
Abstract
Understanding the determinants and spatial distribution of HIV/AIDS awareness is crucial for effective public health interventions, particularly among women of reproductive age in low-resource settings. This study investigates these factors among women in Somaliland, a region facing unique challenges in health service access. This cross-sectional study utilized data from 6,259 women aged 15–49 from the 2020 Somaliland Demographic and Health Survey. We employed multilevel logistic regression to identify individual and community-level determinants of HIV/AIDS awareness and used spatial analysis to map its geographic distribution. Overall, 73.7% of women in Somaliland reported having heard of HIV/AIDS. Multilevel analysis revealed that awareness was significantly higher among older and more educated women, with those having higher education being 24 times more likely to be aware (adjusted odds ratios [AOR] = 24.04). Conversely, rural (AOR = 0.65), nomadic residence (AOR = 0.33), and no radio exposure (AOR = 0.49) were associated with significantly lower odds of awareness. Significant regional variations were also identified. A substantial portion of the variance in awareness (ICC = 24.3%) was attributable to community-level factors, confirming the appropriateness of the multilevel approach. Women’s awareness of HIV/AIDS in Somaliland is shaped by a complex interplay of spatial location, education, media access, and residence type. These findings underscore the necessity for targeted public health interventions that address both individual and community-level barriers. Priority should be given to reaching women in rural and nomadic settings and those with lower educational attainment. This dual-method analysis provides crucial insights to inform more effective and geographically-tailored HIV prevention programs in Somaliland.
Background
Human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) is a serious public health problem worldwide. HIV/AIDS requires awareness and understanding about the virus, its transmission and prevention strategies in the HIV/AIDS epidemic. 1 Having sufficient awareness about HIV is crucial for achieving Sustainable Development Goal 3, which seeks to “ensure healthy lives and promote well-being for all at all ages,” with specific goals to end the AIDS epidemic by 2030. 2 This is especially significant for women of reproductive age, who are disproportionately affected by the epidemic and often play a key role in family health decisions. 3 Bridging gaps in HIV awareness is vital for enhancing individual health outcomes, identifying risks, minimizing stigma and discrimination, implementing protective action and improving societal well-being as a whole. 4
Globally, more than 38 million people are living with HIV infection 5 and more than half of the people living with HIV are women in sub-Saharan African countries.6,7 In 2021 and 2023, an estimated 650,000 and 630,000 people died from HIV-related causes, and 1.5 million and 1.3 million people were newly acquired HIV infections, respectively 8 and 86% of people living with HIV know their status.8,9 The HIV/AIDS epidemic has had a disproportionate impact on low- and middle-income countries worldwide, with sub-Saharan Africa (SSA) experiencing a significant burden. 1 SSA has the highest number of adolescents living with HIV/AIDS. 10 Eastern and Southern African women face the highest burden of HIV/AIDS and young women are three times more likely than their male counterparts to acquire HIV infection.11–13 Studies in East Africa have demonstrated notable differences in HIV awareness levels, frequently associated with disparities in education, media exposure, and socioeconomic conditions. 14 In the Horn of Africa, including Somaliland, limited research indicates that conflict, displacement, and fragile health infrastructure have historically resulted in lower awareness and increased infection rates, disproportionately affecting women.15,16
Worldwide, the comprehensive knowledge of HIV/AIDS among women in reproductive age is <30%. Comprehensive knowledge is defined as correctly identifying the two major ways of preventing the sexual transmission of HIV (using condoms and limiting sex to one faithful uninfected partner), knowing that a healthy-looking person can have HIV, and rejecting the two most common local misconceptions about HIV transmission.1,17 In SSA (39%), 18 in Ethiopia (14.75%), 19 in Bangladesh (51.6%), 20 in Liberia (33.5%), 7 in Nigeria (46%), 5 in Somalia (67.6%), 21 and in Somaliland (73.7%). 9 Previous studies identified that age, education level, TV, radio, wealth status, type of residence, and region of residence are influenced factors of awareness of HIV/AIDS.18,21–26
In addition, wider societal and structural factors play a key role in influencing women’s understanding of HIV. Social norms and cultural beliefs are important in shaping this awareness, including gender inequality and the stigma surrounding HIV, which can obstruct access to information and health care.27,28 In many regions, the widespread lack of autonomy for women affects their ability to seek information and make decisions regarding their reproductive health. 29 The situation is further aggravated by regional challenges such as conflict, political instability, and the breakdown of health systems. These factors impede public health initiatives and restrict access to HIV prevention and treatment services.16,30 As a result, it is crucial to examine these elements from a multidimensional viewpoint to understand how individual and community factors interact to shape levels of HIV awareness among women in Somaliland.
In Somaliland, patriarchal social structures and traditional norms often limit women’s autonomy in seeking health care and information. Gender inequality manifests in lower literacy rates among women and restricted mobility, which directly impacts their ability to access HIV prevention programs. These cultural barriers, combined with the stigma surrounding reproductive health discussions, create significant hurdles for women in acquiring accurate HIV/AIDS information. 15
To the best of our knowledge, despite the increasing amount of research on HIV awareness, significant gaps remain, especially regarding how geographic location affects it. While studies by Mohamud et al. 21 and Abdikarim et al. 9 identified key demographic factors influencing HIV awareness among women in Somalia and Somaliland, they did not use spatial analysis to examine the geographical disparities that may be impacting awareness within regions. This study aims to fill this gap by exploring the spatial distribution of awareness of HIV/AIDS among women aged 15–49 in Somaliland, using data from the Somaliland Health and Demographic Survey (SLHDS). The research also applies a multilevel analytical approach to gain a more comprehensive understanding of how individual, household, and community factors, alongside spatial location, interact to shape women’s awareness of HIV. By bridging the gap between geography and public health, this study seeks to offer valuable insights that can guide targeted interventions to enhance HIV prevention efforts in Somaliland.
Methods
Study area
This study examined Somaliland, a self-declared republic in the Horn of Africa that remains unrecognized internationally. Somaliland is made up of six administrative regions—Awdal, Maroodi Jeex, Sahil, Togdheer, Sanaag, and Sool—covering an area of 176,120 square kilometers, with an estimated population of 5.7 million as of 2021. One of the primary challenges in Somaliland is the limited access to and availability of health care services, especially in its remote rural regions.
Study design and period
This study used a cross-sectional design, utilizing data from the SLHDS, a national-level survey conducted in 2020. The survey was designed to assess spatial distribution and multilevel analysis of having ever heard of HIV/AIDS among women in Somaliland. However, the data from this survey are used in the current study, focusing on determinants of awareness of HIV/AIDS.
