
Abstract
Following a traumatic event such as intimate partner violence (IPV), survivors often experience stress related to the violence. These high levels of stress related to IPV can be associated with the daily activities of survivors and their relationships with their children, such as maternal–child bonding. The purpose of the current study is to explore the relationship between daily activities, daily stress levels, parenting self-efficacy and behaviors, and maternal–child bonding among survivors living in an IPV shelter using an ecological momentary assessment (EMA) methodology. Twenty-five mothers living in an IPV shelter in two states in the Southern United States completed a baseline survey and completed electronic daily diaries for 14 days. Higher daily stress was associated with the number of times the mothers met with the case manager. Higher daily stress was also related to lower parenting self-efficacy. The number of case management appointments and legal appointments were positively correlated with a higher bonding score. More social support was associated with more positive parenting. IPV and post-traumatic stress disorder symptoms were not significantly associated with maternal–child bonding, parenting behaviors, or parenting self-efficacy. Findings suggest that screening for maternal support may be particularly important for positive bonding and positive parenting. Findings also lend preliminary insight into practical places where service providers could act to protect the bonding process or mitigate risks to impede it. Future research should include objective data about the mother’s emotions and her interactive behavior with her child. There is also a need to consider how federal programs fund and incentivize service providers to focus on mother–child dyads and how they can tailor services that promote bonding.
Keywords
The consequences of intimate partner violence (IPV) are pervasive. According to the Centers for Disease Control and Prevention (CDC, 2022), IPV results in a variety of physical and mental health outcomes, many of which are chronic, ranging from depression and post-traumatic stress disorder (PTSD) symptoms to conditions that affect survivors’ digestive, reproductive, and nervous systems, heart, muscles, and bones. Additionally, exposure to IPV can have a variety of effects on children, including their physical and mental health, behavior, and academic achievement (Artz et al., 2014; Peterson, 2019; Ravi et al., 2022). Following a traumatic event such as IPV, survivors often experience stress related to the violence (Haight et al., 2022; Katz et al., 2016). Perceived stress is particularly pronounced among mothers experiencing IPV (Yim & Kofman, 2018). These high levels of stress related to IPV may be associated with the daily activities of survivors (e.g., studies/work, their leisure time, and family lives) and their relationships with their children, such as maternal–child bonding (Cirici Arnell et al., 2023). Recent studies highlight the association between the increase in the association between IPV and stress during the COVID-19 pandemic (Buttell et al., 2021; da Costa Siqueira et al., 2023). Additionally, research demonstrates survivors experience stress while living in an IPV shelter due to various environmental stressors, especially related to communal living (Leat, 2021; Robinson et al., 2020).
Maternal–child bonding is an emotional tie between the mother and her child that develops starting in utero and continues across the child’s lifetime (De Cock et al., 2016; Dubber et al., 2015; Kinsey & Hupcey, 2013). Maternal–child bonding has been shown to be positively associated with children’s behavioral, emotional, and cognitive development (Alhusen et al., 2013; De Cock et al., 2016; Ruiz-Ortiz et al., 2017). Most of the existing research on maternal–child bonding has focused on mothers and infants and has focused on the relationships between maternal (e.g., maternal age, marital status, educational level, and depression) or reproductive characteristics (e.g., number of children, duration of gestation, and whether the pregnancy was planned or desired; Tichelman et al., 2019). There is very little research investigating the associations between exposure to IPV on maternal–child bonding, but given the stress of IPV and living in an IPV shelter, maternal–child bonding could be a protective factor for both the mother and the child from social-emotional difficulties (Pinto et al., 2019). Although maternal warmth and effective parenting skills have been associated with the resilience of children exposed to IPV (Graham-Bermann et al., 2009), maternal–child bonding may also be negatively impacted by IPV (Goldblatt et al., 2014; Jones & Vetere, 2017; Moulding et al., 2015). The purpose of this study is to explore the associations between mothers’ daily stress, activities, social support, parenting behaviors, parenting self-efficacy, and maternal–child bonding with their children.
IPV, Stress, and Parenting
Research regarding the association between IPV and parenting behaviors has been mixed. Numerous studies and systematic reviews have examined the impact of IPV on parenting behaviors (Chiesa et al., 2018; Levendosky & Graham-Bermann, 2000; Sousa et al., 2021). A recent systematic review by Sousa et al. (2021) identified 64 studies that highlighted the association between IPV and lower parental support for the child, warmth, sensitivity, parent–child interaction or bonding, aggression, or abuse toward the child (e.g., Cox & Gustafsson, 2012; Holmes, 2013; Levendosky & Graham-Bermann, 2000). Similarly, Chiesa et al. (2018) found a positive correlation between IPV and physical and psychological aggression toward children in their meta-analysis. Psychological/emotional and sexual IPV, but not physical IPV, have been associated with spanking and lower maternal warmth (Postmus et al., 2012; Yoo & Huang, 2013). Further, several studies identified the indirect effects of maternal depression and parenting stress between IPV and the dependent variables of parenting behaviors, child maltreatment, and lower maternal warmth (e.g., Holmes, 2013; Loucks & Shaffer, 2014; Postmus et al., 2012; Sypher et al., 2022). Other scholars have not found direct or indirect relationships between maternal mental health and parenting warmth or behaviors among survivors (Levendosky & Graham-Bermann, 2000; Yoo & Huang, 2013).
