
Abstract
Sexual and gender minority (SGM) individuals are at an increased risk of experiencing sexual violence (SV). Social reactions received upon disclosure of SV impact survivors’ mental health, and this may be more extreme when social reactions are provided by other SGM individuals. The purpose of the current study was to understand the SV disclosure experiences of SGM young adults, including the identity of disclosure recipients and the quality of the social reactions received by SGM and cisgender/heterosexual disclosure recipients. Additionally, the current study sought to examine how the SGM identity of the disclosure recipient and the quality of the social reactions received were associated with mental health outcomes (depression, post-traumatic stress disorder [PTSD], and alcohol use) among SGM SV survivors. SGM-identifying participants (N = 110) completed a 10-min survey on Qualtrics that was distributed through Prime Panels. Results revealed that 83% of participants (SGM survivors of SV) disclosed their SV experience to other SGM individuals. SGM disclosure recipients provided more positive social reactions and fewer negative social reactions than cisgender/heterosexual disclosure recipients. Regression models indicated that positive social reactions from cisgender/heterosexual recipients were associated with a decrease in depression scores. Negative social reactions from SGM recipients were associated with an increase in depression scores. Unexpectedly, positive social reactions from SGM recipients, while negative social reactions from cisgender/heterosexual recipients, were associated with an increase in PTSD scores. No associations were found between social reactions and alcohol use. Findings highlight the importance of social reactions and disclosure experiences on SGM survivors’ mental health and mitigation opportunities to improve these disclosure experiences.
Introduction
Sexual violence (SV) is a global concern. Among countries with high Human Development Index (i.e., health, knowledge, and standard of living), some research suggests SV has slowly declined from 1990 to 2017 (Borumandnia et al., 2020); however, global research has highlighted the growing rate of SV particularly among sexual and gender minority (SGM) individuals (Chen et al., 2020; Langenderfer-Magruder et al., 2016). Expression of gender and sexual orientation that differ from traditional dominant norms serves as a catalyst for increased rates of many forms of violence against SGM, and in this case, SV (Roberts et al., 2012; Saewyc et al., 2006). Indeed, rates of SV among SGM are consistently higher than rates of SV experienced by cisgender/heterosexual individuals (Blayney et al., 2023; Johnson et al., 2017; Langenderfer-Magruder et al., 2016; Walters et al., 2013).
Friends or family members can be a common source of support upon disclosure of SV (Sylaska & Edwards, 2014). However, research indicates that there can be positive or negative social reactions provided by disclosure recipients, which can mitigate or worsen mental health (Ullman, 2000). Because SGM individuals may have strong kinship bonds and extensive social networks with other SGM individuals (Hailey et al., 2020), it may be likely that SGM victims of SV are disclosing to other SGM individuals, and that the benefits or consequences of receiving positive or negative social reactions may exacerbate mental health outcomes. However, no known research has explored this. Thus, the purpose of the current research is to describe the disclosure experiences of SGM survivors of SV, and to examine the associations between social reactions provided by SGM and cisgender/heterosexual individuals and mental health among SGM survivors of SV.
SV Among SGM Individuals
Research has shown that SGM individuals experience higher rates of SV, including contact SV (e.g., unwanted sexual contact, rape, and unwanted penetration), noncontact SV (e.g., verbal harassment), and sexual coercion, compared to cisgender/heterosexual individuals (Walters et al., 2013). In fact, SGM is at an increased risk of experiencing SV (Beyer et al., 2021; Blayney et al., 2023), potentially due to marginalization and bias against individuals expressing their gender identity and sexual orientation in ways that do not conform to dominant societal values and beliefs (Gordon & Meyer, 2007).
Experiences of SV are associated with poor psychological outcomes, such as depression, anxiety, and post-traumatic stress disorder (PTSD; Chen et al., 2010; Tjaden & Thoennes, 2006), and outcomes are heightened among SGM survivors (Kammer-Kerwick et al., 2021; Sigurvinsdottir & Ullman, 2015). For instance, among those who have experienced SV, SGM individuals tend to report higher levels of depression, PTSD, and revictimization (Balsam et al., 2011; Kalichman et al., 2001; Kammer-Kerwick et al., 2021) compared to cisgender/heterosexual individuals (Sigurvinsdottir & Ullman, 2016; Sigurvinsdottir & Ullman, 2015; Smith et al., 2016).
Disclosure of SV
Globally, SV is understudied and underreported (Ferreira et al., 2023; Parti et al., 2023; Syukriani et al., 2022; World Health Organization, 2007). One reason for underreporting may be that survivors often do not report and disclose their SV experience due to fears of being blamed, judged, or embarrassed (Lombardi, 2009; Lombardi & Jones, 2009). Survivors who choose to disclose their experience often disclose to informal networks such as friends or family members (Sylaska & Edwards, 2014). Relatively few individuals report disclosing to formal resources such as campus resources or law enforcement (Edwards et al., 2022a). Research indicates that this pattern may be more extreme among SGM survivors of SV, with SGM survivors disclosing to informal resources at higher rates and formal resources at lower rates than their cisgender/heterosexual counterparts (Edwards et al., 2022a; Grocott et al., 2022). Potential explanations could be that SGM individuals may have strong kinship-like relationships with other SGM individuals (Hailey et al., 2020), be more distrustful of formal resources and entities that have historically enacted harm on their communities, or fear that their sexual identity could be disclosed without their permission (Edwards et al., 2022a).
