
Abstract
Purpose:
This study examined the relationships among intermediary determinants, structural determinants, and adult smoking status and quit attempts.
Design:
Secondary data analysis of cross-sectional data.
Setting:
Data come from the 2015 Behavioral Risk Factor Surveillance System (BRFSS), Social Context module. A national, representative sample from 12 US states (Alabama, Arkansas, Delaware, District of Columbia, Georgia, Louisiana, Minnesota, Mississippi, Missouri, Rhode Island, Tennessee, and Utah).
Participants:
A total of 64 053 noninstitutionalized US adults aged ≥18 years.
Measures:
Smoking status and quit attempts were outcome variables. Individual-level structural determinants (age, sex, race/ethnicity, marital status, education, and employment status) and intermediary determinants (housing insecurity, food insecurity, health insurance, binge drinking, and general health mental health) from BRFSS.
Analysis:
Weighted multivariate, multinomial logistic regression.
Results:
Current smoking was greater among men, respondents aged between 35 to 64 and 55 to 64, adults who reported food insecurity, housing insecurity, frequent mental distress, binge drinking, and who were unemployed. Current smokers had higher odds of making quit attempts in the past 12 months if they were non-Hispanic Black, graduated college, and reported food and housing insecurity.
Conclusion:
Multifaceted smoking cessation interventions that address food and housing needs also incorporate screening for potential comorbidities such as mental distress and/or hazardous alcohol use and may be needed to enhance smoking cessation rates among racially diverse adults.
Keywords
Purpose
The prevalence of cigarette smoking among US adults declined significantly in the recent years, from 21% in 2005 to 15% in 2015. 1 However, the progress has been uneven across the socioeconomic statuses and among racial/ethnic groups. In fact, among all races/ethnicities, American Indian/Alaska Natives have the highest smoking prevalence (21.9%). 1 Higher prevalence of smoking (26.1%) is reported among adults living below the poverty line, about twice that of people living above the poverty line (13.9%). 1 In the United States, more than 480 000 individuals die from cigarette smoking or second-hand smoke exposure each year. 2 Moreover, tobacco use is responsible for 30% of all cancer deaths in the United States. 3 Tobacco use not only negatively affects individuals’ health but also impacts the household budget. In fact, about 7.4% of all smokers and 11.8% of smokers with low incomes were unable to spend money on household essentials because money was spent on tobacco. 4 Spending household funds on cigarettes is associated with lower spending on health care, education, healthy food, and housing. 5 -7
Previous studies have demonstrated that a significant proportion of adult cigarette smokers are interested in quitting smoking. 8 However, many of them have not been able to quit smoking successfully and experience relapse. 8,9 About 53% of current smokers tried to quit smoking in the past year, but only 6% of smokers had quit smoking successfully 1 year later, 8,10 and majority of them relapse within the first 5 to 10 days of the quitting attempt. 9 Moreover, quit attempts among adults with low socioeconomic status are less likely to be successful, 11 suggesting that interventions for quitting smoking need to be tailored to meet the needs of specific subgroups of individuals. Therefore, identifying determinants of smoking behaviors and quit attempts is important to enhance successful quitting.
We used the Commission on Social Determinants of Health (CSDH) Framework 12 to guide this study. The CSDH Framework illustrates relationships between conditions in which people are born, grow, live, work, and age and their well-being. Authors of the CSDH used structural and intermediary determinants to explain well-being. 12 Structural determinants include factors related to people’s socioeconomic position such as level of education, income level, and occupational status and social class such as gender and race/ethnicity. Structural determinants impact on well-being through intermediary determinants that include living conditions (eg, housing security), food availability (eg, food security), access to health care (eg, health insurance coverage), behavioral factors (eg, alcohol use), and psychosocial factors (eg, stress). 12 Previous research findings indicated that adults who report lower education levels, 11 underemployment, 11,13 lack of health insurance coverage, 1 housing insecurity, 14 food insecurity, 15 binge drinking, 16 and mental distress 17 -19 are more likely to be smokers and less likely to successfully quit smoking.
