
Abstract
The Veterans Justice Outreach (VJO) program of the U.S. Veterans Health Administration has a primary mission of linking military veterans in jails, courts, or in contact with law enforcement to mental health and substance use disorder treatment. National data of veterans with VJO contact were used to describe demographic characteristics, and mental health and substance use disorder diagnoses and treatment use and test correlates of treatment entry and engagement using multi-level logistic regression models. Of the 37,542 VJO veterans, treatment entry was associated with being homeless and having a mental health disorder or both a mental health and a substance use disorder versus a substance use disorder only. Being American Indian/Alaskan Native was associated with lower odds of treatment entry. Engagement was associated with female gender, older age, Asian race, urban residence, and homeless status. Increased utilization of substance use disorder treatment, especially pharmacotherapy, is an important quality improvement target.
Keywords
Introduction
Incarceration rates in the United States have been on the rise since the 1980s (Western & Pettit, 2010) and many incarcerated adults have a mental health and/or substance use disorder (Mumola & Karberg, 2006). In response to its costs, many states have introduced a number of alternatives to incarceration (Piquero, 2010). Alternatives to incarceration include jail diversion programs that divert individuals with mental health and substance use disorders to treatment upon contact with the criminal justice system (i.e., law enforcement, courts, and jails). These programs screen individuals involved in the legal system for an active mental health or substance use disorder, arrange for clinical staff to evaluate those who screen positive, negotiate with legal staff for a mental health disposition to reduce charges or in lieu of prosecution, and link them with community-based treatment (Steadman, Morris, & Dennis, 1995). Pre-booking diversion includes individuals who are arrested and directly transported to mental health treatment by law enforcement, whereas post-booking diversion includes individuals in jail or court who screen positive for mental illness and are ordered into treatment as an alternative to prosecution or jail (Sirotich, 2009). Specialty courts, such as mental health courts, drug courts, and veterans treatment courts, are post-booking diversion programs; that is, the court mandates participants to treatment and monitors for treatment adherence.
Evidence is mixed that jail diversion programs, including treatment courts and court-based diversion, successfully reduce criminal recidivism (Scott, McGilloway, Dempster, Browne, & Donnelly, 2013; Skeem, Manchak, & Peterson, 2011). A review of prebooking, jail-based, and court-based diversion programs found reductions in time spent in jail but no reductions in recidivism for individuals with mental health disorders (Sirotich, 2009). However, individuals with mental health disorders who participated in court-based jail diversion programs (programs that did not use a mental health or drug treatment court model) had fewer arrests and spent fewer days in jail in the following 12-month period compared with the 12 months prior to program enrollment (Case, Steadman, Dupuis, & Morris, 2009). A recent randomized trial of a case management jail diversion program in California found that program participants had more outpatient visits, but fewer days of psychiatric hospitalization, fewer jail bookings, and lower odds of being jailed again in the 12 months after program enrollment compared with participants in the treatment-as-usual group (Cusack, Morrissey, Cuddeback, Prins, & Williams, 2010).
Studies of specialty treatment courts find more positive evidence of their effectiveness. Meta-analyses and reviews indicate that mental health and drug courts are effective at reducing recidivism (Huddleston, Marlowe, & Casebolt, 2008; Marlowe, 2010; Sarteschi, Vaughn, & Kim, 2011). For example, individuals participating in mental health courts also have fewer arrests and fewer days of incarceration compared with a control group (Steadman, Redlich, Callahan, Robbins, & Vesselinov, 2011). However, studies of drug courts that used random assignment found no effects and programs shorter than 1 year were not effective (Latimer, Morton-Bourgon, & Chretien, 2006). In general, the methodologies of the reviewed studies are weak (Sarteschi et al., 2011; Wilson, Mitchell, & MacKenzie, 2006), suggesting that more rigorous work in this area should be done.