Positive parenting (i.e., parenting characterized by caring, teaching, communication, leading, and addressing children’s needs consistently and unconditionally; Seay et al., 2014) has been found to buffer the effects of combined physical and psychological IPV exposure on children (Miller-Graff et al., 2016; Nixon et al., 2017). Sousa et al. (2021) identified 41 studies in their meta-analysis that challenge the assertion that IPV victimization was related to negative parenting behaviors. For instance, Casanueva et al. (2008) did not find any significant differences in parenting behaviors between IPV survivors and individuals not exposed to IPV in their study (N = 1,943). They also reported that there was no significant relationship between current or past IPV and the risk of spanking.
Other scholars have reported a positive association between IPV and parenting effectiveness, maternal–child attachment, and maternal warmth (Buchbinder, 2004; Scrafford et al., 2022). Scholars have highlighted that many survivors strive to make their home a warm and safe place despite IPV and that compassion and nurturance informed their parenting and discipline strategies (Buchbinder, 2004; Scrafford et al., 2022). Additionally, research demonstrates that survivors engage in one-on-one activities and compliment their children to boost their self-esteem (Lapierre, 2010; Nixon et al., 2017). For instance, Nixon et al. (2017) found in their study with 350 survivors that 94% reported showing affection and participating in activities with their children to help them feel good about themselves.
Parenting Self-Efficacy
IPV can also be associated with mothers’ parenting self-efficacy (i.e., a parent’s beliefs about their effectiveness as a parent; Hamilton et al., 2015), especially when they have difficulties providing for their children due to IPV (Sousa et al., 2021). At times, the abusive partner may attempt to undermine mothers’ parenting self-efficacy and mother–child bonds (Goldblatt et al., 2014). For instance, researchers have reported that abusive partners would interfere with the breastfeeding relationship, such as controlling how the mother held the baby to nurse and the duration of the feeding (Goldblatt et al., 2014; Jones & Vetere, 2017).
More than 20 studies indicate that survivors may feel inadequate as mothers, which, in turn, affects their mental health (Sousa et al., 2021). Other studies highlight motherhood as an identity that provides mothers experiencing IPV with a sense of meaning, agency, and purpose (Semaan et al., 2013; Sousa et al., 2021; Wendt et al., 2015). For example, Semaan et al. (2013) identified that for many women, motherhood was a source of strength and affirmation and an area of life they felt positive about and that they could control.
Social Support
When possible, survivors seek social support from informal (e.g., family, friends, and coworkers) and formal sources (e.g., social workers, policy, IPV service providers, childhood intervention, and protection workers; Letourneau et al., 2013; Stylianou et al., 2021). The impact of violent relationships can lead to decreased levels of social support for survivors (Katerndahl et al., 2013). In general, social support relates to the material and psychological resources that individuals may have experienced or perceived having from others (Cohen, 2004; Rains & Wright, 2016). Emotional support is a particularly advantageous form of social support accessible to the support seeker’s physical and mental well-being (Erculj & Ziberna, 2022; Zhu et al., 2018).
Although not all survivors receive social support from informal sources such as friends and families (Park & Ko, 2021; Stylianou et al., 2021), numerous studies have shown the critical role that support networks play in improving the mental health and resilience of survivors (Amar et al., 2015; Machisa et al., 2018; Pinto et al., 2019). Survivors living in IPV shelters have reported mixed experiences with social support while in shelters (Stylianou et al., 2021). In some cases, survivors report increased social support through relationships and services provided at the shelter, while others experience barriers to accessing their existing support systems due to shelter policies and geographical distance (Stylianou et al., 2021).
Existing research demonstrates that social support is associated with positive parenting and maternal communication (Taylor, 1996; Taylor et al., 2008). Among survivors of IPV, a lack of social support has been associated with lower levels of positive parenting (Levendosky & Graham-Bermann, 2000). Levendosky et al. (2003) reported an indirect effect between social support and parenting effectiveness via lower trauma and depressive symptoms. Other studies demonstrate that the social support provided by peer groups, service providers, and group interventions decreased psychological distress and strengthened maternal–child relationships and parenting capacity among survivors (Grip et al., 2011; Letourneau et al., 2013; Mitchell et al., 2006).
Parenting and Maternal–Child Bonding in an IPV Shelter
Emergency shelters are often used as a last resort for protecting women experiencing severe IPV (Chanmugam, 2011; Haj-Yahia & Cohen, 2009; Helfrich et al., 2008). Children’s lives may become disrupted as a result of the numerous changes they go through as they transition from the community to IPV shelters and back again (Vass & Haj-Yahia, 2020). Although there are numerous studies on attachment and the parent–child relationship, comparably much less is known about how living in a shelter is associated with the primary attachment bond, particularly as viewed from the parents’ perspective (Herland & Helgeland, 2017; Swick & Williams, 2010). Several studies have explored mothers’ experiences parenting in homeless and IPV shelters and the role of parenting surveillance by shelter staff to ensure mothers are following the shelter rules related to parenting (e.g., Anthony et al., 2018; Fauci & Goodman, 2020; Glenn & Goodman, 2015; Wood et al., 2017).
Anthony et al. (2018) explored parent and child experiences of homelessness and residing in emergency shelters from parents’ perspectives. They situated their analysis within an attachment perspective, suggesting that parents’ feelings of disempowerment over their parenting role can impact the parent–child relationship (Anthony et al., 2018). For instance, the rule that parents have to be near their child at all times does not allow the time for the mother and child to have time away from each other to “relax, regroup, and recharge,” which can be beneficial for the parent–child relationship (Anthony et al., 2018, p. 12). In another qualitative study of mothers living in an IPV shelter, Glenn and Goodman (2015) found that the shelter rules that required even brief separation (e.g., during meetings or while residents complete chores) had a negative emotional impact on children. The current methods used to analyze maternal–child bonding in shelters have been limited, though, since they typically rely on only one time point rather than across multiple days and are subject to recall bias.
