
Abstract
Policing persons with mental illness and/or emotional/behavioral issues is complex and difficult. Police interactions and encounters of this nature are expected to increase due to dwindling budgets and the resulting deficiencies of local mental health systems. Police departments are responding to this growing need by requiring officers to attend Crisis Intervention Team (CIT) Training. CIT Training is designed to teach officers about mental illness and effective strategies and techniques for engaging and de-escalating potentially volatile interactions and encounters. This study was conducted in a large, Midwestern, municipal police department. The data were triangulated and included: (a) CIT Training pre- and post-tests administered to officers (N=323) prior to and upon completion of the required 40-hour CIT Training held during the months of October through December 2016 and February through May 2017; (b) participant observation with police patrol officers in three of the seven police districts (N=127 hours; April 2017 through May 2017); (c) semi-structured interviews with police patrol officers assigned to three of the seven police districts who had completed the CIT Training (N=32 patrol officers; intensive interviews were conducted during participant observation); (d) in-person semi-structured interviews with service providers/practitioners who interact with officers in the context of their working roles and responsibilities (N=27; July 2017 through January 2018); and (e) interviews with Urbantown Police Department (UPD) executive command staff, CIT coordinators and UPD telecommunications personnel (N=10; September 2017 through January 2018). The assessment finds that the CIT Training administered in a large, municipal police department changed officers’ perceptions, as well as their street-level practices with persons with mental illness and/or emotional/behavioral issues. This assessment also finds that police officers are taking fewer persons into custody for involuntary treatment, and are instead transporting more persons for voluntary treatment.
Keywords
The impact of Crisis Intervention Team Training for police
Police officers routinely interact with persons with mental illness and/or emotional/behavioral issues (Bittner, 1967, 1975; Borum et al., 1998; Engel and Silver, 2001; Livingston et al., 2014). Scholars have argued that with declining budgets and local mental health system deficiencies, these types of interactions are becoming even more frequent (Finn and Stalans, 2002; Green, 1997; Jaffe, 2009; Livingston et al., 2014). In some cases, these interactions can become volatile, as persons in states of crises are oftentimes not completely rational. Worst-case scenario, these interactions may result in major critical incidents in which people’s lives, including those of the officers involved, are forever changed (Finn and Stalans, 2002; Jaffe, 2009). In order to meet the growing need and to prepare police officers for interactions and encounters with persons with mental illness and/or emotional/behavioral issues, many police departments have turned to Crisis Intervention Team (CIT) Training.
CIT Training is designed to better equip officers to interact with persons with mental illness and/or emotional/behavioral issues who may be experiencing crises. More specifically, with respect to police officers, CIT Training focuses, in part, on teaching officers about mental illness and techniques for de-escalating potentially volatile interactions, as well as catastrophic outcomes, with persons with mental illness in states of crises (Compton et al., 2000, 2008, 2011; Hirschel et al., 1994; Watson and Fulambarker, 2012). Over 2700 police agencies have implemented a CIT-type training (Taheri, 2016). Although empirical research has not conclusively established the efficacy of CIT Training, assessments suggest that CIT Training may be effective in changing officers’ perceptions, street-level practices and/or enforcement practices (Compton et al., 2008, 2017; Ellis, 2014; Taheri, 2016; Teller et al., 2006; Watson et al., 2010). The current study adds to the growing body of extant research on the efficacy of CIT Training in policing.
Policing persons with serious mental illness
Many behavioral health experts acknowledge that some persons with untreated serious mental illness tend to be more violent than the general population (Dawson and Langan, 1994; Douglas et al., 2009; Fazel and Grann, 2004; Jaffe, 2017; Joyal et al., 2007; Link et al., 1992; Monahan, 1992; Taylor, 2008; Van Dorn et al., 2012). It is not that persons with serious mental illness have a higher propensity for criminality. It is that persons with untreated serious mental illness react to situations and stressors differently, and oftentimes irrationally, which can prompt aggressive and violent reactions (i.e., going into flight or fight mode when expecting or perceiving imminent harm). That is, persons with untreated serious mental illness who may believe themselves imminently vulnerable to harm from others oftentimes react aggressively and violently (Jaffe, 2017). This is an experiential issue; persons with untreated serious mental illness experience the world differently from members of the general public. They also react and cope differently. Persons with substance abuse issues also experience and respond to situational cues differently, and less rationally, from the general population (Van Dorn et al., 2012).
These volatile, aggressive and violent reactions can be exacerbated during interactions with the police. Police officers personify force, or the threat of force, by their mere presence. Citizen calls for police service involving mentally ill persons, those affected by substance abuse (e.g., alcohol and/or drugs), and engagements where officers must take persons into custody (i.e., arrest or emergency detention) are the most dangerous calls to which police respond (Bierie et al., 2016; Hirschel et al., 1994). Approximately one-quarter of persons killed by police display signs of mental illness (Nix et al., 2017) and/or are under the influence of alcohol or drugs (Hirschel et al., 1994). Each year, there are about 55,000 assaults against police; this represents a risk of one assault for every ten police officers (Bierie, 2017; Zimring, 2017). Further, there is a recent trend demonstrating a 56% upswing in police fatalities, from 41 officers killed in 2015 to 64 killed in 2016 (National Law Enforcement Officers Memorial Fund Fatalities Report, 2016). A significant portion of these incidents involve persons with emotional/behavioral issues and/or those with untreated serious mental illness (Jaffe, 2017).
