
Abstract
This study examined whether, among Veterans Health Administration (VHA) patients, veterans with recent or current justice involvement have equal receipt of pharmacotherapy for alcohol use disorder compared with veterans with no justice involvement. Using national VHA records, we calculated the overall and facility rates of receipt as the number of patients who received pharmacotherapy for alcohol use disorder divided by the number of patients diagnosed with an alcohol use disorder. Using a mixed-effects logistic regression model, we tested whether justice involvement was associated with pharmacotherapy receipt. Male veterans with jail/court involvement had significantly higher odds of receiving pharmacotherapy for alcohol use disorder compared with other male veterans. Justice-involved veterans had equal or better receipt of pharmacotherapy for alcohol use disorder compared with veterans with no justice involvement. Pharmacotherapy rates are low overall, suggesting that more work can be done to connect veterans to these medications.
Keywords
Introduction
Alcohol use disorders (AUDs) are common among veterans involved in the criminal justice system. Among incarcerated veterans, 43% of state prisoners and 36% of federal prisoners self-report alcohol abuse or dependence in the 12 months prior to entering prison (Noonan & Mumola, 2007). Compared with veterans with no incarceration history, veterans with an incarceration history have 2.5 times higher odds of having an AUD (Black et al., 2005). Among veterans who have contact with Veterans Health Administration (VHA) outreach services and subsequently use VHA treatment (after release from incarceration for veterans in jail or prison), 57% of veterans seen during jail/court outreach and 34% of veterans seen during prison outreach are diagnosed with AUD (Finlay et al., 2016; Finlay et al., 2015). These prevalence rates are several times higher than the general VHA patient population in 2011 (7%; Oliva, Dalton, Harris, & Trafton, 2013), and veterans who served in Iraq or Afghanistan and used VHA treatment from 2001 to 2010 (10%; Seal et al., 2011). Having an AUD can also increase a veteran’s risk of incarceration (Erickson, Rosenheck, Trestman, Ford, & Desai, 2008).
There is strong evidence supporting the treatment of AUDs with pharmacotherapy. Meta-analyses of the efficacy and safety of naltrexone, acamprosate, and topiramate indicate that these medications are effective at increasing the number of days of abstinence and reducing heavy drinking days (Arbaizar, Diersen-Sotos, Gomez-Acebo, & Llorca, 2010; Bouza, Angeles, Munoz, & Amate, 2004; Jonas et al., 2014; Kranzler & Van Kirk, 2001; Maisel, Blodgett, Wilbourne, Humphreys, & Finney, 2013). A recent meta-analysis of disulfiram found support for its efficacy in open-label trials, with efficacy tied to monitoring and compliance (Skinner, Lahmek, Pham, & Aubin, 2014). For adults involved in the criminal justice system, pharmacotherapy for AUD is associated with reduced recidivism. Among adults in a drug court who received extended-release naltrexone, 8% were rearrested within a year compared with 26% of a matched control group of drug court participants (Finigan, Perkins, Zold-Kilbourn, Parks, & Stringer, 2011).
Despite the high need for treatment for AUDs among justice-involved veterans and the strong evidence for the benefits of pharmacotherapy, access to and use of pharmacotherapy for justice-involved populations are limited (Chandler, Fletcher, & Volkow, 2009). Patients with a criminal justice history may also experience stigma in seeking substance use disorder (SUD) treatment (van Olphen, Eliason, Freudenberg, & Barnes, 2009). Treatment programs that serve a higher proportion of patients with criminal justice involvement are less likely to use pharmacotherapy for AUD compared with other treatment programs (Ducharme, Knudsen, & Roman, 2006). Criminal justice agencies, such as jails or prisons, provide pharmacotherapy but usually only in limited circumstances such as detoxification or for pregnant women (Friedmann et al., 2012). Reasons for not prescribing these medications include concerns about diversion, a lack of knowledge about pharmacotherapy as an evidence-based practice, and a belief that prisoners did not need the medications because they are “clean” when they arrive at prison. Access to pharmacotherapy may improve by directly addressing criminal justice staff’s negative attitudes toward these medications. For example, an intervention among community correctional staff and treatment providers found improved attitudes about pharmacotherapy and increased intentions to refer clients with AUD to these medications (Friedmann et al., 2015).