Ecological Momentary Assessment in IPV Shelters
One methodological approach to address these limitations is ecological momentary assessment (EMA) (Shiffman et al., 2008). EMA is used to track changes in daily experiences over time from participants in their natural environments and often with minimal researcher intrusion. Resultant data should reflect less recall bias. Moreover, EMA is based on repeated measures over time and theoretically can provide more reliable assessments of human behavior than single point-in-time estimates. EMA is further unique in that it generates daily data from participants in natural settings, thereby reducing recall bias while showing variability in daily behaviors over time (Shiffman et al., 2008)
Few studies have utilized an EMA to collect data related to IPV. Of these, most of the existing studies have analyzed IPV perpetration and victimization data among college students (Derrick & Testa, 2017; Moore et al., 2011; Shorey et al., 2014; Waterman et al., 2019) or community samples (Derrick & Testa, 2017). Study length ranged from 3 weeks to 90 days. Of note, two studies were one-time retrospective interviews in which participants recalled their experience on a weekday and weekend (McNulty et al., 2009) or over the past 90 days using a timeline follow-back method (Stappenbeck et al., 2016).
Only two studies included a sample of all IPV survivors (McNulty et al., 2009; Sullivan et al., 2011). Sullivan et al. (2011) recruited IPV survivors living in the community and focused on incidences of violence. McNulty et al. (2009) included a sample of survivors living in an IPV shelter with the objective of collecting information about the daily activities of survivors living in an IPV shelter but did so retrospectively using interviews. The purpose of the current study is to explore the relationship between daily activities, daily stress levels, social support, parenting self-efficacy and behaviors, and maternal–child bonding among survivors living in an IPV shelter using an EMA methodology.
Method
Participants
Twenty-five mothers participated in the study. Table 1 provides details about the sample regarding racialized identities. The majority of the participants reported racialized identities as Black or White (96%). Specifically, 52% (n = 13) identified as Black/African American, 44% (n = 11) identified as White, and 4% (n = 1) identified as Multiracial. The vast majority of the mothers, 92% (n = 23), identified as Straight/Heterosexual, and 8% (n = 2) as Bisexual/Pansexual/Queer. The mean ages of the mothers and children were 31.88 (SD = 5.55, range 22–41 years) and 6.45 (SD = 3.72, range 2–13 years), respectively. Results also reveal that 24% (n = 6) of mothers had a high school degree, while 40% (n = 10) of mothers had some college experience. Also, 20% (n = 5) of mothers indicated they had full-time employment prior to residing at the IPV shelter, and 40% (n = 10) of mothers revealed they were not working and were not currently looking for work with 56% (n = 14) of mothers at the IPV shelters revealing they cannot make ends meet for their current financial situation. However, 40% (n = 10) of mothers reported that they did have enough to make ends meet for their current financial situation.
Sample Description (N = 25).
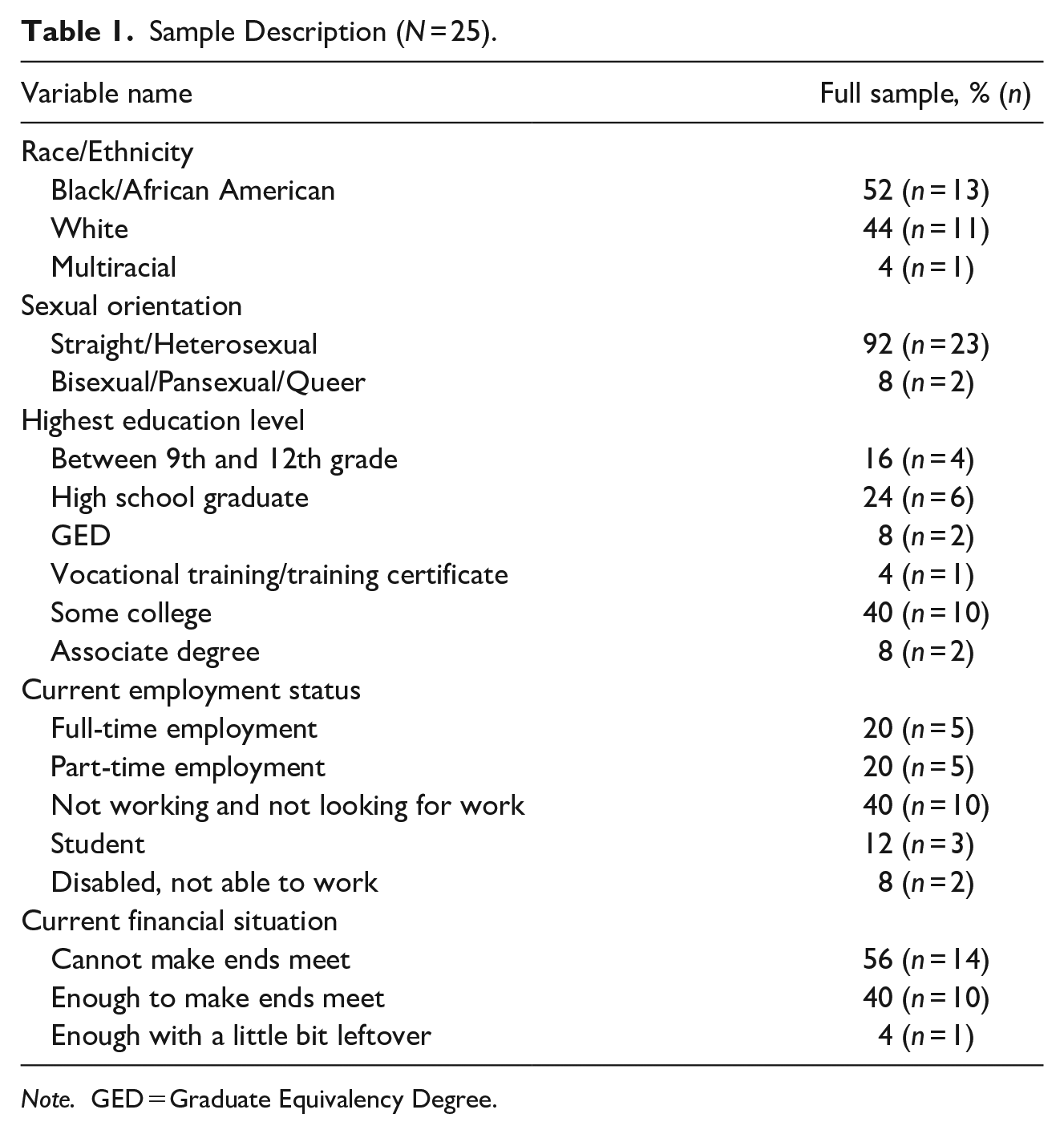
Note. GED = Graduate Equivalency Degree.