Roughly 10% of people incarcerated in the United States are military veterans (Noonan & Mumola, 2007). These numbers were significant enough to justify specialty courts that would improve access to Veterans Affairs (VA) benefits and services. Veterans treatment courts, modeled after mental health and drug treatment courts, are dedicated courts where veterans who have criminal charges are connected to needed mental health and/or substance use disorder treatment. Veterans are also supervised to adhere to treatment with sentences or charges potentially reduced, dismissed, or expunged upon program completion (Cavanaugh, 2010; Clark, McGuire, & Blue-Howells, 2010). Research on veterans treatment courts is in the early stages, but preliminary evidence suggests that recidivism in the 1-year period after program graduation is less than 10% (Holbrook & Anderson, 2011; Russell, 2009). The number of veterans treatment courts is increasing throughout the country and some courts are using electronic or telephone technology to expand access to veterans in rural areas (Smee et al., 2013).
In 2004, at least half of veterans incarcerated in jails or prisons self-reported mental health or substance use disorders. Furthermore, justice involvement and homelessness are strongly correlated with one another (Greenberg & Rosenheck, 2008; Tsai, Rosenheck, Kasprow, & McGuire, 2014). Services that link justice-involved individuals to mental and medical treatment and support their engagement in treatment, are critical for reducing homelessness and recidivism, and improving other outcomes (Mallik-Kane & Visher, 2008). To address their needs, the Veterans Health Administration (VHA) has developed two programs for veterans involved in the criminal justice system (Blue-Howells, Clark, van den Berk-Clark, & McGuire, 2013). The national Health Care for Reentry Veterans (HCRV) program was launched in 2007 and provides outreach to veterans in prison who are reentering the community and links them with appropriate VHA treatments. In 2009, the national Veterans Justice Outreach (VJO) program was created with the core mission of connecting veterans entering the criminal justice system with VHA treatment for mental health or substance use disorders as well as other needed medical services (Clark, Blue-Howells, Rosenthal, & McGuire, 2010). The VJO program is under the auspices of the VHA national homeless program office and shares the overarching goal of reducing and preventing homelessness and criminal justice recidivism among veterans. The VJO program is the focus of this article.
Although service delivery format and program settings vary, generally VJO Specialists are licensed social workers or psychologists who provide outreach to veterans in criminal justice settings, and includes active collaborations with law enforcement, defense counsel, prosecutors, jails, and courts (Blue-Howells et al., 2013). Veterans in legal settings who may be eligible for VHA programming are identified by these criminal justice partners in cooperation with VJO Specialists. Staff in VHA treatment settings and community organizations can also refer veterans to the VJO program, and veterans can also self-refer. While some veterans receive VHA care prior to contact with a VJO Specialist, the program is aimed at connecting veterans who have not yet received VHA treatment. After identification, a VJO Specialist conducts an assessment of the veteran to determine needed treatment services and links the veteran to care at the local VHA Medical Center and/or other appropriate programs in the local community. Veterans are served by more than 200 VJO Specialists nationally encompassing VHA medical centers in all 50 states and Puerto Rico.
VJO is a large and growing program within VHA, yet little is known about the population served and program outcomes. Therefore, to fill this void, the current article is the first to use national VJO data to examine the prevalence of mental health and substance use disorders among veterans enrolled in VJO, and to describe entry to and engagement in VHA mental health and substance use disorder treatment among those enrolled. This information will help to develop a better understanding of which veterans VJO currently serves and whether there are any subgroups of veterans in VJO who are underutilizing VHA services, warranting enhanced identification or linkage efforts.
Method
Participants
Using national VHA outpatient clinical/administrative records, we conducted a retrospective cohort study of veterans participating in the VJO program at any VHA medical center (N = 128 medical centers nationally). A veteran was included in the sample if she or he had contact with the VJO program anytime from fiscal year 2010 (beginning October 1, 2009) through fiscal year 2012 (ending September 30, 2012). We excluded veterans who had a prior outreach visit with a HCRV Specialist because this is a separate VHA program for veterans leaving prison.
Measures
Demographic characteristics
Demographic variables included gender, age, race, ethnicity, marital status, urban or rural residence, homeless status (drawn from a VA homeless indicator variable, VA services related to housing and homelessness clinic stops and residential codes, and International Classification of Diseases–9th Edition [ICD-9] codes for housing and homelessness), and service-connected disability rating, which reflects a disability caused by illness or injury that occurred during or was aggravated by military service.