Although danger is an inherent possibility that accompanies the nature of the job, the threat of danger to officers is intensified in encounters and interactions involving persons not functioning in a fully rational manner (Bittner, 1975). There is no doubt that the job of a police officer, particularly in major urban areas, is complex and that officers’ social responsibilities have expanded over time. In their role as first responders, police officers are now required to act as mental health practitioners, social workers, law enforcers, paramedics, mechanics, animal control agents, crossing guards, teachers, negotiators, building inspectors, health inspectors, customer service representatives, drugs and alcohol specialists, domestic violence advocates, counselors, weapons experts, disciplinarians, translators, loss prevention agents, paralegals, guardians, mediators, public transport servers, and so on. Many are underprepared to meet all of these needs, especially the needs of persons with complex mental illness issues. Consider, for example, that most mental health practitioners have at least one graduate degree in their area of specialization; most are also required to work a certain number of hours in a clinical setting prior to receiving certification to treat persons with serious mental illness.
Conversely, police are regularly mobilized to interact with people who are generally not at their best, those who are in a state of personal and/or mental health crisis, distressed, traumatized, impaired and/or suspected of unlawful activity (Bittner, 1975) with just a minimal required amount of education and police training (Bradford and Pines, 1999; Hirschel et al., 1994; Police Executive Research Forum, 2016). The regularity of these occupational experiences, and the ensuing strain, can influence officers’ street-level responses and interactions, as well as their own mental health (with collateral damage that extends into personal relationships). Specialized training, such as CIT, therefore, is promising in its potential to more adequately prepare officers to deal and cope with these types of encounters on the street, as well as in their personal lives.
CIT Training
The CIT program originated in Memphis and, accordingly, has become known as the “Memphis Model.” The CIT program in Memphis was precipitated by that city’s own major critical incident in which a Memphis police officer fatally shot a man who suffered from mental illness and substance abuse. Understanding the nature of these frequent interactions, the Memphis Police Department, in collaboration with mental health and addiction specialists, created the CIT program to “increase safety in encounters and when appropriate, divert persons with mental illnesses from the criminal justice system to mental health treatment” (Watson and Fulambarker, 2012: 2). More than 2700 agencies have replicated and/or initiated a Memphis CIT-type training program (Taheri, 2016). The International Association of Chiefs of Police (2010) calls CIT a “promising practice.”
In theory, CIT officers who have completed the training are better equipped to engage persons with mental illness and/or emotional/behavioral issues and more capable of de-escalating potentially volatile encounters with persons in crises (Compton et al., 2008, 2011; Hirschel et al., 1994; Watson and Fulambarker, 2012). Although research has not conclusively established the efficacy of CIT Training and the Memphis model (Compton et al., 2008; Taheri, 2016), mental health practitioners and advocates, police administrators and even the United States Supreme Court (see Sheehan v. City and County of San Francisco) stress the need for effective training and policy on police interactions with persons with emotional/behavioral issues and/or mental illness.
The centerpiece of the Memphis model is the voluntary 40-hour collaborative mental health and de-escalation training program for police officers who meet the criteria for selection to the team (Oliva and Compton, 2008; President’s Task Force, 2015). By making the CIT program voluntary, the Memphis Police Department sought to attract officers with a strong interest and, ideally, a passion for working with and helping persons with mental illness. Memphis Police Department leaders expected that officers who volunteered for the program would be more receptive and influenced by the training. Their formal selection process then provided an infrastructure to ensure that not only were these officers interested and passionate but also that, among the officers who volunteered, only the most qualified officers would be distinguished as CIT officers (Dupont et al., 2007; See also City of Memphis CIT website https://www.memphistn.gov/government/police_department/crisis_intervention_team).
The Memphis model CIT Training is designed to provide officers with knowledge regarding the nature and indicators of mental illnesses, how to engage persons in crises, and techniques to de-escalate potentially volatile encounters (Dupont et al., 2007). De-escalation, according to the United States Department of Justice (2015), involves the strategic slowing down of engagements to allow officers the time, distance, space and tactical flexibility needed during dynamic street-level situations. The Police Executive Research Forum (2016: 14), stressing the need for police de-escalation training, has argued that not only will de-escalation strategies reduce dependence on police use of physical force, but that “changing how agencies approach certain types of critical incidents can increase officer safety in those situations.” CIT Training also provides officers with information regarding resources available for persons suffering from mental illness and introduces officers to persons actually suffering from mental illness, the goal of which is to humanize and help officers empathize (Taheri, 2016). Significant attention is also provided on the impact these encounters can have on officers themselves and ways in which to cope. At the conclusion of the week-long voluntary training, police officers become specialized CIT officers who are regularly dispatched to calls for service involving persons with mental illness and/or emotional/behavioral issues who may be in crises (Watson and Fulambarker, 2012).
Current study
In December 2014, following a major critical incident involving police use of lethal force and based upon recommendations from the local mental health task force, Urbantown’s mayor and police chief announced that all police officers would be required to complete the 40-hour CIT Training. This decision marked a departure from the Memphis model, which prescribes voluntary participation and completion of the 40-hour CIT Training. Directly following the press conference and public announcement of the mandate, the decision to require training was regarded positively and deemed responsive to consumers, local mental health professionals and advocates, as well as other concerned parties. About a year into the training, the decision to mandate the CIT Training received only mixed support while, at the same time, garnering much public criticism. What began as concern for the welfare of consumers eventually became political, with some mental health clinicians and advocates withdrawing their support of the CIT Training mandate for a variety of reasons.
Nevertheless, in 2015, the Urbantown Police Department (UPD; a pseudonym) commenced with its mandatory CIT Training. At the end of 2016, they initiated an assessment to determine the efficacy of the CIT Training. This paper presents some of the findings from that larger assessment.