The VHA is an important national health care system that mandates that pharmacotherapy for AUD is made available to all veteran patients when clinically indicated (Department of Veterans Affairs, 2008). However, unknown is whether veterans with current or recent criminal justice involvement have equal use of these medications compared with other patients. Some justice-involved veterans may have court mandates to use pharmacotherapy, whereas other justice-involved veterans may have court restrictions or probation/parole requirements that act as barriers to seeking treatment (Martin, Clapp, Alfers, & Beresford, 2004; Matusow et al., 2013). Stigma may also be a barrier to seeking addiction treatment (Hartwell, 2004).
The current study examined whether recently or currently justice-involved veterans who received health care at VHA experienced equal receipt of pharmacotherapy for AUD compared with veterans without recent or current justice involvement. The goal is to determine whether targeted efforts are needed to increase receipt of pharmacotherapy for AUD among this special population. Our two aims are to (a) describe rates of receipt of pharmacotherapy for AUD among VHA patients who are and are not justice-involved and (b) examine whether justice involvement is associated with receipt of pharmacotherapy for AUD, controlling for patient- and facility-level characteristics identified in prior research (Harris et al., 2013; Harris et al., 2012).
Material and Method
Using national VHA clinical/administrative records, we conducted a study of all veteran VHA users who received an AUD diagnosis (abuse or dependence, excluding in remission; International Classifications of Diseases [ICD]–Ninth Edition-Clinical Modification [CM] codes 291.x, 303.0, 303.9, 303.91, 303.92, 305.0, 305.01, 305.02) during an outpatient or inpatient visit at a VHA facility in Fiscal Year (FY) 2012 (October 1, 2011 through September 30, 2012).
Measures
Outcome
Receipt of pharmacotherapy for AUD was defined as filling at least one prescription for naltrexone, acamprosate, topiramate, or disufiram as indicated in VHA pharmacy records during the person-specific 1-year period after receiving an AUD diagnosis during FY 2012. All four medications are on the national VHA formulary.
Justice-involved
A veteran was considered recently or currently justice-involved (referred to as “justice-involved” hereafter) if he had a clinic code indicating contact with the Health Care for Reentry Veterans program, which provides outreach to veterans in prison, or the Veterans Justice Outreach program, which provides outreach in other justice system settings, primarily jails and courts, prior to or during FY 2012 (Blue-Howells, Clark, van den Berk-Clark, & McGuire, 2013; Clark, Blue-Howells, Rosenthal, & McGuire, 2010). Specialists from each program conduct outreach activities including assessing the treatment needs of veterans and connecting them with VHA and community services. For the purposes of this study, we distinguished between veterans with prison involvement and veterans with jail/court involvement (both groups included veterans on probation/parole) because of sociodemographic and treatment use differences between these groups, which may affect pharmacotherapy receipt (Finlay & Rosenthal, 2015). Veterans exiting prison are older, more live in rural areas, fewer have a service-connected disability rating, and fewer are diagnosed with mental health or SUDs compared with veterans who are jail/court-involved. Veterans with prison involvement are less likely to have contact with VHA services after receiving an outreach visit and are less likely to enter and engage in mental health or SUD treatment compared with veterans with jail/court involvement. Patients who did not have contact with either outreach program were coded as not justice-involved.
Patient characteristics
Demographic variables included gender, age, ethnicity/race (Hispanic, non-Hispanic American Indian/Alaskan Native, non-Hispanic Asian, non-Hispanic Black, non-Hispanic White; based on the Bureau of Census categories), marital status (single, married, separated/divorced, widowed), urban or rural residence (living in an urban city or rural area), and homeless status (drawn from a homeless indicator variable, receipt of housing services, and ICD–Ninth Edition codes for unstable housing and homelessness). Military characteristics included service in Iraq or Afghanistan (yes/no) and service-connected disability rating (None, < 50%, ≥ 50%), which reflects a VHA-determined disability occurring during or aggravated by military service. Demographic and military characteristics were coded from records collected the same day the veteran received his first AUD diagnosis during FY 2012, or from the next available record, except for service in Iraq or Afghanistan, which was drawn from the Iraq/Afghanistan Roster. Patient health characteristics included co-occurring psychiatric disorder (depressive disorders, post-traumatic stress disorder [PTSD], anxiety disorders, bipolar disorder, schizophrenia, other psychosis, or personality disorders), co-occurring SUD (opioid use disorder, cocaine use disorder, amphetamine use disorder, cannabis use disorder, sedative use disorder, or other drug use disorders), and the Deyo comorbidity index, a sum of up to 17 comorbid medical diagnoses, such as HIV, liver disease, diabetes, and congestive heart failure (Deyo, Cherkin, & Ciol, 1992). These health characteristics were coded from records from the 1-year period after first AUD diagnosis.
