.
Psychopathology Outcomes
When interpreting beta regressions, it is important to note that the output has been standardized with values ranging from 0 to 1. Thus, the coefficient for SV stigma means that for a 1-unit increase on the stigma scale, the ratio between the expected symptom score and the difference to the scale’s maximum symptom score (e.g., a 21 on the GAD-7) increases/decreases by exp(\B).
Higher levels of SV stigma were associated with greater symptoms of generalized anxiety disorder (B = 0.02, SE = 0.004, p < .001), depression (B = 0.03, SE = 0.003, p < .001), and PTSD 1 (B = 0.05, SE = 0.01, p < .001) but were associated with fewer symptoms of alcohol misuse (B = −0.02, SE = 0.005, p < .01), net of covariates (Figure 1). Thus, a 1-unit increase in SV stigma is associated with a 2% increase in symptoms of generalized anxiety disorder, a 3% increase in symptoms of depression, and a 5% increase in symptoms of PTSD. In contrast, a 1-unit increase in SV stigma is associated with a 2% decrease in symptoms of alcohol misuse.
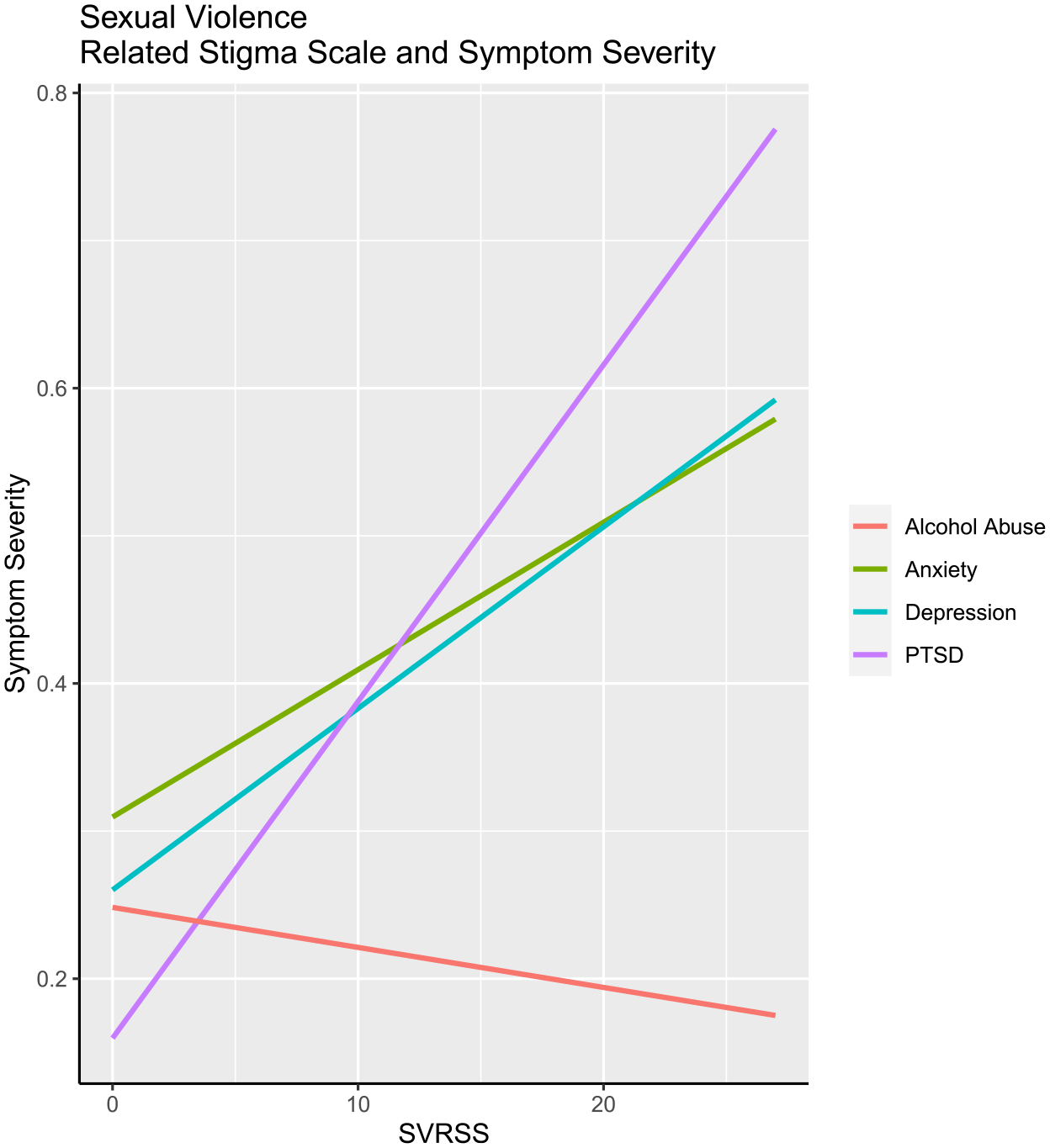
Sexual violence-related stigma scale and symptom severity.