Upon disclosure, research consistently documents that survivors of SV can receive positive or negative social reactions from the disclosure recipient (Ullman, 2000). Positive social reactions include things such as referring to support services and listening without blame, whereas negative social reactions include victim blaming and avoiding future contact with the individual (Ullman, 2000). Importantly, unique social reactions are provided when the sexual assault involved alcohol (whether by the perpetrator, survivor, or both). This includes more negative social reactions (Lorenz & Ullman, 2016), as well as unique alcohol-specific social reactions (Kamke et al., 2022; Koon-Magnin & Schulze, 2019; Relyea & Ullman, 2015). This is important to note because a high number of sexual assaults involve alcohol (Grocott et al., 2022). Furthermore, rates of alcohol use among SGM are heightened compared to cisgender/heterosexual individuals (Parent et al., 2018). Other factors are associated with the type of social reaction provided, including the nature of SV (e.g., unwanted sexual contact or rape, vaginal or anal), the relationship between the survivor and the disclosure recipient, the perpetrator, and race (Franklin & Garza, 2021; Kamke et al., 2022; Koon-Magnin & Schulze, 2019; Lorenz et al., 2018; Ullman, 2021).
The quality of the social reaction is important because of its demonstrated association with mental health, above and beyond the assault experience itself (Edwards et al., 2022a). Positive social reactions appear to slightly ease mental distress associated with the SV experience (Ullman & Peter-Hagene, 2014; Edwards et al., 2022a), whereas negative social reactions are more strongly associated with worsening mental distress (Dworkin et al., 2019; Peter-Hagane & Ullman, 2014). It is important to note that other factors have been identified to mediate the relationship between social reactions and mental health outcomes, such as support, shame, and racial identity (DeCou et al., 2017; Hakimi et al., 2018; Peter-Hagene & Ullman, 2014).
SGM survivors of SV who receive negative social reactions tend to have poorer outcomes such as PTSD and depression and slower recovery, compared to those who receive more positive social reactions (Hakimi et al., 2018; Ullman & Peter-Hagene, 2014). This may be compounded when the person who provides the social reaction is also SGM. Considering how SGM individuals share kinship networks with other SGM individuals to protect against social isolation, rejection, and a general lack of support due to their identities (Hailey et al., 2020), negative social reactions from SGM disclosure recipients may lead to worse psychological outcomes. Elements of Minority Stress Theory (Meyer, 2003), including fears of rejection and internalized negativity, may explain exacerbated mental health symptoms when receiving a negative social reaction, especially from other SGM individuals.
Purpose
There are many unique elements of SV and disclosure among SGM survivors that necessitate an examination of the association between social reactions and mental health, particularly by examining the SGM status of the disclosure recipient. As such, the purpose of this study is to explore the disclosure experience of SGM survivors of SV and examine the association between social reactions and mental health outcomes by the perceived SGM status of the disclosure recipient. Specifically, we aimed to answer the following research questions:
What is the sexual and gender identity of recipients of disclosure of SV experienced by SGM individuals?
What social reactions to the disclosure of SV are provided by SGM and cisgender/heterosexual disclosure recipients to SGM survivors of SV?
What is the association between social reactions provided by SGM and cisgender/heterosexual disclosure recipients and mental health outcomes (depression, PTSD, and alcohol use)?
We hypothesized that negative social reactions would be associated with worse mental health outcomes, while positive social reactions would be associated with better mental health outcomes. Additionally, we hypothesized that these relationships would be stronger for social reactions provided by SGM disclosure recipients.
Methods
Participants
Participants were recruited via Prime Panels (Cloud Research, Prime Panels), compiled opt-in market research panels commonly used in research. Participants were eligible for the study if they: (a) resided in the United States, (b) spoke English, (c) identified as a sexual or gender minority, (d) were between the ages of 18 and 25 years, (e) experienced SV within the past year, and (f) disclosed their SV experience to another individual. We conducted quota sampling in which no more than 70% of participants identified as cisgender women, due to the predominance of cisgender women in SV research (e.g., Borumandnia et al., 2020; Dartnall & Jewkes, 2013; Porter & Williams, 2011). There was a total of N = 110 participants included in the current study. This represents the sample used to answer Research Questions 1 and 2 (descriptive information). Ninety-one participants disclosed to both cisgender/heterosexual and SGM individuals, which represents the sample used to answer Research Question 3 (associations).