Several studies have examined the relationships between isolated social determinant factors associated with smoking such as sociodemographic, psychosocial, or behavioral factors alone. 11,13,14,20 However, a broader range of social determinant factors that might be associated with smoking status and quit attempts have not been studied extensively at the population level. Thus, this study examined the relationships among intermediary determinants, structural determinants, and adult smoking status and quit attempts, using representative, population-based data with a large and diverse sample. These factors could be used to identify important subgroups of individuals that could benefit from tailored smoking cessation interventions.
Methods
Design
We conducted a cross-sectional analysis using data from the 2015 Behavioral Risk Factor Surveillance System (BRFSS), Social Context module that was administered in 12 US states (Alabama, Arkansas, Delaware, District of Columbia, Georgia, Louisiana, Minnesota, Mississippi, Missouri, Rhode Island, Tennessee, and Utah). The BRFSS is a cross-sectional, state-based, nationally representative, computer-assisted telephone survey of noninstitutionalized US adults aged 18 years and older. The BRFSS is conducted annually by the Centers for Disease Control and Prevention (CDC) in all 50 states of the United States as well as the District of Columbia, Puerto Rico, the US Virgin Islands, and Guam. Details about the sampling procedure and methodology are published elsewhere. 21 The core questionnaire addresses information on chronic health conditions, health status, health-related risk behaviors, health-care access, and demographic and socioeconomic characteristics. The core questionnaire is administered in all states and territories. In addition, each state may choose to administer optional BRFSS modules on specific topics such as social context and cancer survivorship. The total sample size for the 2015 BRFSS was 441 456, and the median state-level response rate was 47.2%. 21 This analysis of BRFSS survey anonymized publicly available data and required no institutional review board review.
Sample
In 2015, only 12 states and entities administered the module of questions measuring social context, which included food and housing measures in addition to core questionnaire. The response rate in these 12 states ranged from 37.9% in District of Columbia to 61.1% in Utah. 21 A sample of 84 353 adults, who participated in those 12 states, was restricted to the individuals who answered the questions about housing and food insecurity (n = 68 025). The sample was further restricted to participants who had complete data on outcome variables, smoking status, and quit attempt. Thus, we excluded respondents from the analysis who had incomplete data on smoking status (n = 398) and quit attempt (n = 31). Further, we excluded respondents because of missing values in any of the study variable or they if had responses of “don’t know” or “refused.” Participants were excluded from the analysis who had incomplete data on demographic and socioeconomic characteristics (n = 1467) and clinical and behavioral characteristics (n = 2076). This yielded an analytic sample of 64 053 respondents. For measuring quit attempt, a subset of 9096 of 64 053 participants who were current smokers and responded to the question measuring quit attempt were used.
Measures
Outcome variables
Outcome variables for this study were (1) smoking status and (2) making a quit attempt. Using standard categorizations, smoking status was classified as current smokers (adults who smoked at least 100 cigarettes in their entire life and currently smoke cigarettes every day or some days), former smokers (adults who smoked at least 100 cigarettes in their entire life but do not smoke at all currently), and never smokers (adults who smoked less than 100 cigarettes in their entire life). The smoking status measures have high reliability and validity as well are consistent with CDC definitions. 22 -25 Then, for measuring quit attempts, current smokers were asked “During the past 12 months, have you stopped smoking for one day or longer because you were trying to quit smoking?”. The quit attempt was then classified as yes (current smokers who tried to quit cigarette smoking) and no (current smokers who did not try to quit cigarette smoking). 26
Structural determinants
We obtained data from the survey on the following factors: age of participants (categorized as 18-34, 35-54, 55-64, and 65 or older), sex (male vs female), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, and non-Hispanic other), marital status (married vs not married), education level (did not graduate and graduated high school, attended college or technical school, graduated from college or technical school), and employment status (employed, unemployed, and retired/students).