Facility characteristics
Facility characteristics were drawn from the 2012 Drug and Alcohol Program Survey (DAPS), a biennial survey of key personnel at specialty substance use programs. In 2012, the DAPS was administered to 220 programs with a 100% response rate. Programs were then mapped to the 129 major VHA facilities. Facility characteristics included availability of the following SUD-related services (yes/no): weekend services, weeknight services, women veteran services, Iraq/Afghanistan veteran services, medications for psychiatric problems, dual diagnosis services, pharmacotherapy for smoking, pharmacotherapy for opioid use disorder, and pharmacotherapy for alcohol use disorder. Housing support was indicated by the percentage of veterans treated at the facility who were living in VHA-related housing (VHA housing, contracted or subsidized VHA housing) compared with the percentage who were living in private residences. Other facility characteristics included abstinence required prior to program admittance (yes/no), whether the program provided services to patients who used substances after admittance (yes/no), number of veterans on a waiting list for program admission, average number of months to program admittance, average number of months to residential bed admittance, unique number of SUD patients at the facility, mean number of evidence-based practices available (motivational enhancement therapy, manualized 12-step facilitation, cognitive behavioral therapy, contingency management/motivational incentives, behavioral couples therapy, family therapy, community reinforcement approach, seeking safety), ratio of SUD clinic staff to 100 patients diagnosed with SUD at each facility, and the ratio of clinic staff who can prescribe SUD medications to 1,000 patients diagnosed with SUD at each facility. These facility characteristics have been used in previous studies examining receipt of pharmacotherapy for AUD (Harris, Kivlahan, Bowe, & Humphreys, 2010; Harris et al., 2012).
Analyses
We limited our analyses to male veterans because of the small number of women who were seen by VHA justice programs. We examined descriptive statistics of patient characteristics, stratified by justice-involved status, and tested group differences using chi-squared analyses. The rate of receipt of pharmacotherapy for AUD was calculated as the number of patients who received pharmacotherapy for AUD divided by number of patients diagnosed with an AUD. A mixed-effects logistic regression model was used to test whether justice-involved status was associated with odds of receiving pharmacotherapy for AUD, controlling for patient- and facility-level correlates. A random effect for facility (N = 129) was included to account for patient clustering by facility. Our initial model included all patient- and facility-level covariates. We then trimmed all non-significant (p ≥ .05) covariates, resulting in the final model. This study was approved by the Institutional Review Boards at Stanford University and VA Palo Alto Health Care System.
Results
Characteristics of Veterans Diagnosed With Alcohol Use Disorder
Of VHA male patients in FY 2012, 24% (n = 4,347) of veterans with a history of prison involvement, 46% (n = 17,492) of veterans with a history of jail/court involvement, and 6% (n = 305,809) of veterans without a history of justice involvement were diagnosed with AUD. Characteristics of male veterans with AUD in FY 2012 are displayed by justice-involved status in Table 1. Fewer justice-involved veterans were married than veterans who were not justice-involved (p < .001). Among veterans with a prison or jail/court history, 24% and 18%, respectively, were homeless compared with 5% of veterans not justice-involved (p < .001). Forty percent of veterans with a prison history had a service-connected disability rating compared with 52% of veterans with a jail/court history and 49% not justice-involved (p < .001). In addition to their AUD diagnosis, most veterans who had been prison- or jail/court-involved had a co-occurring mental health disorder diagnosis and a co-occurring SUD diagnosis. About two thirds of veterans not justice-involved had a co-occurring SUD, but less than one third had a co-occurring SUD.
Socio-Demographic Characteristics and Comorbid Diagnoses of Male Veterans With Alcohol Use Disorder in Veterans Health Administration Health Care by Justice-Involved Status in Fiscal Year 2012.

Receipt of Pharmacotherapy for Alcohol Use Disorder
The rate of receipt of pharmacotherapy for AUD is reported in Table 2. In FY 2012, of the 4,347 male veterans with a prison history, 357 (8.2%) received pharmacotherapy for AUD within 1 year of their diagnosis. Of the 17,515 veterans with a jail/court history, 1,959 (11.2%) received pharmacotherapy within 1 year of their diagnosis. Among 305,809 veterans not justice-involved, 15,333 (5.0%) received pharmacotherapy.