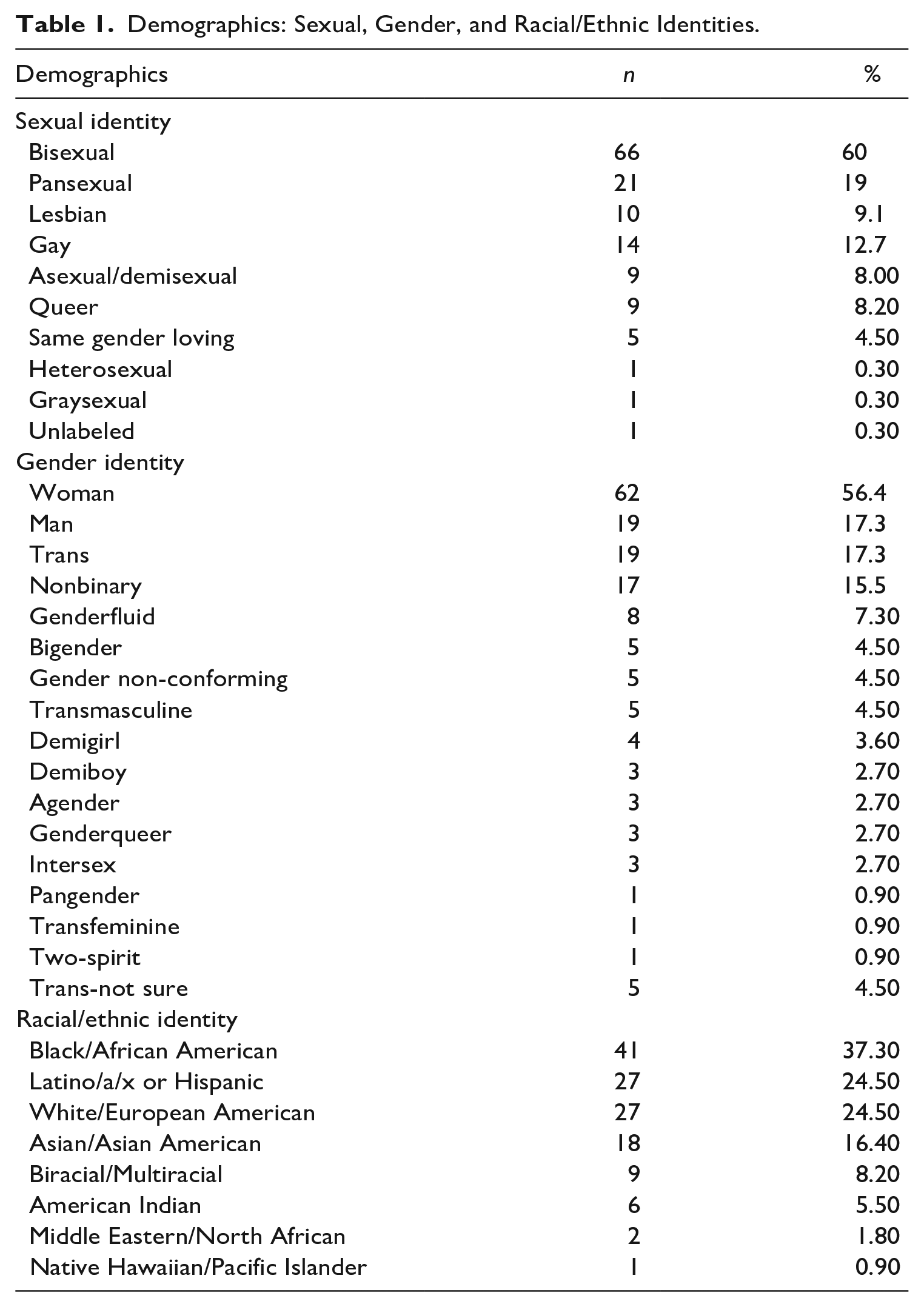
The average age of the total participants (N = 110) was 21.65 (SD = 1.87). The majority of the participants identified as bisexual (60%), followed by pansexual (19%), lesbian (9.1%), and gay (12.7%). The majority of participants identified as women (56.4%), men (17.3%), or nonbinary (15.5%). Just under a fifth (17.3%) indicated they were trans, while 4.5% indicated they were not sure about their gender identity. The sample was racially/ethnically diverse, as the modal race selected was Black/African American (37.3%), followed by Latino/a/x or Hispanic (24.5%) then White/European American (25.4%). Sexual, gender, and racial/ethnic identity information is presented in Table 1.
Demographics: Sexual, Gender, and Racial/Ethnic Identities.
Procedures
Participants completed an informed consent form and inclusion screening. If eligible to participate, participants completed a short, 10-min survey hosted on Qualtrics. After completion of the survey, participants were provided national resources for anti-SGM violence, self-harm, and SV. All procedures were approved by the Institutional Review Board of the first authors’ institution. At the end of the study, participants were thanked for their time and paid for participation.
Measures
Demographics/Eligibility Screening
Seven questions were assessed for participants’ age, U.S. residence, sexual identity, gender identity, and racial/ethnic identity.
SV Exposure
Two items developed by the research team captured exposure to SV including, “In the last year, have you experienced SV that was done against you? This may include sexual assault or rape, being made to penetrate someone else, unwanted sexual contact, among others.” Response options included Yes or No. To identify whether alcohol was involved in the experience of SV within the last year, the following question was asked: “In the most recent SV that you experienced, was alcohol involved (either you or the person who committed violence against you)?.” Response options included Yes, No, or Not sure.A categorical variable was created to categorize whether alcohol was involved in the SV encounter and was dummy coded where 1 = alcohol involvement and 0 = no alcohol involvement.