Methodology
The UPD is a large, municipal police department situated in the Midwest. UPD employs approximately 1800 sworn officers serving a city with a population just under 600,000. According to the 2010 Census, Urbantown is one of the poorest cities in the United States, with a poverty rate in 2016 of 28.4 %. It has above average property and violent crime rates, and FBI uniform crime reports data for 2017 indicates that it is one of the most violent cities in the United States. In addition to its crime problems, Urbantown has a large population of persons in need of treatment, voluntary and involuntary, for mental illness and/or severe emotional/behavioral issues.
A local study found that Urbantown has one of the nation’s highest rates of emergency detentions. An emergency detention involves taking persons into custody for purposes of involuntary treatment (Kissinger, 2013). Kissinger (2013) reports that in any given year, about 13,000 consumers are brought to the county’s psychiatric emergency room; of the 13,000 consumers, about two-thirds are brought in on emergency detentions. Among those 13,000, a little over one-third are frequent utilizers (Kissinger, 2013).
According to state statute, a police officer may take an individual into custody if the officer “has cause to believe that the individual is mentally ill, is drug dependent, or is developmentally disabled, that taking the person into custody is the least restrictive alternative appropriate to the person’s needs….” In Urbantown, police officers are solely responsible for the decision to take a person into custody for involuntary treatment/emergency detention. Furthermore, police officers in Urbantown are not required to consult with mental health clinicians prior to making the emergency detention decision. This is unique to the particular county in which Urbantown is located, as state law mandates that police officers in every other county in the state consult with mental health clinicians prior to taking consumers into custody on emergency detentions.
The emergency detention decision is a critical one, as police officers are infringing on the civil rights of persons when they take them into custody involuntarily for purposes of treatment. For those persons who are taken into custody for involuntary treatment, this process may not only exacerbate mental instability, but actually trigger violent self-protective responses (Jaffe, 2017). The emergency detention decision may also carry with it all of the effects of the stigma, trauma and embarrassment of being arrested for criminal conduct, as emergency detention processes simulate, to some degree and in some cases, arrest processes (Corrigan et al., 2003). Proper training, then, for police officers is crucial.
CIT Training assessment
UPD’s CIT Training curriculum was modeled after the Memphis CIT Training curriculum, but included a strong emphasis on the legal bases and appropriate criteria for initiating emergency detentions. Similar to Memphis, the training was collaborative in nature, including modules taught by local mental health clinicians and advocates, Veteran’s Affairs personnel, UPD police officers, and persons with serious mental illness. The training was 40 hours, spanning five 8-hour days, and was administered in UPD’s Training Academy. The UPD CIT coordinator organized all CIT Training sessions. Sessions were held monthly.
UPD’s mandatory CIT Training began in 2015; UPD initiated the assessment in late 2016. At this time, over half of all officers had already completed the training. This meant the assessment would be limited in scope and statistical power (as a result of a smaller sample size). Additionally, UPD did not have adequate baseline data upon which to compare factors before and after completion of CIT Training. That is, UPD did not systematically collect and archive data on important, related factors, such as the number of emergency detentions, number of voluntary transports for mental health treatment, number of calls involving persons with mental illness, use of force on calls involving persons with mental illness, etc. Consequently, the assessment could not include analyses of important data points and benchmarks without making huge, and likely erroneous, assumptions. For example, there is no way to isolate the impact of CIT Training on street-level indicators of performance, e.g., including analyses of officer use of force data on all calls for service or citizen complaints before and after CIT Training completion. Further, because all officers were required to complete the training, and over half of the officers had already completed it, there was no opportunity for the use of control or comparison groups.
Despite these challenges, the data for the larger assessment were triangulated. The data sources included: (a) CIT Training pre- and post-tests administered to officers (N=323) prior to and upon completion of the required 40-hour CIT Training held during October through December 2016 and February through May 2017; (b) participant observation with police patrol officers in three of the seven police districts (N=127 hours; April 2017 through May 2017); (c) semi-structured interviews with police patrol officers assigned to three of the seven police districts who had completed the CIT Training (N=32 patrol officers; intensive interviews were conducted during participant observation); (d) in-person semi-structured interviews with service providers/practitioners who interact with officers in the context of their working roles and responsibilities (N=27; July 2017 through January 2018); and (e) interviews with UPD executive command staff, CIT coordinators and UPD telecommunications personnel (N=10; September 2017 through January 2018). Data for this paper are primarily drawn from analyses of CIT Training pre- and post-tests, semi-structured interviews with police patrol officers, and participant observation of police patrol officers.
The data in this assessment were both qualitative and quantitative in nature. Individuals, as the units of analyses, were asked their perceptions of various aspects of policing related to contextual understandings of policing persons with mental illness and/or emotional/behavioral difficulties and the CIT Training. Semi-structured interviews allowed for direct comparison of responses across respondents/participants, but also provided opportunities for them to elaborate, discuss other issues of importance, and expand on matters not known or conceived during interview schedule construction. As an assessment of elements of UPD, the data collection and analysis strategy was designed to provide constructive feedback and information to assist UPD commanders and administrators in fashioning more effective training, strategies, and programming regarding policing persons with mental illness and/or emotional/behavioral issues.
CIT Training pre- and post-tests
Pre- and post-tests were administered to all officers who attended the mandated CIT Training sessions conducted during October through December 2016 and February through May 2017. Officers completed the pre-test at the start of the training session before the training commenced; officers completed the post-test at the end of the training session following completion of all training modules. All pre- and post-tests were administered directly by the author. A total of 323 officers completed both the pre- and post-tests.