Procedure
The researchers utilized tablets and electronic links to provide consent and facilitate data collection depending on where the survivor was located. The original study design included providing tablets to a local shelter near the researcher’s university for data collection, but due to recruitment challenges (see Ravi et al., 2023), the researchers expanded the study to shelters both within and outside of the state. Prior to recruitment, the first author and a master’s level graduate research assistant set up and loaded three Qualtrics links onto each tablet. The first link was a link to a consent form. The second was a link to a baseline survey, and the third was a link to the daily diary. The researchers loaned the tablets to the shelter for the duration of the study. Survivors who resided in other shelters utilized links that were sent to them via text message.
Upon university institutional review board approval, survivors were recruited from three shelters and one transitional housing program in two southern states in the United States. Mothers were eligible to participate if they were living in an IPV shelter or transitional housing program with their children who were between the ages of 2 and 17. Case managers provided flyers to survivors with children within that age range. Mothers who were interested in the study texted or called the first author for additional information about the study. The first author called the mothers, who sent a text to explain the study and confirm eligibility. Once eligibility was confirmed, a member of the research team scheduled a Zoom meeting to obtain informed consent and conduct the baseline survey.
The survivors in the local shelter were directed to check out a tablet from the front desk at the shelter and received a copy of the informed consent document prior to the Zoom meeting. Survivors who lived in a different shelter or in transitional housing were asked if a copy of the consent form could be emailed to them to review prior to the Zoom meeting. During the Zoom meeting, a member of the research team provided instructions on how to access the link to the informed consent document. The member of the research team reviewed the informed consent document with the survivor. Participants who consented to participate in the study were directed on how to access the link to the baseline survey. The participants completed the baseline survey on their own while the members of the research team remained on Zoom to answer any clarification questions that the participants had. Upon completion of the baseline survey, a member of the research team provided instructions on how to access the link to the daily diary that the participant would complete. The participants completed the daily diaries for 14 days. They received a reminder text each day and were provided an electronic $10 Walmart gift card for each diary completed. A member of the research team reviewed Qualtrics each morning to ensure that the participant had completed the daily diary and emailed the participant a gift card each day that they completed a daily diary. The university institutional review board approved this study prior to recruitment and data collection activities.
Measures
Daily Diary Measures
Maternal–Child Bonding
We utilized a researcher-created daily measure of bonding based on Fusco’s (2017) attachment questions. Which included “I am able to soothe my child,” “I am able to soothe my child when he/she is upset,” and “I am happy being with my child.” The response items ranged from 1 = Strongly disagree to 5 = Strongly disagree. Participants were also asked to report the number of times they played with their child, read with their child, cuddled with their child, and the number of times they gave their child a hug and kiss, respectively. The response options ranged from 0 to 5 or more times. A seven-item mean bonding index was created by combining the responses to the bonding items across the 14 days. The Cronbach’s alpha for the bonding index for the same was .72, indicating acceptable reliability. When examining the missing data for the bonding variables, results indicated that missing data ranged from 3.1% for the item “felt happy around my child” to 9.7% for the item “read to my child.”
Daily Activities
Participants also reported the activities that they completed each day in a check box format (check all that apply) developed by the research team. Options included “took my child to school or childcare,” “went to job training/school,” “went to work,” “met with a case manager,” “visited with friends/family,” “did something recreational (movie, clothes shopping, etc.),” and “went to park/hiking/biking/outdoors.” There was no missing data for these items.
Daily Stress
Participants rated their daily stress level on a researcher team-developed scale that ranged from 1 = very low to 6 = very high. The results revealed that the missing data was 2.4% for the mother’s daily stress level.
Baseline Measures
Intimate Partner Violence
IPV was measured using the mean score of the 15-item Composite Abuse Scale—Short Form (Ford-Gilboe et al., 2016). Example items include “Blamed me for causing their violent behavior,” “Tried to convince my family, children, or friends that I am crazy or tried to turn them against me,” and “Forced or tried to force me to have sex.” Participants are asked whether any of the items have ever happened to them, and if yes, they are asked how often they occurred in the past 12 months (1 = never to 7 = almost daily). The Cronbach’s alpha for the current sample was .90, indicating excellent internal consistency. The missing data for the IPV variables indicated a range from 15.2% for 11 items (i.e., “Partner tried to convince my family, children, or friends that I. . .,” “Partner used or threatened to use a knife or gun or another weapon,” “Partner made me perform sex acts that I did not want to perform,” “Partner followed me or hung around outside my home or work,” “Partner threatened to harm or kill me or someone close to me,” “Partner choked me,” “Partner forced me or tried to force me to have sex,” “Partner harassed me by phone, text, email, or using social media,” “Partner hit me with a fist or object, kicked or bit me,” “Partner confined or locked me in a room or other space,” and “Partner kept me from having access to a job, money, or financial resource”) to 21.2% for two items “Partner blamed me for causing their violent behavior” and “Partner shook, pushed, grabbed, or threw me.”