SV Disclosure Questionnaire
Eight items were developed to assess whether participants disclosed their SV experience to another individual and their relationship with the person they disclosed to (peer, family member, friend, intimate partner, coworker, therapist, or formal support service (e.g., police officer). Further, researchers assessed whether the individual(s) disclosed to people who also identified as a sexual and/or gender minority. This included a question that asked “Of the people that you talked to about your experience of SV, do any of them identify as LGBTQ+? (Either assumed or known identity).” Response options included Yes, No, and I’m not sure. Additionally, participants were asked to indicate what percentage of the people they disclosed to were LGBTQ, with response options including 0% to 25%, 26% to 50%, 51% to 75%, and 76% to 100%.
Social Reactions Questionnaire—Shortened
The Social Reactions Questionnaire—Shortened is the brief version of the Social Reactions Questionnaire that consists of 16 items that assess for frequency of receiving both positive (“Comforted you by telling you it would be all right or by holding you”) and negative (“Told you to go on with your life”) social reactions (Ullman et al., 2017). Responses range from 0 (Never) to 4 (Always). Mean composites were created for positive and negative reaction items, in which higher scores indicate more frequent positive or negative social reactions to SV disclosure. This measure was administered to participants who disclosed to cisgender/heterosexual individuals (α = .84) and SGM individuals (α = .84) separately. To probe for social reactions received from cisgender/heterosexual recipients, the questions were framed as “Thinking of the cisgender, heterosexual people you have disclosed to. . .,” while the questions were framed as “Thinking of the LGBTQ+ people you have disclosed to. . .” for SGM disclosure recipients.
Mental Health Symptomatology
To assess for mental health symptomatology, four items were taken from the Patient Health Questionnaire (PHQ; Kroenke et al., 2001). The severity of depression was assessed using two items (“Little interest or pleasure in doing things” and “Feeling down, depressed, or hopeless”). Response options included 1 (Not at all) to 4 (Every day). Cronbach’s alpha was .74. PTSD symptoms were assessed using two items from the post-traumatic stress disorder checklist (PCL; Blevins et al., 2015). These items included, “How much were you bothered by repeated, disturbing, and unwanted memories of the stressful experience?” (α = .71). Response options ranged from 1 (Not at all) to 4 (Extremely). Three items from the alcohol use disorder identification test (AUDIT; Saunders et al., 1993) were used to assess symptoms of alcohol use disorder. These included, “How often do you have five or more drinks on one occasion?” and “How many drinks containing alcohol do you have on a typical day when you are drinking?”(α = .80). Response options captured the frequency of drinking (Never to four or more times a week) and the average number of drinks on one occasion (1–10 or more).
Data Analysis
Data were analyzed using SPSS Software Version 28 (IBM Corporation, 2021; IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp). For Research Questions 1 and 2, descriptive statistics (means and standard deviations for continuous variables) and frequencies (for categorical variables) were produced to examine SV disclosure information including identities of the people disclosed to, and their social reactions using the total sample (N = 110). For Research Question 3, multiple regressions were conducted to examine whether social reactions to SV disclosures among both cisgender/heterosexual and SGM individuals (N = 91) were associated with depression, PTSD, and drinking outcomes. Whether the SV experience involved alcohol was included as a covariate because of its demonstrated associations with receiving negative social reactions (Relyea & Ullman, 2015). All assumptions were examined and met prior to running analyses.
Results
Descriptive Information
Among all SGM survivors (n = 110), 67.3% disclosed to friends, 47.3% disclosed to family members, 40% disclosed to their intimate partner(s), 8.2% disclosed to their coworkers/other students, and 28.2% disclosed to their therapist/psychologist. Only 10% disclosed to formal support services such as police, title IX, or SV support services, and 2.7% indicated they disclosed to another person, including people in public and a school advisor. Response options were not mutually exclusive, and many individuals disclosed to multiple sources. However, only one individual disclosed solely to formal sources. Table 2 depicts participant-reported disclosure recipients by type and identity.
Participant Reported Disclosure Recipients by Type and Identity.