Among the 323 officer respondents who attended the CIT Training and completed a pre- and post-test, approximately 73% (N=227 out of 312) were white, 11% black (N=35), 10% Latino/Hispanic (N=30 out of 312), 3% Asian (N=8) and 4% other/multiracial (N=12). Eighty-five percent (N=268 out of 315) of the participants were male; 15% were female (N=47 out of 315). Almost Eighty percent of the respondents had at least an associate degree (N=249 out of 323), with almost 37% of those (115 out of 323) having either a bachelor’s degree and/or master’s degree. Most of the respondents were assigned to patrol (N=255 out of 307, 83%), with an average of 13 years on the force (range was 2 to 30 years). Thirty-three percent (N=106) of the respondents reported that they had a family member with a diagnosed mental illness; 26% (N=85) reported that they had a friend with a diagnosed mental illness.
There were three outcome measures on the CIT pre- and post-test: (a) general perceptions of emotionally disturbed persons, (b) perceptions of the dangerousness of emotionally disturbed persons and (c) perceptions of preparedness to handle encounters with emotionally disturbed persons. In this context, “emotionally disturbed person” was operationalized as: “a person exhibiting indicators of a mental health issue/crisis and/or emotional impairment (e.g., impairment due to drugs, alcohol, medical condition, etc.) that is affecting behavior” (explicitly stated on the pre- and post-test). The Mental Health Attitude Survey for Police (Clayfield et al., 2011) provided the measurements for two of the outcome measures: general perceptions of emotionally disturbed persons and perceptions of preparedness to handle encounters with emotionally disturbed persons. The perceptions of the dangerousness of emotionally disturbed persons scale was taken from the work of Phelan and Link (2004). Minor changes to the measurements were made based on context specific information and feedback from the UPD CIT coordinator.
Interviews and observation of police patrol officers
The author conducted 127 hours of participant observation with police patrol officers in three of seven police districts. Semi-structured interviews were conducted with these patrol officers during participant observation. The interview schedule consisted of 25 open-ended questions (in addition to questions regarding demographics of respondents). Data from the questions regarding the efficacy of the CIT Training are utilized in this paper. All field notes and responses were recorded with pen and paper and later transcribed into Microsoft Word; these data were then imported into Microsoft Access to allow for analyses.
Among the officers who participated in the participant observation and semi-structured interviews, all but six were male (81%, N=26 of 32). Twenty-seven of the participating officers (84%) were white; the remaining five were Hispanic. All of the respondents were assigned to patrol with an average of about 8 years on the force (range 1 to 17 years). All but one of the officers had completed the mandatory CIT Training. Seven of the 32 participating officers had completed mandatory CIT Training while in the academy for initial recruit training. All other officers completed the mandatory CIT Training as in-service training (78%, N=25 of 32). Twelve of the participating officers (∼ 37%) volunteered to take the CIT Training prior to it becoming mandatory, and nine officers (28%) were CIT designated officers.
Findings
The CIT pre- and post-test data indicate that the CIT Training had a positive impact on officers’ perceptions of the utility of the training as well as its efficacy. For example, 87% (281 of 323 officers) reportedly thought the CIT Training was “useful.” Officers also reported learning quite a bit during the training. On the post-test, officers were asked: “On a scale of one to ten [with one representing ‘nothing’ and 10 representing ‘a lot’], how much did you learn during the CIT Training that you did not know before?” The mean among the 311 officers who answered the question was 6.48 (range 1 to 10), with a standard deviation (SD) of 1.979. The standard deviation indicates that 75% of responding officers marked between 4.501 and 8.459. Most officers, then, conveyed that they learned a substantial amount of new information during the CIT Training that they did not know before completing the training. Only two officers, or 0.6%, reported that they learned “nothing” during the training.
As stated above, there were three outcome measures on the CIT pre- and post-test: (a) general perceptions of emotionally disturbed persons, (b) perceptions of the dangerousness of emotionally disturbed persons, and (c) perceptions of preparedness to handle encounters with emotionally disturbed persons. Difference of means testing (paired samples t-tests) was used to determine whether there were statistically significant differences in mean scores from the pre-test to the post-test for each of the three outcome measures. Again, “emotionally disturbed person” was operationalized as, “a person exhibiting indicators of a mental health issue/crisis and/or emotional impairment (e.g., impairment due to drugs, alcohol, medical condition, etc.) that is affecting behavior” (explicitly specified on the pre- and post-test instruments).
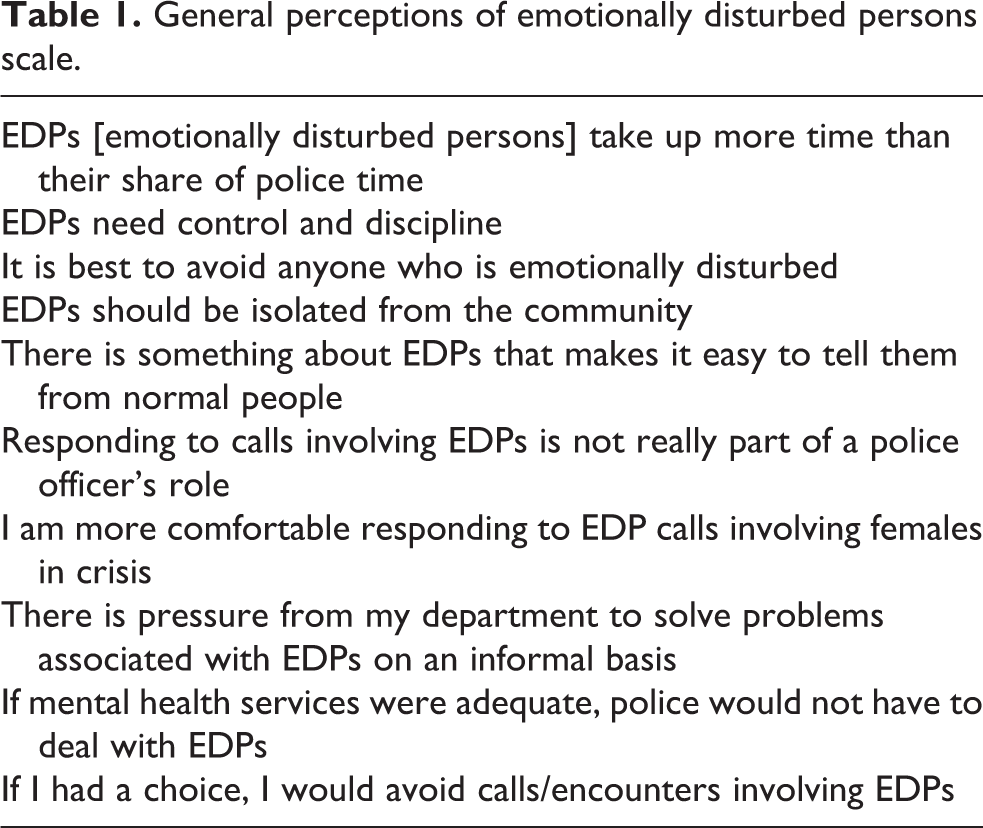
The general perceptions of emotionally disturbed persons scale was comprised of eight items; Cronbach’s alpha reliability coefficient was .736 for the pre-test and .757 for the post-test (Table 1). There were no statistically significant differences between officers’ general perceptions of emotionally disturbed persons from the pre-test (M=2.1838) to the post-test (M=2.1570).
