
Abstract
Purpose:
The Healthy Food Financing Initiative (HFFI) aims to expand access to healthy foods in low-resourced communities across the United States. This study examined changes in food and beverage availability and marketing in nearby small food stores after the opening of an HFFI-supported supermarket in a predominately low-income and African American community.
Design:
Natural experiment.
Setting:
Rockford, Illinois.
Participants:
A full audit was conducted of the small grocery and limited service stores located in a 1-mile radius around the new supermarket (N = 22) and a 1-square mile area within a nearby demographically matched comparison community (N = 18). Stores were audited in 2015 (1 month preopening) and 2016 (1 year afterward).
Measures:
Store characteristics, item availability, and interior and exterior promotions/advertisements were examined.
Analysis:
Difference-in-difference (DID) regression models assessed pre- and postintervention changes in availability and marketing between small food stores in the intervention and comparison communities.
Results:
The DID regression models indicated no difference between intervention and comparison communities with respect to changes in availability and marketing of all food items with the exception of frozen vegetables which had higher availability postintervention in the comparison community versus intervention (β for interaction term = .67; standard error: 0.33; P = .04).
Conclusion:
After the opening of the HFFI-supported supermarket, food and beverage availability and marketing in nearby small food stores did not change significantly. However, the wide range of staple foods offered by the supermarket contributed to the expansion of healthy food retail in the intervention community.
Purpose
In the United States, research shows that living in a community with limited availability of healthy food is associated with increased risk of poor dietary intake and chronic diseases such as obesity. 1,2 Communities with limited healthy food availability are often majority African American and low income. 3 -6 Strategies to increase availability of healthy foods in these communities are in high demand at the federal, state, and local levels. 7 -11
In 2011, the federal government announced the Healthy Food Financing Initiative (HFFI), a multimillion dollar collaborative effort to expand healthy food retail in urban and rural areas of the United States that are considered food deserts by the US Department of Agriculture. 12,13 Since its establishment, the HFFI has provided financial and technical assistance to communities, organizations, and businesses across the country in an effort to (1) build new food retailers (eg, supermarkets and farmers markets) and (2) increase the amount of healthy foods offered by existing small food retailers (eg, convenience stores). 13
The Illinois Fresh Food Fund received funding from the HFFI in 2012 to build a new chain supermarket in Rockford, Illinois—a midsize city approximately 90 miles northwest of Chicago. 14 The location selected for the new HFFI-supported supermarket is directly west of the downtown area in a low-income neighborhood that lacked a supermarket for nearly 30 years. 14 The purpose of this natural experiment is to evaluate the extent food and beverage availability and marketing changes in Rockford, Illinois, after the opening of the HFFI-supported supermarket. To accomplish this aim, we assessed food and beverage availability and marketing in the existing small food stores that surround the new supermarket before its opening and 1 year after.
Currently, there is limited information in the scientific literature on the impact that a new chain supermarket has on the retail food environment in a food desert. 15 -17 Existing retailers may alter their food and beverage offerings and advertisements for the better (ie, they may increase their supply and promotion of healthy staple foods like fruits and vegetables) or the worse (ie, they may increase their supply and promotion of unhealthy foods like snacks and sweetened beverages) in response to increased competition from the new supermarket. These changes to the stocking practices of existing food retailers are important to study because they may have significant consequences on the diet and diet-related behaviors of community residents over time. 18,19 Thus, the current study will contribute to our knowledge of whether and how the retail food environment in low-resourced communities may change following the introduction of an HFFI-supported supermarket in terms of the availability and marketing of staple food items (eg, milk, bread, fruits, and vegetables) and other items (eg, snacks, sugar-sweetened beverages [SSBs]) in the existing small food retailers that surround the HFFI-supported supermarket. This research is guided by the Nutrition and Obesity Policy Research and Evaluation Network’s policy research and evaluation framework. 20 The framework suggests that policy initiatives, such as the HFFI, directed at one component of the physical, social, or economic environment may impact another environment. 20 Thus, we hypothesize that significant changes to food availability and marketing will be observed 1 year after the opening of the HFFI-supported supermarket in west Rockford, Illinois.