Mental health and substance use disorder diagnoses
A veteran was considered to have a mental health or substance use disorder if she or he had at least one instance of the diagnosis associated with her or his health record in the 1-year period after her or his VJO Specialist encounter—each veteran was on a 1-year person-specific timeline trajectory. Some veterans had contact with a VJO Specialist more than once (e.g., if they were under supervision of a veterans treatment court), but only the first visit was used to calculate the 1-year period. During an outreach visit, a VJO Specialist conducted an assessment to match a veteran with treatment, but did not enter a mental health or substance use disorder diagnosis into a veteran’s health record. Diagnoses, if any, were determined as part of a more detailed clinical assessment by other VHA clinicians (typically a physician or psychologist) who had contact with the veteran after the VJO encounter. These diagnoses can be documented in a variety of clinical settings including primary care and mental health settings. Mental health and substance use disorders were defined based on ICD-9 diagnosis codes. Mental health disorders included the following: depressive disorders, posttraumatic stress disorder (PTSD), anxiety disorders, bipolar disorder, schizophrenia, other psychosis, and personality disorders. Substance use disorders included the following: alcohol use disorder, opioid use disorder, cocaine use disorder, amphetamine use disorder, cannabis use disorder, sedative use disorder, and other drug use disorders.
Engagement in mental health and substance use disorder treatment services
We counted the number of visits to mental health and substance use disorder treatment clinics for each veteran in the 1-year period after her or his VJO encounter. Clinic visits were grouped into the following: (a) mental health disorder outpatient; (b) mental health disorder inpatient; (c) mental health disorder residential; (d) substance use disorder outpatient; (e) substance use disorder residential; (f) pharmacotherapy for alcohol use disorder, including naltrexone, acamprosate, and disufiram; and (g) pharmacotherapy for opioid use disorder, including methadone, buprenorphine, and naltrexone. Entry into VHA mental health or substance use disorder treatment was defined by use of any mental health or substance use disorder outpatient or residential care or any pharmacotherapy for alcohol or opioid use disorders within 1 year of contact with a VJO Specialist. Engagement in VHA mental health or substance use disorder treatment was defined as six or more mental health disorder outpatient visits, six or more substance use disorder outpatient visits, or any mental health or substance use disorder residential treatment in the 1-year period after contact with a VJO Specialist.
Analysis
First, we examined descriptive statistics of demographic characteristics of all veterans in our sample. Second, we excluded veterans who did not have a face-to-face visit at a VHA facility in the 1-year period after her or his VJO visit because these veterans would not have had the opportunity to receive a diagnosis. For the remaining veterans, we examined their prevalence of mental health and substance use disorder diagnoses. Third, we further limited the sample to veterans who were diagnosed with a mental health disorder to examine the descriptive statistics of mental health treatment use. Fourth, we limited the sample to veterans with a substance use disorder and reported descriptive statistics of their substance use disorder treatment use. Finally, we limited the sample to veterans with mental health or substance use disorder diagnoses. We conducted two logistic regression tests with a random effect for facility (n = 128 medical centers) to model the odds of entry (Model 1) or engagement (Model 2) in VHA mental health or substance use disorder treatment, adjusting for demographic characteristics and type of diagnosis. Cases with missing data (n = 180; <1%) were excluded from the logistic regression models.
Results
Demographic Characteristics
There were 36,358 veterans who received an outreach visit from a VJO Specialist in fiscal years 2010 to 2012. Table 1 displays the demographic characteristics of the sample. The majority of veterans were men age 45 or above, though 23% were less than 35 years old and 4% were women. Most justice-involved veterans were White (59%) or Black/African American (32%), and single (40%) or divorced/separated (37%). Nearly a quarter of veterans in contact with the VJO program resided in rural areas (21%) or were homeless (23%), and 45% had a service-connected disability rating.
Demographic Characteristics of Justice-Involved Veterans Seen by Veteran Justice Outreach Specialists in Fiscal Year 2010 to Fiscal Year 2012.