PTSD Symptoms
PTSD symptoms were assessed using the mean score of the five-item Primary Care PTSD Screen for DSM-5 (PTSD-5; Prins et al., 2015). The PTSD-5 is a screening tool to identify individuals who may have PTSD. Participants are asked to respond (yes/no) to whether they experienced symptoms of PTSD in the past month, such as “been constantly on guard, watchful, or easily startled” or “felt numb or detached from people, activities, or your surroundings.” Scores range from 0 to 5. The Cronbach’s alpha was .66, which indicated lower but still acceptable reliability, potentially due to the small number of items (Tavakol & Dennick, 2011).
Parenting Self-Efficacy
Parenting self-efficacy was measured using the mean score of the three-item self-efficacy subscale of the Me as a Parent Scale (Hamilton et al., 2015). Example items include “I have all the skills necessary to be a good parent to my child” and “I know I am doing a good job as a parent.” Participant responses range from 1 = strongly disagree to 5 = strongly agree. The Cronbach’s alpha for the current sample is .83 indicating good reliability. Missing data for the self-efficacy variables revealed a range of 15.2% for all items except one (i.e., “I know I am doing a good job as a parent” and “I have all the skills necessary to be a good parent to my child”) to 18.2% for the item “I have confidence in myself as a parent.”
Positive Parenting Behaviors
The mean scores of the five-item positive parenting subscale and the 10-item involvement subscale of the Alabama Parenting Questionnaire (Frick, 1991) were used to measure parenting behaviors. The positive parenting subscale includes items such as “You reward or give something extra to your child for obeying you or behaving well” and “You tell your child that you like it when he/she helps out around the house.” When examining the missing data for positive parenting, the results demonstrated a range of 15.2% for all items except for one (i.e., “You let your child know when he/she is doing a good job with something,” “You reward or give something extra to your child for obeying you or behaving well,” “You praise your child if he/she behaves well,” and “You tell your child you like it when he/she helps out”) to 18.2% for the item “You hug or kiss your child when he/she does something well.” The parent involvement subscale includes items such as “You play games or do other fun things with your child” and “Your child helps plan family activities.” Participant responses range from (1 = never to 5 = almost always). Both the positive parenting (α = .72) and involvement (α = .85) subscales demonstrate acceptable to good reliability. One item from the involvement scale related to attending a parent-teacher association meeting was dropped due to the amount of missing data due to most of the data collection occurring in the summer. The missing data for the parent involvement variables indicated a range from 15.2% for the items “You have a friendly talk with your child” and “You play games or do other fun things with your child” to 27.3% for the items “You volunteer to help out with special activities that your child is involved in (such as sports, boy/girls scouts, church youth groups),” “You help your child with his/her homework,” and “You drive your child to a special activity.”
Social Support
Social support (i.e., tangible, affectionate, positive social interaction, emotional, and informational support) was measured using the mean score of the Medical Outcomes Study Social Support Survey (Holden et al., 2014). Participants are asked to respond to the prompt “How much of the time would you say you CURRENTLY have someone in your life who could” for various items related to social support such as “take you to the doctor,” “do something enjoyable with,” and “low and make you feel wanted.” Participant responses ranged from (1 = none of the time to 5 = all of the time). Cronbach’s alpha for the total scale in the current sample is .89, which demonstrates strong reliability. Results for the missing data for the social support variables indicated that the missing data ranged from 15.2% for all items except one (i.e., someone to “help if confined to bed,” “take you to the doctor,” “share your most private worries and fears,” “do something enjoyable with,” and “love and make you feel wanted”) to 18.2% for the item “turn to for suggestions about problems.”
Data Analysis
All data analyses were conducted using SPSS v.29. Before conducting the main data analysis. The first, second, and third authors met to assess the amount and type of missing data and determine patterns among the missing data. Based on the missing data analysis, the researchers determined that the missing data were due to missing at random (MAR). The researchers used multiple imputation to address the missing data since the maximum amount of missing data was 27.3% and data were MAR (Enders, 2010). All variables were included to create the imputed dataset.
Upon completion of the imputation process, the researchers aggregated the daily diary entries for daily stress, daily activities, and bonding using the aggregate feature in SPSS. The aggregated scores were merged with the baseline data. The researchers used descriptive statistics to analyze the frequency and type of daily activities and bonding behaviors and perceptions. Descriptive statistics (means and standard deviations) were utilized to assess the frequency of IPV, bonding, daily stress, PTSD symptoms, parenting self-efficacy, and social support. Pearson’s correlation coefficient provided information about the association between the key study variables.
Results
Table 2 results show the mean score for the mother’s daily stress was M = 3.13 (SD = 0.88). The mean bonding index scores were M = 181.69 (SD = 52.61). Results also indicate for the daily activities, meeting with a case manager, and going to a legal appointment, the mean scores were M = 2.72 (SD = 2.26) and M = 0.44 (SD = 0.65), respectively. In terms of IPV, social support, and PTSD symptoms experienced by mothers, the results reveal mean scores of M = 64.99 (SD = 18.72) for IPV, M = 16.64 (SD = 7.12) for social support, and M = 4.20 (SD = 1.17) for PTSD. Additionally, the findings indicate parenting involvement had a mean score of M = 4.17 (SD = 0.70), and positive parenting had a mean score of M = 4.67 (SD = 0.41). Finally, parent self-efficacy indicated a mean score of M = 11.86 (SD = 2.29) in Table 2.