Methods
Community Selection and Data Collection
We collected data from small food stores in 2 Rockford, Illinois, communities—the community in west Rockford where the HFFI-supported supermarket is located and a demographically matched comparison community in south Rockford that also lacked a supermarket. The HFFI-supported supermarket opened for business at the end of August 2015. We collected baseline data in August 2015 just prior to the store opening; follow-up data were collected in August 2016, 1 year after the store opening. At baseline, 48% of the residents in the 1-mile radius of the HFFI-supported supermarket were African American and 47% lived below the federal poverty line. In the demographically matched comparison community, 40% of the residents were African American and 46% lived below the federal poverty line.
Trained study staff performed a complete audit of all small grocery stores and limited service stores (ie, convenience stores, gas stations, pharmacies, liquor stores, dollar/discount stores) found within a 1-mile radius of the new HFFI-supported supermarket in west Rockford. Study staff also audited the same types of stores found within a 1-square mile area of the demographically matched comparison community in south Rockford.
The Illinois Prevention Research Center’s (Illinois PRC) Food Store Audit Tool, which was adapted from the Bridging the Gap Food Store Observation Form, was used to collect food and beverage availability and marketing data from the new HFFI-supported supermarket and all food stores found during the audit. 21 Detailed information about the validity and reliability of the Illinois PRC Food Store Audit Tool is available elsewhere. 22 To summarize, the tool includes over 600 items that measure general store features, food and beverage availability, interior store item promotion, and exterior store item advertisement. Among the food and beverage items included on the tool are a variety of fresh fruits and vegetables, canned/shelf-stable foods, breads, cereals, fresh meat, dairy products, SSBs, and snack items (eg, candy, chips, and prepackaged baked goods). The institutional review board at University of Illinois at Chicago determined that this was nonhuman subjects research.
Measures
General store features
Information on the following store features was recorded for each store: store type, Supplemental Nutrition Assistance Program (SNAP) authorization status, number of cash registers, food service counter availability, and availability of on-site parking. Stores were classified as either a small grocery store or a limited service store. A store was considered a small grocery store if it sold fresh meat. Stores classified as a limited service store were further categorized as a convenience store, pharmacy, liquor store, or dollar/discount store. Additionally, gas stations were classified as convenience stores. Stores that sold convenience food items and prescription medications were considered a pharmacy. Over 50% of a store’s inventory had to be alcohol products for it to be considered a liquor store, and a large selection of nonfood items such as clothing, gifts, decorations, small furniture, and household cleaning products had to be sold for a store to be considered a dollar/discount store.
Study staff scanned the interior and exterior of each food store to find signs indicating the store was authorized to accept SNAP benefits. If no signs were found, study staff were instructed to ask a manager, or store employee, about the acceptance of SNAP benefits. The number of available cash registers was recorded. Self-checkout terminals and unused registers counted toward the total; lottery terminals and registers located at the makeup counter, pharmacy, or photo counter did not count toward the total. Study staff recorded yes or no if a butcher counter, bakery counter, or deli service counter were available and if the store had on-site off-street parking.
Food and beverage availability
Food and beverage availability information was collected from all small food stores before and after the opening of the HFFI-supported supermarket. Furthermore, availability of food and beverages was assessed at the HFFI-supported supermarket after the opening. Study staff counted and recorded the number of fresh fruit options, fresh vegetable options, frozen fruit options, frozen vegetable options, canned fruit options, and canned vegetable options in each store. After surpassing 20 options, study staff stopped counting and recorded 20+ for fresh fruit and vegetable options. They stop counting frozen and canned fruit and vegetable options after surpassing 10 options and recorded 10+. An “option” denoted a particular fruit or vegetable item, for example, apples, bananas, and oranges were considered different fresh fruit options.
Other food items assessed include the following: 100% whole wheat bread, white bread, low-sugar cereal (<6 g of sugar per serving), regular cereal (≥6 g of sugar per serving), brown rice, white rice, lean ground beef (≤10% fat), regular ground beef (>10% fat), reduced-fat cheese, regular cheese, low-fat chips (<4 g of fat per serving), and regular chips (≥4 g of fat per serving). Packaging for bread had to have the words “100% whole wheat” on it to count toward the availability of that item. An item counted toward reduced-fat cheese availability if the packaging included the words “reduced-fat” or “part-skim.”
Among the beverages examined were milk, soda, and juice. Study staff recorded yes or no if the store had low-fat milk (ie, skim or 1%), regular milk (ie, whole or 2%), diet soda, regular soda, 100% juice, and/or juice drink (<50% juice). For milk availability, only unflavored cow’s milk was considered. Packaging for soda had to have the words “diet” or “zero-calorie” on it for the item to count toward diet soda availability; packaging for juice had to have to words “100% juice” on it for the item to count toward 100% juice availability.