Self-Referent Encoding Task
Higher levels of SV stigma were associated with a lower score on the SRET, consistent with greater shame, after controlling for covariates (B = −0.02, SE = 0.04, p < .001).
Treatment Utilization Outcomes
Participants who reported greater SV stigma were more likely to report that they needed treatment in the past 12 months (adjusted odds ratio (AOR) = 1.07, 95% CI [1.03, 1.10], p < .001). These results remained statistically significant after additionally controlling for symptoms of generalized anxiety, depression, alcohol misuse, and PTSD (AOR = 1.06, 95% CI [1.01, 1.12], p < .05). We did not observe a significant association between SV stigma and reported past-year treatment use (AOR = 1.02, 95% CI [0.97, 1.07], p = .45).
Supplementary Analyses
We analyzed each subscale of SV stigma as an independent variable predicting each of our outcomes and found that the direction and magnitude of each model were comparable across stigma levels. These results suggest that each of the three levels of stigma is similarly associated with study outcomes, and thus that no one level appears to be independently driving these associations.
Discussion
The aim of this investigation was to quantify experiences with SV-related stigma among a diverse group of young adults with a history of two forms of SV, and to determine whether greater SV stigma burden was associated with psychopathology, shame, and treatment-seeking outcomes. To do so, we created a new scale, adapted from the HIV stigma literature, that measures subjective experiences of stigma across individual, interpersonal, and structural levels, consistent with conceptualizations of stigma as a multi-level construct (Hatzenbuehler, 2016; Link & Phelan, 2001). This scale reliably measured participants’ negative self-image related to their experience of SV, disclosure concerns, and concerns about public attitudes, respectively.
Our results indicated that SV stigma is associated with symptoms of generalized anxiety, depression, and posttraumatic stress disorder in a sample of individuals with heterogeneous experiences of SV—including both lifetime SA and past-year IPSV—suggesting that SV stigma may serve as a broad risk factor for post-assault psychopathology. Moreover, greater SV stigma was associated with fewer symptoms of problematic alcohol use. A well-developed literature has identified problematic drinking as a frequent but maladaptive coping mechanism following SA (Fossos et al., 2011; Rhew et al., 2017; Ullman, 2016; Ullman et al., 2018). However, to our knowledge, no study has examined the association between SV stigma and alcohol misuse. In a review by Gravelin (2018), 11 out of 16 studies that manipulated intoxication levels in vignettes about SA found that individuals who were described as intoxicated were blamed more for acquaintance rape than individuals described as sober. Given this strong cultural association between SV and alcohol, individuals who reported higher levels of SV stigma may be compelled to reduce their alcohol use as a means of counteracting victim blaming narratives. Given the lack of research on the relationship between SV stigma and alcohol use, as distinct from exposure to SV, future work is needed to determine whether there are distinct profiles of alcohol misuse among those who are reporting experiences of SV stigma and to identify potential mechanisms and moderators of this relationship.
Contributions of the Current Study to the SV Stigma Literature
Findings of this investigation are consistent with results of previous work in this area. For example, an earlier investigation by Murray and colleagues (2018) employed a scale tailored to stigma among survivors of IPV in the Democratic Republic of Congo and found a positive association between stigma burden and general psychological distress (Murray et al., 2018). Our investigation advances this research in five key ways.
First, we employ a population-based sample, a rarity in the SV literature broadly and the SV stigma literature specifically. In doing so, we reduce selection biases in ways that not only increase external validity, but also potentially internal validity, given that the range of stigma experiences in non-probability samples can be restricted (Meyer & Wilson, 2009). For example, non-probability samples of sexual minorities identify participants who are more open about their sexual orientation, thus restricting the range of identity concealment behaviors present in the sample (e.g., Salway et al., 2019). Applying this research to survivors of SV, non-probability samples, especially those that recruit heavily from rape crisis centers and mental health clinics (Hakimi et al., 2018), may be capturing a disproportionate number of survivors who have disclosed and/or sought help, thereby restricting the range of SV stigma experiences, including those captured herein (e.g., disclosure concerns, internalized stigma).