General perceptions of emotionally disturbed persons scale.
The perceptions of the dangerousness of emotionally disturbed persons scale was comprised of seven items; Cronbach’s alpha reliability coefficient was .640 for the pre-test and .702 for the post-test (Table 2). The mean difference in officers’ perceptions of dangerousness of emotionally disturbed persons from the pre-test (M=2.5806) to the post-test (M=2.3523) was statistically significant (t 310=10.534; p<.001). Statistical significance indicates that officers perceived emotionally disturbed persons to be less dangerous after the CIT Training.
Perceptions of the dangerousness of emotionally disturbed persons scale.
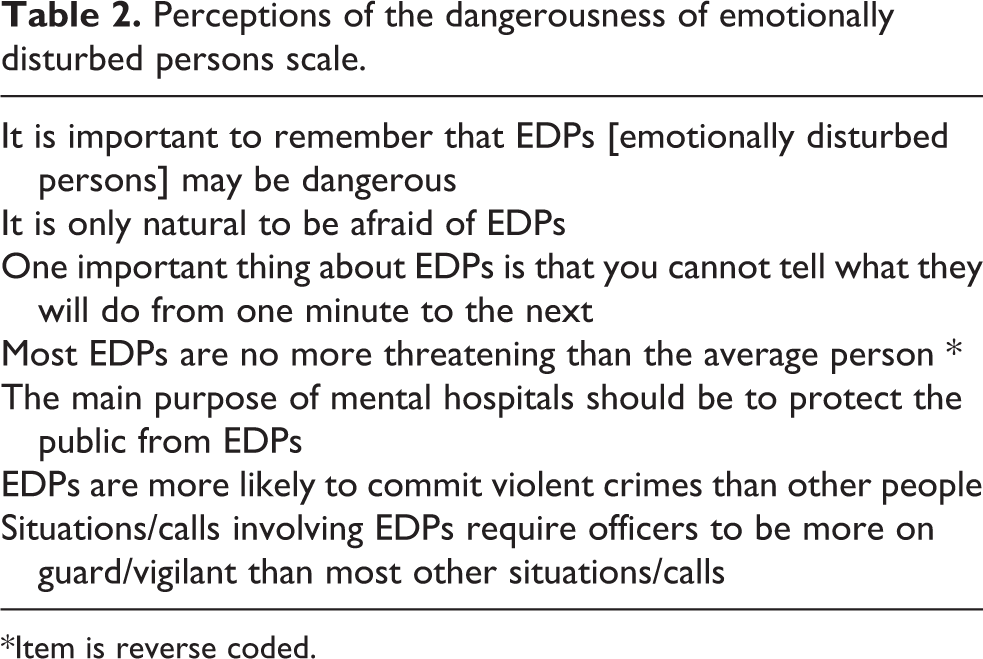
*Item is reverse coded.