Data source and sampling methodology
The SLHDS used a detailed sampling method to ensure representation across different areas. The six regions of Somaliland were divided into urban, rural, and nomadic areas. In urban and rural areas, computer mapping (GIS) helped select specific areas (enumeration areas or EAs) for the study. Researchers identified 2,806 homes in these areas. For the nomadic population, temporary settlements were used as the basis for the study, identifying 1,448 homes. In each region, 35 EAs were chosen, and then 10 smaller areas (primary sampling units or PSUs) were selected within those EAs. Homes were then systematically chosen from these areas for participation.
The survey interviewed 6,285 women between the ages of 15 and 49. This particular analysis explores what influences women’s awareness of HIV/AIDS. After accounting for any missing information, the final number of women included in this analysis was 6,259. Trained interviewers used a standardized questionnaire on Android tablets to collect the data. Survey staff received training, and the questionnaire was tested beforehand. Fieldwork was carefully monitored, including the use of GPS to track interviewers and ensure accuracy. 31
Study variables
The dependent variable for this study was awareness of HIV/AIDS, which was operationalized as a dichotomous variable, based on whether the women responded “yes” or “no” to the question “Have you ever heard of HIV/AIDS?”. It is important to note that this measures awareness, not comprehensive knowledge of transmission or prevention.
Independent variables were individual-level factors including respondent’s age, educational level, wealth quintiles, exposure to radio, and exposure to television. In addition, community-level variables, such as place of residence and region, were included in the analysis. Wealth status was measured using an asset-based index constructed via Principal Component Analysis and divided into quintiles, following standard DHS methodology.
Data processing and analysis
Data handling involved importing the collected information into two distinct software environments: STATA v14.0, designated for intricate hierarchical analyses, and R Studio, used for geospatial mapping and visualization. Within R Studio, geographical position data were leveraged to construct visual representations of HIV/AIDS awareness distribution among women residing in Somaliland. Specialized R libraries, including sf, sp, ggplot2, and leaflet, were employed to develop cartographic outputs illustrating HIV/AIDS awareness prevalence across various locales, pinpointing awareness hotspots, and uncovering underlying spatial relationships. Basic descriptive statistics were generated through computations of common metrics like averages, event frequencies, and proportional representations. To discern the independent influences on the primary study focus, a multilevel random-intercept logistic regression model was used to account for the hierarchical nature of the data, with women (level 1) nested within enumeration areas (level 2). This methodology was implemented across a sequence of four analytical models: Model 0 (baseline, devoid of explanatory factors), Model I (incorporating individual-level traits), Model II (incorporating community-level traits), and Model III (encompassing both individual and community traits). Furthermore, stochastic effects, standard error magnitudes, and intra-cluster dependencies were evaluated, with resulting estimates calibrated to mirror the broader population. Factors exhibiting adjusted odds ratios (AOR) coupled with probability values below 0.05 were deemed demonstrably linked to HIV/AIDS awareness in the regression analysis. For the exploratory spatial autocorrelation analysis, a significance level of p < .1 was used to identify potential clustering. Spatial analysis helps to identify geographical patterns and variations in the proportion of the population who have ever heard of HIV/AIDS in the regions of Somaliland. This analysis provides insights into regions with high awareness and potential clusters for targeted intervention.
Results
Characteristics of the study participants
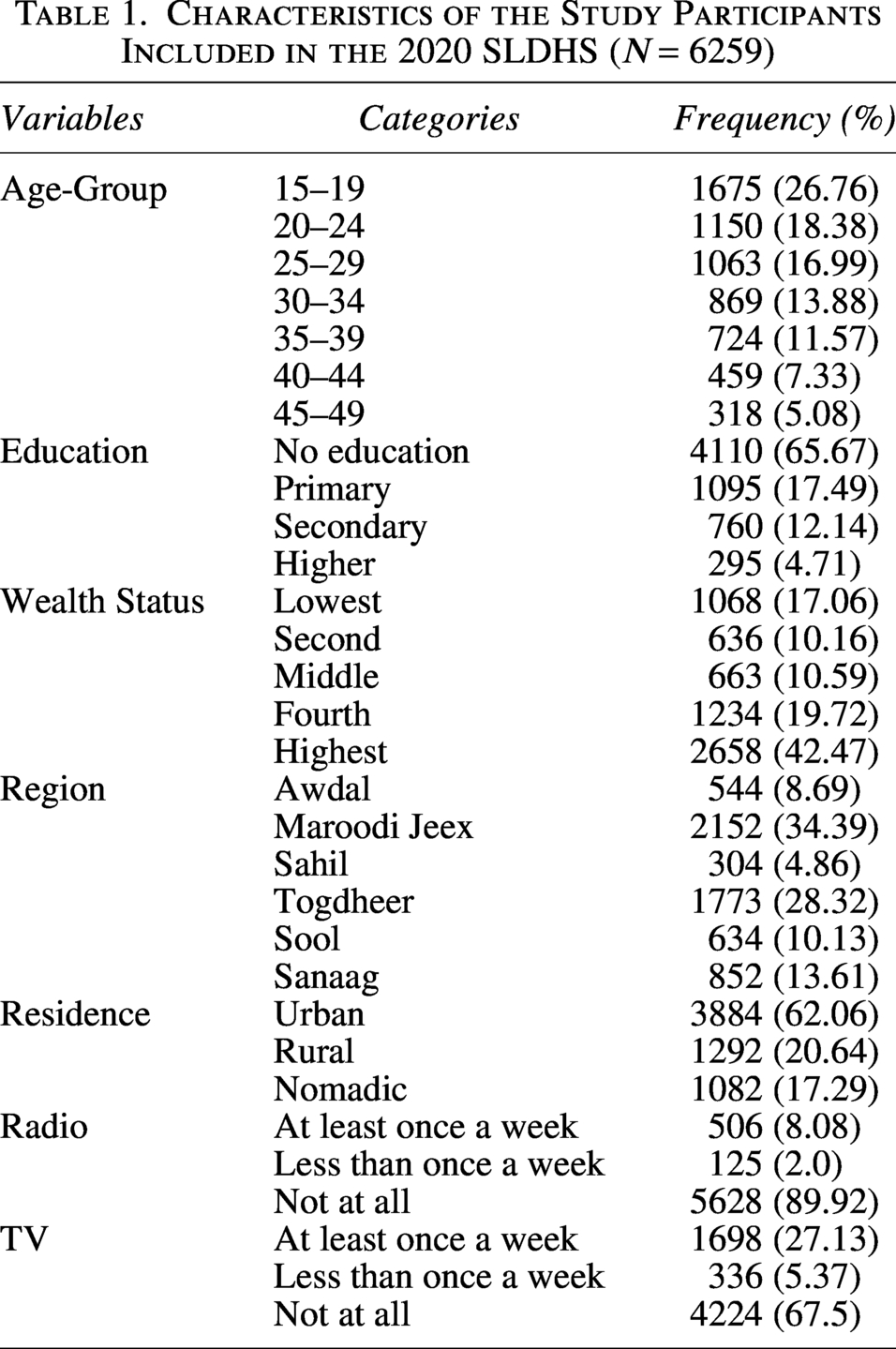
This study included 6,259 participants categorized across several demographic variables. In Table 1, the largest age group was 15–19 years old (26.76%), followed by 20–24 years old (18.38%). In terms of education, most participants had no formal education (65.67%), with smaller proportions having primary (17.49%), secondary (12.14%), or higher education (4.71%). The distribution of wealth status showed a wide range, with the highest quintile comprising 42.47% of participants, compared with 17.06% in the lowest wealth quintile. Geographically, the Maroodi Jeex region accounted for the largest proportion of the sample (34.39%), while the Togdheer region was the second largest (28.32%). Regarding residence, a majority of the participants lived in urban areas (62.06%), with the remainder living in rural (20.64%) or nomadic (17.29%) settings. Access to media varied, with most reporting no radio use (89.92%) and not watching television (67.5%).