Second, the sample of participants included in this analysis is diverse with respect to sexual orientation, given the oversample of sexual minorities, a group at heightened risk for SV (Chen et al., 2020), in the PLUS dataset. This feature of our dataset stands in contrast to much of the literature on SV, which has frequently drawn from “convenience” (i.e., non-probability) samples of heterosexual, cisgender women recruited from college campuses (Kennedy & Prock, 2016). Further, there are no studies to date that evaluate SV stigma in a representative sample of sexual minority young adults. Thus, we increase the generalizability of our findings while also furthering a broader goal for the field of psychological science, which is to recruit larger and more diverse samples of participants (Gravelin, 2018).
A third contribution of this investigation to the SV stigma literature is that our measure assessed perceived SV stigma at the individual, interpersonal, and structural levels. With a few exceptions (Deitz et al., 2015; Eckstein, 2016), prior work has assessed SV stigma only at a single level, or, more rarely, across two levels (typically individual and interpersonal). Further, to our knowledge, no previous investigation has evaluated a measure capturing all three levels of SV stigma as a predictor of a wide range of mental health, treatment-seeking, and behavioral outcomes.
A fourth contribution of this investigation is that we incorporated a multi-modal assessment of the consequences of SV stigma, thereby overcoming the limitations associated with same-source bias (Diez Roux, 2007), in which the exposure and outcomes are measured via the same method, as well as with social desirability bias, which can lead to underreporting of negative emotions such as shame (Pachankis et al., in press). Whereas our psychopathology and mental health-seeking outcomes are assessed via self-report, we also employed a behavioral measure of shame via a modified version of the SRET. We observed that SV stigma was associated with faster reaction time to a shame-related word (vs. proud), suggesting that exposure to more SV stigma may lead to internalization of shame, a key maintenance factor for anxiety, depression, and PTSD symptoms in people who have experienced SV (Badour et al., 2020; DeCou et al., 2019; Shorey et al., 2011). Testing shame as a mediator linking SV stigma and psychopathology will be possible in future waves of the PLUS dataset.
Finally, in addition to exploring the relationship between SV stigma and psychopathology, we explored outcomes related to treatment utilization. Overstreet and Quinn (2013) highlighted that in previous work exploring IPV stigma and treatment, distinctions between disclosure and treatment-seeking are not always made clear. Much of the work around SV stigma has either been qualitative (e.g., Gruenfeld et al., 2017) or has focused on quantifying how many and to whom people disclose following an experience of SV (e.g., Ullman & Peter-Hagene, 2014). Importantly, disclosure and treatment-seeking are distinct behaviors, and not all those who disclose a history of SV do so with the goal of seeking treatment. In our investigation, SV stigma was associated with higher rates of perceived past-year treatment need. This association remained robust even after controlling for symptoms of generalized anxiety, depression, alcohol misuse, and PTSD. However, we did not find evidence of an association between SV stigma and past-year treatment use, which may be due to the fact that our measure of treatment-seeking did not include items specifically about SV, an important avenue for future research.
Taken together, it is the unique confluence of each of these areas—that is, employing (a) a multi-level measure of SV stigma (b) in a diverse, population-based (i.e., nationally representative) sample that includes (c) a multi-modal assessment of (d) a range of psychopathology, treatment-seeking, and behavioral consequences of SV stigma—that makes this study one of the most comprehensive tests of SV stigma in the literature to date.
Future Research
Results of our investigation would be strengthened by future work quantifying SV stigma using objective measures, especially those that capture stigma at the structural level (for an example of structural measurement of homophobia, see Lattanner et al., 2021). Objective measures provide corroboration of subjective reporting, reduce the risk of confounds with mental health, and can help identify clear instances of discrimination and opportunities for structural intervention (Hatzenbuehler, 2016). While studies have begun to develop structural measures of SV stigma (Dworkin et al., 2017), research in this area is sparse and additional structural measures of SV stigma are sorely needed, especially in light of recent recommendations for deeper consideration of sociocultural factors in post-assault recovery (Dworkin & Weaver, 2021).
In addition to the development of objective measures of SV stigma, future work should investigate relationships between SV stigma and other psychopathology outcomes that have been observed following experiences of SV, such as disordered eating, obsessive compulsive disorder, bipolar disorder, and suicidal ideation and attempt (for review, Dworkin et al., 2018). Further, additional research exploring the relationship between SV stigma and correlates of post-assault recovery would help determine whether widely accepted correlates of recovery, like event centrality, represent a person’s response to the trauma itself, to stigma encountered following experiences of SV, or to both.
