
Abstract
Probation and parole research in the late 1980s and early 1990s explored the negative health and wellness effects that officers may experience. However, little current research exists on health and wellness outcomes for probation and parole officers. Furthermore, little research has been conducted on the factors that may predict health and wellness for probation and parole officers. This study provides survey results of 342 probation and parole officers working for one probation and parole department in a southern U.S. state. Binary logistic regression results reveal officer age and tobacco use are significant predictors of officer injury. Moreover, sex, alcohol use, fast food consumption, sleep, and feeling in control of one’s job are significant predictors of self-reported officer depression. Policy implications for the above-mentioned findings and future directions for research are also discussed.
Introduction
The overall health and wellness of criminal justice practitioners has been the focus of scholars for approximately 30 years (Cullen, Link, Wolfe, & Frank, 1985; Lambert & Paoline, 2008; Stevens, 2008). Research has identified substantial role issues and conflicts inherent within key criminal justice actor’s positions in the duties required of their job. For example, the roles of police officer and correctional officer, respectively, have shown to be rife with issues that impact both their professional and personal lives. Most notably, these roles have been shown to suffer from substantial stress, which can lead to poor health, high divorce rates, job burnout, and other significant professional and personal issues (McCoy & Aamodt, 2010; Mumford, Taylor, & Kubu, 2015). These role issues ultimately tend to impact general recruitment and retention of these positions, placing further burdens upon criminal justice agencies and administrators in attempting to recruit and retain personnel (McCarty, Zhao, & Garland, 2007).
Despite the strong focus on the overall health and wellness of important criminal justice positions, community correctional officers have seldom been the focus of such research. Specifically, examination into important health habits of community correctional officers, such as diets, tobacco/alcohol use, exercise, and sleep have been largely neglected. Charged with supervising nearly 4,500,000 of the 6,613,500 individuals believed to be under some form of correctional supervision currently in the United States (Kaeble & Cowhig, 2018), high caseloads (DeMichele & Payne, 2007), and the supervision of a variety of special offender populations (e.g., sex offenders, mentally ill, etc.), community correctional officers have been found to face many of the same issues as law enforcement and correctional officers (Slate, Wells, & Johnson, 2003). Although recent statistics suggest a slight decrease in the number of individuals under community supervision, more than 90,000 estimated officers are still responsible for supervising nearly 70% of the current correctional population in the United States (American Probation and Parole Association, n.d.; Kaeble, 2018). It is imperative that continued research examine the overall health/wellness of these practitioners.
The current study attempts to ascertain what individual qualities might be differential predictors for work-related and health/wellness issues suffered by probation/parole officers. Specifically, the present study has two primary goals. First, what demographic, physical, substance use, health, and job characteristics lead to varying levels of likelihood in the receipt of an injury while on the job? Second, what demographic, physical, substance use, health, and job characteristic factors lead to the likelihood of experiencing self-reported depression? Policy implications and future directions for research will also be discussed.
Literature Review
Substantial research has been conducted on the overall health and wellness of law enforcement officers and correctional officers. However, fewer studies have focused on the health/wellness of probation/parole officers. Most prior research related to community correctional officer well-being has been on workplace injuries.
Injuries
Injuries related to one’s position in a law enforcement setting have been the subject of research for decades. In some situations, law enforcement officers succumb to fatal occupational injuries while on duty. For example, Tiesman, Hendricks, Bell, and Armandus (2010) found that for the years 1992-2002, there were 2,280 law enforcement officers who suffered a fatal occupational injury with 36% (n = 815) from homicide and 5% (n = 122) from suicide. The prevalence rates of officer injuries are also alarming. Specifically, the rate of 635 injuries per 10,000 full-time employees from 2003 to 2014 was 3 times worse than other full-time U.S. workers in other occupational fields (Tiesman, Gwilliam, Konda, Rojek, & Marsh, 2018). Law enforcement officer injuries also vary as a product of demographic factors. For example, female officers have been found to have higher rates of injury (Boyce, Hiatt, & Jones, 1992) and older officers are more likely to experience injury (Knapik et al., 2011).
Correctional officers have also been documented to have a multitude of work-related fatal and nonfatal injuries. Some of the most recent estimates place correctional officers as having experienced 544 work-related injuries or illnesses serious enough to require medical attention per 10,000 full-time employees (Harrell, 2011). Most injuries are found to have occurred when correctional officers search for contraband, inform offenders to relocate, or when conducting routine inmate searches (Light, 1991).
Current numbers regarding instances of community correctional officer injuries are lacking. Some of the more comprehensive reports are now several decades old. Between 1980 and 1993, the Federal Probation and Pretrial Officers Association conducted a study on all state and federal U.S. territorial jurisdictions where it found 1,818 reported serious physical attacks and 792 attempted assaults against officers (Bigger, 1993). A more recent study by the U.S. Department of Justice of four states found that between 39% and 55% of community corrections officers had been violently assaulted (Gonzales, Schofeild, & Hart, 2005).