Characteristics of the Study Participants Included in the 2020 SLDHS (N = 6259)
Level of knowledge of having ever heard HIV/AIDS among women in Somaliland, SLDHS 2020
Figure 1 illustrates the distribution of responses regarding participants’ awareness of HIV. Specifically, this pie chart visualizes the proportion of individuals who reported ever hearing about HIV versus those who had not. The data reveal that a substantial majority, 80.55%, of participants indicated they had heard of HIV. Conversely, a notable minority, 19.45%, reported having never heard of HIV/AIDS. This represents a contrast in awareness levels within the surveyed population.
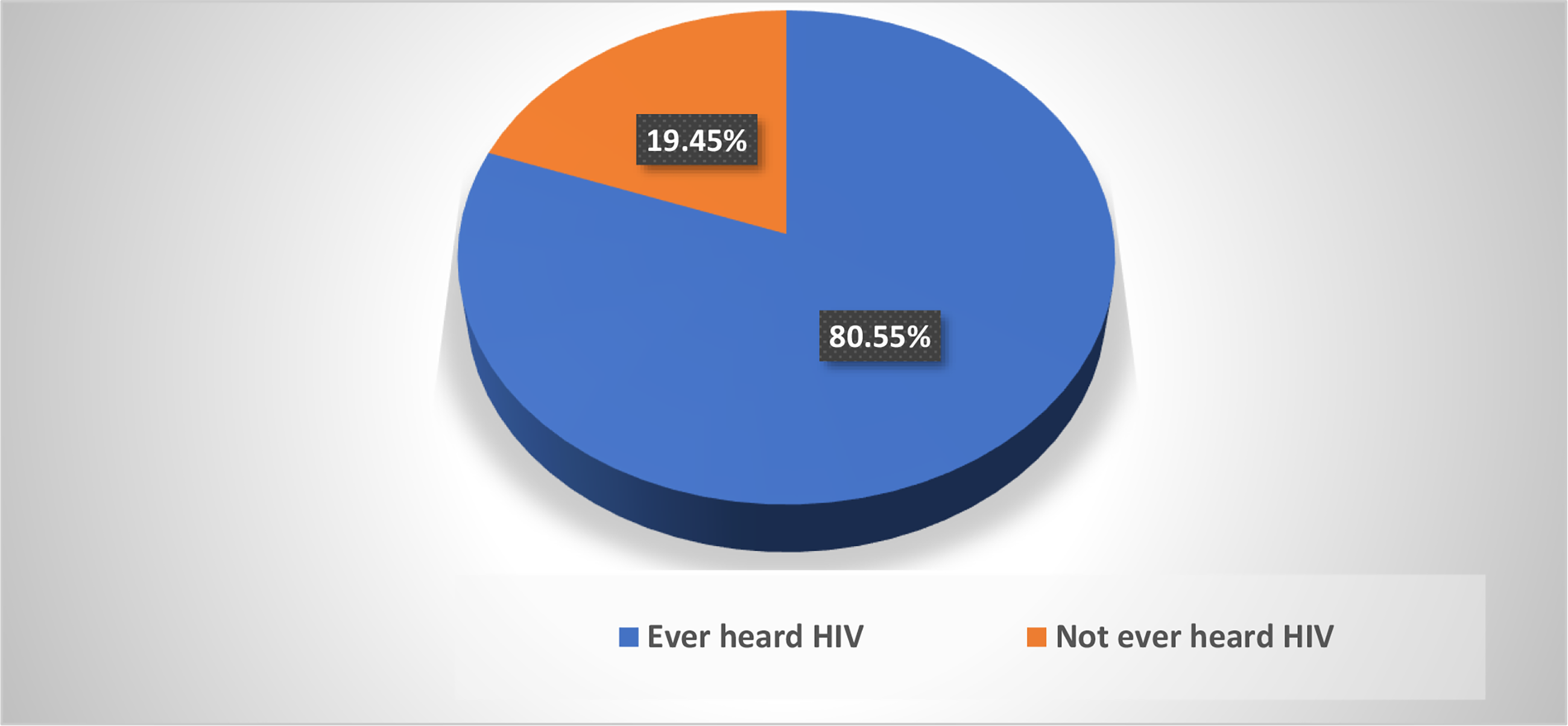
Prevalence of having ever heard HIV/AIDS among women in Somaliland, SLDHS 2020.
Results of multilevel logistic regression
The findings of Table 2, based on the final model (Model III), indicate that several individual and community-level factors were significantly associated with the likelihood of having ever heard of HIV. Specifically, increased age was associated with higher odds of awareness, with the 20–24 age group (AOR: 1.80, CI: 1.48–2.18) and all older age groups up to 45–49 showing significantly greater odds compared with the 15–19 age group. Similarly, higher levels of education were also linked to increased odds of HIV awareness, as participants with primary (AOR: 2.14, CI: 1.75–2.63), secondary, and higher education demonstrated significantly higher odds of having ever heard of HIV compared with those with no formal education. In the final model (Model III), wealth quintile was not a statistically significant predictor of having heard of HIV/AIDS. Conversely, not listening to the radio at all was associated with significantly lower odds of awareness (AOR: 0.49, CI: 0.30–0.82), while frequency of watching TV was not statistically significant. At the community level, those in the Maroodi Jeex and Sahil regions showed significantly higher odds of having heard of HIV compared with those in the Awdal region, while those in the Sool region had significantly lower odds. In addition, both rural and nomadic participants had significantly decreased odds of having ever heard of HIV compared with urban participants.
