
Abstract
As police departments in the United States strive to improve their capacity to effectively engage individuals with mental illness (IMI), Crisis Intervention Team (CIT) training has become increasingly common. Limited empirical work has studied the effectiveness of CIT, and available studies demonstrate split evidence on the effectiveness of the approach. Variation in previous findings may indicate that CIT inadequately addresses key factors that create challenges for officers when engaging IMI, such as mental illness stigma. Survey data collected from 185 officers were analyzed to assess whether mental illness stigma affects officers’ perceptions of preparedness for engaging IMI beyond CIT training itself. Findings suggest that although there are few differences in perceptions of preparedness between officers who have completed CIT training and those who have not completed CIT training, variation in levels of mental illness stigma explain differences in officers’ perceptions of preparedness to engage IMI. Policy recommendations are discussed.
In recent years, public attention toward the relationship between individuals with mental illness (IMI) and the American criminal justice system has intensified. It has become increasingly apparent that the way mental health calls are often handled by law enforcement is not the way these calls should be handled. For example, of the nearly 2,000 fatal police shootings in 2015 and 2016, mental illness played a role in one in four cases (The Washington Post, n.d.-a, n.d.-b). To improve the interaction between law enforcement and IMI, various specialized response programs have been created and implemented. Among these, the Crisis Intervention Team (CIT) model has seen precipitous growth in adoption by police organizations. However, despite the growth, few evaluations have demonstrated the effectiveness of CIT training. Moreover, the limited studies available have rendered conflicting evidence concerning CIT training’s ability to prepare officers to successfully engage IMI.
Given contradictory findings on CIT training in policing, other factors likely influence officers’ sense of preparedness for IMI interactions. Mental illness stigma, the tendency to apply negative attributes to IMI, remains a significant barrier for positive outcomes for IMI across a variety of domains (Guimon, Fischer, & Sartorius, 1999; Hinshaw & Cicchetti, 2000; Stier & Hinshaw, 2007; Wahl, 1999), and although CIT focuses on tools and skills to render better outcomes in IMI interactions, CIT training may not effectively mitigate mental illness stigma in officers. Thus, officers’ perceptions and beliefs related to mental illness stigma may persist after CIT training accounting for differences in their sense of preparedness regarding engaging IMI.
Review of the Literature
On October 31, 1963, President John F. Kennedy signed the Community Mental Health Centers Act. Originally intended to move IMI from long-term psychiatric hospitals to mental health treatment centers in the community and to increase public acceptance of IMI, some argue that the policy’s goals have not been met (Sheth, 2009). Existing community mental health services are inadequately prepared to handle the vast number of individuals requiring mental health treatment. As a result, this special population has become the de facto responsibility of law enforcement who often serve as first responders when IMI are experiencing psychiatric crises. All too often, IMI end up in the criminal justice system where it is virtually impossible for them to get the necessary treatment. In fact, housing IMI in jails and prisons is much more common today than treating them in hospitals (Fields & Phillips, 2013; Torey, Kennard, Eslinger, Lamb, & Palve, 2010).
Evidence demonstrates that IMI are disproportionately in contact with officers and constitute a substantial portion of officers’ time. It is estimated that 7% to 10% of police activity involves responding to mental health calls, and police encounters with IMI are typically longer in duration than calls with the non–mentally ill population (Deane, Steadman, Borum, Veysey, & Morrissey, 1999). The combined impact of these encounters results in other deleterious effects with IMI having 3 to 5 times more contact with law enforcement than other non–mentally ill individuals, and an arrest rate that is substantially higher (60% vs. 37%; Hartford, Heslop, Stitt, & Hoch, 2005; Heslop, Stitt, & Hoch, 2013). A review of literature regarding interactions between IMI and police revealed that, overall, 40% of IMI have been arrested at least once in their lifetime (Brink et al., 2011), and 76% of IMI in contact with police have a history of previous charges (Schulenberg, 2016). Despite the number of charges, many of the violations represent minor nuisance offenses (Hartford et al., 2005; Schulenberg, 2016).