Some individual states have examined this issue. For example, a survey of Minnesota community corrections officers discovered that 74% of them had been verbally or physically threatened while 19% had been physically assaulted at some point in their career (Arola & Lawrence, 1999). Other studies have found the percentage of probation/parole officers intimidated, threatened, or assaulted to be closer to 40% (Parsonage & Bushey, 1987) with most of these threats and injuries believed to occur in the office (Rapp-Paglicci, 2004). Thus, the contextual nature of community correctional officer jobs is in contrast to that of law enforcement and institutional correctional officers. Drawing upon related law enforcement occupations may lend a better understanding to what issues might impact community correctional officer health. These identified correlates can be largely categorized as demographic factors, health habits, alcohol use, and largely stress-induced mental health issues.
Identified Factors Related to Injuries and Mental/Physical Health Issues
Demographic factors
The field of criminal justice is predominately male, especially law enforcement officers. However, according to the Bureau of Labor Statistics (BLS; 2019), 63.5% of all probation and parole officers are female. This is in stark contrast to the Federal Bureau of Investigation’s (FBI; 2013) data that show the number of females as less than 12% of police community. Women as law enforcement or probation/parole officers have been known to be able to neutralize dangerous situations without use of physical force as they are intrinsically able to facilitate trust and cooperation, a key to building relationships with offenders on probation/parole (Lonsway, Moore, Harrington, Smeal, & Spillar, 2003).
Similar to law enforcement officers, probation/parole officers are mostly Caucasian at 63.8% according to BLS (2019). Furthermore, just like the law enforcement officers, Caucasian probation and parole officers are not wholly representative of offenders in the criminal justice system. This disproportionation can result in difficulty for the officer’s ability to relate to offenders of different races/ethnicities (Theobald & Haider-Markel, 2008).
For age, older officers have been found to be more likely to experience depression (Darensburg et al., 2006). Other demographic factors, such as marital status, have been found to not be significant predictors of officer stress (Armstrong, Atkin-Plunk, & Wells, 2015). Despite this, some research fails to show a significant relationship between individual demographic factors (e.g., age) and shows more support for the occupational/contextual factors on stress (Getahun, Sims, & Hummer, 2008). Officer health habits have also been identified as important.
Health habits
Although most of the issues that cause stress and health problems within officer roles are inherent in the modern function of their position, prior research has identified ways to reduce some of these negative health effects. Oftentimes, prior literature has pointed to stress reeducation as the primary mechanism for reducing any negative effects (Finn & Kuck, 2005) with exercise as one of the more frequently cited, and more realistic, ways to mitigate these health issues compared with addressing deeper organizational/role issues (Gerber, Kellman, Hartmann, & Pühse, 2010). Recommended comprehensive health programs that provide information on diets, stress reduction techniques, and exercise education have shown a positive health effect for officers who participate (Kuhns, Maguire, & Leach, 2015). Although some research has focused on positive health habits, most have focused on negative maladaptive coping strategies, such as alcohol consumption.
Alcohol use
There have been numerous works that have suggested a causal connection between the stress associated with law enforcement and alcohol use as a coping mechanism (see Swatt, Gibson, & Piquero, 2007). For example, one study by Kirschman (2006) found that police officers consume alcohol more than double the rate of the general population. Alcohol use as a maladaptive coping mechanism has also been found among correctional officers (Cheek, 1983). A recent comparison between police officers and other individuals in protective service positions (PSOs; for example, correctional officers, firefighters, etc.) found that individuals in PSOs did not consume alcohol more frequently, nor did these individuals have higher likelihoods of alcohol dependence (Weir, Stewart, & Morris, 2012). Despite this, individuals in PSOs did report a greater likelihood of binge-drinking when compared with non-PSOs with being male, single, and suffering from psychological issues were found to be related to greater alcohol dependency (Weir et al., 2012). Similar in position to police officers and institutional correctional officers, it would be reasonable to assume that community correctional officers might also cope with stressors by using alcohol.
Stress-induced mental/physical health issues
Officer role-induced stress has multiple negative health effects for individual officers. As such, this has been the subject of much criminal justice research for law enforcement (see Mumford et al., 2015) and institutional correctional officers (see Lambert, Hogan, Paoline, & Clarke, 2005). Results largely suggest stress is built into the individual roles they occupy.
For law enforcement, officers deal with a variety of stressors. These categories of stresses are typically organized into (a) work-related factors and (b) individual-related factors. Work-related factors include poor management, lack of resources for equipment, excessive overtime, shift-work, and frequent duty changes. Individual factors include family problems, financial issues, health concerns, additional employment, officer fatigue, various health/wellness issues, and poor job performance (Fiedler, 2011; National Institute of Justice, 2012).
For institutional correctional officers, overall exposure to the conditions found within their position has also been identified to lead to a number of psychological disorders with stress oftentimes cited as the underlying cause. For example, multiple recent studies have found between 22% and 35% of their sampled correctional officers reported high levels of stress (Lambert et al., 2005; Management and Training Corporation, 2011). Continued stress can lead to a multitude of work-related issues, including, but not limited to, decreased commitment/involvement to their position (Lambert, Hogan, & Barton, 2004), burnout (Lambert et al., 2005), and turnover intentions (Patenuade, 2001). Stack and Tsoudis (1997) even found that correctional officers had a 39% higher suicide rate than the general working age population. Although community correctional officer roles are similar to law enforcement and institutional correctional officers, there are some important contextual differences inherent within their position.