Multilevel Regression Analysis of Predictors of Having Ever Heard of HIV/AIDS in Somaliland, SLDHS 2020
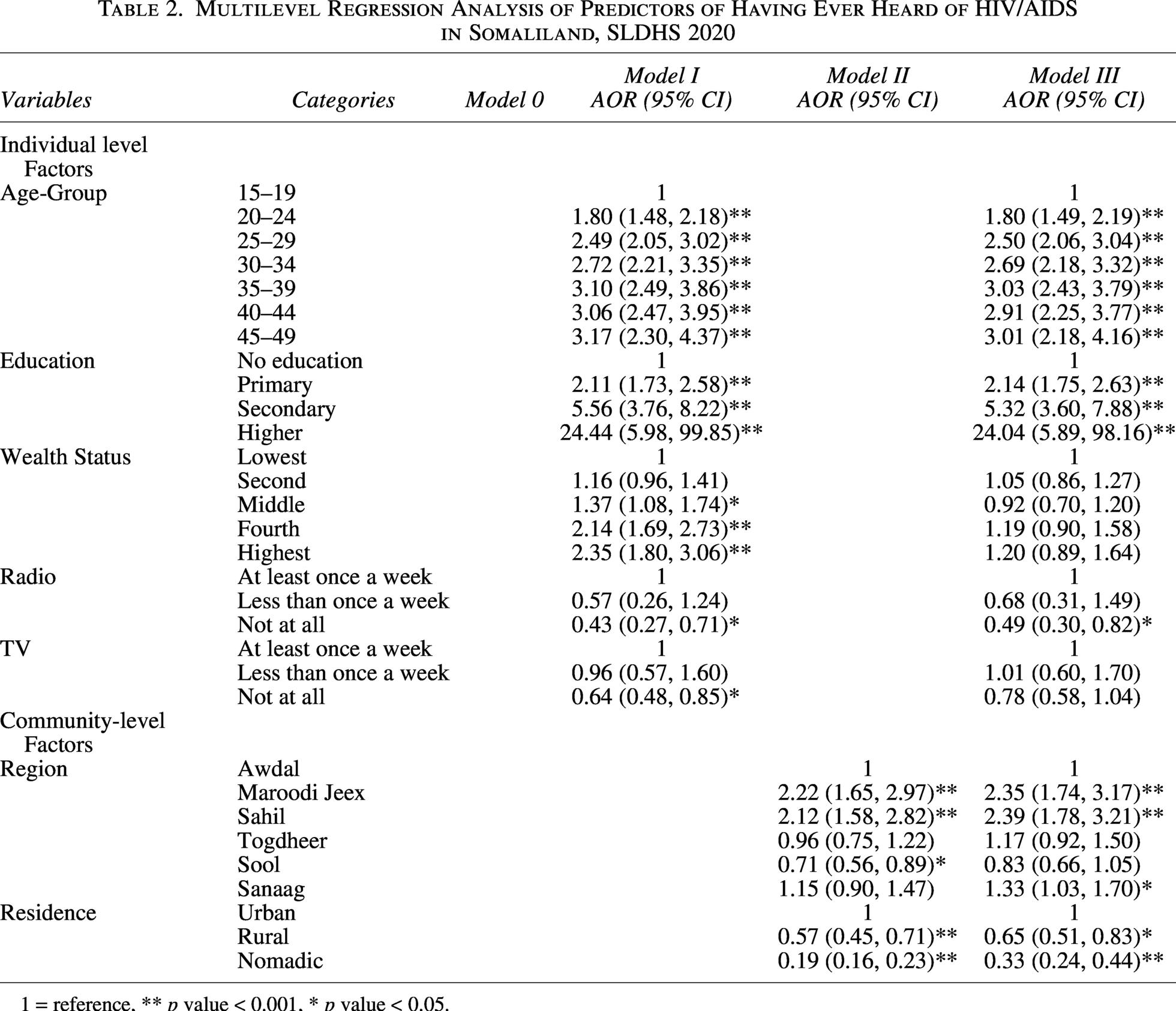
1 = reference, ** p value < 0.001, * p value < 0.05.
Since there is a significant clustering effect, a measure of variation (ICC) was performed. The ICC for the empty model (Model 0) was 0.243, which indicates that the variation in the outcome could be due to unmeasured community-level characteristics. The ICC value decreases across all models, with Model I having an ICC of 0.070, Model II having an ICC of 0.026, and Model III having an ICC of 0.023. The final model (Model III) was the best fit since the goodness of fit test statistically values (AIC, BIC) were lower than the remaining models. Specifically, Model III had the lowest AIC (6196.58) and BIC (6371.82). The log-likelihood ratio also increased across the models, with model 0 being −3368.58, and model III being −3072.3, indicating improved model fit (Table 3).
Model of Fitness
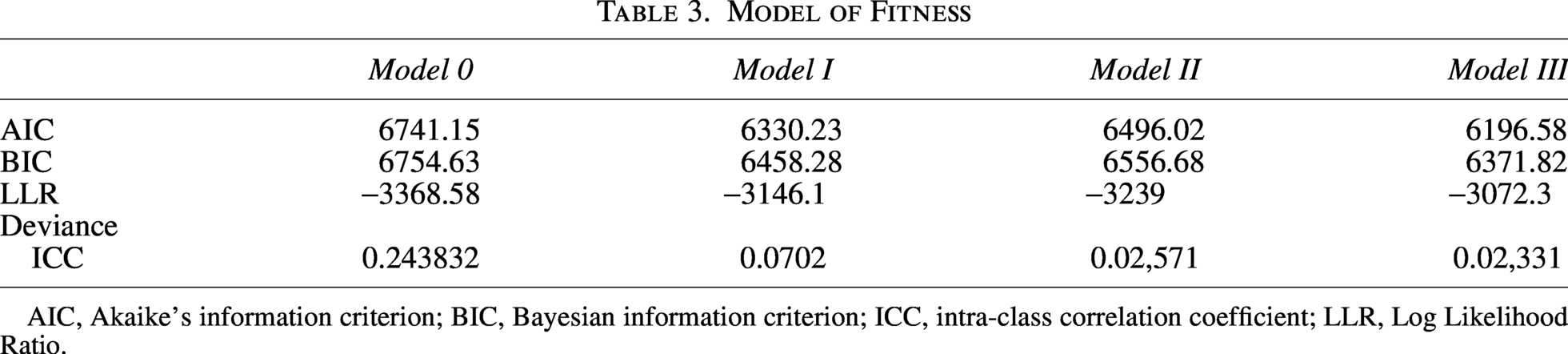
AIC, Akaike’s information criterion; BIC, Bayesian information criterion; ICC, intra-class correlation coefficient; LLR, Log Likelihood Ratio.