Interior and exterior store marketing
Interior and exterior store marketing of certain foods and beverages was examined at each small food store before and after the opening of the HFFI-supported supermarket. Also, marketing of foods and beverage was examined at the HFFI-supported supermarket after its opening. Study staff recorded yes or no if the following items were available in the checkout area: fresh fruit, fresh vegetables, unflavored cow’s milk, plain bottled water, regular soda, diet soda, other sweetened beverages, salty snacks, candy, and sweetened baked goods. Both self-serve items (items the customer can pick up) and clerk-assisted items (items behind a counter that the store clerk must hand to the customer) counted toward items available at checkout. Other sweetened beverages referred to juice drinks, fruit punch, ready-to-drink coffees, ready-to-drink teas, lemonade, and so on. Salty snacks referred to chips, popcorn, crackers, salted nuts, jerky, and so on. Items such as snack cakes, donuts, muffins, and cookies were considered sweetened baked goods.
Study staff scanned the interior of the food store to record yes or no if the same food and beverage items assessed in the checkout area were being promoted on a special floor display or an end-aisle display. Special floor displays were defined as stand-alone interior store displays that advertise for a particular food or beverage. These displays often force customers to walk around them. They include bins, items arranged for display on a table, and items arranged for display on the floor. End-aisle displays were defined as displays of foods or beverages that appear on the endcap of a store aisle. All endcaps in the middle of an aisle, facing toward the front of the store, and facing away from the front of the store were examined. If an item was being promoted on a special floor display or an end-aisle display, the store was considered to have an interior store promotion for that particular item.
Study staff collected information on the exterior store advertisement of specific foods and beverages. Separate counts for the number of ads featuring the following items were recorded: fresh fruits and vegetables, regular soda, diet soda, energy drinks, sports drinks, and unflavored milk. Furthermore, separate counts for the numbers of ads featuring any food item and any beverage item were also recorded. These counts include ads appearing on the building exterior and the store property (eg, in the parking lot, gas pumps, fencing). Ads smaller than a standard sheet of paper (8 in × 10 in) were not counted.
Statistical Analysis
Data analyses were performed with STATA version 9.4. Means and frequencies were calculated to examine baseline food store features among all stores, by food store type (small grocery vs limited service) and by store location (HFFI vs comparison). Chi-square and t tests were used to identify statistically significant differences in baseline store features between small grocery stores and limited service stores. Means and frequencies were calculated for measures of food availability and marketing among all small food stores before the opening of the HFFI-supported supermarket (preintervention) and 1 year after the store opening (postintervention). Difference-in-difference (DID) regression models were used to identify significant differences in the change in food and beverage availability and marketing pre- to postintroduction of the HFFI-supported supermarket between small food stores in the intervention community and small food stores in the comparison community. The DID regression models were adjusted for food store type. The availability and marketing of foods and beverages at the HFFI-supported supermarket were examined and reported; data collected from the supermarket were not included in the DID regression models. P values less than .05 were considered statistically significant.