Intervention Strategies
In response to ongoing challenges with IMI, a variety of strategies have been developed in policing. The three basic strategies to handle mental health calls include a mental health–based specialized mental health response, a police-based specialized mental health response, and a police-based specialized police response (Deane et al., 1999). Mental health–based specialized mental health responses include programs that rely on mobile crisis teams that are part of the local mental health service system and provide on-site assistance when called (Deane et al., 1999). In essence, these programs use mental health professionals to respond and call on police as needed (Spaite & Davis, 2005). In contrast, police-based specialized mental health responses involve police departments hiring mental health consultants who provide officers with either on-site or telephone assistance (Deane et al., 1999). In this model, mental health professionals co-respond with police assisting with mental health emergencies (Spaite & Davis, 2005). The third model, police-based specialized police responses, involve sworn officers receiving special mental health training on how to provide crisis intervention services (Deane et al., 1999). In this way, specially trained police officers are able to manage crisis intervention situations and act as liaisons to the mental health system (Spaite & Davis, 2005). Specialized responses may mitigate some of the aforementioned issues that confront IMI, and police-based response programs have been shown to reduce both the inappropriate use of arrest and use of jails to house IMI (Steadman, Deane, Borum, & Morrissey, 2000). The CIT model, also known as the Memphis Model, is one such response.
Developed after an individual with a mental illness was killed in a police shooting in Memphis, Tennessee (Steadman et al., 2000), the CIT program’s purpose has been to unify law enforcement and mental health professionals and services in the hope of improving interactions between police officers and IMI. As a diversion program, CIT seeks to divert IMI from the criminal justice system to mental health treatment centers, thereby reducing the risk of injury to both officers and IMI (Compton, Bahora, Watson, & Oliva, 2008). Although surveys in the late 1990s demonstrated that few departments utilized a police-based specialized police response at that time, CIT programs have been implemented in more than 2,700 communities in 45 different states over the last two decades (National Alliance on Mental Illness [NAMI], 2017).
CIT is a prebooking diversion program, designed to redirect IMI from the criminal justice system to the health care system, while maximizing officer and consumer safety during mental health calls (Dupont, Cochran, & Pillsbury, 2007). Implementation of CIT requires 10 critical core elements. These elements are classified as ongoing (i.e., partnerships between law enforcement, mental health professionals, and the community), operational (i.e., CIT training), or sustaining (i.e., evaluation and research; Dupont et al., 2007). Officers are trained in the CIT model using a 40-hr training program during which officers are taught how to recognize symptoms of mental illness and de-escalate situations involving individuals in crisis (Hanafi, Bahora, Demir, & Compton, 2008).
The training consists of three phases: structured learning, consumer and family interactions, and intensive scenario workshops. The lectures in Phase 1 cover a wide range of topics, including mental health issues (e.g., mood, thought, and cognitive disorders; substance abuse; suicide; basic psychopharmacology) and mental health support services or resources available within the community. In the interaction phase, officers visit mental health facilities or other similar sites, where they engage directly with IMI and family members. In the final phase of training, officers are taught de-escalation and safety skills and strategies, which they then practice and perfect through role-playing crisis event scenarios (Dupont & Cochran, 2002; University of Memphis CIT Center, n.d.). Self-selection is a key component of the CIT model. Departments are encouraged to maintain the voluntary aspect of the program, based on the notion that there is variation in officers’ interpersonal skills, de-escalation abilities, and experience with mental illness.
Although changing attitudes is not an explicit goal of the CIT model, officers’ perceptions and mental illness stigma are acknowledged and discussed throughout training. For instance, during lectures on psychopharmacology, CIT training highlights the importance of discussing the negative beliefs associated with individuals who use psychotropic medications. Furthermore, the national curriculum explains that the purposes of interacting with advocate organizations are, in part, to help officers understand the experiences and perspectives of IMI and to discuss beliefs about IMI (University of Memphis CIT Center, n.d.). Dupont and Cochran (2002) explain that attitudinal change, which leads to learning, is often precipitated by the consumer and family interaction phases of training.