Community corrections officers interact with offenders in the community, not in a secure facility. This social aspect opens the possibility that situations can become unpredictable and even life-threatening (Finn & Kuck, 2005). Similar to law enforcement and institutional corrections, occupational stress has been indirectly linked to a probation officer’s intentions to quit their job (Simmons, Cochran, & Blount, 1997). According to Slate and Johnson (2013), there are four realms of stress that community correctional face. These realms are the (a) public and those in the community, (b) internal stress of community correctional organizations, (c) external stress associated with the criminal justice system, and the (d) stress of their personal life. The particulars of these stressors often require officers to reduce the amount of time they spend with each offender due to their ever-increasing caseloads (Salyers, Hood, Schwartz, Alexander, & Aalsma, 2015). Some of these cases involve violent offenders, attempted suicides, and threats/assaults (Lewis, Lewis, & Garby, 2013). Probation/parole officers are often given the additional duties/role of law enforcement officer or social worker, placing further strains on them personally and professionally (Slate et al., 2003). Severson and Pettus-Davis (2013) referred to the social work role given to probation and parole officers as secondary trauma. That is, these officers are exposed to their clients recounting prior traumatic experiences.
Individual caseloads can also impact an overall correctional officers’ well-being. For example, Lewis et al. (2013) found that officers supervising violent and sex offenders experienced more traumatic stress and burnout. It is the underlying issue of stress that has been pointed to causing or worsening preexisting depression among officers (Gayman & Bradley, 2013). An ethnography on probation officers who work with high-risk offenders found that officers sometimes reported feelings of anger, depression, exhaustion at work, and general frustration (White, Gasperin, Nystrom, Ambrose, & Esarey, 2005). Rebman (2003) found that symptoms of depression among probation officers oftentimes manifest themselves in the form of restlessness/agitation, fatigue, and sleep difficulties. Depression among community correctional officers can lead to serious secondary effects, such as difficulties with the cardiometabolic system and respiratory function that can increase obesity, arthritis, and gastrointestinal issues (Kessler et al., 2008). Ramifications from such health issues can lead to increased job turnover or even death.
Job turnover has been linked to an increase in a number of important issues detrimental to the overall function of community correctional organizations. In fact, these identified issues include, but are not limited to, recruiting and job training costs, unidentified violations/recidivism, and higher caseloads for the other officers still working for the department (Lee, Joo, & Johnson, 2009; Simmons et al., 1997). Ultimately, these issues can compound, ultimately leading to general departmental performance issues (Lee et al., 2009). These issues do not appear to dissipate over time as Wirkus (2015) discovered that probation officers with more experience (26 or more years of service) felt almost 40% more stress than those officers who had less experience (14 years or less). Finally, the occupational stressors that are attributed to working as a probation/parole officer can also affect their home life. Further examination can lead to discovering potential ways to mitigate or eliminate potential stressors while simultaneously increasing productivity, safety, and the overall quality of life for officers and their respective departments.
The Present Study
Although prior research has examined indicators of increased risk for injuries in the professions of police officer (Stevens, 2008) and correctional officers (Lambert & Paoline, 2008), research has rarely examined factors related to community correctional officer injuries or physical/mental well-being. Examination into this area is crucial, as the overwhelming majority of individuals under correctional supervision are under community correctional supervision (Kaeble, 2018). The current research examines two total research questions. First, what demographic measures, physical health characteristics, and job characteristics lead to varying levels of likelihood in the receipt of an injury on the job? Second, what demographic measures, physical health, and job characteristics factors lead to the likelihood of experiencing self-reported depression? Policy implications and future directions for research will also be discussed.
Method
Data
Data for the current study involve a survey distributed to probation and parole officers employed in a southern state. 1 Probation/parole officers were asked to respond to a variety of demographic, health/wellness, job characteristics, and overall job experience questions. Individuals were asked to respond to a variety of health and wellness questions, as this was originally part of a larger research project comparing the health habits of police officers with community correctional officers. Approval from the respective state’s Department of Corrections (DOC) and the Institutional Review Board (IRB) was received. Data collection took place in fall 2015.
Sample
The total population of probation and parole officers from the respective state was 840. Official email addresses for all 840 probation and parole officers employed were provided by the state DOC. Each probation and parole officer was sent an email with a link to complete a survey via Survey Monkey™. Five days after the original survey requests were emailed, a follow-up attempt was sent to all potential participants. In total, 342 (40.7%) responses were received.