Spatial distribution of having ever heard HIV/AIDS among women in Somaliland
Spatial analysis helps to identify geographical patterns and variations in the proportion of the population who have ever heard of HIV/AIDS in the regions of Somaliland. This analysis provides insights into regions with high awareness and potential clusters for targeted intervention. As shown in Figure 2, the spatial distribution of the population who have heard of HIV/AIDS is presented in the map, highlighting significant regional disparities. Regions such as Sool and Togdheer demonstrate higher awareness levels (1.277–1.392), indicated by the darkest shading, while regions Maroodi Jeex and Sahil (1.143–1.267) show the lowest levels, as represented by the lightest shading.
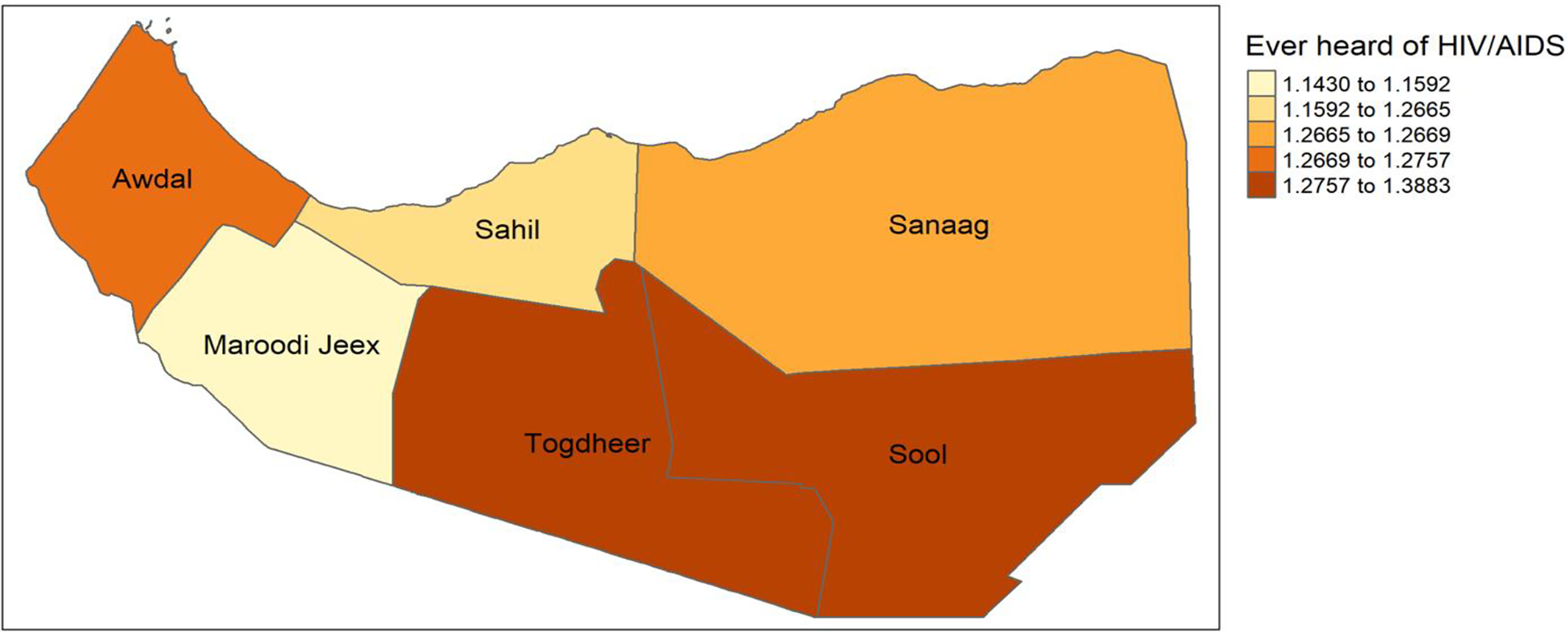
Spatial distribution of having ever heard HIV/AIDS among women in Somaliland.
Global Moran’s I spatial autocorrelation
A Global Moran’s I test was conducted to examine spatial autocorrelation in the distribution of factors related to having ever heard of HIV/AIDS in the region. As shown in Table 4 and Figure 3, based on the given statistics, the results indicate a weak positive spatial autocorrelation (Moran’s I = 0.105, Z-score = 1.418, p = .078). This suggests that regions with similar levels of the measured HIV/AIDS indicator may have a tendency to cluster spatially. With a p-value of .078, the spatial autocorrelation is statistically significant at the 0.1 significance level, indicating that the observed clustering is unlikely due to random chance. This finding implies that the distribution of the HIV/AIDS-related factor is not entirely random, and there may be underlying spatial dependencies that warrant further investigation.