Intermediary determinants
Housing insecurity and food insecurity were each measured using 1 item. Respondents were asked “How often in the past 12 months would you say you were worried or stressed about having enough money to pay your rent/mortgage?” and “How often in the past 12 months would you say you were worried or stressed about having enough money to buy nutritious meals.” These questions had response choices of “always,” “usually,” “sometimes,” “rarely,” and “never”. Based on current literature, 27 housing insecurity and food insecurity responses were classified as yes (respondents answering “always,” “usually,” or “sometimes” to these questions) and no (respondents answering “rarely” or “never” to these questions). Health insurance coverage was measured as yes (having health insurance) and no (not having health insurance). Binge drinking status (categorized as yes/no) was defined as males having 5 or more drinks on one occasion and females having 4 or more drinks on one occasion. 23 General health status was reclassified from 5 into 2 categories as (fair/poor vs good/very good/excellent). Mental distress was reclassified as infrequent mental distress (when adults reported from 0 to 13 days mental health not good during the past 30 days) and frequent mental distress (when adults reported from 14 to 30 days mental health not good during the past 30 days). The classification for mental health is consistent with previously established classification and with the literature examining infrequent and mental distress using BRFSS data. 17 -19,28
Analysis
Survey weights were used to account for the complex survey design of the BRFSS and generate representative results. Thus, the sample of 64 053 participants corresponds to a population estimate of 26.5 million, and the subset of 9096 participants corresponds to a population estimate of 5 million in the included 12 states. Descriptive statistics, percentages, and 95% confidence intervals (CIs) were conducted to describe the sample characteristics and population estimates. Multivariate, multinomial logistic regression was used to examine the associations between structural and intermediary determinants and smoking status. In regression analysis, we compared current versus never smokers and current versus former smokers. Separate multivariate logistic regression analyses restricted to the subset of current smokers were conducted to examine the association between structural and intermediary determinant factors and quit attempt. In all models, we estimated weighted adjusted odds ratios (AORs) and their 95% CIs. A 2-sided P value of ≤.05 was considered statistically significant. Stata version 14 was used to perform analyses.
Results
Sample Characteristics
Table 1 presents the study sample characteristics. Overall, more respondents were non-Hispanic white (72.5%) and female (52.9%), and about 39.0% were aged 55 years and older. Among the subset of respondents from the 12 states, about 19.0% (5 million) of the 26.5 million adults were current smokers, 25.0% (6.6 million) were former smokers, and 56.0% (14.8 million) were never smokers. Among current smokers, 61.2% (3 million) tried to quit smoking during the past 12 months. Approximately 33.0% (8.8 million) reported housing insecurity and 24.0% (6.3 million) reported food insecurity in the past 12 months.
Characteristics of Study Participants, BRFSS 2015, United States.
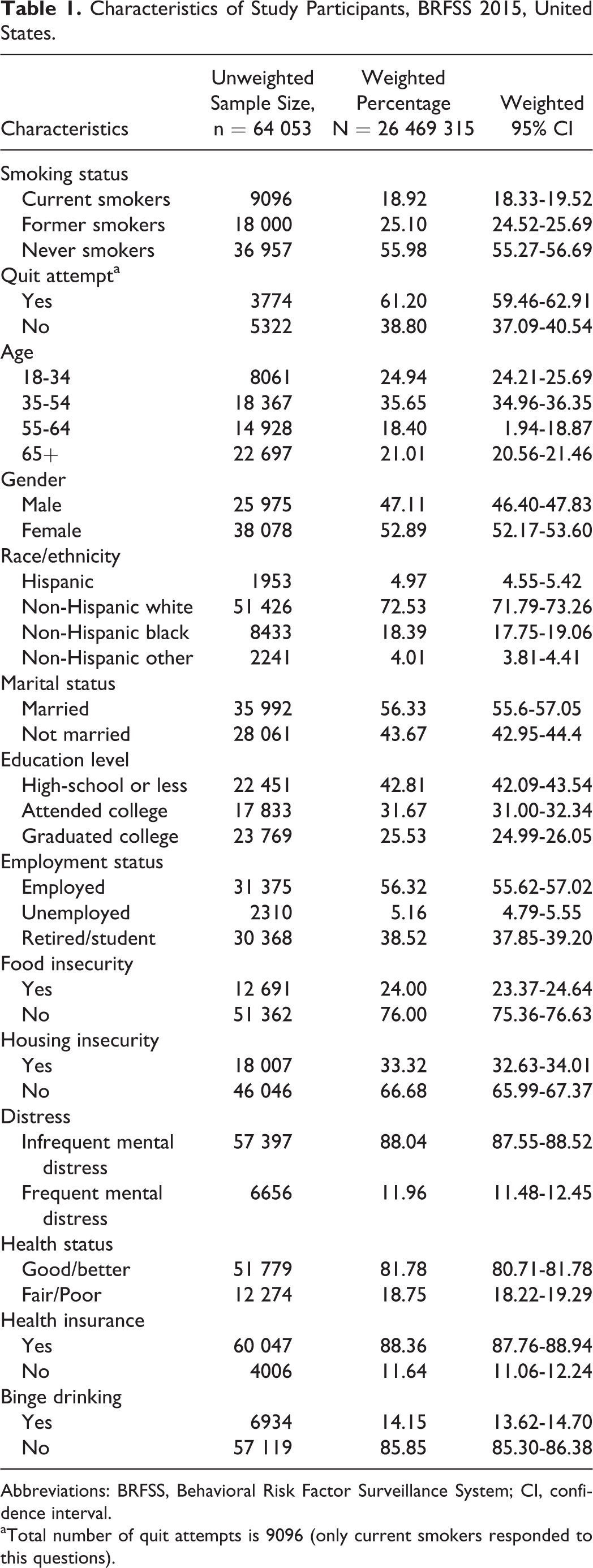
Abbreviations: BRFSS, Behavioral Risk Factor Surveillance System; CI, confidence interval.