Results
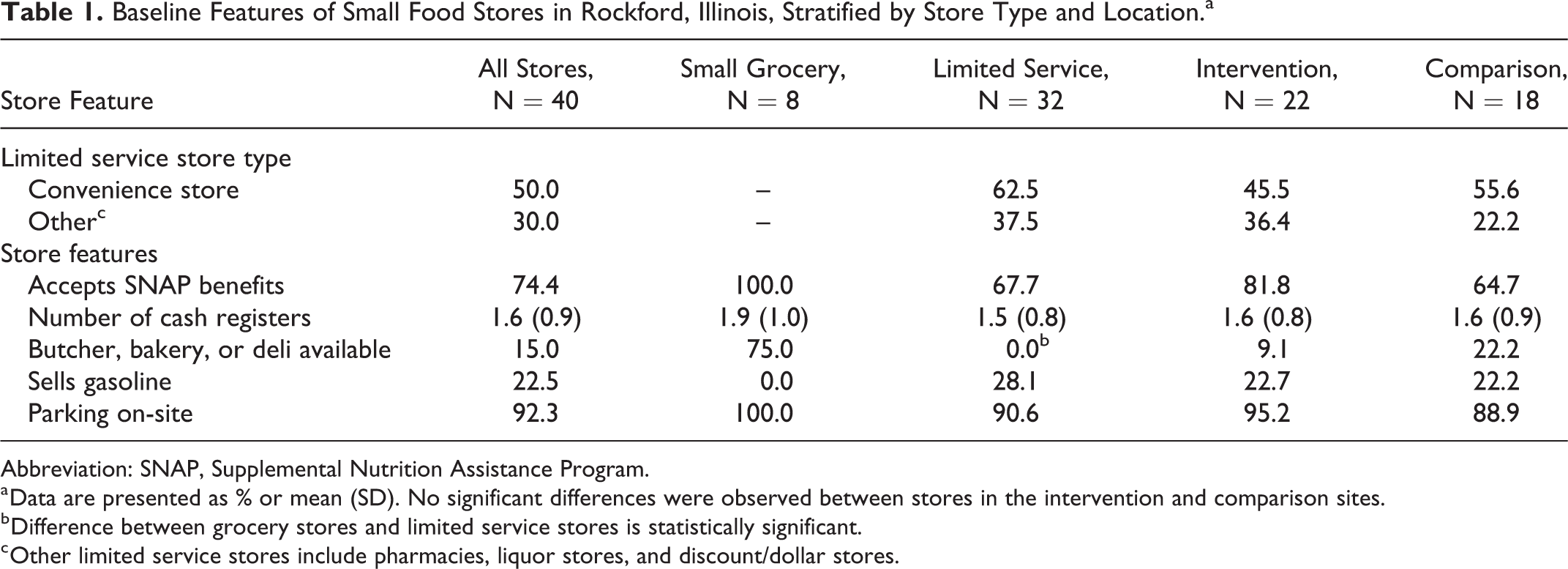
Table 1 displays information on the baseline features of the small food stores in Rockford, Illinois that were found during the audit. Data were collected from 22 small food stores in the intervention community and 18 small food stores in the comparison community (N = 40). Of the 40 stores examined, 8 were classified as small grocery stores and 32 were classified as limited service stores. While most limited service stores were convenience stores, 37.5% of them were classified as a pharmacy, liquor store, or dollar/discount store. All small grocery stores were authorized to accept SNAP benefits, while 67.7% of limited service stores were SNAP authorized. The baseline features of stores in the intervention community were similar to stores in the comparison community.
Baseline Features of Small Food Stores in Rockford, Illinois, Stratified by Store Type and Location.a
Abbreviation: SNAP, Supplemental Nutrition Assistance Program.
a Data are presented as % or mean (SD). No significant differences were observed between stores in the intervention and comparison sites.
b Difference between grocery stores and limited service stores is statistically significant.
c Other limited service stores include pharmacies, liquor stores, and discount/dollar stores.
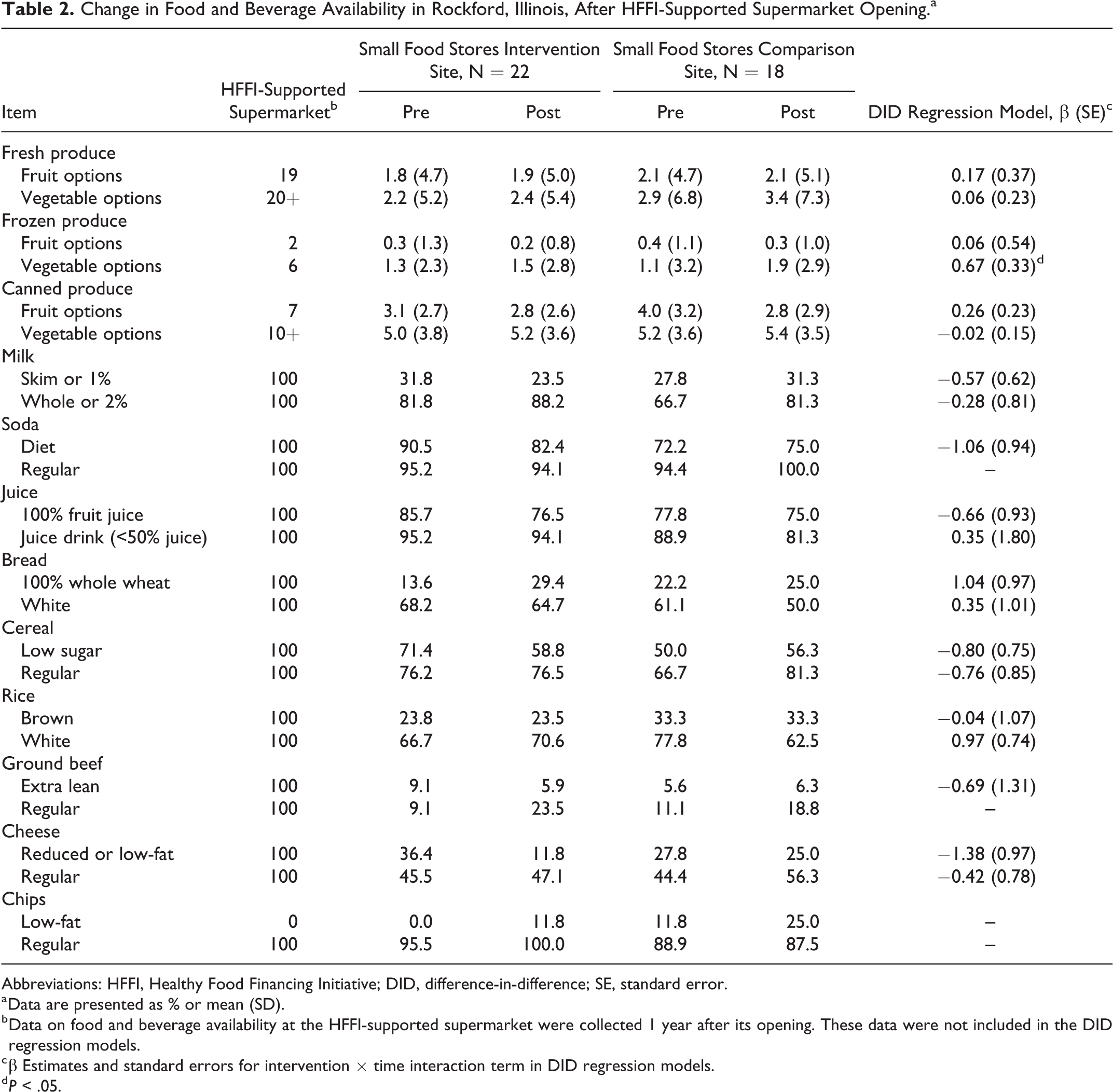
Table 2 details the food and beverage availability of the HFFI-supported supermarket and the small food stores included in the audit pre- and postintervention. Data from the small food stores are presented at baseline and 1 year after the opening of the HFFI-supported supermarket. The HFFI-supported supermarket carried about 20 fresh fruit and vegetable options. One year after the supermarket’s opening, small food stores in the