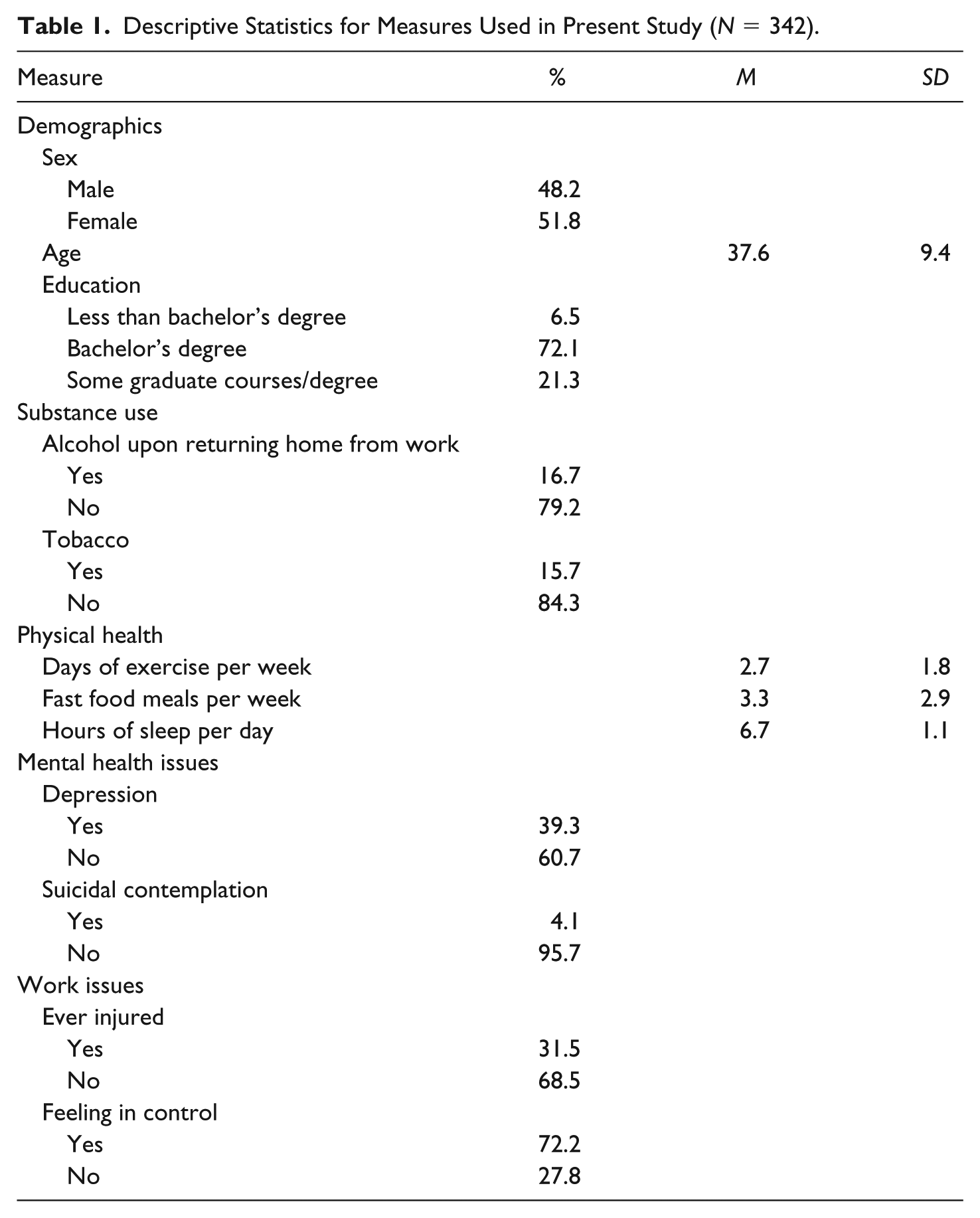
The representation of sex in the sample was fairly even with 51.8% (n = 177) respondents being female and 48.2% (n = 165) being male. The ages of probation and parole officers ranged from 21 to 68 years with a mean of 37.7 years, a mode of 30, and a standard deviation of 9.4 years. The average length of time on the job was 7.8 years. Race/ethnicity and marital status were not collected. 2 The overwhelming majority of participants had a minimum of a bachelor’s degree at 71.6% with a substantial minority either being enrolled in graduate courses (10.2%; n = 35) or having completed a graduate degree (11.1%; n = 38). Despite the individual DOC’s policy of requiring a minimum of a bachelor’s degree, 2.6% (n = 9) reported their highest education as a high school diploma, 2.3% (n = 8) reported some college, and 1.5% (n = 5) had earned an associate’s degree.
Dependent measures
Two different models with two individual dependent measures were used in the analysis: first, whether or not a probation/parole officer was ever injured on the job, and second, whether a probation/parole officer has experienced depression. All measures were self-reported by the individual probation/parole officer.
For the first dependent variable, this was a composite of two total questions in the survey. The first question asked respondents, “Have you ever experienced any of the serious injuries listed below while on the job?” while being given the following options to choose from: broken bone (4%), deep cut or laceration (7%), significant tendon/muscle damage (11%), skin burn (3%), significant head injury/trauma (i.e., concussion) (3%), and other (11%). The second question asked individuals whether they have ever been taken to the emergency room in relation to their job. In total, 13% of respondents reported having been hospitalized for an “on-the-job” injury. These two variables were combined to measure whether any individual had ever (a) received any form of injury while on the job or (b) had ever been taken to the emergency room for an injury sustained while on the job. If respondents had met either of the aforementioned criteria, they were dichotomous with injured (coded as 1) and not injured (coded as 0). The majority (68.5%; n = 224) reported never being injured while a sizable minority (31.5%; n = 103) reported being injured at some point while on the job.
The second dependent variable—whether or not a probation/parole officer has experienced depression—was also a dichotomous measure. Specifically, this measure distinguished between probation/parole officers with self-reported depression and those without self-reported depression. Although the majority (60.7%; n = 198) of respondents reported not suffering from depression, nearly half (39.3%; n = 128) of the sample did report suffering from depression. Those reportedly suffering from depression were coded as 1 while those not reportedly suffering from depression were coded as 0. It is also important to note that respondents were asked whether they had ever contemplated suicide since working in community corrections. Only 4.3% (n = 14) stated they had contemplated suicide while 95.7% (n = 310) had not. 3
Independent measures
Independent variables assessed three demographic characteristics, one workplace, and one substance use measure.