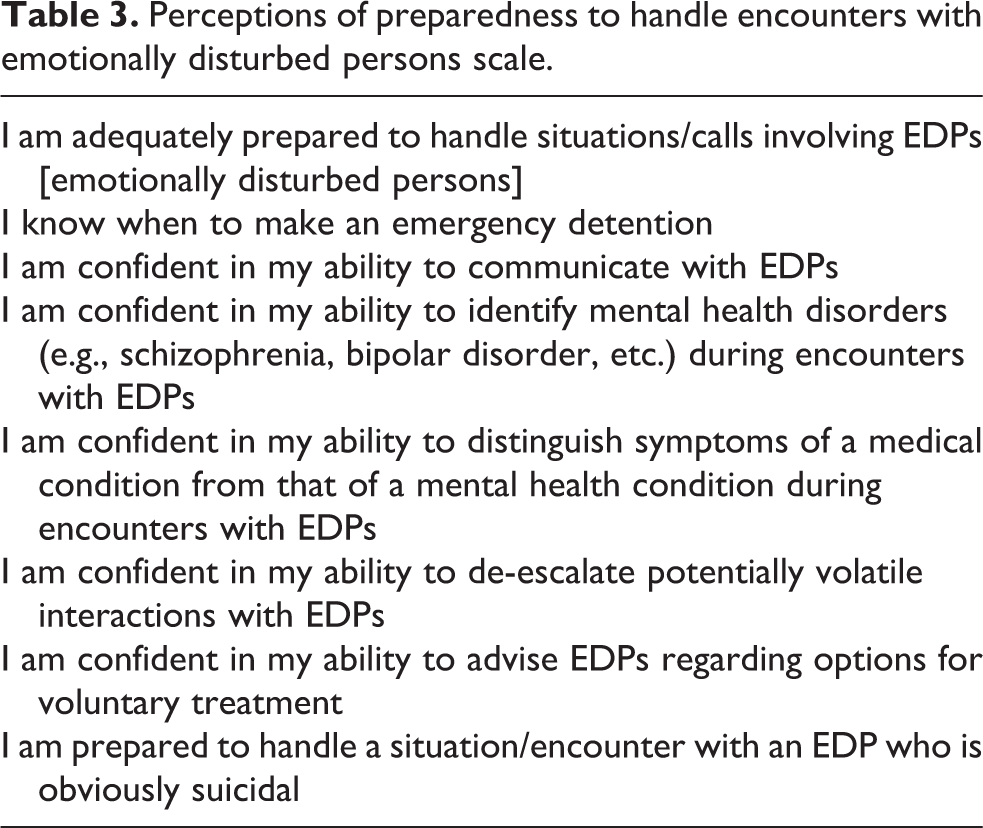
The perceptions of preparedness to handle encounters with emotionally disturbed persons was comprised of eight items; Cronbach’s alpha reliability coefficient was .856 for the pre-test and .885 for the post-test (Table 3). The mean difference in officers’ perceptions of preparedness to deal with emotionally disturbed persons from the pre-test (M=2.8351) to the post-test (M=3.0335) was statistically significant (t 309=−9.177; p<.001). Statistical significance indicates that officers perceived themselves to be better prepared to deal with emotionally disturbed persons after the training.
Perceptions of preparedness to handle encounters with emotionally disturbed persons scale.
Overall, these findings are positive. Quantitative analysis of the immediate impact of the CIT Training revealed that the training improved measures of officers’ perceptions of the dangerousness of emotionally disturbed persons as well as their perceived preparedness to handle encounters with emotionally disturbed persons. Additionally, most of the participating officers reported that the training was “useful” and that they had learned a lot that they did not know prior to the training.
During participant observation, officers were observed interacting with members of the public, including persons with mental illness and/or emotional/behavioral issues. Most officers, understanding the nature of the data collection effort, requested that UPD communications personnel dispatch them to respond to the Mental Observation (MO) calls when possible, so that the nature of these types of interactions could be observed. Most of the observed calls that involved persons with mental illness and/or emotional/behavioral issues were not actually dispatched as MO calls. These calls were coded by dispatch in a variety of ways, and officers had no forewarning that the subjects of these calls were mentally ill and/or emotionally disturbed. Calls involving emergency detentions were oftentimes complex, as well as labor and time intensive, typically involving multiple officers and, sometimes, spanning two to three police shifts. There were two observed instances where officers would have been justified in using lethal levels of force but did not; there were also two instances where officers were injured, requiring emergency room treatment.
Given this complex and multifaceted context of policing persons in crisis, the primary goal of the CIT Training was to improve street-level interactions with persons with mental illness and/or emotional/behavioral issues. In order to gauge street-level impact, officers were asked whether they had changed anything as a result of the CIT Training. In response to that question, 78% (25 of 32) of the participating officers said they changed how they deal with persons with mental illness and/or emotional/behavioral issues as a result of the training. More specifically, most of the officers explained that they have changed the way they approach and engage persons experiencing mental health crises, and believe themselves better able to de-escalate situations.
Many of the officers discussed changes in the manner in which they speak to persons with mental illness and/or emotional//behavioral issues, explaining that effective communication is key. One officer summed up his thoughts regarding engaging people, “You can deal with 95% of all issues by talking.” Another officer simply replied, “Talk so you don’t need to act.” Officers explained that these changes were primarily due to a better understanding of mental illness and/or emotional/behavioral issues. As some officers imparted: Be empathetic instead of sympathetic. For example, going from “I’m sorry you feel that way” to “I can see where that would cause you stress and grief.” Show empathy instead of sympathy. Thoroughly investigate these calls. An ED [emergency detention] is used as a last option. Try to make it voluntary instead of ED. [I am a] better talker, better listener, and more patient. Calls take more time now. Put yourself in their shoes for a minute. Let them talk. Don’t be judgmental. If they’re angry, let them yell a bit. Police are there as a resource, not there to arrest them. We are trying to help and guide them in the right direction. [The CIT Training] made me a better listener and a better talker. Helped me be more patient. There are times when you have to act and use force for their safety, but you use the least amount of force necessary to take them into custody. [I use] more of a personal aspect. [I have a] better understanding of what a person goes through in a crisis. I use more of a personal touch, more sympathetic, better idea of where they are coming from. [The training] changed my thinking, more empathetic. Now I put in that little extra effort in verbal discussion before going hands on. More of a personal touch, understanding them more. I learned techniques. I knew them before, but I was better when I got out of CIT. I have changed the way I talk to people with MO calls. I recognize the signs of different disorders, different medications, [and] interactions to meds. Before I just took people to [the psychiatric emergency room]. Now I investigate what is actually going on…. [I am] more confident and knowledgeable. I can figure out what the person needs. I talk more, engage them. Talk softly. It’s no big deal. Can now go directly to the problem. I used to go directly to the callers. Now I go to the person who needs help. I build rapport right away. Then go to the caller. They [persons in crisis] are the ones in need. The caller does not need us.