Rate of Receipt of Alcohol Use Disorder Pharmacotherapy in Fiscal Year 2012.
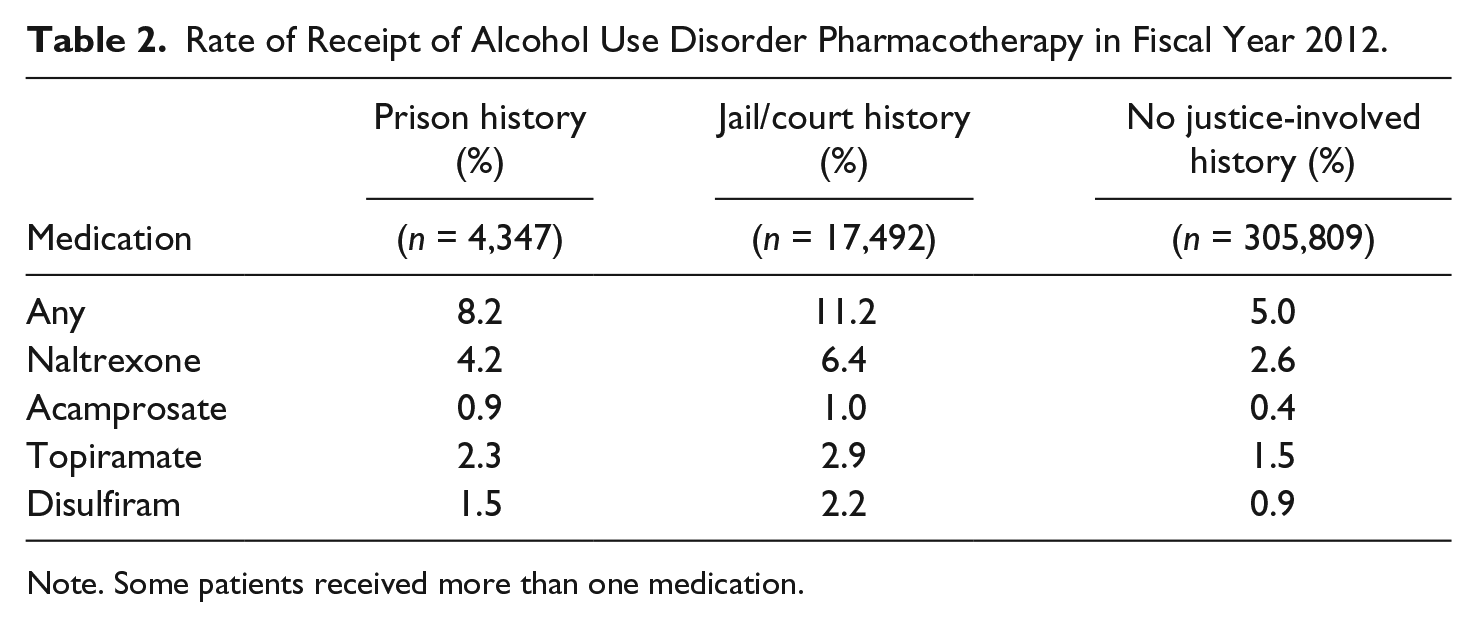
Note. Some patients received more than one medication.
Variation in Rate of Receiving Pharmacotherapy for Alcohol Use Disorder
There was wide variation across VHA facilities in the rate of receipt of pharmacotherapy for AUD (Figure 1). Variation in the rate of receipt ranged from 0% to 36% for veterans exiting prison, 0% to 41% for veterans jail/court-involved, and 1% to 16% for veterans not justice-involved. The within-facility gaps between veterans with prison involvement and with no justice involvement was also notable ranging from −10% to +31%, with 38% of facilities having a +5% or greater difference. For jail/court-involved veterans compared with veterans with no justice involvement, the rate of receipt differed from −7% to +32%, with 60% of facilities having a +5% or greater difference.

Rate of receipt of pharmacotherapy for alcohol use disorder by facility for male veterans with prison involvement, jail/court involvement, or without justice involvement.