Demographic characteristics
There were a total of three demographic characteristics included in the respective models. The first variable of probation/parole officer sex was dichotomized and dummy-coded with females (coded as 0) at 51.8% (n = 177) and males (coded as 1) at 48.2% (n = 165). The second variable of probation/parole officer age was a continuous variable with the average age at 37.7 years, a mode of 30, and a standard deviation of 9.4 years. The third and final demographic measure was probation/parole officer education. As there was little variation between many of the educational categories, the six categories were collapsed into the three of (a) less-than bachelor’s degree (coded as 1), (b) bachelor’s degree (coded as 2), and (c) some graduate courses or completed graduate degree (coded as 3).
Workplace measure
Officers were also asked whether they felt in control of their job through a four-point Likert-type scale ranging from strongly disagree to strongly agree. Due to the lack of variability in responses, the measure was later recoded into a dummy variables with agree/strongly agree responses recoded to feeling in control at their job (coded as 1) and disagree/strongly disagree coded to not feeling in control at their job (coded as 0). Fully 72.2% (n = 234) reported feeling in control of their job while 27.8% (n = 90) reported they did not feel in control at their job.
Substance use measure
There were two substance use measures used in the two models. Respondents were asked whether they typically drink when they get home from work. Fully 16.7% (n = 57) responded yes (coded 1) while 79.2% (n = 271) responded no (coded as 0). Respondents were also asked whether they used tobacco products (e.g., cigarettes, chewing tobacco, etc.). A total of 15.7% (n = 54) responded yes (coded 1) with the majority (84.3%; n = 288) reported no (coded 0).
Physical/mental-health measures