Mean Scores and Standard Deviations of Key Variables (N = 25).

Note. IPV = intimate partner violence; PTSD = post-traumatic stress disorder.
Table 3 displays the bivariate results, which indicate that higher daily stress was associated with the number of times the mothers met with the case manager (r = .63, p < .01). Higher daily stress was also related to lower parenting self-efficacy (r = −.48, p < .05) but not bonding. Additionally, the number of case management appointments and legal appointments were positively correlated with a higher bonding score (r = .40 and r = .44, respectively, all p < .05). More social support was associated with more positive parenting (r = .42, p < .05), and bonding (r = .41, p < .05). In addition, social support was also positively correlated with legal appointment visits (r = .46, p < .05). Further, positive parenting was positively related to legal appointment visits (r = .53, p < .01). The results also reveal a positive association between PTSD and IPV (r = .55, p < .05). Lastly, results in Table 3 show that parent self-efficacy is positively correlated with parent involvement (r = .45, p < .05). IPV and PTSD symptoms were not significantly related to maternal–child bonding, parenting behaviors, or parenting self-efficacy.
Bivariate Correlations of Key Variables (N = 25).
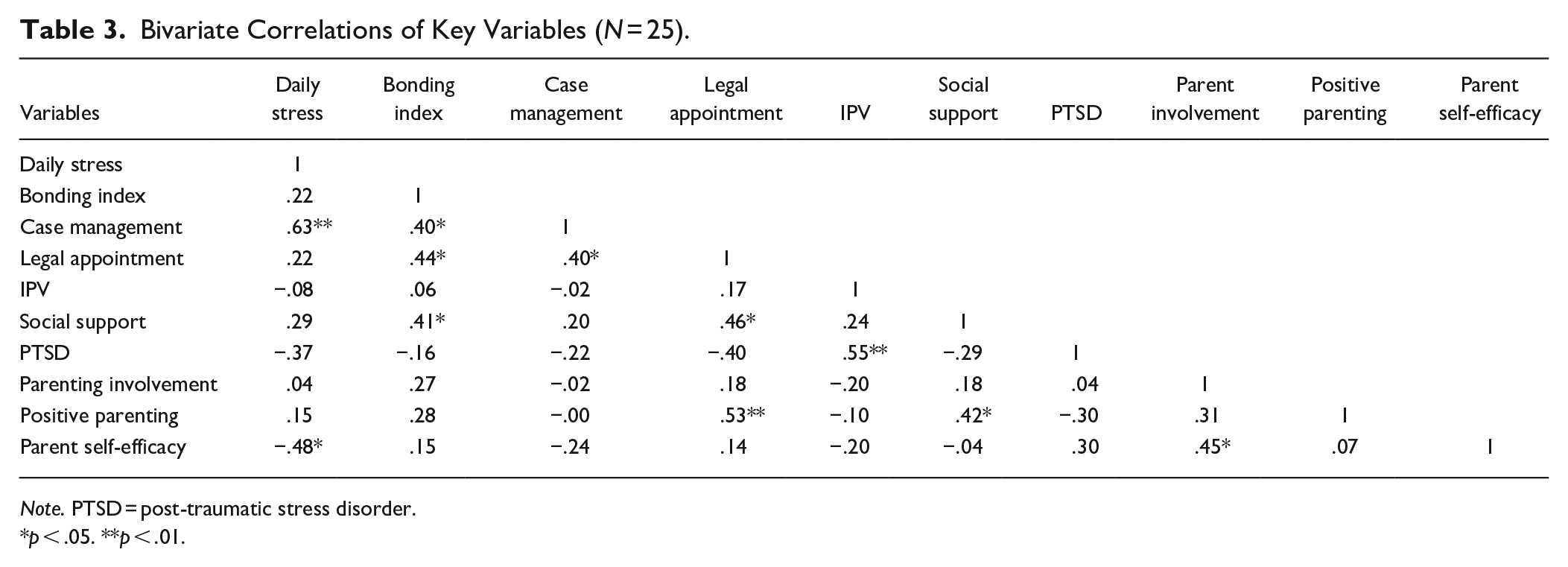
Note. PTSD = post-traumatic stress disorder.
p < .05. **p < .01.
Discussion
This study aimed to investigate factors influencing maternal-child bonding among mothers and children living in emergency or transitional shelters after fleeing IPV. It represents one of the very few efforts to link daily experiences within the stress of relocation and IPV-induced trauma with this parenting process, which has been shown to be essential to healthy child development. Our study shows evidence that maternal–child bonding is positively associated with mothers’ daily activities attending to case management and legal services. As an exploratory study, our results do not offer an explanation for the relationship, but they do offer areas for future research. The relationship may be indirect in that taking care of key activities necessary for exiting an IPV relationship allows mothers more time or emotional energy to focus on their children. This supposition is further strengthened by our finding that social support was positively associated with maternal–child bonding. Some research shows the benefits of social support among mothers (Amar et al., 2015; Emmanuel et al., 2011; Machisa et al., 2018), and specifically maternal–child bonding (McGuire-Schwartz, 2007). Our findings are consistent with existing studies related to social support positive parenting and maternal–child bonding (Emmanuel et al., 2011; Levendosky & Graham-Bermann, 2000; Machisa et al., 2018; McGuire-Schwartz, 2007; Taylor, 1996; Taylor et al., 2008). While there are some studies exploring social support among IPV survivors, our study represents the first linking social support to maternal–child bonding within IPV. As such, our ability to explain the relationship in our sample is purely speculative at this point but clearly warrants further investigation.