Odds of Receiving Pharmacotherapy for Alcohol Use Disorder
The results from the mixed-effects logistic regression model indicated that male jail/court-involved veterans had 1.42 higher odds of receiving pharmacotherapy for AUD compared with those without recent justice involvement (95% confidence interval [CI] = [1.34, 1.50]; Table 3) and 1.29 higher odds than veterans exiting prison (95% CI = [1.14, 1.46]). Veterans exiting prison did not have significantly different odds of receiving pharmacotherapy compared with veterans who were not justice-involved. The adjusted rates of receipt were 8.3% for prison-involved veterans, 11.2% for jail/court-involved veterans, and 5.1% for veterans not justice-involved. Other factors associated with higher odds of receiving pharmacotherapy included being ages 35 to 44 or 45 to 54, being homeless, having a service-connected disability of 50% or greater, having a co-occurring SUD diagnosis, and having a co-occurring mental health diagnosis. Factors associated with lower odds of receiving pharmacotherapy were being 55 years old or older, being Hispanic, being non-Hispanic Asian, being non-Hispanic Black/African American, being unmarried, and living in a rural area.
Multivariable Model of Receipt of Alcohol Use Disorder Pharmacotherapy Among Veterans in Fiscal Year 2012.
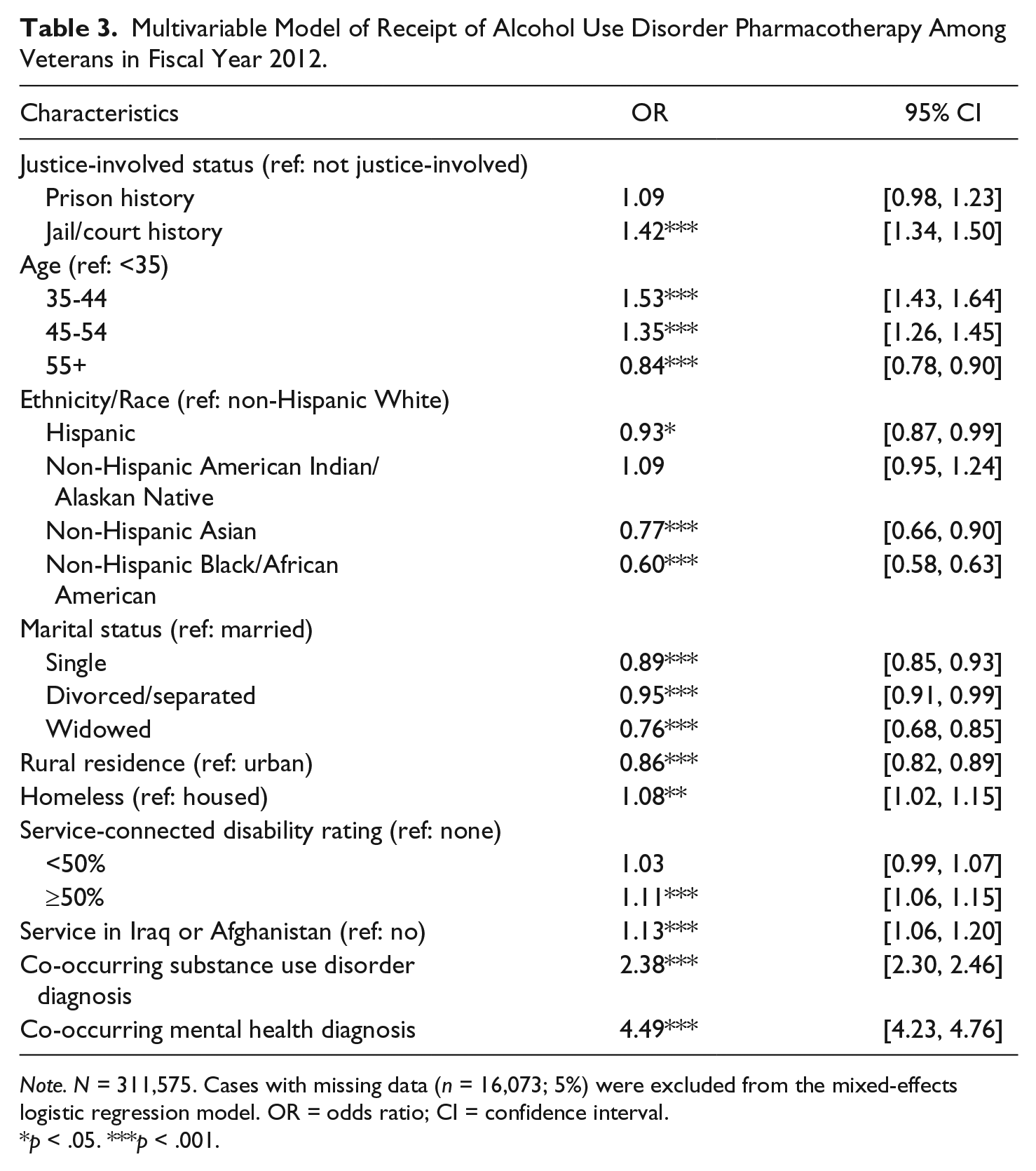
Note. N = 311,575. Cases with missing data (n = 16,073; 5%) were excluded from the mixed-effects logistic regression model. OR = odds ratio; CI = confidence interval.