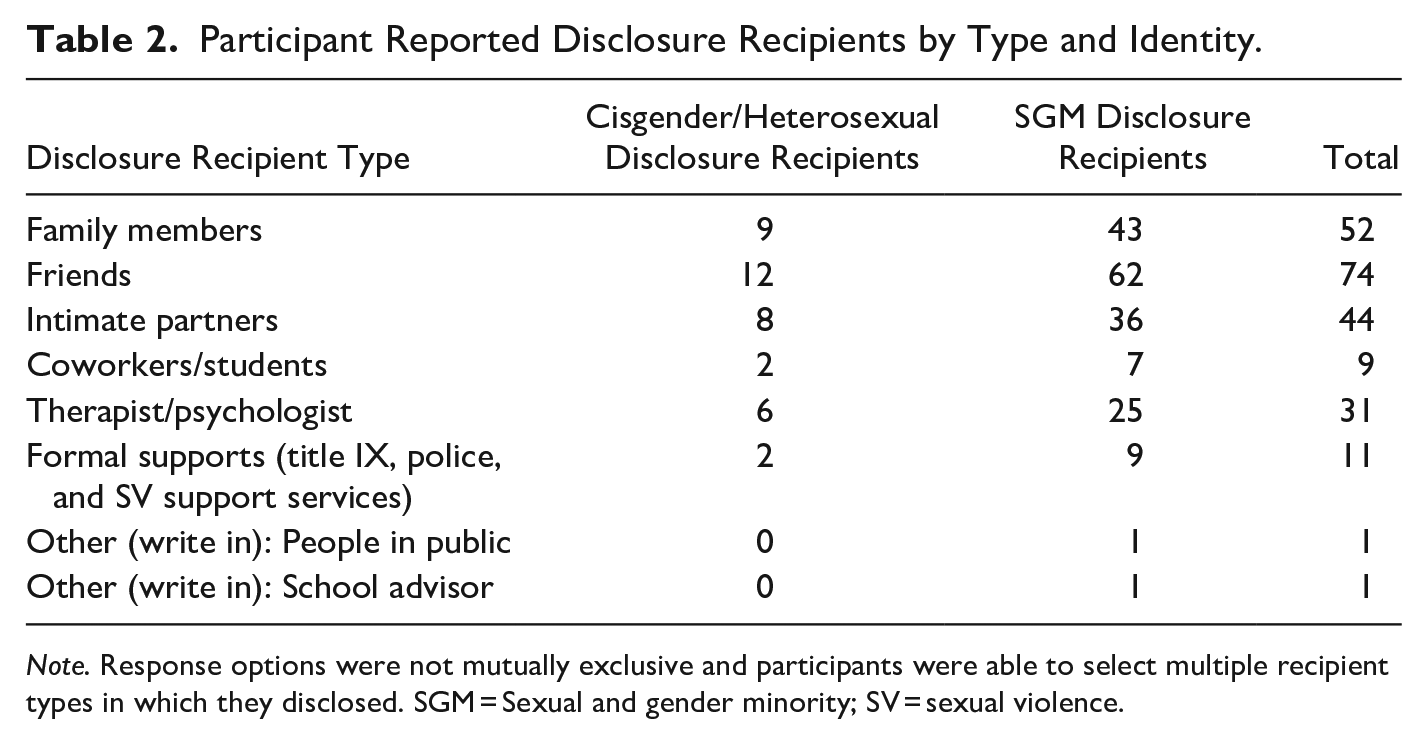
Note. Response options were not mutually exclusive and participants were able to select multiple recipient types in which they disclosed. SGM = Sexual and gender minority; SV = sexual violence.
Research Question 1: Identities of Disclosure Recipients
Regarding sexual identity, 82.7% of individuals disclosed to a person they perceived to be SGM. More specifically, many participants (44.0%) indicated that 26% to 50% of the people they talked to about their SV were SGM, followed by 51% to 75% (25.3% of participants), 76% to 100% (15.4% of participants), and 0% to 25% (15.4% of participants).
Research Question 2: Social Reactions Provided
Table 3 provides descriptive information for the social reactions received by the identity of the disclosure recipient. Among those who disclosed to cisgender/heterosexual individuals (N = 110), the average positive social reaction received upon disclosure was 2.56 (SD = 0.82), and the average negative social reaction was 2.23 (SD = 0.71). Among those who disclosed to individuals identifying as an SGM individual (N = 91), the average positive social reaction was 2.87 (SD = 0.78), and the average negative social reaction was 1.89 (SD = 0.70). With a total possible SRQ-S score of 4, SGM survivors reported less frequent positive social reactions and more frequent negative social reactions received from cisgender/heterosexual disclosure recipients compared to social reactions received from SGM disclosure recipients. Only 15.5% of SGM survivors reported at least one negative social reaction from an SGM disclosure recipient, while 32.7% reported receiving at least one negative social reaction from a cisgender/heterosexual disclosure recipient. Over half, 59.1%, of participants reported receiving at least one positive social reaction from a cisgender/heterosexual disclosure recipient, while 70% reported receiving at least one positive social reaction from an SGM disclosure recipient.
Correlations Among Predictor and Outcome Variables for Total Sample.
