
Abstract
Purpose:
To examine differences in physical activity (PA) uptake between black and white employees during a financial incentive-based workplace intervention.
Design:
Prospective cohort study from July 2014 to June 2015 (NCT02850094).
Setting:
Tertiary academic medical center.
Participants:
Forty-three black and 182 white nonclinical employees.
Intervention:
Participants self-selected or were assigned to teams. Participants completed a 24-week intervention receiving rewards for meeting weekly PA goals (increasing moderate-to-vigorous PA [MVPA] by 10% from previous week or meeting Guidelines threshold of 150 minutes of MVPA).
Measures:
Outcomes included weekly MVPA in minutes, average daily step counts, number of weeks meeting personal goals and the Guidelines, and Fitbit adherence in days and weeks.
Analysis:
We performed an analysis of covariance for each outcome, with race as the primary independent variable of interest, adjusting for demographic and health-related covariates.
Results:
During the intervention, blacks walked 9128 steps per day while whites walked 7826 steps per day, a difference of approximately 1300 steps (P < .05). Blacks also demonstrated a greater uptake in both steps and MVPA from baseline than did whites, resulting in similar MVPA throughout the intervention.
Conclusions:
Findings suggest that workplace PA interventions using financial incentives may result in similar engagement in MVPA among white and black employees, while black employees walk more steps during the intervention. Limitations include a primarily white female sample which may not generalize.
Purpose
Regular physical activity (PA) has been found to reduce the risk of chronic health conditions including but not limited to cardiovascular disease, diabetes, cancer, hip fractures, high blood pressure, and obesity. 1,2 Despite the abundant evidence of the health benefits associated with regular PA, 3 –5 more than half of Americans fail to meet the Physical Activity Guidelines for Americans, 2nd Edition (ie, the Guidelines) recommending 150 minutes per week of moderate-intensity PA or 75 minutes per week of vigorous-intensity aerobic PA or an equivalent combination. 6 –8 Furthermore, PA patterns differ by race. According to the Healthy People 2010 Final Review, black individuals engage in less moderate-to-vigorous physical activity (MVPA) than whites and are less likely to participate in any form of leisure-time PA.9 Such racial differences in PA may contribute to the racial disparities in the prevalence of chronic health conditions. Black individuals have a higher prevalence of hypertension, stroke, diabetes, kidney and bladder problems, and stomach ulcers than do whites. 10 As a result, they live for fewer years than any other racial/ethnic group and live for more years with chronic health problems. 11
While workplace wellness programs are generally effective in improving PA, nutrition, reducing body weight, and reducing health-care costs, 12 –18 heterogeneity in specific outcomes may be related not only to differences in the interventions (eg, nutrition, PA, or both) and outcomes measured (eg, weight loss, adherence to nutrition guidelines, and PA) but also to individual differences in the people participating in these programs. Due to the black/white differences in overall PA, 9 one may posit that uptake in PA resulting from workplace wellness interventions may also differ between black and white employees.
Furthermore, variability in the design of workplace wellness programs may lead to the variability in specific outcomes. For example, financial incentive models have been shown to be effective for improving PA, 16,19,20 but these effects seem to differ for individual- versus team-based interventions with team-based interventions proving more effective than individual interventions. 19,21,22 However, it remains unclear how team formation (ie, choosing your teammates or being assigned a team) impacts the effects of workplace wellness programs aimed to improve PA. Moreover, given the known black versus white differences in cooperative and competitive behavior, black participants may be more likely to form a team, thus capitalizing on the opportunity for cooperation. 23 It is therefore also important to identify how team formation may differ among black and white employees.
In summary, there is evidence supporting the effectiveness of workplace wellness programs in improving PA 14,16 ; however, it is unknown whether the outcomes of such programs differ between black and white employees. Further, the design characteristics of the intervention, such as team formation, may also differ between these racial groups. By better understanding whether there is differential effectiveness of such programs among blacks and whites, we can better tailor workplace wellness interventions to meet the needs of employees. The current study examined black versus white differences in PA uptake during a financial incentive-based workplace wellness program aimed to increase PA (B-Well). As a secondary objective, we examined the interaction between black versus white race and team formation on the uptake PA.
Methods
Design
Data were collected as part of the B-Well initiative, a prospective cohort study conducted from July 2014 to June 2015 at Brigham and Women’s Hospital, a tertiary academic medical center in Boston, Massachusetts. The B-Well study consisted of a 26-week program that included 24 weeks of financial incentives aimed to increase PA among insufficiently active hospital employees.16 This study was approved by the Partners Healthcare Institutional Review Board (Protocol #P2014P000970).
Sample
Eligible participants were nonclinical employees (ie, could not be physicians, nurses, physical therapists, or clinical psychologists) who reported ≤30 minutes of exercise per week prior to program inception, had access to a computer, and were at least 21 years of age. For the purposes of this analysis, only participants who reported white/caucasian or black/African American race were included. All data were collected from July 2014 to June 2015.
Eligible participants either formed a 3-person team of their choice or were paired with 2 other participants by research staff based on common departments, divisions, office locations, or positions to form a team. Participants met as a team with research staff to review the study protocol, the PA monitoring schedule, and financial incentive detail. During this meeting, participants were also given a commercial accelerometer, the Fitbit Flex (Fitbit Inc, San Francisco, California), and instructed on how to use it. All participants also provided informed consent.