There were a total of three physical health measures and one mental health measure used across the two models. Respondents were asked how many days per a given week they typically exercise. This was a continuous variable ranging from 0 to 7 days with an average of 2.73 days, a mode of 3, and a standard deviation of 1.8 days. Respondents were also asked how many fast food meals they consumed in a typical week. This was also a continuous measure. Responses ranged from 0 to 21 fast food meals consumed per week with a mean of 3.25 meals, a mode of 3, and a standard deviation of 2.87 meals. For the third and final physical health measure, respondents were asked how many hours of sleep they typically receive on a given night. Similar to the two other physical health measures, sleep was also continuous. Responses ranged from three to 10 total hours per night, a mean of 6.7 hours, a mode of 7, and a standard deviation of 1.2 total hours.
For mental health, there was only one measure included for whether probation officers had experienced depression. This is the same measure that was described above that is used for Model 2 as the dependent variable. Descriptive statistics for measures used in all models can be found in Table 1.
Descriptive Statistics for Measures Used in Present Study (N = 342).
Analysis Strategy
Binary logistic regression techniques were utilized to examine which demographic, wellness, and/or job characteristics may differentially predict receipt of injury or self-reported depression. All assumptions for binary logistic regression were satisfied with both dependent variables being dichotomous (Pampel, 2000). Moreover, in binary logistic regression, a linear relationship between the independent variables and dependent variables does not need to be assumed. All measures for both models were well above the acceptable tolerance levels of 0.65 or higher (Menard, 1995; see Tables 2 and 3).
Logistic Regression Model for Predictors of Ever Being Injured (n = 304).
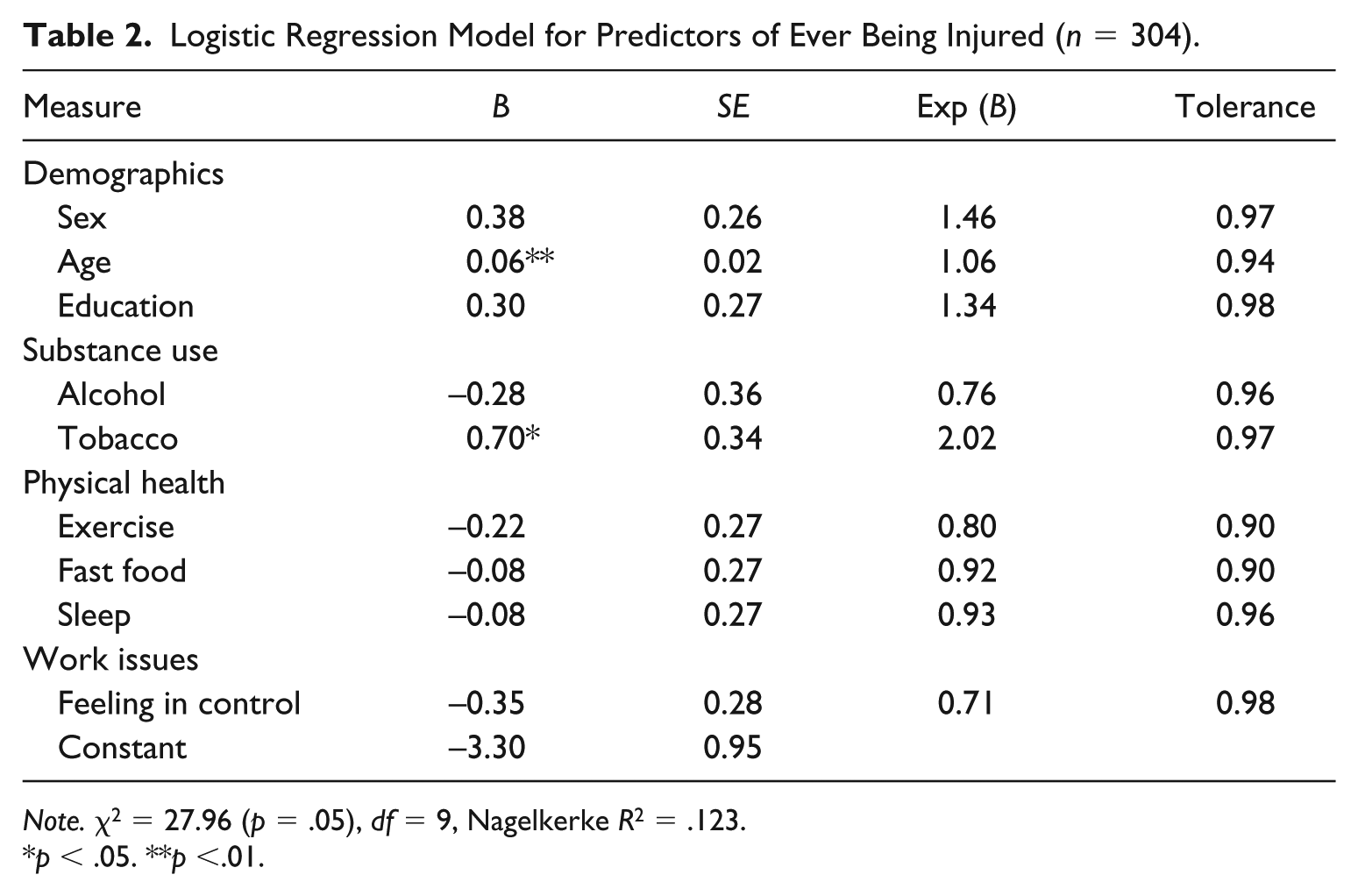
Note. χ2 = 27.96 (p = .05), df = 9, Nagelkerke R2 = .123.
p < .05. **p <.01.
Logistic Regression Model for Predictors of Depression (n = 302).
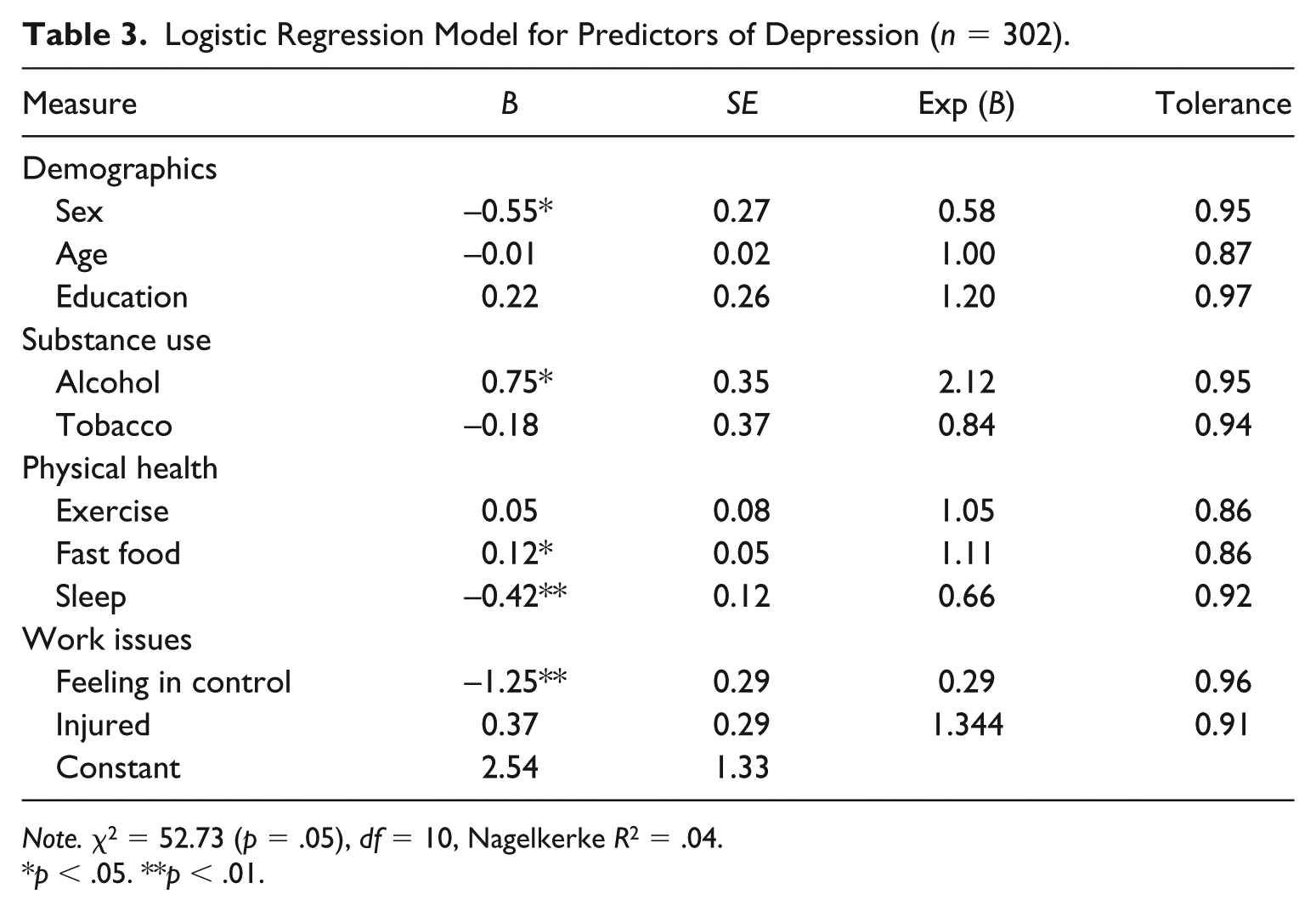
Note. χ2 = 52.73 (p = .05), df = 10, Nagelkerke R2 = .04.