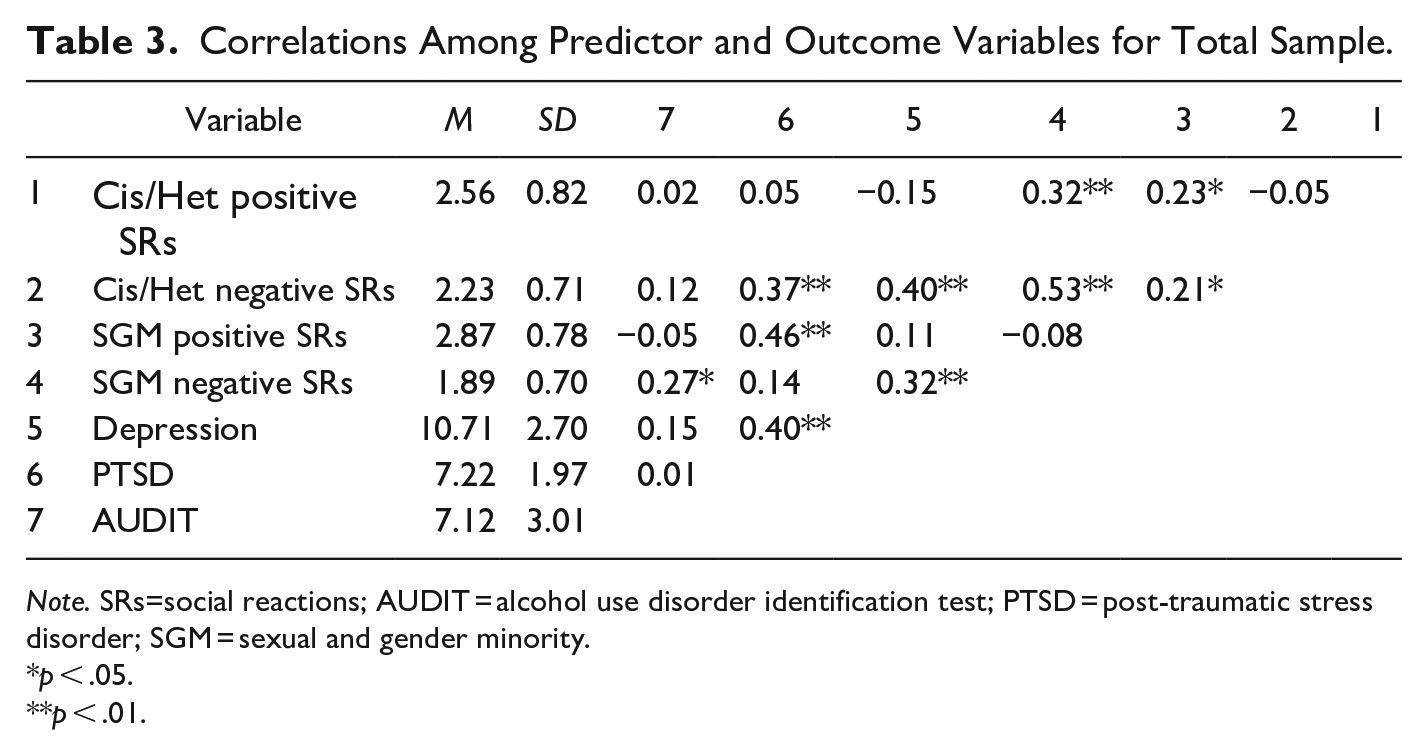
Note. SRs=social reactions; AUDIT = alcohol use disorder identification test; PTSD = post-traumatic stress disorder; SGM = sexual and gender minority.
p < .05.
p < .01.
Research Question 3: Social Reaction Association with Mental Health
Table 3 also provides correlations among social reactions and mental health outcomes. Table 4 presents regression models with mental health outcomes as the dependent variable, and social reactions from cisgender/heterosexual and SGM recipients as the main independent variable. Model 1, associating depression scores with social reactions, was significant and explained 22% of the variance in depression scores after adjusting for whether alcohol was involved during SV encounter (F[5,80] = 4.476, p < .001, R2 = .22). Positive social reactions from cisgender/heterosexual recipients (b = −0.84, p = .02) and negative social reactions from SGM recipients (b = 1.14, p = .04) significantly contributed to depression scores. For every one-unit increase in a positive social reaction from cisgender/heterosexual recipients, depression scores decreased by 0.84. For every one-unit increase in a negative social reaction from SGM recipients, depression scores increased by 1.14. Positive social reactions from SGM recipients and negative social reactions from cisgender/heterosexual participants were not significant predictors in this model.
Regression Model Coefficients for Those Who Disclosed to Both Cisgender/Heterosexual and SGM Recipients (N = 91).
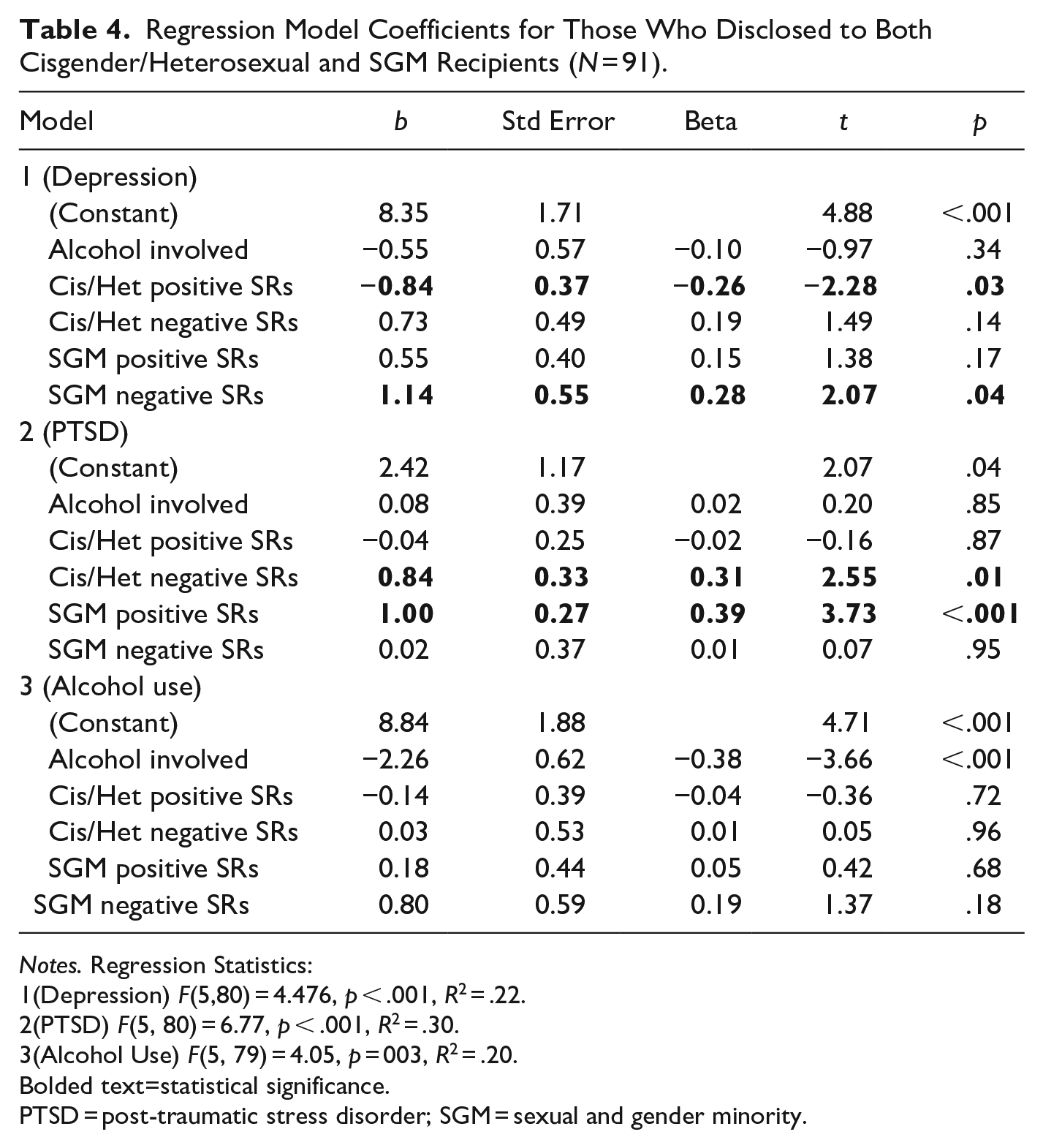
Notes. Regression Statistics:
1 (Depression) F(5,80) = 4.476, p < .001, R2 = .22.
2 (PTSD) F(5, 80) = 6.77, p < .001, R2 = .30.
3 (Alcohol Use) F(5, 79) = 4.05, p = 003, R2 = .20.
Bolded text=statistical significance.
PTSD = post-traumatic stress disorder; SGM = sexual and gender minority.
Model 2, associating PTSD scores and social reactions, was significant and explained 30% of the variance in PTSD scores after adjusting for alcohol involvement in the SV experience (F[5, 80] = 6.77, p < .001, R2 = .30). Negative social reactions from cisgender/heterosexual recipients (b = .84, p = .01), and positive social reactions from SGM recipients (b = 1.00, p < .001) significantly contributed to PTSD scores. For every one unit increase in a negative social reaction from cisgender/heterosexual recipients, PTSD scores increased .84. For every one-unit increase in a positive social reaction from SGM recipients, PTSD scores increased 1.00. Positive social reactions from SGM recipients and negative social reactions from cisgender/heterosexual recipients were not significant predictors in this model.