p < .05. ***p < .001.
Discussion
Both unadjusted and adjusted models indicated that veterans who were recently or currently jail/court-involved had a higher rate of receipt of pharmacotherapy for AUD compared with other veterans. Prison-involved veterans did not have significantly different odds of receiving pharmacotherapy as veterans not justice-involved. The wide variation in rates of receipt suggests that some VHA facilities have fewer barriers to pharmacotherapy for AUD for justice-involved veterans than at other facilities. It is also worth highlighting that the overall rate for veterans with and without justice involvement was low, especially compared with pharmacotherapies for other mental health disorders (Rubinsky, Chen, Batki, Williams, & Harris, 2015).
Veterans Justice Programs
The existence of Veterans Justice Programs may partially explain the difference in receipt of pharmacotherapy between veterans with and without justice involvement. Specialists from these programs provide outreach to veterans in justice settings, conduct assessments, and link them to needed treatment. A noteworthy emphasis of the program is on connecting veterans to SUD treatment, and AUD is known to be a common disorder among justice-involved veterans (Black et al., 2005; Finlay et al., 2016). Therefore, these Specialists may be identifying veterans who need treatment for AUD and directly linking them to addiction treatment services where providers have more extensive knowledge of the benefits of these medications compared with other primary care or mental health providers. One goal of these programs is to reduce recidivism. Future studies examining the long-term impact of linkage to pharmacotherapy for AUD on recidivism among veterans are needed.
Policies Related to Pharmacotherapy for Alcohol Use Disorder
Legal supervision may partially explain the higher rate of receipt of pharmacotherapy for AUD among veterans with jail/court involvement. Prior work with a general justice-involved population found that legal supervision was associated with higher odds of entry into SUD treatment (Hartwell et al., 2013). For some veterans in treatment courts, receiving treatment for SUD is part of their court requirements, which may increase their use of these medications as well as behavioral treatments. Given the recent success of an intervention that found improvements in attitudes and intentions to refer clients to pharmacotherapy (Friedmann et al., 2015), mandated trainings for probation and parole staff on the effectiveness of these medications and partnerships with addiction treatment agencies may result in increased use of pharmacotherapy. Models for utilizing VA trainers with particular domains of expertise in working with veterans, which are currently being used to train justice system personnel in other content areas, may be instructive.
Prior research has found wide variation in provision or funding for pharmacotherapy for AUD in criminal justice settings (Friedmann et al., 2012; Matusow et al., 2013); however, recent changes in U.S. drug policy may result in an increase in use of these medications. To receive federal funding, federal courts can no longer prohibit use of medications to treat SUD (Grim & Cherkis, 2015). The Department of Justice (2015) has also recently updated its policy for state, local, and tribal governments such that courts that receive funds from the Department of Justice cannot deny eligible clients access to the treatment drug court because of their use of Food and Drug Administration (FDA) -approved medications for SUD treatment. Future work examining whether veterans have access to pharmacotherapy for AUD in criminal justice settings and coordination between agencies as veterans move from incarceration to VHA treatment is needed.