aTotal number of quit attempts is 9096 (only current smokers responded to this questions).
Prevalence of Smoking Status
Table 2 shows the prevalence of current, former, and never smoking by characteristics of study participants. In 2015, 29.0% of adults aged 55 years and older, 20.6% of males, 19.8% of non-Hispanic blacks, 25.4% of not married adults, 26.2% of adults with high-school or less education were current smokers. In addition, 29.0% of adults who reported housing insecurity, 30.5% of adults who reported food insecurity, and 36% who reported frequent mental distress were current smokers.
Prevalence of Smoking Status by Characteristics of Study Population, BRFSS 2015 (n = 64 056), United States.

Abbreviations: BRFSS, Behavioral Risk Factor Surveillance System; CI, confidence interval.
Association Between Structural and Intermediary Determinants and Smoking Status
Structural determinants
Multivariate, multinomial logistic regression models indicated that compared to never smoking, current smoking was greater among men (AOR: 1.37; 95% CI: 1.25-1.50), respondents between 35 to 64 (AOR: 1.47; 95% CI: 1.30-1.67) and 55 to 64 (AOR: 1.48; 95% CI: 1.29-1.70) years of age and individuals who were unemployed (AOR: 1.49%; 95% CI: 1.22-1.82). The odds of being a current smoker (vs a former smoker) were higher among unemployed adults (AOR: 1.30; 95% CI: 1.04-1.64) than employed adults.
Intermediary determinants
Compared to the odds of being a never smoker, the odds of being a current smoker were higher among respondents who reported food insecurity (AOR: 1.20; 95% CI: 1.05-1.35), housing insecurity (AOR: 1.55; 95% CI: 1.38-1.73), frequent mental distress (AOR: 1.83; 95% CI: 1.60-2.10), and binge drinking (AOR: 3.19; 95% CI: 2.82-3.62). The logistic regression model comparing current smoking versus former smoking indicated that adults who reported housing insecurity (AOR: 1.42; 95% CI: 1.26-1.62), frequent mental distress (AOR: 1.49; 95% CI: 1.29-1.72), and binge drinking (AOR: 1.76; 95% CI: 1.47-1.89) had higher odds of being a current smoker than a former smoker (Table 3).
Multivariate Logistic Regression Models for Smoking Status and Quit Attempt, BRFSS 2015, United States.

Abbreviations: AOR, adjusted odds ratio; BRFSS, Behavioral Risk Factor Surveillance System; CI, confidence interval.
a P ≤ .001.
b P ≤ .05.
c P ≤ .01.
Association Between Structural and Intermediary Determinants and Quit Attempt
Structural determinants
Multivariate logistic regression model indicated that current smokers had higher odds of making a quit attempt in the past 12 months if they were non-Hispanic Black (AOR: 1.87; 95% CI: 1.48-2.37) and a college graduate (AOR: 1.28; 95% CI: 1.04-1.58; Table 3).