The CIT Model and Mental Health Stigma
Despite the widespread implementation of CIT and established goals of the training, research regarding the program’s success has yielded inconsistent results. A recent systematic review of CIT research examined the situational outcomes of the three goals of the program as asserted by NAMI: officer use of force, officer injury during mental health calls, and outcomes of arrest of IMI (Taheri, 2016). The evidence suggests that, compared with non–CIT-trained officers, CIT-trained officers were less likely to arrest IMI and more likely to transport them to community mental health services; however, there were conflicting results with one study finding that CIT-trained officers were more likely to arrest IMI (Teller, Munetz, Gill, & Ritter, 2006). Of the five studies in the meta-analysis that examined use of force, none found that CIT reduced use of force outcomes. However, one study demonstrated evidence that CIT-trained officers exhibited higher levels of use of force when interacting with IMI than non–CIT-trained officers (Morabito et al., 2010). Overall, based on the evidence, Taheri (2016) concluded that the CIT model is neither significantly beneficial, nor detrimental, for either officers or IMI. Given the conflicting findings, others factors may affect officers’ interactions with IMI. Mental illness stigma may be one such factor.
Mental health stigma
Mental illness is a common problem in the United States. Evidence suggests that more than 25% of American adults live with a mental illness, and more than 11% demonstrate symptoms of multiple distinct disorders (Kessler, Chiu, Demler, & Walters, 2005). Among the issues faced by IMI, stigma is an ongoing challenge. Stigma is the tendency for outsiders to attribute any and all aspects of an IMI with mental illness itself. This process fuels a vicious cycle of social ostracism further harming IMI, and stigma represents one of the most serious issues facing IMI (Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000; Hinshaw & Cicchetti, 2000; Stier & Hinshaw, 2007). In essence, misconceptions and negative attitudes concerning IMI negatively affect these individuals (Link, Cullen, Struening, Shrout, & Dohrenwend, 1989).
Mental illness stigma is a significant barrier to positive outcomes for IMI across a variety of domains (Guimon et al., 1999; Hinshaw & Cicchetti, 2000; Stier & Hinshaw, 2007; Wahl, 1999). Society generally perceives IMI to be dangerous, incompetent, and violent, and general associations between mental illness and violence or danger lead to increased stigmatization (Corrigan & Cooper, 2005; Link, Phelan, Bresnahan, Stueve, & Pescosolido, 1999; Phelan, Link, Stueve, & Pescosolido, 2000). Evidence, likewise, suggests that fear of the dangerousness of IMI reduces helping behavior from others (Corrigan et al., 2002; Stier & Hinshaw, 2007).
Stigma has been shown to influence how police interact with IMI, and individual officers’ attitudes and beliefs, including stigma, have been shown to influence how police manage confrontations with IMI, largely affecting dispositions of the interactions as well (Ritter, Teller, Munetz, & Bonfine, 2010; Tribolet-Hardy, Kesic, & Thomas, 2015; Watson & Angell, 2007; Watson, Corrigan, & Ottati, 2004). Implicit attitudes toward IMI can drive behaviors during interactions (Dovidio, Major, & Crocker, 2000); thus, improving attitudes toward IMI is an important step in reducing stigma and improving outcomes. Moreover, classes on mental illness stigma have been shown to improve attitudes toward IMI among professional groups, thereby reducing mental illness stigma (Barney, Corser, & White, 2010; Costin & Kerr, 1962; Frailing & Slate, 2016; Madianos, Priami, Alevisopoulos, Koukia, & Rogakou, 2005; Olade, 1983).
To date, there is a paucity of empirical research examining the stigma held by law enforcement officers toward IMI, specifically research investigating how mental illness stigma differs between CIT-trained and CIT-untrained officers. The limited research that has been conducted on officers’ understanding of IMI is more consistent than the research on situational outcomes of CIT, with findings generally supporting the effectiveness of training at improving officers’ knowledge about IMI (Compton, Esterberg, McGee, Kotwicki, & Oliva, 2006; Hanafi et al., 2008; Wells & Schafer, 2006). Some CIT research suggests that officers’ recognition of IMI may be positively affected by the training, with CIT-trained officers exhibiting a greater ability to appropriately identify IMI; also, CIT-trained officers demonstrate a greater knowledge base about available mental health treatment and services (Compton et al., 2008; Wells & Schafer, 2006). Furthermore, qualitative assessment demonstrates that CIT-trained officers generally report a greater sense that they are able to handle mental health calls (Hanafi et al., 2008). Despite the findings of the previous research on CIT training’s impact on officer attitudes, less is understood concerning CIT training’s impact on mental illness stigma and the interplay between mental illness stigma and officers’ sense of preparedness for handling calls involving IMI. This limitation in the literature is noteworthy, given the availability of validated scales measuring mental illness stigma.