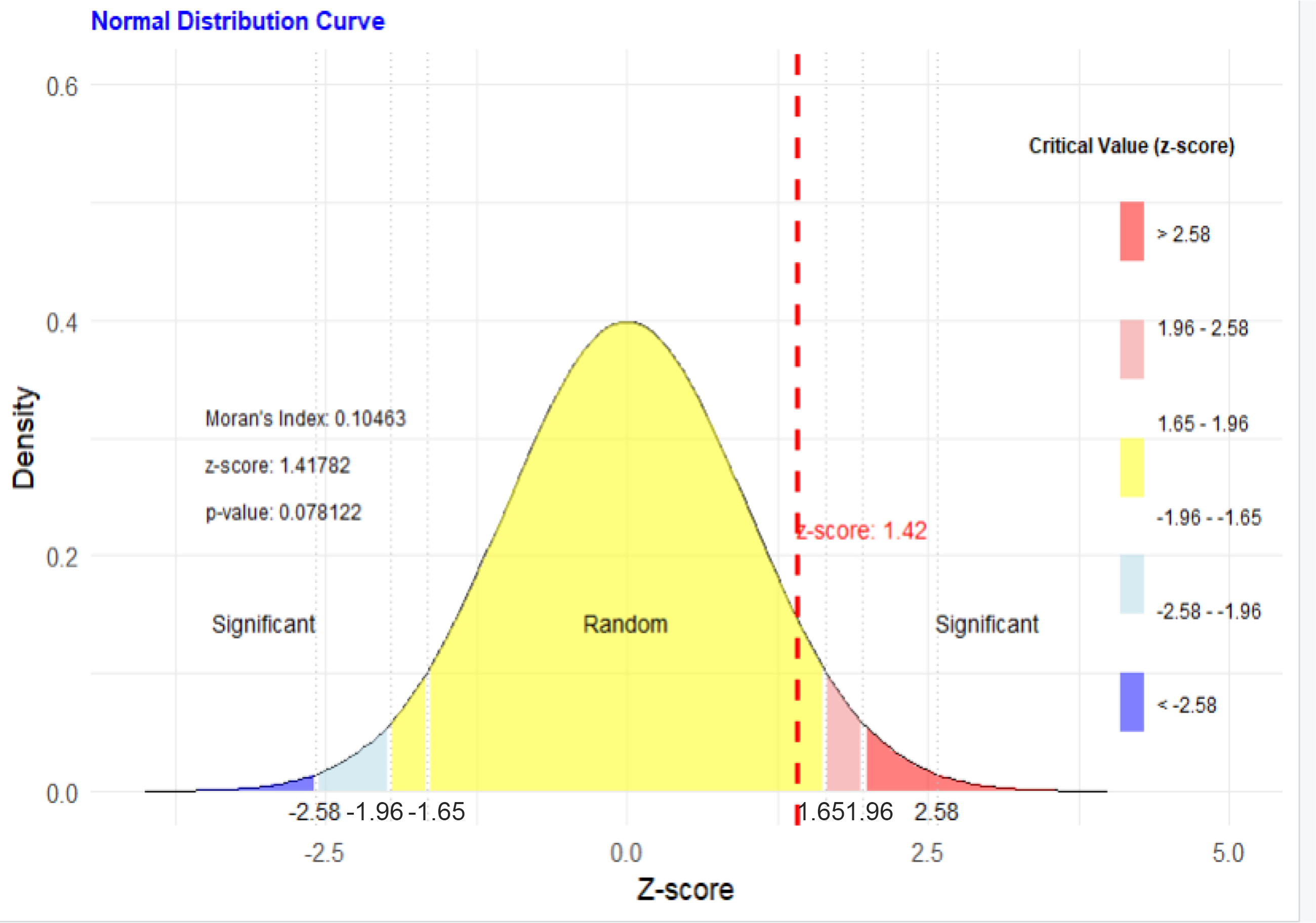
Z-score.
Global Moran’s I
Local Moran’s I spatial autocorrelation
Local spatial autocorrelation analysis, utilizing Moran’s I and associated p values, reveals nuanced patterns in HIV/AIDS-related indicators across the study area. Figure 4 depicts spatial clustering, with Maroodi Jeex and Sool exhibiting positive Moran’s I value (0.256–0.432), indicative of localized homogeneity in either high or low levels of the measured indicator. Conversely, Awdal displays a marginally negative Moran’s I (−0.245 to −0.040), suggesting greater spatial heterogeneity. Statistical significance, as determined by p values in Figure 4, is only observed in Sahel and Sool (p < .1), implying a robust clustering effect warranting focused investigation of local drivers. The absence of significant clustering in Awdal, Maroodi Jeex, Togdheer, Sahel, and Sanaag (p > .1) suggests that while spatial patterns may exist, they are not statistically robust at the regional level, necessitating broader-scale analyses to identify underlying determinants of HIV/AIDS disparities and inform evidence-based intervention strategies.
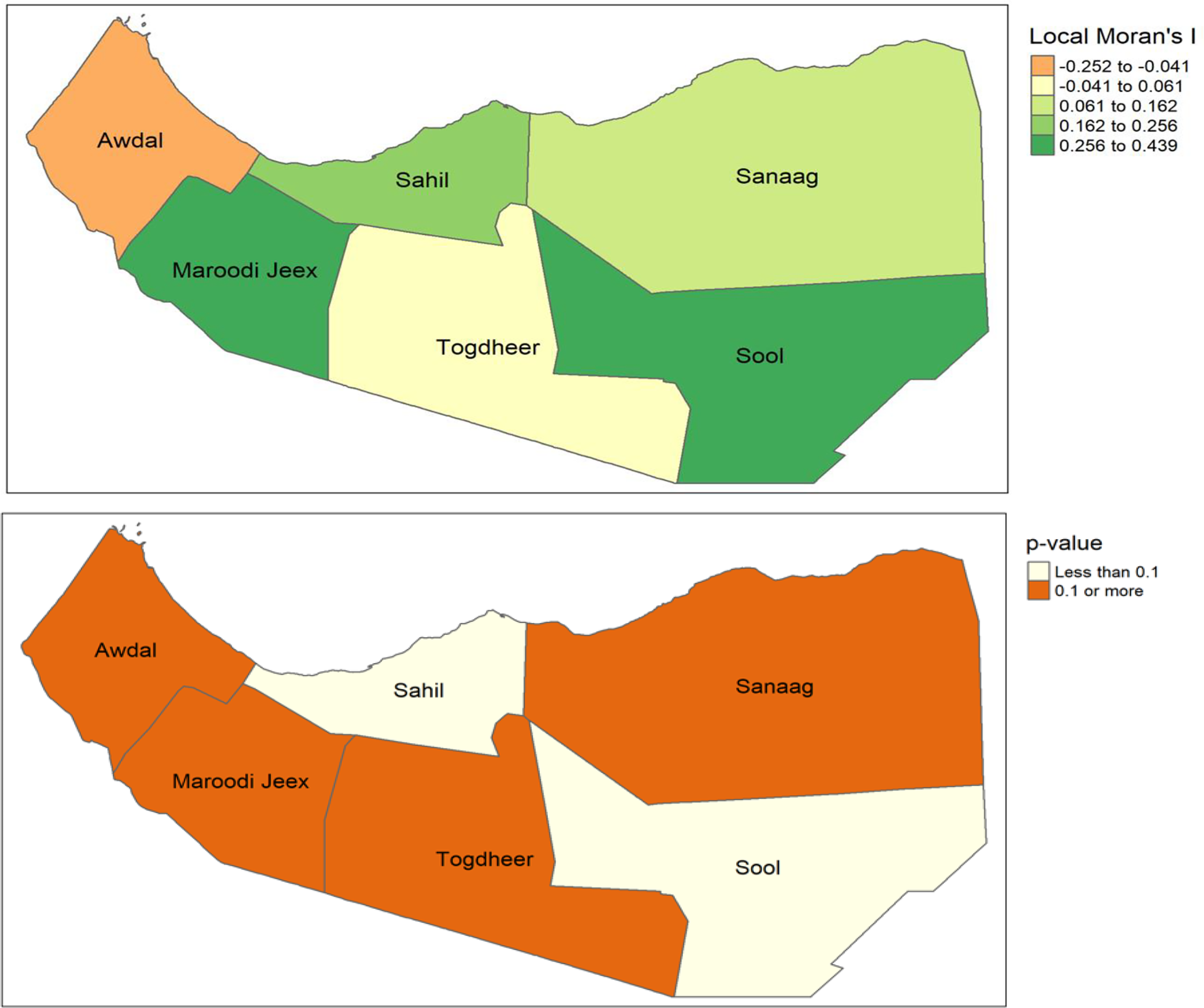
Local Moran’s I and p value.