p < .05. **p < .01.
Findings
Table 2 presents the result of the logistic regression analysis for the dependent measure of a probation/parole officer ever being injured on the job. The model is significant with two of the nine measures being statistically significant indicators of having received an injury while on the job. Specifically, age was a significant indicator (p < .01) of receipt of an injury while on the job. As an officer increased in age by 1 year, then their likelihood of having received an injury on the job increased by 6%, Exp(B) = 1.06. The second significant (p < .05) variable was tobacco use. Officers who reported tobacco use in some form had a 102%, Exp(B) = 2.02, greater overall likelihood of being injured on the job when compared with those who did not report using tobacco.
Table 3 presents the findings for the second logistic regression model on whether a probation/parole officer had self-reported depression. This model was also significant with five of the 10 measures being significant indicators of suffering from depression. The first significant (p < .01) measure was sex. Specifically, male officers were found to have a 42%, Exp(B) = 0.58, lower overall likelihood of reporting to have suffered from depression when compared with females. The second significant (p < .05) measure was a substance use measure of alcohol use that found those who typically consume alcohol when they arrive home from work have a 112%, Exp(B) = 2.12, higher overall likelihood of reporting to suffer from depression when compared with those who do not typically drink when they arrive home.
There were two physical health measures significant in this model. These were the measures of fast food consumption (p < .05) and sleep (p < .01). For fast food consumption, every additional fast food meal consumed on a weekly basis results in an 11% higher overall likelihood, Exp(B) = 1.11, of suffering from self-reported depression. For sleep, each additional hour of reported sleep resulted in a 34%, Exp(B) = 0.66, lower overall likelihood of depression. The fifth and final significant measure (p < .01) was whether probation/parole officers felt in control at their job. Specifically, those who felt in control had a 71%, Exp(B) = 0.29, lower overall likelihood of suffering from depression.
Discussion
The purpose of this article was to add to the existing literature on probation and parole officer health and wellness issues. To do this, we examined several demographic, job, and health/wellness factors in an exploratory fashion, which were thought to be predictors of two negative physical and mental health outcomes; those dependent variables were probation and parole officer injury and experiences with depression. By controlling for factors thought to be potential predictors of the dependent variables of interest, the researchers hoped to isolate predictive effects of significant independent variables. Results of logistic regression analyses revealed several significant predictors for the two dependent variables of interest. First, for officer injuries, age and tobacco use were found to be positive significant predictors. Next, officer sex (being male), alcohol consumption, fast food consumption, sleep, and whether officers feel in control of their jobs were identified as significant predictors of officer self-reported depression, with alcohol and fast food consumption showing a positive association and all other significant predictors showing a negative association with officer depression.
For the first model, age demonstrated a positive association with officer injury. This significant positive relationship between officer age and chance of injury is perplexing. On one hand, previous research has shown younger officers experience a greater risk of injury (Kaminski & Sorensen, 1995) and that police officers show physical health deterioration similar to individuals who work in professional occupations compared with those who perform manual labor (Case & Deaton, 2005). That is, officers do not physically decline nearly as much as manual laborers. Less physical deterioration would therefore translate to fewer injuries. This could also simply mean that greater job experience leads to more opportunities to be injured. The cross-sectional nature of these data makes it impossible to disentangle this finding. In addition, older officers experience the natural decline of physical health that comes with age (Burke, 1989). This finding requires more attention in future research utilizing longitudinal data.
The second statistically significant relationship that officer tobacco use is related to being injured could mean that officers who use tobacco are also less likely to take care of their physical health as well as officers who do not use tobacco; officers who are more physically fit are less likely to experience an injury (Quinones, n.d.). Prior studies have also found nicotine in various tobacco products reduce one’s reaction time and decision making (Bates, Pellett, Stough, & Mangan, 1994; Vallath, Joshi, & Vaidya, 2015). Therefore, officers using tobacco products simply might not be able to contain the situation as quickly as their coworkers who do not use tobacco products.
For the second model, being male demonstrated a negative relationship with experiencing depression. This is not surprising, as women, globally, are more likely to experience problems with depression (National Institute of Mental Health, n.d.). Some suggestions for this difference are because men have externalizing symptoms (e.g., losing one’s temper, physical/verbal aggression) and women have internalizing symptoms (e.g., loneliness, anxiety; Albert, 2015). Women have also been shown to have more forms of depression-related issues, such as postmenopausal depression. Simply stated, there are more opportunities for women to seek medical help and identify their depression than men (Albert, 2015). It could also mean that female officers are more open to sharing their mental health issues than their male counterparts due to issues of masculinity and traditional gender norms as has been found with male police exposed to trauma (Pasciak & Kelley, 2013).