Mental illness stigma includes seven specific dimensions. Interpersonal anxiety reflects feelings of anxiousness, nervousness, uneasiness, fear of physical harm, and general danger when around IMI (Day, Edgren, & Eshleman, 2007; Hawke, Michalak, Maxwell, & Parikh, 2014; Stone & Merlo, 2011). Relationship disruption includes feelings about mental illness impairing meaningful relationships, and typically measures whether or not an individual believes he or she can have a normal and healthy relationship with an IMI (Day et al., 2007; Stone & Merlo, 2011). Although this may reflect a belief that IMI cannot maintain meaningful relationships, it can likewise reflect an individual’s sense that he or she cannot maintain a personal relationship with an IMI (Hawke et al., 2014; Imhoff, 2016). Poor hygiene reflects stereotypes about the physical appearance of IMI including a perceived lack of ability among IMI to care for themselves (Day et al., 2007; Hawke et al., 2014; Imhoff, 2016; Stone & Merlo, 2011). Visibility reflects an individual’s belief that he or she can discern mental illness in others through the recognition of visual clues (Day et al., 2007; Hawke et al., 2014; Imhoff, 2016; Stone & Merlo, 2011). Treatability reflects an individual’s beliefs about whether mental illness can be treated (Day et al., 2007; Hawke et al., 2014; Stone & Merlo, 2011). Professional efficacy concerns the belief that mental health professionals have appropriate skills and are effective at the treatment of mental illnesses (Day et al., 2007; Hawke et al., 2014; Imhoff, 2016; Stone & Merlo, 2011), and recovery reflects beliefs that IMI have the potential to recover from their mental illness (Day et al., 2007; Hawke et al., 2014; Stone & Merlo, 2011).
Whereas the previous research on CIT has demonstrated that officers’ understanding of mental illness and awareness of resources for assisting IMI generally improve after CIT training, the need for further research in this area is discussed in the available literature on CIT (Compton et al., 2006; Hanafi et al., 2008; Ritter et al., 2010). The present study considers the impact of CIT training on mental illness stigma in officers, which is important for two key reasons. First, the national curriculum for CIT asserts that interacting with advocate organizations should help officers understand the experiences and perspectives of IMI and facilitate discussions about mental illness stigma (University of Memphis CIT Center, n.d.). Furthermore, Dupont et al.’s (2007) paper on the core elements of CIT and The University of Memphis CIT Center’s online site both specifically assert that CIT reduces stigma. Despite these claims, the impact of CIT training directly on mental illness stigma remains unstudied.
Second, the present study moves beyond limitations in the available research on CIT. Previous research has examined officers’ attitudes about IMI using scales, such as the Opinions About Mental Illness (OMI) Questionnaire, that, although used extensively to assess attitudes about mental illness (see, for example, Holmes, Corrigan, Williams, Canar, & Kubiak, 1999; Keane, 1990, 1991; Todor, 2013), were designed for use by psychiatric hospital personnel, a population that has extensive experience with IMI (Cohen & Struening, 1962). Furthermore, these scales measure factors, such as benevolence, authoritarianism, and interpersonal etiology that are conceptually distinct from mental illness stigma. Utilizing a validated scale for measuring the key dimensions of mental illness stigma, the present study assesses whether levels of mental illness stigma vary between CIT-trained and CIT-untrained officers. Also, the study explores whether differences in mental illness stigma affect officers’ sense of preparedness for handling IMI calls while controlling for CIT training.
Method
To determine the impact of CIT training on mental illness stigma and the impact of mental illness stigma on officer perceptions of preparedness when encountering IMI, 185 police officers from five police departments in Connecticut were surveyed. The sample was predominately White (70.7%), with about a quarter self-identifying as either Hispanic or Black (13.8% and 10.5%, respectively). Four officers did not report their race. Almost 90% of participants were male (n = 163), 10.4% were female (n = 19), and three participants did not indicate sex. All officers had some level of postsecondary education, except for 19 officers whose highest level of education was a high school diploma or equivalent. Seventy officers had some college education, whereas 82 officers held a bachelor’s degree. Ten officers held a graduate degree and four did not indicate their level of education. The average age of participants was 37.11 years (min = 25, max = 63, SD = 9.36 years). Officers’ years of experience ranged from 6 months to 40 years (M = 10.59, SD = 9.14). Just more than half of participants had completed CIT training at the time the survey was administered (n = 94). Eighty-four non–CIT-trained officers participated in the current study, and five did not report their CIT status. All departments had CIT-trained officers in the study, and the percent of CIT-trained officers did not statistically vary between departments.