intervention community carried, on average, about the same number of fresh, frozen, and canned fruit and vegetable options as they did at baseline with the exception of frozen vegetables. Results from the DID regression models suggested the number of frozen vegetable options observed between the intervention and comparison community increased by an average of 0.67 items between baseline and follow-up (standard error = 0.33; P < 0.04). No other significant differences in the availability of fruit and vegetables pre- to postopening of the HFFI-supported supermarket were observed.
Change in Food and Beverage Availability in Rockford, Illinois, After HFFI-Supported Supermarket Opening.a
Abbreviations: HFFI, Healthy Food Financing Initiative; DID, difference-in-difference; SE, standard error.
a Data are presented as % or mean (SD).
b Data on food and beverage availability at the HFFI-supported supermarket were collected 1 year after its opening. These data were not included in the DID regression models.
c β Estimates and standard errors for intervention × time interaction term in DID regression models.
d P < .05.
The HFFI-supported supermarket carried every food and beverage item of interest except low-fat chips. The percentage of stores in the intervention community carrying specific staple food items, such as milk, bread, and cereal, did not change 1 year after the supermarket’s opening. The percentage of stores carrying healthier items such as low-fat milk and 100% whole wheat bread continued to be low compared to those carrying convenience items such as chips and regular soda. The DID regression models indicated there was no significant difference in the change in food and beverage availability over time between the intervention and comparison communities.