Intermediary determinants
Adults who reported food insecurity (AOR: 1.25; 95% CI: 1.03-1.53) and housing insecurity (AOR: 1.48; 95% CI: 1.23-1.79) had higher odds of making quit attempt in the past 12 months. On the other hand, adults who reported binge drinking were less likely to try to quit cigarette smoking during the past 12 months (AOR: 0.76; 95% CI: 0.63-0.93) than those not reporting binge drinking (Table 3).
Discussion
This study investigated structural and intermediary determinant factors associated with smoking status and quit attempts using representative, population-based data composed of a large and diverse sample of adults living in 12 US states. The results demonstrate significantly higher odds of current smoking among study respondents who were between 35 and 64 years of age, male, unemployed, reported food insecurity, housing insecurity, frequent mental distress, and binge drinking. Several previous studies have reported similar findings. For example, a study that investigated the relationship between food insecurity and smoking status among Latinos found that a larger proportion of study participants who reported low (25.7%) or marginal (26.4%) food security had higher rates of current smoking than those who reported higher (19.7%) food security. 15 Stahre et al found that adults who reported housing insecurity were more likely to be current smokers than adults who did not report housing insecurity. 14 However, direct comparisons between the current study with past studies are challenging due to the different populations studied and methods used. Specifically, we used population-based survey data that used different scales to define and measure food and housing insecurities. In addition, we assessed a wider range of social determinants including structural and intermediary factors when compared to previous studies.
The findings from our study highlight the influence that social determinants play in continued smoking. This type of information can be used to guide the development of more novel smoking cessation interventions, which have high potential to increase smoking quit rates and reduce tobacco-related disparities. For example, Haas and colleagues 29 conducted a randomized controlled trial evaluating a proactive tobacco treatment approach for adult smokers who were socioeconomically disadvantaged. The treatment included (1) telephone-based motivational counseling, (2) six weeks of free nicotine replacement therapy, (3) access to community-based referrals to address sociocontextual mediators of tobacco use, and (4) integration of all these components into their health care through the electronic health record system. They found that adult smokers in the intervention group who were women, black and white, had low socioeconomic status, and higher than a high school level of education were significantly more likely to quit smoking than the control group. 29
In our study, one of the significant determinants of smoking was mental distress. Like other studies, 18,30 our analysis found that adults with frequent mental distress had higher odds of being a current smoker (rather than being a never or former smoker) than those with infrequent mental distress. However, we did not find a significant association between mental distress and quit attempts. This finding suggests that adults with frequent mental distress might need a more intensive smoking cessation intervention and mental health support to make quit attempts and quit smoking successfully. Thus, screening for mental distress prior to smoking cessation interventions and providing mental health services if needed appear to be important factors that need to be integrated into tobacco control programs. 31
Another important finding of this study was related to the association between binge drinking and smoking status. Compared to adults who did not report binge drinking, adults who reported binge drinking had higher odds of being a current smoker (vs never or former smoker) but lower odds of making a quit attempt. This finding is consistent with previous studies. A recent study found that the prevalence of cigarette smoking was higher (38% vs 18%) and quit rate was lower (49% vs 19%) among adults with alcohol use disorders than those without alcohol use disorder. 32 Tobacco and alcohol use are highly correlated behaviors; therefore, concurrent treatment for tobacco and alcohol use may help to increase the quit rate. Some research found increased smoking abstinence after smoking cessation intervention among individuals also receiving outpatient alcohol treatment 33 and recommend providing smoking cessation intervention concurrent with intensive outpatient alcohol treatment. 34,35 Thus, it might be beneficial to incorporate screening for hazardous alcohol use so that tailored tobacco treatment can be provided for those with comorbid conditions such as dual substance use and/or mental health issues.
It is important to mention that unemployed adults had higher odds of being current smokers than employed adults. This finding is in line with previous studies showing positive association between smoking and unemployment. 13,36 Similar to other studies, 1 we found that men had higher odds of being a current smoker than women. However, we did not find gender differences in quit attempts; this finding is not consistent with current literature. A 2016 study found that men were more likely to make a quit attempt than women. 37 The difference might be due to using different analytical approaches such as controlling for other factors in regression models.