Measures
The survey was administered to officers during roll call at the beginning of each shift. In total, researchers attended 15 roll calls at five different police departments. The survey was distributed after researchers explained the study and obtained informed consent from officers. Participants generally took 10 to 15 min to complete the questionnaire, and no incentives were offered. Survey participation was voluntary, and the overall response rate was 91%. Law enforcement attitudes toward IMI were assessed using a survey instrument, a modified version of Day’s Mental Illness Stigma Scale (Day et al., 2007). The scale measures the seven factors of mental illness stigma: interpersonal anxiety, relationship disruption, poor hygiene, visibility, treatability, professional efficacy, and recovery. The original survey consists of 28 items assessed on a Likert-type scale ranging from 1 (completely disagree) to 7 (completely agree). The data were analyzed to determine the reliability of the question sets associated with each factor measuring mental illness stigma. Reliability for each factor was assessed using Cronbach’s alpha, and the initial reliability analysis is presented in Table 1.
Reliability of Factors in Day’s Mental Illness Stigma Scale.

Although six of the seven factors demonstrated acceptable reliability, visibility did not. The three questions that formed visibility rendered an initial alpha of .587. As such, one question was dropped from the set rendering an alpha of .61. Based on the reliability analysis, the question sets measuring each factor were converted into scale measurements by calculating the mean for all questions retained. This rendered measurements, where higher values indicate increasing agreement. These scale measurements were then used for analysis. In addition to mental illness stigma, two items were included to measure officers’ sense of preparedness when encountering IMI. The prompts were “I feel comfortable handling mental health calls” and “Force is more likely necessary when dealing with individuals with a mental illness.” As with the mental illness stigma measurements, higher levels for the officer perception measures indicate greater comfort with IMI calls and a greater likelihood that use of force may be required.
Analyses
Two sets of analysis were run. The first set sought to discern whether CIT-trained and non–CIT-trained officers differed in levels of mental illness stigma. These differences were assessed through independent samples t tests conducted for each of the mental illness stigma factors. Next, ordinary least squares (OLS) regression models were estimated to determine the impact of CIT training, the seven stigma factors, and demographic characteristics of officers on officers’ individual perceptions of level of comfort when handling calls for service involving IMI as well as individual perceptions concerning the likelihood that these calls may involve the use of force. One OLS regression model was estimated for each outcome.
Findings
Initial analysis indicated that, in general, officers exhibited higher levels of visibility and professional efficacy, indicating that officers believe they can identify mental illness, and professionals are capable of handling IMI. However, they also generally disagreed with the idea that mental illness is treatable or that IMI can recover from mental illness. Officers reported low levels of anxiety related to IMI interactions and low levels of stigma concerning hygiene. Regarding officer perceptions of interactions with IMI, officers indicated slight disagreement that they were comfortable handling calls with IMI. Similarly, they indicated relatively strong agreement that calls involving IMI may require the use of force. Descriptive statistics for all mental illness stigma and officer perceptions are presented in Table 2.
Descriptive Statistics.