Model 3, associating problematic alcohol use with social reactions, was significant, and explained 20% of the variance in drinking scores after adjusting for alcohol involvement in the SV experience (F[5, 79] = 4.05, p = .003, R2 = .20). None of the predictors significantly contributed to the model.
Discussion
While the entire sample was disclosed to cisgender/heterosexual individuals, many also reported their SV to SGM individuals. This may be due to a preponderance of SGM individuals in their networks, and/or that SGM individuals are seeking to optimize the social reactions received. Indeed, our findings support the latter. SGM disclosure recipients provided more positive and fewer negative social reactions than cisgender/heterosexual disclosure recipients. It is possible that cisgender/heterosexual disclosure recipients, especially those with discriminatory attitudes toward SGM people, may possess less empathy for SGM survivors and therefore respond in more negative and less positive ways compared to SGM disclosure recipients. Hequembourg et al.’s (2021) study of sexual minority cisgender women experiencing SV found many participants deliberated intensely before disclosing to others. Anticipated stigma may likely be a component of this deliberation. These findings suggest that whereas all emerging adults could likely benefit from training in how to respond to disclosure of sexual assault from peers, cisgender/heterosexual students may be in most need of this type of programming.
As found in previous literature (Edwards et al., 2022a), social reactions were associated with mental health symptoms. However, our findings reveal that the strength and direction of this association are dependent on the SGM identity of the disclosure recipient. Depression was influenced in expected directions by positive social reactions from cisgender/heterosexual individuals and negative social reactions from SGM individuals. However, there was neither an association between negative social reactions from cisgender/heterosexual individuals nor positive social reactions for SGM individuals. This could be related to collapsing sexual and gender identities together; Flanders et al. (2022) report greater bisexual stigma from heterosexual individuals compared to cisgender participants for nonbinary individuals. Although existing literature highlights the ways how the identities of the person experiencing SV affect reactions (e.g., Ullman, 2021), more research may be needed to identify how the disclosure recipient’s identities affect whether a person discloses, their reaction, as well as the way the reaction is received.