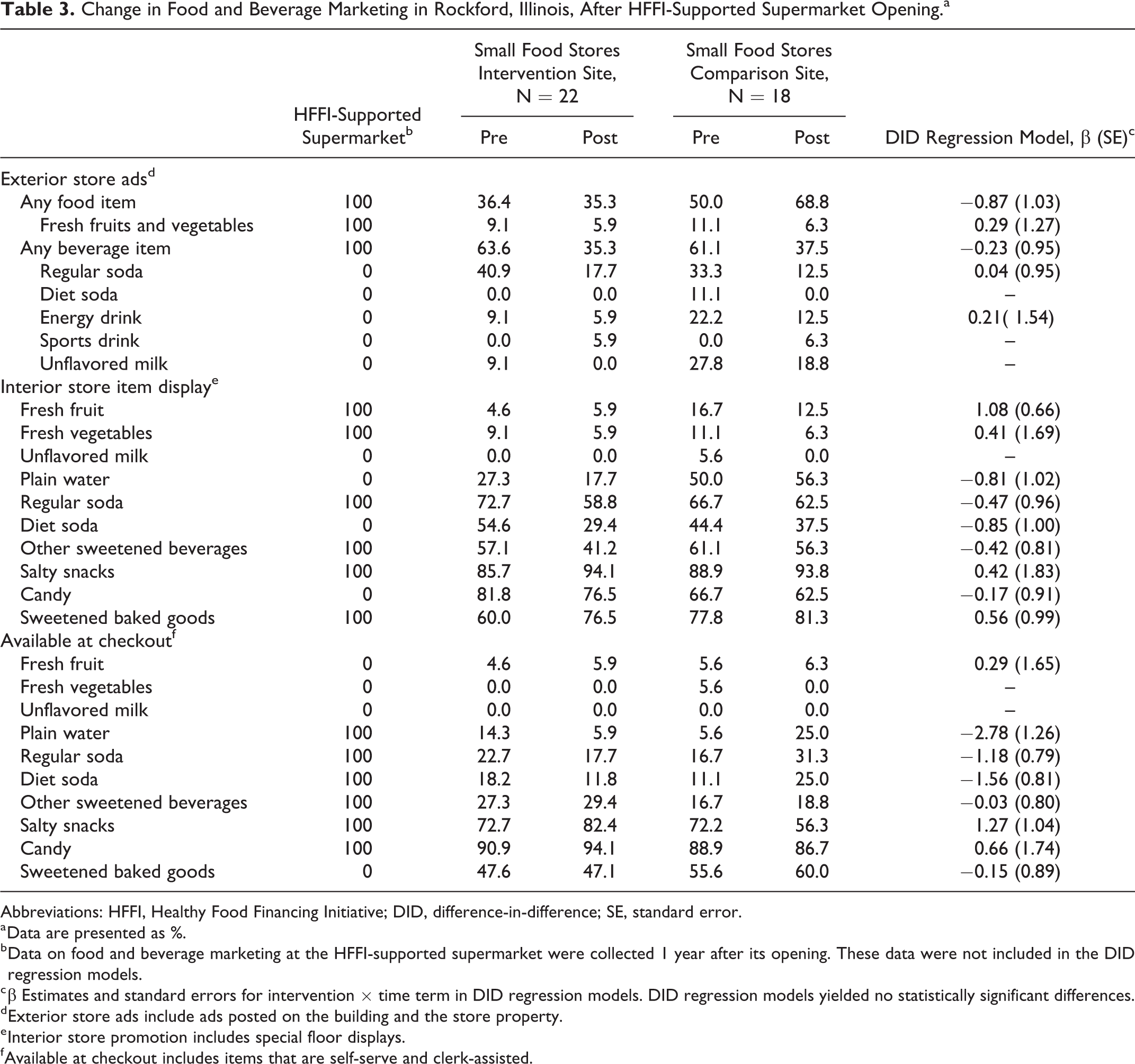
Pre- and postintervention information on food and beverage marketing in the HFFI-supported supermarket and the small food stores included in the audit is provided in Table 3. The HFFI-supported supermarket did not have fresh fruit or vegetables available at checkout; however, we did find interior store item displays and exterior store ads for fresh fruit and vegetables. Regular soda and salty snacks were available at checkout and promoted via an item display inside the HFFI-supported supermarket. There were no exterior store ads for regular soda or any other SSB at the supermarket.
Change in Food and Beverage Marketing in Rockford, Illinois, After HFFI-Supported Supermarket Opening.a
Abbreviations: HFFI, Healthy Food Financing Initiative; DID, difference-in-difference; SE, standard error.
a Data are presented as %.
b Data on food and beverage marketing at the HFFI-supported supermarket were collected 1 year after its opening. These data were not included in the DID regression models.
c β Estimates and standard errors for intervention × time term in DID regression models. DID regression models yielded no statistically significant differences.
d Exterior store ads include ads posted on the building and the store property.
e Interior store promotion includes special floor displays.
f Available at checkout includes items that are self-serve and clerk-assisted.