It is possible that both the practical and social processes that case management and legal services provide have a very beneficial effect on mothers exiting IPV. It is also possible that the results are evidence of pre-existing differences among the mothers in this sample and that mothers with the strongest bonds with their children may have been more likely to engage in case management and legal services. Future research could statistically control for this potential sampling bias by measuring maternal–child bonds at the time of study enrollment and then controlling for baseline bonding in the analyses.
Other interesting patterns also emerged in the data, specifically the positive association between stress and case management appointments and the negative association between stress and parenting self-efficacy. The scope of our study precludes an explanation for the somewhat counter-intuitive relationship between higher stress and more case management, but temporal ordering could be one explanation. It is possible that the women sought out case management more often when they were experiencing higher stress levels. Regardless, this is an area for future research to understand the mechanisms by which case management helps women in these situations and whether there are any unintended negative consequences of case management interactions. In contrast, the negative relationship between stress and parenting self-efficacy is intuitive given that conceptually, self-efficacy involves feeling able to overcome obstacles and having the capacity to act. Lower stress would seem to contribute to a higher sense of capacity.
The current study did not find a significant association between the frequency of IPV and the dependent variables of maternal–child bonding, parenting behaviors, and parenting self-efficacy. This non-significant association differs from existing studies, which have found that IPV was significantly related to harsher parenting or lower maternal warmth (Chiesa et al., 2018; Levendosky & Graham-Bermann, 2000; Sousa et al., 2021). The non-significant finding also differs from research that showed IPV can be associated with parenting effectiveness, maternal–child attachment, and maternal warmth (Casanueva et al., 2008). It is plausible that the current study did not find significant findings due to the small sample size compared to studies with larger sample sizes and more statistical power (e.g., Casanueva et al., 2008; Levendosky & Graham-Bermann, 2000; Yoo & Huang, 2013). Additionally, variable measurement may have contributed to the differences in the findings. Larger existing studies (Casanueva et al., 2008; Cox & Gustafsson, 2012; Levendosky & Graham-Bermann, 2000; Yoo & Huang, 2013) used researcher observations of maternal–child interactions, whereas the current study utilized self-report. Further, the majority of existing studies (e.g., Cox & Gustafsson, 2012; Holmes, 2013; Loucks & Shaffer, 2014; Sypher et al., 2022) measured IPV using the conflict tactics scale, whereas this study used the Composite Abuse Scale-Short Form (Ford-Gilboe et al., 2016).
This study also did not find a significant relationship between trauma symptoms and the dependent variables of maternal–child bonding, parenting behaviors, and parenting self-efficacy. Our finding is consistent with existing research that identified a non-significant direct relationship between maternal trauma symptoms and maternal warmth and non-supportive parenting (Gurtovenk & Katz, 2020; Levendosky & Graham-Bermann, 2000). However, our findings differ from Greene et al. (2018), who found that PTSD symptoms mediated the relationship between IPV and mothers’ restrictive/punitive parenting in a sample of 308 mother–child dyads. Other studies conducted by Levendosky and Graham-Bermann (2000) and Levendosky et al. (2003) combined trauma symptoms, depression symptoms, and other psychological symptoms into a variable termed “negative maternal psychological functioning,” which was significantly related to lower positive parenting; however, it is not possible to identify to what extent trauma symptoms impacted parenting behaviors. Finally, parenting stress has been shown to mediate the relationship between IPV and negative parenting behaviors (Loucks & Shaffer, 2014; Sypher et al., 2022). Future studies should consider including parenting stress in addition to trauma symptoms.
Study Limitations and Implications for Future Research
It is important to underscore that the findings were based on an observational study. Therefore, no claims about causality or direction of effects can be made. Our study focused on mothers residing in shelters within the Southern United States, and findings from our study might not generalize to other populations. Larger, more diverse studies are needed to test out casual pathways among more IPV survivor mothers who are more representative of the population, including Indigenous, Latina and Asian American, LGBTQ+, and immigrant survivors. A larger and more diverse sample would allow for the exploration of bonding across racial and ethnic groups. Qualitative research related to bonding among culturally diverse mothers could inform culturally responsive interventions. It is important to understand how mothers from diverse backgrounds define and engage in bonding activities with their children. Additionally, research is needed with Black, Indigenous, People of Color (BIPOC) survivors and LGBTQ+ mothers in order to understand how structural factors such as racism and homophobia could create additional stressors and unique needs influencing maternal–child bonding. Finally, our study used an innovative method, EMA, that poses both benefits and potential limitations to the validity of the results. By asking participants to complete the same set of questions daily for 14 days, we may have influenced them to change their behaviors. For example, as participants responded to the positive parenting scale, they may have become more aware of positive parenting behaviors and adjusted their behaviors accordingly. While this response bias is possible, we did not observe significant shifts in participants’ responses over time, indicating that there were fairly stable trends and that such a risk, while possible, was minimal in this study.
The small sample size also precludes the ability to control for confounding variables and reduce omitted variable bias. Moreover, we conducted a number of statistical tests, so the results should be interpreted with caution. Although this is the first study to utilize experience sampling, consistently obtaining data proved challenging. Future research is needed to examine potential barriers for mothers.