The results of this study indicated that current smokers had higher odds of making quit attempts in the past 12 months if they were non-Hispanic black, graduated college, and reported food and housing insecurities. A recent literature review also confirmed that African Americans were more likely to have made a quit attempt in the past 12 months than whites. 38 Thus, the result of our study underscores the need to consider racial/ethnic background when designing and implementing smoking cessation interventions. Adults who reported food and housing insecurity were more likely to be current smokers than never smokers, as well as more likely to make a quit attempt. This finding confirms that food insecurity and housing insecurity are important factors that influence smoking behaviors. Smokers who have difficulty paying for nutritious meals and housing have a significant financial burden, which may be why we observed higher odds of quit attempts among this population. Our results suggest that race/ethnicity, education level, food insecurity, and/or housing insecurity are motivators for quit attempts. Although making quit attempts is an essential first step to increase smoking cessation rates, 22 it is critical to identify individuals who are motivated to quit smoking so that health-care providers can provide the assistance needed to help them quit smoking successfully for the long term. Taken together, the findings from this study suggest that multifaceted smoking cessation interventions that address food and housing needs as well as incorporate screening for potential comorbidities such as mental distress and/or hazardous alcohol use may be needed to enhance smoking cessation rates among racially diverse adults with lower level of socioeconomic status.
Study Strengths and Limitations
A major strength of this study is its use of a representative, population-based data with a large and diverse sample from 12 US states and entities. Thus, our findings should be generalizable to the adults living in these 12 states. This study has several limitations. Because the food and housing items were administered in only 12 US states and entities, it limits the generalizability of the study results to the overall US adults. Most (72.5%) of the respondents were non-Hispanic whites. The population in the United States is increasingly becoming more racially diverse; therefore, future studies with more diverse sample will be needed. Using cross-sectional data does not allow one to determine whether there were causal relationships between the determinant factors, smoking behavior, and quit attempts that were examined in this study. Additionally, all measures were self-reported, and consequently our findings might be subject to response bias. In tobacco-related research, using biochemical verification of smoking status is recommended to minimize the risk of underestimating smoking prevalence. 39 The BRFSS used 1 item to measure food insecurity and 1 item to measure housing insecurity. Future longitudinal studies are needed to test these relationships using valid and reliable multi-item scale to measure food insecurity and housing insecurity. In addition, food and housing insecurities were measured at the individual level. Thus, the possibility of misclassification bias was decreased compared to studies that measured food and housing insecurities at the household level.
Conclusions
This large, representative, population-based study identified significant determinant factors associated with smoking status and quit attempt. The findings underscore the need to screen for mental distress, alcohol use, food insecurity, and housing insecurity during health-care provider office visit that will help to identify target populations for multifaceted interventions such as addressing tobacco and alcohol use. Also, they will help to identify individuals who might need referral to a mental health-care provider and food and housing assistance referrals. For example, health-care providers can refer individuals to federal-funded and state-funded food programs such as Special Supplemental Nutrition Assistance Program. 40 Tobacco control, subsidized housing, and food programs might be an important means for improving smoking cessation rates and overall health.
So What? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
Previous studies have examined the relationships between isolated social determinant factors associated with smoking such as sociodemographic, psychosocial, or behavioral factors alone. However, a broader range of social and structural determinant factors that might be associated with smoking behaviors have not been studied at the population level and may have implications for creating innovative smoking cessation interventions.
What does this article add?
This study extends the literature by examining the relationships among intermediary determinants, structural determinants, and adult smoking status and quit attempts using representative, population-based data with a large and diverse sample. Our results showed that current smoking was greater among those who were between 35 and 64 years of age, male, unemployed, reported food insecurity, housing insecurity, had frequent mental distress, and reported binge drinking. In addition, race/ethnicity, education level, food insecurity, and/or housing insecurity were motivators for quit attempts.
What are the implications for health promotion practice or research?
Providing multifaceted smoking cessation interventions that address food and housing needs as well as incorporate screening for comorbidities such as mental distress and/or hazardous alcohol use may be needed to enhance smoking cessation rates among racially diverse adults with lower level of socioeconomic status. Future research testing innovative strategies that incorporate a tailored smoking cessation intervention addressing these important social determinants of health along with evidence-based tobacco treatment using pharmacotherapy and behavioral counseling are suggested to assess the impact on improving cessation rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.