Historically, officers explained, patrol officers would take every person who presented with indicators of mental health issues to the psychiatric emergency room on an emergency detention. The training sought to change this practice, and, in fact, according to participating officers, it did. As officers explained: I do fewer EDs and more voluntary transports. I am more understanding. Try to figure out what is really going on. Family problems? Drugs? Alcohol? I have changed the way I talk with them. [Mental health consumers] just want people to listen. They want to vent a little. Keep eye contact, listen, let them know you are there to help out and not just go to the next call. The big change is that I stopped ED’ing everybody and now get people to go voluntary.
Officers expressed support for assisting consumers with seeking voluntary treatment; the issue is whether they are able to persuade the consumer to seek voluntary treatment. In cases where the consumer does not meet the legal requirements for an emergency detention and the officer cannot convince the consumer to seek voluntary treatment, the officer has no other option but to clear the call and go back into service. When this occurs, officers expressed concern regarding potential consequences. Constant in their thinking: “What happens if I don’t do an emergency detention and something bad happens?” In these cases, almost every officer expressed hyperawareness of the potential for a catastrophic outcome if the consumer did not want to seek voluntary treatment and was left to their own devices. They detailed their apprehension regarding not taking persons in crisis into custody on emergency detentions: Police officers have different rules and [regulations] than doctors at [psychiatric emergency room]. They stressed voluntary admission. Per [UPD] rules, an ED is a physical hold. If there is a problem, we are at fault. Police get blamed.…[The psychiatric emergency room] is a revolving door. The liability and blame is on police. If voluntary, and they leave the hospital, then something bad happens, [it is] on police, a police liability issue. Back in the day, anybody who said they wanted to kill themselves, officers did [an emergency detention form]. Now the training teaches officers to do voluntary. The issue is what if they leave and something bad happens? We saw how it was before. Regularly ED’ing was simpler back then. Now you have to ask yourself, ‘Do I put my neck out there and get in trouble if I don’t ED [and something bad happens]? It is tough for officers to decide whether to ED. You are on the hook if something bad happens later. Police ED to cover themselves.
Overall, the data indicate that the CIT Training was effective in producing street-level changes to improve the delivery of police services to persons with mental illness and/or emotional/behavioral issues. The training improved participating officers’ perceptions of the dangerousness of emotionally disturbed persons and officers’ perceptions of preparedness to handle situations involving emotionally disturbed persons. A large majority of participating officers thought the CIT Training was useful. Officers reported having a better understanding of mental illness and the impact of mental illness. This understanding, officers relayed, has changed the manner in which they approach and engage persons with mental illness and/or emotional/behavioral issues. Officers are also transporting more persons in crises for voluntary treatment versus taking persons into custody for purposes of involuntary treatment/emergency detention.
Discussion and conclusions
In 2014, following a major critical incident in which a police officer used lethal force against a person with serious untreated mental illness who became violent and combative, the Urbantown mayor and police chief jointly decided to mandate the 40-hour CIT Training for all police officers. The training started in 2015; UPD initiated an assessment of the CIT Training in late 2016. Overall, the results of the assessment are positive. The data indicate that the CIT Training had an immediate influence on officers’ perceptions of the dangerousness of emotionally disturbed persons and their preparedness to handle encounters with emotionally disturbed persons. The data also uncover street-level changes in participating officers’ methods for engaging and interacting with persons with mental illness and/or emotional/behavioral issues. Officers reported having a better understanding of persons with mental illness and/or emotional/behavioral issues. The knowledge and understanding imparted during the training has made officers more adept at communicating with persons in crises; officers conveyed that they are better listeners and more patient during these types of interactions and encounters than they were prior to the completion of the CIT Training. Officers expressed that by being able to listen and talk to persons with mental illness and/or emotional/behavioral issues who may be in crisis, they can de-escalate the majority of potentially volatile encounters and interactions.
Officers also expressed changes in the rate of emergency detentions. The officers explained that they make fewer emergency detentions, and are better able to persuade consumers to seek voluntary treatment; officers will even transport persons for the purposes of voluntary treatment. Given the high rate of emergency detentions in Urbantown, this change represents a significant and positive impact of the CIT Training. This conclusion is important for other reasons as well. The primary intended effects of reducing the rate of emergency detentions are clear, and include potentially reducing dependency on limited county-level, public mental health resources; improving assessment and treatment plans for consumers in need (to reduce frequent utilization); and producing more positive outcomes during police–consumer interactions and encounters.
As is well established (principal rationale for CIT Training), interacting with police in an official capacity, including being taken into custody involuntarily, can be a traumatic experience, sometimes evoking aggressive and violent self-protective and/or assaultive behaviors (Compton et al., 2000, 2008, 2011; Finn and Stalans, 2002; Hirschel et al., 1994; Jaffe, 2017; Joyal et al., 2007; Link et al., 1992; Watson and Fulambarker, 2012). Violent and aggressive reactions to police can escalate into catastrophic events, forever impacting those involved, including the officers (Finn and Stalans, 2002; Jaffe, 2017; Nix et al., 2017; National Law Enforcement Officers Memorial Fund Fatalities Report, 2016; Shucard et al., 2012). The impact and consequences of these encounters and interactions, however, extend beyond just the individuals involved.
State legal requirements for taking a person into custody involuntarily for purposes of mental health treatment vary. In the state where Urbantown is located, the legal requirements for emergency detentions is restrictive. Police are essentially limited to persons who are, at the time of police involvement, experiencing and/or exhibiting indicators of homicidal ideation, suicidal ideation and/or the inability to care for one’s own basic needs. This statutory constraint sometimes leaves officers without the formal capacity to help persons they believe to be in need, yet who do not meet the explicit criteria for emergency detention.