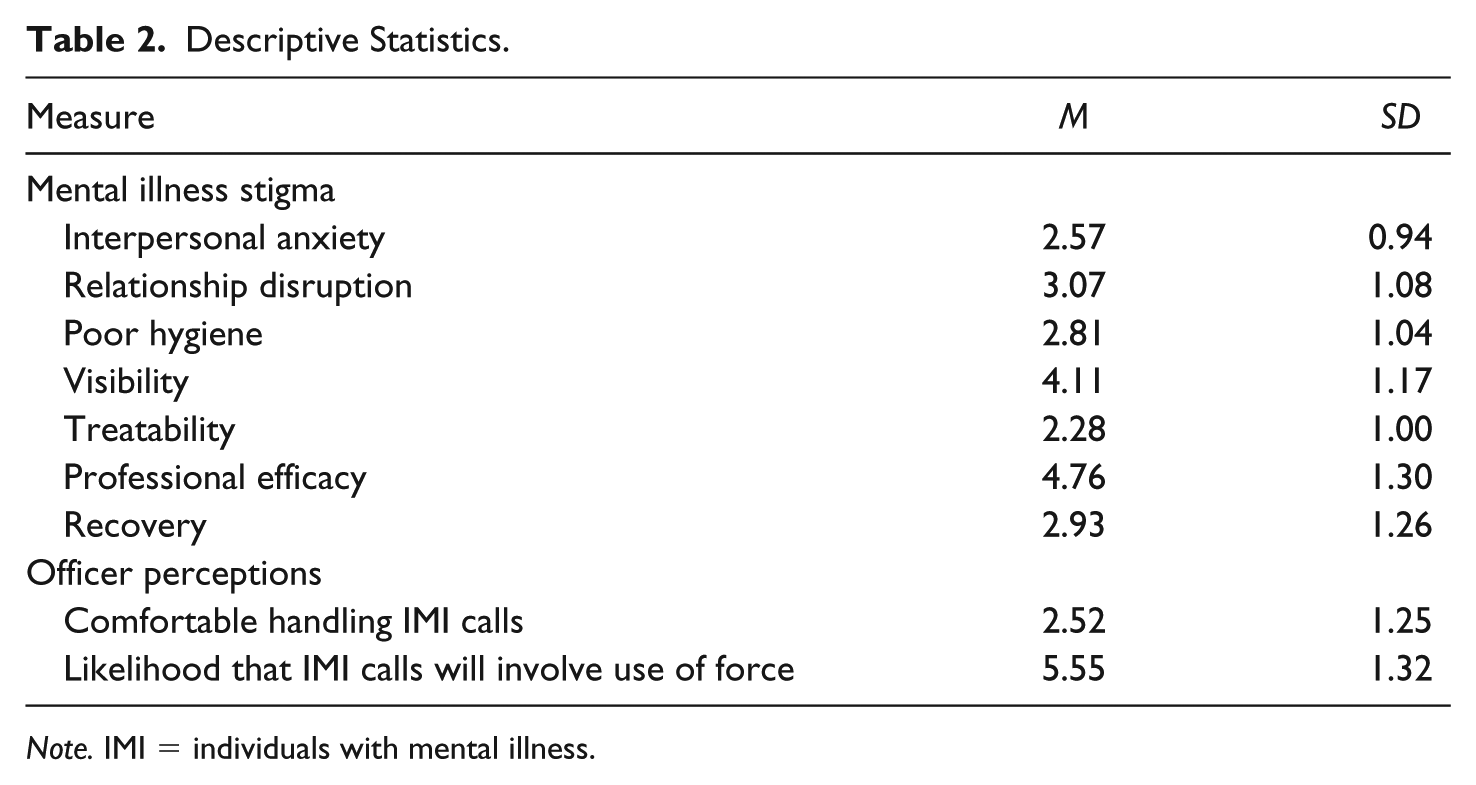
Note. IMI = individuals with mental illness.
CIT Training and Mental Illness Stigma
The first set of analyses sought to determine whether CIT training affects levels of mental illness stigma among officers. Independent samples t tests were conducted to determine whether CIT-trained officers exhibited lower levels of mental illness stigma than non–CIT-trained officers. Results of the tests are reported in Table 3. The findings suggest that CIT training does not effectively reduce mental illness stigma among officers.
Differences Between CIT-Trained and Non–CIT-Trained Officers.