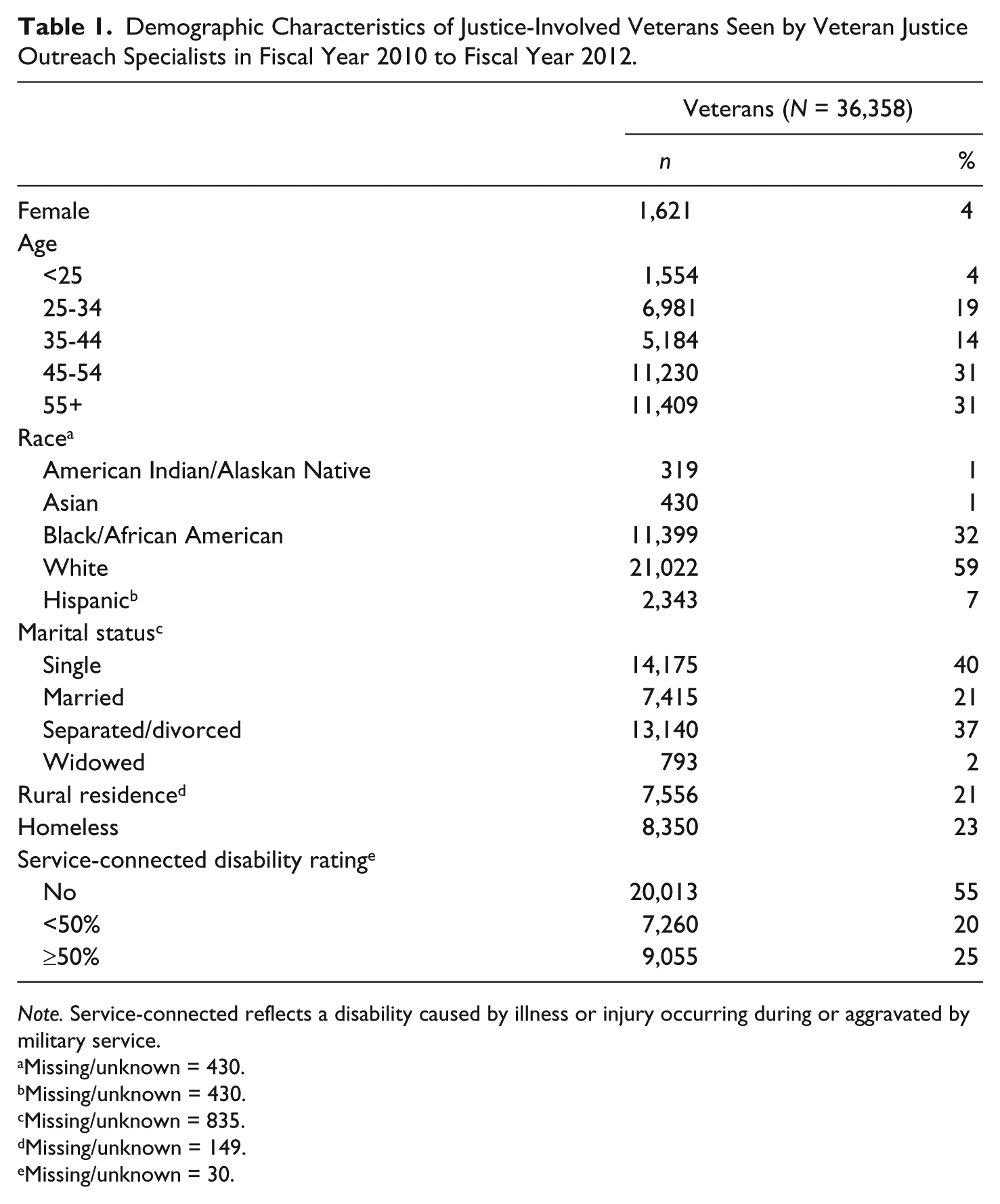
Note. Service-connected reflects a disability caused by illness or injury occurring during or aggravated by military service.
Missing/unknown = 430.
Missing/unknown = 430.
Missing/unknown = 835.
Missing/unknown = 149.
Missing/unknown = 30.