This restriction is a concern for officers in Urbantown. Every officer expressed awareness (many hyperawareness) that if something goes wrong during an interaction/encounter with a person with mental illness and/or emotional/behavioral issues, they will face public and administrative (and potentially legal) backlash. At the same time, every officer expressed the same awareness (and hyperawareness) that they would suffer identical consequences if something bad happened after an encounter/interaction with a person with mental illness and/or emotional/behavioral issues who was not taken into custody for purposes of involuntary treatment. The legal constraints in these types of encounters/interactions, given the current national public discourse and sentiment regarding police, leaves officers feeling vulnerable and exposed. Essentially, to them, it is a realism that they may be “damned if you do, damned if you don’t.”
While all officers expressed genuine concern for consumers in need/crisis, they simultaneously conveyed unease and/or anxiety over the potential impact their decision-making—including not making an emergency detention—can have on their professional and personal lives. The unease and anxiety in this context is chronic, given their current reality. The police chief terminated the officer involved in the major critical incident that precipitated the mandatory CIT Training. Not only did the officer lose his job, he spent almost a year awaiting the results of the district attorney’s investigation into whether he would be criminally charged and received hurtful public criticism as well as harmful threats to his and his family’s safety.
This constraint can also tax already limited police resources, as officers are forced to repeatedly interact with what they term “frequent utilizers” (persons with mental illness and/or emotional/behavioral issues who form the basis for frequent 911 calls for police service). In these cases, officers respond to multiple and/or frequent 911 calls regarding the same person without any formal recourse for addressing the underlying issue. Again, if the consumer does not meet the requirements for emergency detention and refuses transport for voluntary treatment, the officer has no other option, except to continually respond to calls for service involving the same person when dispatched to do so. Moreover, in the major critical incident that precipitated the CIT Training mandate, telecommunications personnel received multiple calls for service during the same shift regarding the same person who was simply sleeping on a park bench. These calls all involved police interactions with a person suffering from an untreated serious mental illness, who, we later learned, believed someone was trying to kill him. It was the third police response that resulted in tragedy.
At the same time, the statutory restrictiveness regarding emergency detention is centered on the protection of civil liberties, along with the fundamental rights of persons with mental illness (in the same way that laws protect persons with limited physical capacity and mobility). Making an unjustified and inappropriate (illegal) emergency detention is a civil rights infringement. It is also a risk management matter, as there could, in fact, be legal consequences when police officers make unjustified and inappropriate emergency detentions. This is not only potentially a civil liability issue, but there are serious implications regarding police legitimacy, as the perception of procedural fairness is the primary antecedent for police legitimacy and why people obey the law (Lind and Tyler, 1988; Tyler, 1990, 2001; Tyler and Fagan, 2008). In essence, unjustified and inappropriate use of emergency detention not only encroaches on the rights of consumers and puts the agency at risk for civil liability, but it also jeopardizes the very foundation of policing a free society: voluntary compliance via police legitimacy.
Recommendations
Based upon this assessment, it is recommended that other large municipal police departments give serious consideration to making the CIT Training a requirement for all line-level officers, sergeants and lieutenants. Also that line-level officers, sergeants and lieutenants complete an 8-hour crisis-oriented in-service training biennially. Policing persons with mental illness will continue to be a pressing issue for police executives and administrators, as scholars project that police interactions and encounters with persons with mental illness and/or emotional/behavioral issues will become more frequent, given declining budgets and local mental health system deficiencies (Finn and Stalans, 2002; Green, 1997; Jaffe, 2009, Livingston et al., 2014). Furthermore, the benefits of CIT Training extend beyond just encounters and interactions with persons in crisis; the skills and techniques learned in CIT Training will assist officers in all of their calls for service and encounters/interactions.
The nature of police–citizen encounters/interactions, in general, has become increasingly convoluted and hot-tempered (Comey, 2015; MacDonald, 2016; Nix et al., 2018). There are growing levels of public noncompliance, largely as a result of isolated incidents of police misconduct and negative public discourse (MacDonald, 2016; Morin et al., 2017; Nix et al., 2018; The Ferguson Effect, 2016). There is also more hostile public scrutiny of police behavior, a heightened focus on police accountability, and growing utilization of civil liability (Nix et al., 2018). The context in which contemporary police officers navigate and operate is growing progressively more complex and antagonistic.
Police officers are already aware of the antagonistic public scrutiny and potentially severe consequences that accompany the decisions they make on the job (Comey, 2015; Morgan and Pally, 2016; Nix et al., 2018). Inadequate training, preparation and administrative support exacerbates the already challenging function of policing a free society (Police Executive Research Forum, 2016; Wolfe and Nix, 2016). Without adequate administrative support and preparation, the ultimate result may be disengagement and absolute avoidance, the effects of which have already been modeled (Comey, 2015; Morgan and Pally, 2016; Morin et al., 2017; Nix et al., 2018; Sutton, 2015; The Ferguson Effect, 2016).
Interactions and encounters with persons with mental illness and/or emotional/behavioral issues who find themselves in crisis are even more difficult and stressful, and oftentimes unpredictable and dangerous. Essentially, police officers are trying to communicate and negotiate with persons who are not fully rational and in varying states of crisis; if struggling with untreated severe mental illness, these persons may literally be psychotic and/or hallucinogenic (situational effects of some serious mental illnesses). In some cases, these same persons may also be armed and/or primed for violent action and/or reaction.
Learning the skills and knowledge to be able to engage all persons, including those in crisis, while concomitantly de-escalating potentially precarious and aggressive encounters/interactions is paramount to officers’ abilities to perform their jobs. These skills and techniques are central features of CIT Training. For those officers who routinely interact with persons with mental illness and/or emotional/behavioral issues, these skills and techniques could literally be the difference between life and death.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.