Greater PTSD symptoms were associated with both negative social reactions from cisgender/heterosexual individuals as well as, surprisingly, positive social reactions from SGM individuals. Previous studies have shown that positive social reactions do not convey as many benefits as negative social reactions’ potential risk (Dworkin et al., 2019), but instead are associated with increased perceived control over recovery, adaptive social coping, and individual coping (Ullman & Peter-Hagene, 2014) Assessing coping methods among participants after SV and their disclosure of SV would have been useful to explain this unexpected finding. It may be that those who received positive social reactions also received more impactful negative social reactions and were unable to engage in adaptive social coping; however, positive and negative social reactions were not positively and significantly correlated in the data and we were unable to assess coping methods as a moderator.
Another explanation may be that individuals with greater PTSD symptoms only disclosed to other SGM individuals they perceived to be supportive. Additionally, it is possible that the associations between positive social reactions and PTSD are explained by other variables unaccounted for, such as sexual assault severity (Pegram & Abbey, 2019) or intensity of SGM stigma and gender visibility (Staples & Fuller, 2021). For instance, those who have greater transgender visibility, or those who are more likely to be perceived as transgender, experience more stigma and have reported more severe sexual assault (Staples & Fuller, 2021). The severity of SV experienced and the stigma experienced by SGM, both internally and externally, may complicate the post-victimization recovery process. Thus, the positive social reactions may be more of a reflection of the severity of the situation, potentially explaining why there was an association between positive social reactions from SGM individuals and PTSD.
In contrast to previous findings on the relationship between SGM SV and substance use outcomes (Blayney et al., 2021), social reactions, regardless of the sexual/gender identity of the disclosure recipient, were not associated with problematic alcohol use. This nonsignificant finding could be an artifact of our decision to measure alcohol use using a shortened version of the AUDIT, which focuses on alcohol use disorders. SGM individuals who experience SV may be drinking for a myriad of reasons and their drinking may not cross over into thresholds of disordered drinking. Therefore, a more sensitive measure (such as drinking to cope or drinking frequency/quantity) could have yielded different findings. Alternatively, it may be that the impact of social reactions on substance use is moderated by other factors, including high engagement with their own SGM communities that promote adaptive coping (Phillips li et al., 2020). Further, specific forms of SV experience (i.e., rape) have been associated with greater hazardous drinking (Blayney et al., 2021). As we did not account for the type of SV experience experienced, additional research is necessary to explore these nuances more thoroughly.
Overall, our findings add to the growing body of literature demonstrating the importance of social reactions on the mental health of survivors of SV, particularly among SGM survivors. We add nuance to this conversation by demonstrating that many SGM survivors of SV disclose this experience to other SGM individuals, and that the quality of the social reaction received is worse when the disclosure recipient is cisgender/heterosexual compared to SGM. Findings that the influence of social reactions on mental health is different depending on the sexual and gender identity of the disclosure recipient suggest that all students should receive training in providing positive social reactions, but also that this training should be tailored to the sexual/gender identity of the disclosure recipient. College campuses across the country have been developing and delivering social reactions trainings; however, only one known program has been rigorously evaluated (Supporting Survivors and Self; Edwards et al., 2022b). In this evaluation, the program appeared to be more effective at improving intentions to provide social reactions among SGM participants compared to cisgender/heterosexual participants. Future programs could be developed that capitalize on this by tailoring content to be specific to SGM disclosure recipients. Additionally, trainings provided to cisgender/heterosexual students should integrate content around SV for SGM individuals, as well as underscoring the influential role their social reactions have on the mental health of SGM survivors.
Limitations
We are limited by the cross-sectional nature of this study as we did not examine whether the mental health symptoms occurred concurrently, before, or after disclosure. Mental health symptoms have been shown to be associated with revictimization and with subsequent negative social reactions among heterosexual cisgender women (Ullman & Peter-Hagene, 2016). Considering our findings that positive social reactions from SGM disclosure recipients were associated with higher PTSD scores, longitudinal research is needed to examine the temporal ordering of that relationship. Relatedly, we did not ask about the severity of the SV experience, which limits our interpretation of the results, as it is a possible confounding variable.
Further, we were not able to separate social reactions from different types of recipients, such as social reactions from family versus friends, or friends versus formal support services, which may further explain variance in mental health outcomes. For instance, receiving negative social reactions from family compared to friends may have different impacts on their mental health (e.g., Lorenz et al., 2018). In addition, questions about participants’ specific SV experiences, such as duration, frequency, and type of harm experienced were not included in the study measures and served as a limitation to the study. Finally, the sample was recruited from the U.S. and future research can explore these relationships globally. Altogether, additional research is necessary to examine these more nuanced relationships and their impact on SGM survivors’ mental health.
Conclusions
Findings from the current study highlight the importance of understanding social reactions in relation to mental health outcomes among SGM college students. Future research is needed to better understand these associations and programming is also needed to enhance positive social reactions and reduce negative social reactions in response to SGM student disclosures. In addition to individual-level programming, efforts are also likely needed to enhance campus climate to be inclusive of and affirming to SGM students as hostile campus climates likely fuels negative social reactions to disclosures especially among cisgender/heterosexual students.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by funds from UNC Charlotte’s College of Health and Human Services.