Diagnoses
Of the veterans who had a VJO outreach visit, 32,013 (88%) had a face-to-face VHA visit later. Table 2 shows the prevalence of each mental health and substance use disorder diagnosis among VJO veterans who had a face-to-face VHA visit. Most veterans (90%) were diagnosed with a disorder: 77% were diagnosed with at least one mental health disorder and 71% were diagnosed with at least one substance use disorder. Multiple diagnoses were also common; 47% were diagnosed with more than one mental health disorder, 46% with more than one substance use disorder, and 58% with at least one mental health disorder and at least one substance use disorder. The three most common mental health disorders were depressive disorders (55%), PTSD (37%), and anxiety disorders (22%). More than half (57%) of veterans were diagnosed with an alcohol use disorder, 13% with opioid use disorder, and 36% with other drug use disorders.
Mental Health and Substance Use Disorder Diagnoses Among Justice-Involved Veterans Seen by VJO Specialists in Fiscal Year 2010 to Fiscal Year 2012 Who Had a Face-to-Face VHA Visit After Their VJO Visit.

Note. The sum of percentages exceeds 100% because 15,069 (47%) patients were diagnosed with more than one mental health disorder, 14,581 (46%) patients were diagnosed with more than one substance use disorder, and 18,537 (58%) patients were dually diagnosed with at least one mental health and one substance use disorder. VJO = Veterans Justice Outreach; VHA = Veterans Health Administration; PTSD = posttraumatic stress disorder.
Use of Mental Health or Substance Use Disorder Treatment Services
The majority of veterans who were diagnosed with mental health or substance use disorders subsequently utilized mental health or substance use disorder care. Utilization of mental health treatment was nearly universal; 97% of veterans diagnosed with a mental health disorder entered mental health treatment in the 1-year period after their VJO outreach visit. Table 3 displays the mental health disorder treatment utilization rates. Veterans who used mental health outpatient care had a mean of 31 mental health outpatient visits (SD = 37) in a year. Patients in mental health residential treatment had a mean of 85 days (SD = 69) of care in a year.
VHA Mental Health and Substance Use Disorder Treatment Use by Justice-Involved Veterans Seen by VJO Specialists in Fiscal Year 2010 to Fiscal Year 2012 Who Had a Mental Health or Substance Use Disorder Diagnosis.

Note. The number of people with a mental health or substance use disorder who had at least one instance of that type of care is reported. The descriptive statistics reflect only patients who received that type of care. VHA = Veterans Health Administration; VJO = Veterans Justice Outreach.
Among veterans diagnosed with a substance use disorder, 72% entered substance use disorder treatment (Table 3). Veterans who used substance use disorder outpatient care had a mean of 31 visits (SD = 35) in a year. Veterans in substance use disorder residential care had a mean of 37 days (SD = 33) of treatment in a year. Limiting the sample to veterans diagnosed with alcohol use disorder, 11% received pharmacotherapy for alcohol use disorder in a year. Among veterans diagnosed with opioid use disorder, 20% received pharmacotherapy for opioid use disorder in a year.
Entry to and Engagement in Mental Health or Substance Use Disorder Treatment
Among veterans who had a mental health or substance use disorder, 97% entered mental health or substance use disorder outpatient or residential treatment or received pharmacotherapy for alcohol or opioid use disorders. We tested the demographic characteristics and diagnosis types associated with entry to mental health or substance use disorder treatment (Table 4). Being 55 years or older (compared with younger than 25) was associated with lower odds of entry into treatment (odds ratio [OR] = 0.55, 95% confidence interval [CI] = [0.38, 0.83]). Being American Indian/Alaskan Native compared with White was also associated with lower odds of entry into treatment (OR = 0.52, 95% CI = [0.28, 0.96]). Factors associated with higher odds of entry into mental health or substance use disorder treatment were being homeless (OR = 1.67, 95% CI = [1.39, 2.01]), and having only a mental health disorder (OR = 1.53, 95% CI = [1.30, 1.81]) compared with more mental health disorders, or both a mental health and a substance use disorder (OR = 10.54, 95% CI = [8.75, 12.71]) compared with a substance use disorder only.