Low Treatment Rates
Despite the higher rates of receipt of pharmacotherapy among veterans with a history of jail/court involvement compared to veterans with a history of prison involvement or without justice involvement, the rates of receipt are low for all three groups. Previous research has found that among veterans, use of medications to treat AUD is less than 5% at VHA nationally (Harris et al., 2012), and SUD settings outside of VHA have also been slow to adopt pharmacological treatments (Abraham, Knudsen, & Roman, 2011). Some veterans may not want to use medications, particularly if they are exiting incarceration after a period of sobriety. However, reluctance to take medications in general is not an issue for veterans with AUD. Prior research showed that among veterans with co-occurring AUD and a psychiatric disorder, 4.3% received medication for AUD, whereas 52.6% received medications for depression, anxiety, PTSD, or eating disorders (Harris et al., 2010). More recent research found that rates of receipt of pharmacotherapy for mental health disorders among VHA patients with AUD range from 69% to 82% (Rubinsky et al., 2015). Efforts to address barriers to medication use, such as academic detailing to improve clinicians’ knowledge of treatment effectiveness, are underway at VHA. Research with justice-involved veterans and justice outreach program staff at sites where veterans have high rates of receipt may provide additional insights that can augment current implementation efforts to increase use of these medications.
Age Differences
The youngest and oldest veterans in the sample had lower odds of receiving pharmacotherapy for AUD compared with veterans aged 35 to 54. These age differences are consistent with previous research examining receipt of pharmacotherapy for alcohol dependence at VHA facilities (Harris et al., 2012). Younger veterans may have traumatic brain injury (Carlson et al., 2010), which could create cognitive impairments that affect their treatment use. Conditions such as dementia are more prevalent among older veterans (Frayne et al., 2014) and may create challenges to using medications. Older veterans may also have more health problems that require medications; thus, concerns about drug interactions may limit prescribing. Although VA providers screen for traumatic brain injury, veterans with cognitive problems may need more enhanced support to ensure they are using these medications. There may also be age-related treatment preferences, but we do not know what drives these age differences.
Homeless Programs
Homeless veterans in this study had higher odds of receiving pharmacotherapy for AUD. The Veterans Justice Programs are part of VHA’s Homeless Programs; thus, the VHA’s focus on ending veteran homelessness by providing comprehensive services (O’Toole, Pape, & Kane, 2013) may explain this finding. Also, part of our definition of homelessness included veterans in homeless programs such as supportive housing. Such programs may have provided more support and motivation for veterans to seek pharmacotherapy for AUD. Facility-level research at sites where justice-involved veterans have much higher rates of receipt compared with other veterans will help shed light on strategies or context factors that increase use of these medications.
Limitations
There are limitations to our study. First, our sample was limited to veterans who received treatment at VHA facilities and may not generalize to veterans who do not use VHA care. Some veterans may have used community treatment or have received treatment while incarcerated, and we were unable to capture these visits in our data. Second, there are likely other justice-involved veterans who received care at VHA that we were unable to identify in our sample. Third, although we attempted to control for numerous patient- and facility-level differences, there may be other differences between prison- and jail/court-involved veterans compared with those not justice-involved that we were unable to account for. There may also be differences between veterans exiting prison and those who are jail/court-involved, such as requirements related to supervision and challenges associated with exiting prison, that we were unable to capture in our sample. Fourth, more nuanced work understanding severity of AUD, optimal dose of medication, and detoxification treatment related to pharmacotherapy is needed, but we were unable to assess these measures with our data. Finally, due to small sample sizes of justice-involved women, we were unable to include them in our analyses while adjusting for potential gender differences. Thus, more work is needed to examine any differences they may experience in access to pharmacotherapy for AUD.
Conclusion
Veterans with a history of jail/court involvement had higher odds of accessing pharmacotherapy for AUD compared with veterans not justice-involved or veterans with a history of prison involvement. Understanding why veterans with a jail/court history are more frequently prescribed these medications may provide unique insights into implementation efforts to improve receipt of pharmacotherapy for AUD more broadly at VHA and other addiction treatment settings. However, many facilities have very low or no use of these medications for justice-involved and other veterans, and quality improvement efforts are needed to address this gap in care.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily reflect the position nor policy of the Department of Veterans Affairs (VA) or the U.S. government.
Declaration of Conflicting Interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors are employed by the U.S. Department of Veterans Affairs, with the exception of Dr. Binswanger who is employed by Kaiser Permanente Institute for Health Research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Finlay was supported by a Veterans Affairs (VA) Health Services Research & Development (HSR&D) Career Development Award (CDA 13-279). Dr. Timko was funded as a VA HSR&D Senior Research Career Scientist (RCS 00-001). Dr. Harris was funded as a VA HSR&D Research Career Scientist (RCS 14-132).