Alcohol consumption demonstrated a positive relationship with officer depression and whether officers feel in control of their jobs a negative association with officer depression. The relationship between alcohol consumption and officer depression is certainly not surprising, given prior research. Numerous studies have revealed positive associations between law enforcement alcohol consumption with mental health problems such as depression or post-traumatic stress disorder (PTSD), which largely result from officer stress (Swatt et al., 2007). Thus, it appears that community correctional officers with depression engage in maladaptive coping mechanisms with alcohol as has been found with police and correctional officers (Cheek, 1983; Swatt et al., 2007).
The association between fast food consumption and depression is also not surprising, given that newer research in the physical sciences has also identified such a relationship (Sánchez-Villegas et al., 2012). It is thought that foods high in trans unsaturated fatty acids and cholesterol (as many fast food choices are) are to blame for increased risk of depression, although researchers in the physical sciences are unsure of the specific biological mechanisms in this relationship (Sánchez-Villegas et al., 2012). Officers working long hours might gravitate toward these foods out of convenience, thus increasing their susceptibility to depression.
The negative relationship between sleep and depression is not surprising because there is a well-documented research pattern of an association between depression and sleep, as depression can deprive individuals of sleep (Nutt, Wilson, & Paterson, 2008). Correlations between sleep and mood patterns are difficult to interpret, although they are frequently observed in research, because mood can cause a lack of sleep, or inversely, a lack of sleep can affect one’s mood (National Sleep Foundation, 2019). The relationship between officer depression and officers feeling in control of their jobs is not surprising given previous research has demonstrated an association between officers feeling in control of their jobs and significantly lower chances of experiencing depression (see Copenhaver, 2016). At the same time, research generally shows that depression correlates significantly with occupational stressors of law enforcement (Bhui, Dinos, Stansfeld, & White, 2012).
There are several important policy implications from the findings in this study. First, most of the factors identified as significant predictors of negative physical and mental health outcomes for probation/parole officers mirror findings from much of the health/wellness research on police. Emphasizing the importance of health/wellness for probation/parole officers (e.g., no use of tobacco) deserves the same attention that researchers and practitioners place on the health/wellness training and education of police.
Second, community officers must be educated on the importance of practicing physically healthy lifestyles to protect against the risks associated with aging and working in a law enforcement profession. To accompany such educational training, probation/parole officers must have the risks emphasized of not seeking help for mental health problems. This is especially the case as officers are vulnerable to increased alcohol consumption and problems with depression when they do not feel in control of their jobs. Negative coping mechanisms, such as alcohol consumption, could potentially lead to alcoholism, worsen depression symptoms already present (if applicable), and could even lead to job performance issues. To head-off problems with depression, research should examine what causes their officers to not feel in control of their jobs.
There are several limitations to this study which must be acknowledged. First, the survey used to collect data used in this study was administered to all probation/parole officers in one state. Given that this particular state has fewer metropolitan areas, results may not be generalizable to all probation/parole departments across the United States. In addition, some may consider the study response rate to be low; however, the scope of the survey distribution was quite large, as the probation and parole department operations in the study state spans four regions and is comprised of 20 district offices. Second, race/ethnicity and marital status were not collected. Future research examining these issues should include both measures as prior literature has suggested their importance in occupation-related issues. Examination of this issue in a more racially/ethnically diverse state would also be beneficial to examine any potential differences that may exist.
Third, the depression measure used in this study is a single question measure of the depression construct. Other studies measuring depression use the Beck Depression Inventory (BDI), which contains 21 attitudes and symptoms to assess depression. The researchers elected not to use such an instrument for purposes of this study given the high caseloads of probation and parole officers in the study host state. Future studies may want to consider using a more comprehensive depression measure.
Fourth, the cross-sectional nature of the data could limit full understanding of how these issues develop, especially in relation to depression. Future studies utilizing longitudinal data on probation/parole officer wellness could correct this issue. Fifth and final, the study chose quality over quantity in terms of the survey research strategy. Due to low pseudo-R2 values, this indicates that there is certainly more at play when explaining these key issues than solely health habits of individual officers, such as organizational and role stress (see Wells, Colbert, & Slate, 2006). Because of this, there are several important health- and wellness-related factors (i.e., body mass index, heart rate, cholesterol levels) and organizational issues (i.e., stress), which could have potentially had an impact on the dependent variables of interest. However, these measures were intentionally negated from the study because of the reasons mentioned above.
Despite the above-mentioned limitations, this research study helps to improve our understanding of the factors predictive of negative probation and parole officer health and wellness outcomes. This study showed officer age and tobacco use are associated with officer injury and that officer sex, alcohol use, fast food consumption, sleep, and whether officers feel in control of their jobs are associated with officer depression. In sum, if we want to understand what needs to be done to reduce probation and parole officer experiences with injury and depression, we must first identify factors contributing to these problems. Dealing with the individual health and wellness effects of modern correctional organizational contexts provides a short-term fix on organizational stress effects which would require a larger and more comprehensive overhaul if to be fully and adequately addressed. Continued examination of these issues is vital as community correctional officers will likely assume even more responsibility in coming years.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.