Demographic Characteristics and Mental Health/Substance Use Disorders Associated With Mental Health or Substance Use Disorder Treatment Entry and Engagement Among Justice-Involved Veterans Seen by VJO Specialists in Fiscal Year 2010 to Fiscal Year 2012 Who Had a Mental Health or Substance Use Disorder Diagnosis (n = 28,629).

Note. Cases with missing data (n = 180; <1%) were excluded from the logistic regression models. Entry to treatment is defined as any use of mental health or substance use disorder outpatient or residential services or pharmacotherapy within 1 year of initial contact with a VJO Specialist. Engagement in treatment is defined as 6+ mental health disorder outpatient visits, 6+ substance use disorder outpatient visits, or any mental health or substance use disorder residential stays within 1 year of initial contact with a VJO Specialist. ORs in bold indicate a significant value. VJO = Veterans Justice Outreach; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
The rate of treatment engagement, defined as six or more mental health outpatient visits, or six or more substance use disorder outpatient visits, or any mental health or substance use disorder residential treatment, was 79%. Among patients with a mental health or substance use disorder diagnosis, demographic characteristics associated with higher odds of engagement in mental health and substance use disorder treatment included being female, between ages 25 and 54 years (compared with less than 25), and being Asian (compared with White). Veterans who lived in urban areas (compared with rural areas) or who were homeless (compared with housed) also had higher odds of engaging in treatment. Having a service-connected disability rating or having both a mental health and a substance use disorder compared with only a substance use disorder were also associated with higher odds of engagement in treatment.
Discussion
This study is the first to document the prevalence of mental health and substance use disorders among veterans in the VJO program and their subsequent use of VHA treatment. The findings are consistent with literature on the prevalence of self-reported mental health and substance use disorders in the general and veteran criminal justice populations (Binswanger et al., 2010; James & Glaze, 2006; Mumola & Karberg, 2006). Nonetheless, the prevalence of mental health and substance use disorders among veterans in contact with VJO is remarkable with 76% diagnosed with at least one mental health disorder, 71% diagnosed with at least one substance use disorder, and 58% diagnosed with both a mental health and a substance use disorder. By comparison, the prevalence of these disorders in the overall VHA veteran population is 28% for mental health disorders, 9% for substance use disorders, and 6% for both a mental health and a substance use disorder (Frayne et al., 2014). The prevalence of substance use disorders among veterans in the VJO program is especially remarkable.
Treatment usage was also high overall and higher than other VHA patients with mental health or substance use disorders. For example, among VHA veterans the rate of mental health visits for patients with a mental health disorder diagnosis was 71% (Frayne et al., 2014). One reason for the high rate of engagement in the current sample may be that a portion of the sample attends treatment that is mandated by the court. However, less than half of the veterans in the VJO program are under court supervision suggesting that the high rate of treatment engagement can be explained by other factors.
Mental Health Disorder Treatment
Although not a jail diversion program, the VJO program coordinates with legal system staff around diversion activities to connect eligible veterans with health care and benefits. Almost all veterans (97%) who entered VHA care after contact with a VJO Specialist and were subsequently diagnosed with a mental health disorder received some mental health treatment. These results suggest that these veterans who see a VJO Specialist are doing far better than the general VHA patient population at connecting to care. Among veteran patients at VHA in fiscal year 2012, 71% of patients with a current mental health diagnosis had at least one mental health treatment visit that same year (Frayne et al., 2014). VJO veterans with a mental health disorder, with or without a co-occurring substance use disorder, had higher odds of entering treatment than those with only a substance use disorder, which is consistent with prior literature (Golub, Vazan, Bennett, & Liberty, 2013). Perhaps the availability of mental health treatment, such as mental health clinics embedded in primary care clinics, lessens the stigma associated with mental health treatment. Receipt of care for substance use disorders in mental health treatment settings may also explain why veterans with co-occurring mental health substance use disorders received more substance use disorder treatment. Further work examining individual clinic codes, chart reviews, and interviews with patients and providers may highlight particular patterns of treatment entry.