Hotspots and cold spots analysis (Getis-Ord Gi*)
As illustrated in the Figure 5, the Getis-Ord Gi* statistic identifies both hotspots and cold spots, indicating regions with significantly high or low HIV/AIDS awareness levels. Regions such as Sanaag and Sool exhibit positive Gi* values, signifying significant clustering of higher HIV/AIDS awareness. These areas, highlighted in green, suggest more effective HIV/AIDS education programs, better access to information, or greater community engagement in addressing the issue. Conversely, the region including Awdal displays negative Gi* values, indicating clustering of lower HIV/AIDS awareness and highlighting areas that may require targeted intervention efforts such as awareness campaigns, increased access to educational resources, or culturally sensitive outreach programs. Regions like Togdheer, Sahil, and Maroodi Jeex exhibit Gi* values closer to zero, suggesting a more dispersed or inconsistent pattern of HIV/AIDS awareness and the absence of statistically significant spatial clustering. These findings highlight the need for targeted, evidence-based strategies to address spatial disparities and improve HIV/AIDS awareness across the region.
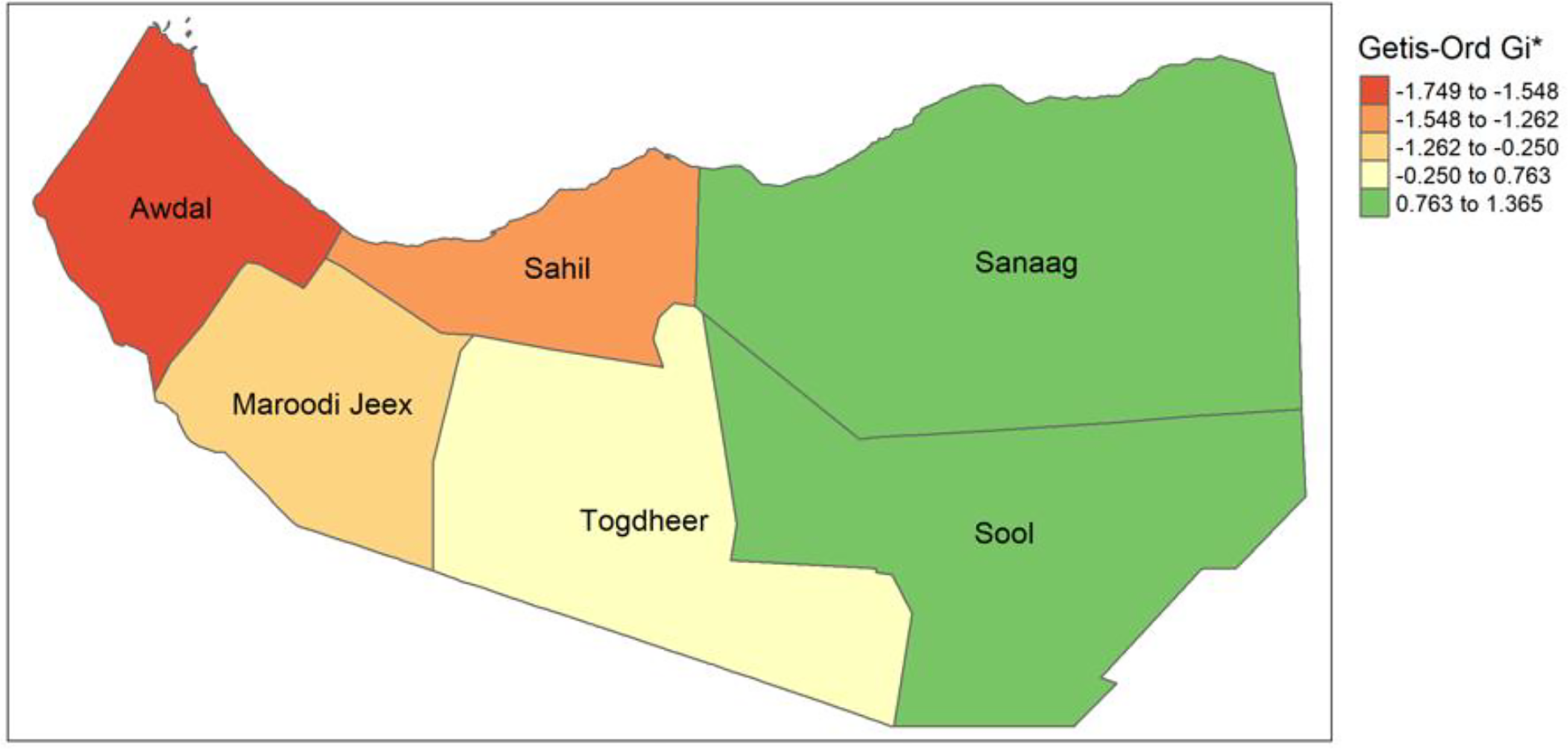
Getis-Ord GI*.
Discussion
The present research aimed to explore spatial variation and various related factors with women’s knowledge of HIV/AIDS in Somaliland using data from the 2020 Somaliland Demographic Health Survey.
This study highlighted that despite the high-risk pandemic of HIV/AIDs in Somaliland, only 80.55% of Somaliland women have ever heard of HIV/AIDS. It showed that more than 19.45% of women were unaware of HIV/AIDS, rising high concerns. The findings were higher than previous studies in Uganda (38%), 17 in Ethiopia (51.1%), in Bangladesh (60%), 32 and Somalia (67.6%), 21 and lower than studies in Ecuador (88%), 33 in Nigeria (83%), 5 illustrating the regional heterogeneity in HIV awareness within Countries. This underscores the urgent need for targeted interventions specifically tailored to the context of Somaliland.