Maternal ratings could also be subject to social desirability bias. Mothers may present a positive view of their relationship with their children, particularly if they feel vulnerable living in temporary housing. Mothers may be more likely to report a higher sense of self-efficacy, positive parenting, and involvement than they would if they were not in transitional housing. Moreover, mothers’ subjective appraisal of their degree of bonding may differ from the child’s experience. It would be particularly informative to get objective information about the mother’s emotions and her interactive behavior with her child. Collecting observational maternal–child interaction and other dyadic information would be useful. It would also be useful to get child perceptions of their mother’s bonding and involvement along with children’s perceptions of their own bonding with their mother. Future research should consider collecting data directly from children to understand their perspective of the relationship with their mothers. It is also important to note that our measure of maternal–child bonding assessed items related to parent soothing ability, which may measure emotion regulation and be confounded with child temperament. The frequency with which a parent engages in activities with their child does not directly assess the affective quality of the activity. Moreover, there was a large age span (ages 2–13 years), so some of the activities may not have been of interest or developmentally appropriate or age-typical for the child (e.g., “read with your child”). This may have underestimated the maternal bonding with older children. It would also be important to examine relations at different developmental periods as the nature of the bonding relationship and activities and the children’s needs will vary. Indeed, during developmental transition periods such as early childhood and early adolescence, instances of heightened emotional and sleep dysregulation may make maternal bonding and positive and involved parenting particularly difficult. Moreover, it would be important to examine mothers’ emotions and sleep dysregulation as our findings showed that IPV was significantly associated with maternal PTSD, of which disrupted sleep is a symptom. Future research should examine synergistic relations between emotion and sleep patterns of mothers who have experienced IPV and their children residing in residential shelters.
Additionally, our study did not separate tangible and emotional social support. Future research could focus on exploring whether there are any differences in the benefits of social support based on the type of social support. Future research should consider parsing out formal and informal social support (e.g., social support from case managers and shelter support groups) based on the findings from existing studies examining formal social support within IPV shelters (Grip et al., 2011; Letourneau et al., 2013; Mitchell et al., 2006). Moreover, it would be particularly interesting to examine instrumental (e.g., providing transportation) versus emotional, social support (e.g., expressing empathy) mothers in IPV shelters as they may have different associations with maternal bonding and positive parenting (Morelli et al., 2015). We encourage further study into the specific sources of social support that are helpful for mothers and specific aspects of case management that support them, as well as potentially detrimental aspects.
Despite these limitations, there are many strengths. It is important to note that, despite the small sample size, we were able to engage and conduct this study with a very hard-to-reach and transient population. To our knowledge, this is the first study to examine maternal bonding and parenting among mothers in an IPV shelter. Therefore, we contribute to and extend prior literature to demonstrate important correlates of maternal bonding and parenting, such as social support, among this population.
Practice and Policy Implications
Our findings suggest that screening for maternal support may be particularly important for positive bonding and positive parenting. Assessments of the type and quality of support in a mother’s life would be important for service providers to consider. Although it would need to be tested, it is possible that interventions designed to increase maternal social support may lead to increases in maternal–child bonding and parent involvement (for a review of social support interventions, see Ogbe et al., 2020). Moreover, it may be particularly important to assess parent self-efficacy in mothers due to the link with parent involvement. Interventions designed to enhance parent self-efficacy, such as those used with infants, may be adapted for parental relations with older children to demonstrate increases in parental involvement (Shoemark et al., 2021). In shelters, however, it may be most practical and feasible to observe the type and quality of the activities in which the mother and child engage as it may provide some information regarding mothers’ bonding. Among mothers who have experienced trauma, Mom Power (Rosenblum et al. 2017) is an intervention that has been demonstrated to be effective in improving maternal mental health and parenting of young children. Paraprofessionals could be trained to provide the group intervention or potentially some components of it to mothers. Additionally, Mom’s Empowerment Program (Howell et al., 2015), an evidence-based intervention to promote positive parenting among mothers who have experienced IPV, could be a beneficial intervention for mothers who have experienced IPV, though a shorter intervention would likely be needed for the shorter lengths of shelter stays.
Findings also lend preliminary insight into practical places where service providers could act to protect the bonding process or mitigate risks to impede it. Overall, these findings suggest that linking mothers with other people who are able to help them attain the resources that they need for independence is a critical service that providers should not overlook within their programs. Helping the mothers feel as though they have a support network and that this support network can help them overcome logistical and legal hurdles that impede independence.
Programmatic efforts to reduce women’s stress could be very beneficial for women in their roles as mothers. While many stressors in women’s lives are outside of the organization and programmatic control, they can think strategically about what factors they can alter to reduce stress. For example, organizations offering emergency or transitional housing could consider how the physical living space calming environments such as access to nature and green outdoor space (Peters et al., 2021) and private, quiet indoor space.
Given the preliminary and exploratory nature of our study, emergent policy implications are nascent at best. However, the central thesis of maternal–child bonding within our study and its relationship to service activities does point toward a need to consider how federal programs fund and incentivize service providers to focus on mother–child dyads as a specific client population and how they can tailor services that promote bonding. For example, the Office of Violence Against Women or Department of Justice might consider funding demonstration projects for parent ambassadors or navigators within shelters to serve as unique peer support for mothers. Alternatively, policymakers and funders could support more programming within shelters that engage mothers and children with mutual activities such as baking, gardening, and hiking that reinforce relationships through time together and shared tasks and accomplishments. Finally, the positive relationship of legal services with bonding underscores the ongoing critical importance of the law in helping women exit from IPV relationships and gain independence from IPV perpetrators. Family Justice Centers may be uniquely positioned to consider how maternal advocates or peer support within their program could be matched with IPV survivors who are mothers to help them with unique legal issues such as child custody.
Conclusion
This study is one of the first studies to utilize EMA methodology within an IPV shelter. Our study explored the association between daily activities, parenting behaviors and self-efficacy, social support, and maternal–child bonding. One of the most important findings from this study was the association between social support and positive parenting while living in an IPV shelter. Future research is needed to further investigate this relationship with larger, more diverse samples.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received funding for this research from the University of Tennessee Professional and Scholarly Development Award.