Substance Use Disorder Treatment
Among VJO veterans with a substance use disorder, 72% received some substance use disorder care. In contrast, among the general VHA veteran population with a current substance use disorder diagnosis in fiscal year 2010, only 34% received any substance use disorder specialty care (Oliva, Dalton, Harris, & Trafton, 2013). Although we could not assess how many veterans in our sample were in contact with the VJO program through court settings, court mandated treatment likely explains a substantial proportion of the high entry rate among VJO veterans. Ex-inmates with co-occurring mental health disorders have been found to use more substance use disorder treatment when under correctional supervision compared with ex-inmates not under supervision (Hartwell et al., 2013). For all VJO veterans, whether or not they were mandated to treatment, the VJO Specialists’ assistance in navigating the VHA health care system may also be a key factor in the program’s success. Despite high treatment utilization, our regression analyses indicated that veterans with only a substance use disorder had lower odds of receiving and engaging in VHA treatment compared with veterans with only a mental health or both mental health and substance use disorders. These findings are consistent with prior studies that found that unmet substance use disorder treatment needs are higher than unmet mental health disorder treatment needs (Golub et al., 2013).
In addition, an examination of treatment type suggests that pharmacotherapy is being underutilized in this population even more than it is generally recognized. Among VJO program participants diagnosed with opioid use disorder, only 20% received pharmacotherapy for their disorder, which is lower than the roughly 25% to 27% of general VHA veteran patients with opioid use disorder who received this treatment (Oliva, Trafton, Harris, & Gordon, 2013). This is unfortunate as evidence suggests that among criminal justice populations use of pharmacotherapy to address opioid use disorder can reduce drug use and help minimize clients’ return to criminal behaviors (Gryczynski et al., 2012; Kinlock et al., 2007). Pharmacotherapy for alcohol use disorder reduces alcohol and drug use and criminal justice recidivism (Finigan, Perkins, Zold-Kilbourn, Parks, & Stringer, 2011). However, only 10% of VJO veterans with alcohol use disorder received this evidence-based treatment. Although this rate is roughly twice as high compared with other VHA patients with alcohol use disorder (Harris et al., 2012), it highlights an important quality improvement target for all VHA patients.
Many veterans served by VJO are under the supervision of specialty courts and probation officers where barriers to pharmacotherapy may exist depending on the rules of that jurisdiction. In a study of U.S. drug court staff, court policy against pharmacotherapy, cost of treatment, and negative attitudes or lack of knowledge about pharmacotherapy have been cited as barriers to pharmacotherapy (Matusow et al., 2013). Targeted educational outreach in justice settings is being tested as one strategy to increase use of pharmacotherapy (Friedmann et al., 2013). It is unknown whether these barriers also exist in veterans treatment courts, but future studies focused on increasing implementation of these evidence-based treatments would be beneficial.
Vulnerable Groups of Veterans
Overall, veterans who received services from VJO are accessing VHA mental health and substance use disorder care at relatively high rates, but our results indicate that there are vulnerable subgroups who may benefit from targeted outreach and linkage efforts. American Indian/Alaskan Native veterans were less likely to enter care after VJO contact. Other studies have also found similar disparities in use of VHA care or receipt of antidepressant therapy and guideline-concordant depression treatment among American Indians/Alaskan Natives compared with White veterans (Harris et al., 2014; Quinones et al., 2014). One issue may be that veterans living on reservations may have difficulty accessing treatment due to lack of VHA facilities near their residences. To address this issue, VHA has a Memorandum of Understanding with Indian Health Services to deliver health care services. Thus, some American Indian/Alaskan Native veterans may be receiving care through Indian Health Services, either paid for by VA or not, but we were unable to assess these data for examination. Future work with VA fee basis records or Indian Health Service data may better determine if American Indian/Alaskan Native veterans are being served through a different mechanism or if disparities in treatment entry exist among VJO veterans.
Consistent with prior studies (Harpaz-Rotem & Rosenheck, 2011; Seal et al., 2010), veterans under the age of 25 and those with rural residences were less likely to engage in care than older or urban veterans. Younger veterans may be less likely to engage in care for various reasons including stigma (Hoge et al., 2004), but techniques such as telephone-based motivational interviewing show promise for increasing engagement in mental health and substance use disorder treatment (McKay et al., 2010; Seal et al., 2012). Telephone and computer technologies have also been utilized in rural areas among justice-involved veterans to allow them to comply with their court mandates without missing treatment (Smee et al., 2013).