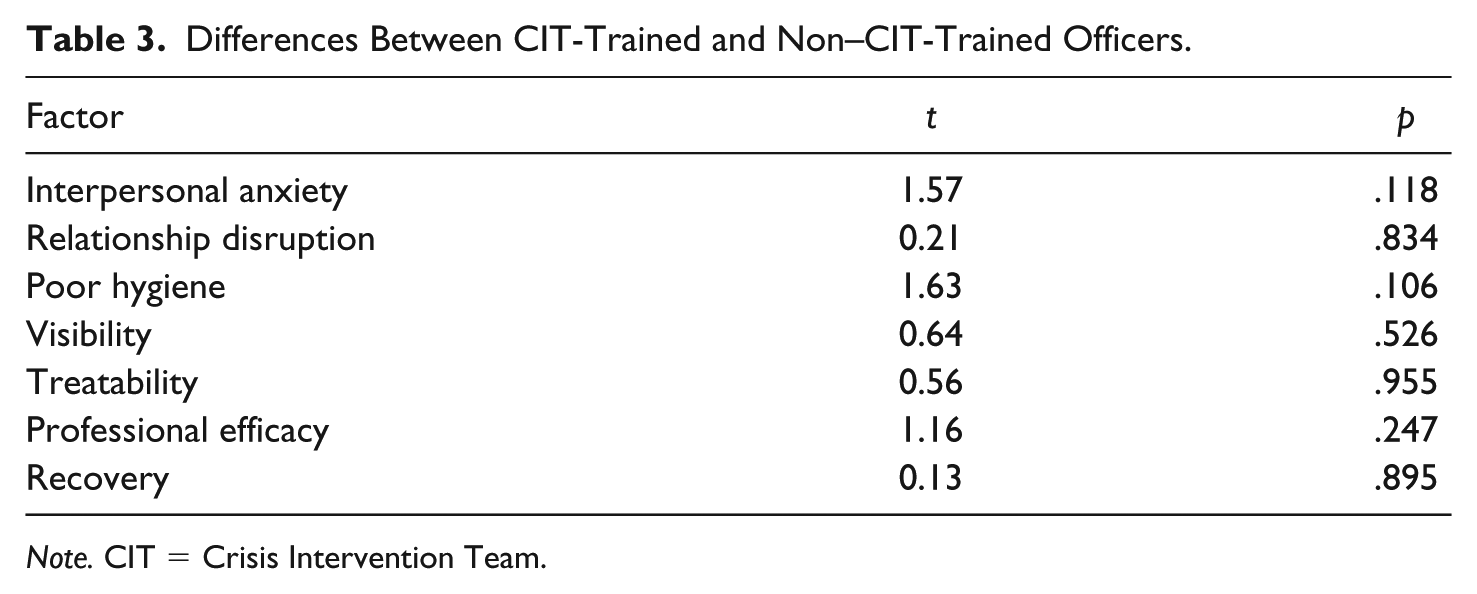
Note. CIT = Crisis Intervention Team.
Although none of the mental illness stigma factors statistically varied between the groups of officers, CIT-trained and non–CIT-trained officers did vary on some specific items. First, CIT-trained officers had a lower level of agreement than non–CIT-trained officers with an item from the hygiene factor, “People with mental illnesses tend to neglect their appearance” (p = .047). For an item in the anxiety construct, “When I am around someone with mental illness I worry that he or she might harm me physically,” CIT-trained officers again had a lower level of agreement (p = .043). In contrast, CIT-trained officers had a higher level of agreement than non–CIT-trained officers with an item in the professional efficacy factor, “Psychiatrists and psychologists have the knowledge and skills needed to effectively treat mental illnesses” (p = .032).
Mental Illness Stigma and Officer Perceptions
The next set of analyses sought to determine whether mental illness stigma accounted for differences in officers’ perceptions regarding comfort handling IMI calls as well as their sense that use of force may be required on these calls. Two separate regression models were estimated, one for each perception. The first model considered sense of comfort, and the second considered likelihood of use of force. The regression results are presented in Table 4. The first model for handling calls revealed independent variables that were related to officers’ sense of comfort when responding to calls involving IMI. The model was significant and explained 22.4% of the variation in officers’ sense of comfort. Three variables had independent impacts on officers’ sense of comfort. Officers reporting higher levels of interpersonal anxiety typically expressed less comfort with IMI calls. Officers reporting higher visibility typically expressed greater comfort with IMI calls, and male officers typically expressed greater comfort with IMI calls. Of the related variables, interpersonal anxiety had the largest effect on level of comfort.
OLS Regression Models (Standardized Coefficients Reported).

Note. OLS = ordinary least squares; CIT = Crisis Intervention Team.
p < .10. *p < .05. **p < .01. ***p < .001.
The second model for use of force revealed independent variables that were related to officers’ sense that calls involving IMI may result in the use of force. The model was significant and explained 28.0% of the variation in officers’ perceptions. Four variables had independent effects. Officers reporting higher levels of interpersonal anxiety, poor hygiene, and recovery typically expressed greater perceptions that IMI calls may involve use of force. Similarly, White officers typically expressed greater perceptions that IMI calls may involve use of force. As before, interpersonal anxiety had the largest effect size. Two exploratory findings were noted, visibility and age were both negatively related to perceptions that IMI calls may involve the use of force.