Finally, SV stigma may intersect with other identity-related stigmas (e.g., race, immigration status, gender, sexual orientation) such that SV stigma is experienced differently by members of multiple stigmatized groups. In our sample, SV stigma was correlated with our outcomes of interest regardless of sexual orientation and birth-assigned sex. However, research that is specifically designed to capture the variation in SV stigma experiences among members of diverse racial, ethnic, gender, sexuality, and disability statuses, to name a few, is an important future direction.
Limitations
Results from this study should be considered in light of its limitations. First, although the PLUS study is a longitudinal investigation, the SRVSS was only included in the third wave of data collection. As such, our results are cross-sectional and cannot establish causal relationships. Indeed, it is possible that mental health symptoms might cause greater awareness of, and/or likelihood of reporting, stigma experiences (Meyer, 2003). Although longitudinal research with other stigmatized groups (e.g., racial minorities) demonstrates that reports of stigma are prospectively related to mental health (Paradies et al., 2015), it will be necessary for future studies to follow participants longitudinally to determine whether mental health symptoms change as a function of exposure to SV stigma. Longitudinal research would also help inform whether SV stigma is relatively stable over time (trait-like) or whether it is variable across social contexts, as identity threat theories of stigma would suggest (Major & O’Brien, 2005).
Second, as is the case in other large-scale cohort studies, the PLUS dataset used self-reported surveys rather than clinical diagnoses of mental health. Though there are many strengths of using a large population-based study design, one disadvantage is that it is typically not feasible to have clinician-administered diagnoses. Future studies should therefore determine whether the results generalize across DSM-5 diagnoses of psychiatric morbidity.
Third, our measure was adapted from an HIV scale. Although the stigmas of HIV and SV share many overlapping features, there are important distinctions, and thus it is likely that our scale does not capture the full range of experiences relevant to understanding stigma as it relates to SV. Going forward, qualitative work can be used to deepen our understanding of SV stigma in order to improve upon our scale. For example, one avenue for future qualitative work may be to expand the range of stigma experiences related to SV exposure and provide justification for a potential future iteration of this scale.
Fourth, our study was conducted in Sweden given the high quality of its national public health data. This context has implications for generalizability. While research indicates that levels of SV are fairly comparable between the U.S. and Sweden (Öberg et al., 2021), it will be important to explore whether our results yield similar associations between SV stigma, psychopathology, shame, and treatment need and use in other social contexts, particularly those with greater diversity with respect to race/ethnicity.
Fifth, although we inquired about past-year treatment use, participants were not asked whether they were specifically seeking treatment related to their experience(s) of SV, as this question was administered to all participants in the PLUS sample regardless of SV history. Finally, in this investigation we measured two types of SV (SA and IPSV), yet there are other forms of SV (e.g., childhood sexual abuse, sexual harassment) that we have not considered. We hope that our SV stigma scale will be used by other researchers to evaluate its predictive validity across a wider range of SV experiences.
Conclusion
Despite these limitations, this investigation offers a potentially useful and broadly applicable tool for the measurement of multi-level SV stigma experiences that can be used across at least two common forms of SV. By observing associations between SV stigma and multiple types of psychopathologies, treatment-seeking outcomes, as well as a behavioral measure of shame, we provide initial evidence to motivate further work at the intersection of stigma and SV. Our results suggest that exposure to SV stigma at the individual, interpersonal, and structural levels may be a critical, but often overlooked, correlate of post-assault recovery, and they raise several important directions for future research on this important topic.
Supplemental Material
sj-R-1-jiv-10.1177_08862605231179715 – Supplemental material for Sexual Violence-Related Stigma, Mental Health, and Treatment-Seeking: A Multimodal Assessment in a Population-Based Study of Young Adults
Supplemental material, sj-R-1-jiv-10.1177_08862605231179715 for Sexual Violence-Related Stigma, Mental Health, and Treatment-Seeking: A Multimodal Assessment in a Population-Based Study of Young Adults by Emily J. Mellen and Mark L. Hatzenbuehler in Journal of Interpersonal Violence
Supplemental Material
sj-R-2-jiv-10.1177_08862605231179715 – Supplemental material for Sexual Violence-Related Stigma, Mental Health, and Treatment-Seeking: A Multimodal Assessment in a Population-Based Study of Young Adults
Supplemental material, sj-R-2-jiv-10.1177_08862605231179715 for Sexual Violence-Related Stigma, Mental Health, and Treatment-Seeking: A Multimodal Assessment in a Population-Based Study of Young Adults by Emily J. Mellen and Mark L. Hatzenbuehler in Journal of Interpersonal Violence
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: R01 MH118245 from National Institute of Mental Health.
Notes
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.