Treatment Entry and Engagement Among Homeless Veterans
In the current study, veterans who were homeless had higher odds of entry and engagement in mental health or substance use disorder care compared with housed veterans. VHA is committed to ending veteran homelessness and has made progress toward that goal (O’Toole, Pape, & Kane, 2013). A recent study showed that outpatient, inpatient, and emergency department use was greater among formerly homeless veterans housed through the U.S. Department of Housing and Urban Development–VA Supportive Housing program compared with currently homeless veterans (Gabrielian, Yuan, Andersen, Rubenstein, & Gelberg, 2014). This study suggests that housing along with primary care referrals is one effective mechanism for addressing health care disparities frequently observed among homeless populations. Availability of dedicated programs for homeless populations accessible through VJO Specialists may partially explain why homeless veterans who have contact with the VJO program have higher odds of entry and engagement in care.
Strengths and Limitations
To our knowledge, this is the first study to document demographic characteristics, prevalence of mental health and substance use disorders, and VHA mental health and substance use disorder treatment entry and engagement patterns among veterans who were in contact with VJO Specialists. However, there are notable limitations to our findings. First, our sample was limited to veterans in the VJO program, which primarily focuses on veterans with treatment needs. This enhanced case-finding may partially explain the high prevalence of mental health and substance use disorders in our results. A more comprehensive study is needed of all veterans involved in the criminal justice system, including those not connected to VJO, veterans who are incarcerated and unable to see VA clinicians, and/or veterans ineligible for VA benefits. Veterans not eligible for benefits may be a particularly vulnerable group as some of these veterans were discharged from the military with less than honorable status after criminal behavior related to combat stress and post-deployment adjustment issues (Seamone et al., 2014). These veterans would likely have mental health or substance use disorder issues, but would have fewer options for treatment as they would not qualify for VA services. Second, our measures were limited to existing diagnoses from VHA administrative records rather than prospective structured diagnostic interviews; thus, some mental health or substance use disorders may not have been captured, particularly in patients with infrequent use of VHA. Third, we aggregated diagnoses and treatment use into broad categories. Given the number of VJO veterans with multiple mental health or substance use disorders, determining whether they are being treated for the specific diagnoses they received would be an important next step for future work. Finally, we were unable to assess reductions in mental health or substance use disorder symptoms or subsequent risk for homelessness or recidivism in this VHA administrative data set. Long-term follow-up of this justice-involved veteran population would provide evidence of the effectiveness of the VJO program in achieving its goals.
Conclusion
The VJO program appears to be an important national initiative fostering the engagement of vulnerable and often underserved veterans involved in the criminal justice system with needed treatment services. The majority of veterans in contact with this program subsequently enter face-to-face VHA treatment. Furthermore, among veterans diagnosed with a mental health disorder, almost all received at least one mental health treatment service, and the majority who had a substance use disorder received at least one substance use disorder treatment service. Thus, the VJO program appears to be linking justice-involved veterans to VHA services where their substantial mental health and substance use disorders are diagnosed and treated at high rates. Even so, more work needs to be done to increase use of evidence-based treatments, such as pharmacotherapy for opioid or alcohol use disorders, and to meet the needs of vulnerable groups that may be currently underusing the VJO program. Although there is still much to be learned about VJO’s effectiveness, these results suggest that developers of other health care linkage programs for non-veterans might learn and benefit from the VJO program and its learned experiences.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily reflect the position nor policy of the Department of Veterans Affairs (VA) or the U.S. government. The VA had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Veterans Affairs (VA) Substance Use Disorder Quality Enhancement Research Initiative (SUDQ-LIP1404). Dr. Finlay was supported by the VA Office of Academic Affiliations Advanced Fellowship in Health Services Research and Development (HSR&D) and a Career Development Award (CDA 13-279). Dr. Timko was funded as a Senior Research Career Scientist (RCS 00-001) in VA HSR&D. Dr. Harris was funded as a Research Career Scientist (RCS 14-132) in VA HSR&D. A portion of this work was also supported by the VA National Center on Homelessness Among Veterans.