Discussion
The stigma associated with mental illness constitutes one of the most significant obstacles encountered by IMI and can often be worse than the illness itself (Mental Health Commission of Canada, n.d.). The central tenet of a set of guidelines developed to identify the common features of effective responses to mental health calls is the need for law enforcement to always resist assuming stereotypic attitudes and to be mindful of the harmful effects that stereotyping can have on IMI. It is imperative that during mental health crisis situations, “stigma, false assumptions, and stereotypes do not inappropriately and adversely influence the process” (Coleman & Cotton, 2010, p. 47). The findings from the present study yielded several important considerations for police departments and training development related to this concern.
First, and perhaps most surprising, there were no significant differences in levels of mental illness stigma between officers who had completed CIT training and those who had not. This is generally inconsistent with previous research, which has found improvement in officer attitudes toward IMI and an increase in self-efficacy post-CIT training (Compton et al., 2006; Hanafi et al., 2008; Wells & Schafer, 2006). Independent of CIT training, higher interpersonal anxiety was related to less comfort in handling mental health calls and greater concerns that use of force may be necessary. Importantly, this factor emerged as having the greatest effect on both outcomes. This suggests that further addressing anxiety related to IMI might be beneficial. In addition, officers who expressed greater belief that they can recognize mental illness expressed more comfort in handling mental health calls. This, likewise, suggests that further developing officers’ recognition of mental illness would support better outcomes for IMI and officers.
Overall, the findings indicate that CIT training may not influence officers’ attitudes toward IMI in all regards. Previous research does not identify which elements of CIT training are most important to which outcome (Ritter et al., 2010; Watson, Morabito, Draine, & Ottati, 2008); yet, the results herein indicate that certain factors, such as interpersonal anxiety and visibility, are associated with key perceptions among officers that likely define interactions with IMI. Specifically, because these factors were related to officer sense of comfort and the perceived likelihood that use of force may be necessary, targeting these factors may be an important part of the process of better addressing the challenges related to officer interaction with IMI. These components of stigma may define officers’ initial attitudes when encountering IMI; thus, these factors may ultimately relate to negative outcomes resulting from these interactions. Given these findings, the CIT curriculum may need modification placing greater emphasis on these areas to provide greater value for police departments.
The findings are, likewise, informative for police organizations more generally. Given challenges related to implementing the CIT model at a departmental level (Watson et al., 2008) and challenges to altering CIT curriculum already in place, the findings suggest that departments could potentially benefit by offering trainings aimed at reducing officers’ stigma toward mental illness in these specific areas as an adjunct to CIT training. For organizations that have not currently adopted the CIT model, rather than implementing the CIT model as a whole, addressing these key areas through other training programs might render benefits. Because research on the effectiveness of CIT continues to produce inconsistent findings, it is possible that focusing on certain categories of attitudes could be more cost efficient and more effective at decreasing stigma.
The present study has three key limitations. Given that perceptions of CIT officers were not assessed prior to the training, it cannot be concluded that CIT does not change mental illness stigma in officers. The voluntary nature of CIT training may relate to a lack of differences between CIT- and non–CIT-trained officers. Given that CIT training may be recommended within departments to officers who exhibit a greater struggle with IMI-related calls for service, CIT training may affect their levels of stigma without raising them above non–CIT-trained officers. Additional research using a pre-/postdesign should address this issue.
Second, the study is based on perceptual data rather that outcome data. Although officers may report that they feel uncomfortable when encountering IMI, this does not necessarily mean that they will respond differently than officers who feel more comfortable with the situation. Likewise, a perceived sense that IMI encounters may require use of force does not indicate that these officers will use force in different circumstances than other officers. Given the available research that associates mental illness stigma with worse outcomes for IMI in interactions in other arenas, the available data on police perceptions of preparedness provide an initial glimpse into challenges created by mental health stigma. Future research should further investigate these issues. Although mental health trainings aimed at reducing stigma in specific categories of attitudes may affect officers’ perceptions, examining whether and how changes in attitude are associated with changes in behavior is key to developing and implementing effective trainings that improve interactions between IMI and law enforcement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.