Among the small food stores located in the intervention community, the marketing of fresh fruits and vegetables did not change between baseline and the follow-up assessment. Less than 10% of these stores promoted fresh fruits or vegetables on the interior or exterior of the store at follow-up. On the other hand, the percentage of food stores with interior store promotions of regular soda, salty snacks, candy, and sweetened baked goods continued to be high at follow-up. The DID regression models indicated there were no statistically significant changes in food and beverage marketing over time between stores in the intervention community and stores in the comparison community.
Discussion
This research aimed to examine how the retail food environment in a low-resourced community in Rockford, Illinois, changed 1 year after it received a new HFFI-supported chain supermarket. To accomplish this aim, we assessed food and beverage availability and marketing in the small food stores that surrounded the new supermarket and small food stores located in a nearby comparison community that also lacked a supermarket. We hypothesized that food and beverage availability and marketing would change among the small food stores in the intervention area after the opening of the HFFI-supported supermarket. Results showed that no changes occurred 1 year after the supermarket’s opening, with the exception of a small increase in availability of frozen vegetables in small food stores in the intervention versus comparison area.
The net availability of healthy foods could have increased in the nearby small food stores if they intended to compete with the HFFI-supported supermarket that offers a wide array of healthy food items. On the other hand, the availability and marketing of unhealthy items could have increased if the small stores decided to focus their market on that niche and not compete for the sales of staple food items. Overall, we found that the availability and marketing of healthy and unhealthy foods and beverages did not change between baseline and the 1 year follow-up period. One explanation for these null findings is that customers use supermarkets and small food stores for different types of shopping. Small food stores may be used primarily to purchase small convenience items (eg, candy, snacks, sweetened beverages), while supermarkets are used to perform major shopping and purchase staple food items. Another potential explanation for these findings is the small sample size of food stores found during the audit. Our ability to observe statistically significant differences between the intervention and comparison community may have been hindered due to a lack of statistical power. Furthermore, we only conducted one follow-up assessment after the opening of the HFFI-supported supermarket. Additional follow-up periods may have been needed to observe meaningful changes to healthy and unhealthy food retail in the intervention community.
Scientific evidence on the impact of a large chain supermarket on the retail food environment in a low-resourced community is scarce. Research on this subject has only become available in the past year. 15 Ghosh-Dastidar and colleagues conducted a similar study where they examined the impact of a new HFFI-supported grocery store on food availability and pricing in a predominately low-income and African American community in Pittsburgh, Pennsylvania. 15 They found no change in the net availability of healthy foods in neighboring food stores after the grocery store’s opening. 15 Similar study limitations were reported; a small number stores (N = 24) were found during the audit and only one assessment period was conducted after the grocery store opened. 15 Our study extends this prior study by testing for changes in food and beverage marketing in addition to availability.
Economic research on the effects of introducing a supercenter, such as Wal-Mart or K-Mart, to an area that previously lacked this type of outlet sheds some light on this topic. 16,17 A study conducted by Jia concluded that when a Wal-Mart or K-Mart enters a market, the nearby smaller discount stores often become unprofitable because they are unable to compete with the supercenter’s discount prices. 16 Furthermore, an analysis of household-level panel data collected by Hausman and Leibtag reported that the average price paid by households for specific staple food items decreased after the supercenter’s opening. 17 Unlike these studies, we found no evidence to support that the introduction of a new chain supermarket results in a significant number of nearby store closings. Considering a major product of the HFFI has been the development of new supermarkets and grocery stores in low-resourced areas, more research is needed to better understand the influence these food retail outlets are having on the retail food environment in the United States. Future studies should consider the limitations of the current study reported below.
It is important to note that the new HFFI-supported supermarket in west Rockford offered a large supply of fresh fruit and vegetables and other staple food items. At follow-up, the existing small food stores near the supermarket carried few fresh fruit and vegetable options, and a low percentage of stores stocked low-fat milk and 100% whole wheat bread. Snack items and SSBs were prevalent in all stores at follow-up. Other studies have documented low availability of staple foods and beverages in small food stores located in predominately low-income and minority communities. 23 -28 The addition of the HFFI-supported supermarket contributed to an overall increase in the supply of healthy food and beverage items in west Rockford.