Significant geographical differences in HIV/AIDS awareness were found by spatial analysis utilizing the Getis-Ord Gi* statistic. Sanaag and Sool are hotspots for HIV/AIDS awareness, as evidenced by the statistically significant clustering of higher awareness levels. On the other hand, Awdal exhibits lesser awareness clustering, designating it as a cold spot. There is no statistically significant grouping in areas like Togdheer and Maroodi Jeex, which show a more scattered pattern. In order to successfully address and raise HIV/AIDS awareness throughout the region, these spatial disparities underscore the necessity of focused interventions, such as awareness campaigns in cold spots and additional research on the achievements of hotspot regions.
Our findings confirm that increased age is a significant association, with women aged 20–24 having higher odds (AOR: 1.80, 95% CI = 1.48–2.18) of awareness of HIV compared with those aged 15–19. This finding is similar to studies conducted in Somalia, 21 Mozambique, 34 and Nigeria. 35 Thus, mature women, understanding their susceptibility to health problems, may be more proactive in seeking information to maintain their well-being. 36
Our study found that education level was positively associated with women’s HIV awareness. This shows higher levels of education were also linked to increased odds of HIV awareness, as participants with primary (AOR: 2.14, CI: 1.75–2.63), Secondary, and higher education demonstrated significantly higher odds of having ever heard of HIV compared with those with no formal education. This was supported by other findings14,17,22,37 and contradicts studies conducted in Uganda 17 and Nigeria.38,39
Consistent with studies in Ghana, 40 Ethiopia, 22 Nigeria, 38 Rwanda, 41 and Pakistan, 32 this research reveals an awareness gap regarding HIV among women. Specifically, women in rural and nomadic areas demonstrate lower HIV awareness compared with women in urban settings. This is potentially attributable to the economic hardships faced by rural women and their restricted access to educational resources and HIV/AIDS information campaigns, ultimately impeding the distribution of accurate information.
Interestingly, while spatial analysis identified Sool as a hotspot for raw awareness, the multilevel regression (Model III) showed lower adjusted odds for this region. This suggests that the high awareness in Sool may be concentrated in specific clusters or driven by demographic factors like age and education; once these variables are controlled for in the regression model, the independent “region effect” for Sool is less pronounced than in regions like Maroodi Jeex.
Finally, the study revealed a significant correlation between media access and HIV awareness. Women of reproductive age who reported not using the radio (AOR: 0.49, CI: 0.30–0.82) were significantly less likely to be aware of HIV compared with those who did.
Policy implications
This research offers important policy recommendations to improve HIV/AIDS awareness and prevention efforts in Somaliland. The study highlights the need for a comprehensive approach that takes into account both individual and community-level factors influencing HIV awareness. Policymakers should prioritize educational initiatives, especially for girls and women, to strengthen their understanding of HIV/AIDS. It is crucial to implement targeted public health programs that effectively reach women in rural and nomadic areas, using channels like radio and community health workers to deliver accurate information. In addition, addressing socioeconomic inequalities is critical, as poverty limits access to education, health care, and vital information. The spatial disparities uncovered in this study underscore the importance of strategically allocating resources and designing tailored interventions to address gaps in access to HIV/AIDS awareness and prevention services across different regions. By adopting evidence-based policies informed by these findings, Somaliland can enhance its efforts to combat HIV/AIDS and improve the health and well-being of its female population.
Strengths and limitations
This study leverages the nationally representative 2020 SLDHS, employing a rigorous multistage sampling design to ensure generalizability to the target population of women aged 15–49. A key strength lies in the application of multilevel modeling, facilitating the examination of factors at individual, household, and community levels, thereby providing a nuanced understanding of HIV/AIDS awareness. Furthermore, the integration of spatial analysis techniques, including the identification of statistically significant hot and cold spots, offers valuable insights for targeted public health interventions. Finally, this research addresses a notable gap in the existing literature by focusing on the understudied context of Somaliland.
Despite these contributions, several limitations should be acknowledged. The cross-sectional design prevents drawing conclusions about cause and effect. Reliance on self-reported data carries the risk of recall inaccuracies and social desirability bias. The absence of data on specific cultural factors limited a more in-depth understanding of influences on HIV/AIDS awareness. In addition, a change of data years between previous studies and this study might affect the accuracy of results. Furthermore, the lack of longitudinal data restricts the examination of changes in knowledge over time. Nevertheless, the study offers valuable insights into the geographical patterns and factors associated with HIV/AIDS awareness among women in Somaliland.
Conclusion
This study provides a detailed analysis of the factors associated with Somaliland women’s awareness of HIV/AIDS and its determinants. The results highlight how urgently comprehensive and focused initiatives are needed to raise HIV/AIDS awareness and slow the virus’s spread in the area. Somaliland can significantly advance its public health objectives and enhance the well-being of its female population by addressing the important individual- and community-level factors found in this study and customizing interventions to the unique requirements of various regions and populations. The findings of the study draw attention to spatial disparities that need to be addressed in order to close gaps in access to HIV/AIDS resources and education. Stakeholders and governments may improve equity and women’s well-being across Somaliland by using evidence-based measures.
Ethics Approval and Consent to Participants
Ethical board review and participant consent were not specifically required for the present analysis due to its nature as a secondary analysis of publicly accessible data from the SLHDS. Access to the requisite data was formally requested by the authors and subsequently approved by the SLHDS program administrators. Verbal informed consent had been previously obtained from all respondents participating in the primary SLHDS study. All methodologies utilized herein conform to the tenets of the Declaration of Helsinki.
Authors’ Contributions
The research initiative was crafted by M.M.A., M.H.D., and H.A.A. M.M.A. handled data organization, executed the formal analysis, formulated the methodology, and directed the project. The study was conducted by M.M.A., K.H.J.O., Y.D.A.A., M.H.D., and H.A.A. The initial article draft was prepared by M.M.A., K.H.J.O., Y.D.A.A., and M.H.D. A.H.M. provided his methodological expertise, ensured validation, and offered supervision. All authors engaged in the article’s review and editing. Each author has read and given their approval for the final version of the submitted article.
Footnotes
Acknowledgments
The authors would like to express sincere thanks to the Ministry of Health, Somaliland, for providing access to the SLHDS data for this study.
Availability of the Data and Materials
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No specific fund was received for this work.