The role of food and beverage marketing on the obesity epidemic in the United States has gained much attention in recent years. 28,29 Studies have reported disproportionate interior and exterior store marketing of unhealthy food and beverage items between food stores in low-income and higher income communities and have linked interior and exterior store advertisement of unhealthy food items to increased odds of obesity among nearby community residents. 30 -35 In the current study, less than 20% of small food stores in both communities had exterior store ads or interior store promotions for fresh fruit, fresh vegetables, or unflavored milk at follow-up. On the other hand, fresh fruits and vegetables were marketed via exterior store ads and interior store item displays at the new HFFI-supported supermarket. Therefore, the HFFI-supported supermarket also contributed to the marketing of healthy foods and beverages in west Rockford.
This research has strengths and limitations. A key strength to this research was the data collection approach. A complete audit of all small food stores in the intervention and comparison communities was conducted. This permitted the collection of data on the availability and marketing of several foods and beverages. As mentioned before, the limited number of follow-up assessments and the small sample size of food stores found during the audit were the key limitations of this research. Price data on a select number of food and beverage brands and package sizes were collected, but the small sample sizes of food stores carrying these items prevented our ability to assess difference in price change among small food stores between baseline and the 1-year follow-up assessment. It is important to note that this study focused solely on food and beverage availability and marketing in Rockford, Illinois; results might not be generalizable to the retail food environment in other geographic areas. Furthermore, because no individual-level data were collected from community residents, we are unable to determine how food purchasing behavior changed in the intervention community after the introduction of the HFFI-supported supermarket.
So What?
Changes to food and beverage availability and marketing among small food retailers have implications for health promotion and community nutrition because the food purchasing behavior of community residents may be affected. 18,19 Overall, we observed that food and beverage availability and marketing did not significantly change in existing food stores in the intervention community 1 year after the supermarket’s opening. Although the small store food retail environment did not change during this time period, it is important to acknowledge that the HFFI-supported supermarket contributed to the expansion of healthy food retail in the intervention community. The availability and marketing of fresh fruits and vegetables, and staple food items such as milk, bread, and ground beef, has improved because of the supermarket’s presence. Future research in this area should evaluate the long-term effects of a new chain supermarket on food availability, price, and promotion in nearby food stores as well as individual-level factors such as dietary intake and food purchasing behavior.
The current study contributes to the growing literature on the impact of large-scale state and federal initiatives to increase healthy food retail in the United States. 36 -44 While our project solely focused on changes to the retail food environment, studies documenting how the introduction of a new supermarket or grocery store influences factors such as body mass index, dietary intake, food purchasing behavior, and perceived access to healthy food among nearby community residents have been published. 36 -42 Overall, the evidence supporting the premise that adding a large supermarket or grocery store to a low-income neighborhood results in significant changes at the individual level is mixed. A study by Dubowitz and colleagues observed that regular use of a new grocery store in a low-income neighborhood in Pittsburgh was significantly associated with improvements in perceived access to healthy food. 38 Improvements in diet quality were reported, but these improvements were not associated with use of the new grocery store. 38 Cummins and colleagues reported that introducing a new grocery store to a low-income community in Pennsylvania did not improve weight status or fruit and vegetable intake. 39 Furthermore, Rogus and colleagues found that eating at home increased and SSB consumption decreased among community members in a low-income New York neighborhood that received a new supermarket. 42 As the HFFI continues to yield positive change to the retail food environment in low-resourced communities, more research will be needed to better understand the long-term economic and public health effects at the individual and community levels.
Footnotes
Authors’ Note
L.M.P., S.N.Z., and A.O.Y. conceptualized this research project. C.R.S., Y.L., and L.M.P. were involved in developing the statistical analysis plan. Y.L. performed the data analysis. C.R.S. lead the drafting of the manuscript. All authors participated in editing the manuscript. All authors reviewed and approved the final version of the manuscript prior to submission for publication. This study was conducted according to the guidelines laid down in the Declaration of Helsinki. This research was deemed nonhuman subjects research by the institutional review board at the University of Illinois at Chicago. Chelsea Singleton is now an Assistant Professor in the Department of Kinesiology and Community Health at the University of Illinois at Urbana-Champaign. She can be reached at (217) 300-8139. Email:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this manuscript was supported by the Centers for Disease Control and Prevention (grant number 5U48DP005010) and the National Cancer Institute of the National Institutes of Health (CS, grant number R25CA057699).