Measures
At this baseline visit, participants underwent a health screening that included measurements of the height and weight (used to calculate body mass index [BMI] 24 ), blood pressure, and pulse. Participants then completed an online survey containing questions related to their general health including frequency of health-care utilization, self-reported comorbidities including heart disease, hypertension, diabetes, osteoarthritis and others, medications used, and smoking status. Participants reported their sex, age, education, and household income via a demographic questionnaire. Participants also completed the Monetary Choice Questionnaire, a 27-question survey for the measurement of delay discounting. 25 Delay discounting is a measure of impulsivity describing whether persons place higher value on immediate smaller rewards than delayed larger rewards. 26 –28
Intervention
The first 2 weeks of the program were spent in an introductory period, where participants earned monetary rewards for wearing their Fitbit as instructed. Following these first 2 weeks, participants could earn monetary rewards during each of the 24 subsequent intervention weeks for either increasing their time spent engaging in MVPA by at least 10% from the preceding week (ie, meeting their personal goal) or by meeting the Guidelines for MVPA (ie, at least 150 minutes of moderate PA). If all team members successfully met their personal or Guidelines MVPA goals, each individual’s reward was doubled that week. Participants received individualized weekly e-mails throughout the intervention detailing the time spent engaging in MVPA during the previous week, their new weekly goal (10% increase in MVPA), and their recent rewards. Participants could also view their step count via the Fitbit website but were unable to receive real-time feedback regarding minutes of MVPA per week. Please refer to Losina et al (2017),16 Losina et al (2017),29 and Smith et al, (2017)30 for the detailed structure of the financial incentives.
During the intervention, valid days of data were determined as those with at least 10 hours of recorded accelerometer activity, while valid weeks consisted of at least 4 days of valid Fitbit wear. 31 –33 Physical activity outcomes were calculated only for valid days or weeks. We then calculated the average number of minutes spent in bouts of MVPA. Details of MVPA calculation have been reported previously. 16,29,30 We also averaged daily step count across interventions weeks. Then, we measured Fitbit adherence by counting both the number of valid days and the number of valid weeks of Fitbit wear. Finally, we calculated the number of weeks participants met either their personal MVPA goals (a 10% increase in minutes of MVPA from the previous week) or the Guidelines MVPA goal.
Analysis
Our primary outcomes of interest were as follows: (1) average weekly MVPA, (2) average daily step count, (3) valid Fitbit wear days, (4) valid Fitbit wear weeks, (5) number of weeks meeting the Guidelines MVPA goal, and (6) number of weeks meeting their personal MVPA goal. To examine black versus white differences in baseline demographic and health-related variables (ie, sex, age, education, household income, BMI, comorbidities, blood pressure, medications, smoking status, delay discounting, and team formation), we conducted χ2 tests for categorical variables and t tests for continuos variables. We used Pearson correlations and analyses of variance to assess the bivariate associations between primary outcomes and the abovementioned demographic and health-related variables as potential covariates advanced to our multivariate model. Finally, we conducted a 2 × 2 analysis of covariance (ANCOVA) to examine the main effects of black versus white race and team formation as well as the interaction between black versus white race and team formation for each outcome. Covariates that were significantly associated with black versus white race as well as with outcomes at the P ≤ .05 were included in each ANCOVA model. Final models only included significant interaction effects. As a sensitivity analysis, we included the following covariates in each model: age, sex, education, income, delay discounting, and BMI. All statistical analyses were done in SAS 9.4.
Results
Sample Characteristics
Three hundred participants were enrolled in the study. However, 75 were excluded from the current analyses for identifying as a race other than white or black (Hispanic [n = 21], Asian [n = 31], other [n = 23]), leaving a final sample of 225 participants (see Table 1). Participants were primarily white (81%) and female (84%). Black participants were older on average (mean = 43, standard deviation [SD] = 10) than white participants (mean = 39, SD = 12). White participants were more likely to have graduated from college (79%) than black participants (53%). Likewise, white participants were more likely to report an annual household income ≥$100 000 (48%) than black participants (16%). Team formation also differed between black and white participants, with white participants more likely to self-select their team (80%) than black participants (67%).
Participant Characteristics.

Abbreviation: SD, standard deviation.
Associations Between Demographic and Heath Variables and Adherence and PA Outcomes
Across our sample, older participants were more adherent to Fitbit wear with more valid days (r = .198) and weeks (r = .195) of wear. On average, males (mean = 9482, SD = 3464) walked 1300 more steps each day than females (mean = 8157; SD = 2577). Participants with a greater preference for smaller, more immediate rewards (ie, greater delay discounting score) averaged fewer daily steps (r = −.140). No other demographic or health-related variables were associated with study outcomes.
Fitbit Adherence and PA
During the 2 weeks prior to the start of the intervention, 98% of black and 99% of white participants had valid weeks of Fitbit wear. Black participants averaged 64 minutes of MVPA and 8755 steps per day, while white participants averaged 81 minutes of MVPA and 8492 steps per day (see Figure 1). During the first week of the intervention, black participants averaged 80 minutes of MVPA and 9263 steps per day while white participants averaged 87 minutes of MVPA and 8528 steps per day. Moderate-to-vigorous physical activity peaked for black participants in week 21 with 169 minutes, while average daily steps peaked in week 3 with 9981. Moderate-to-vigorous physical activity peaked for white participants during week 10 with 129 minutes and average daily steps peaked in week 2 with 8787 steps.
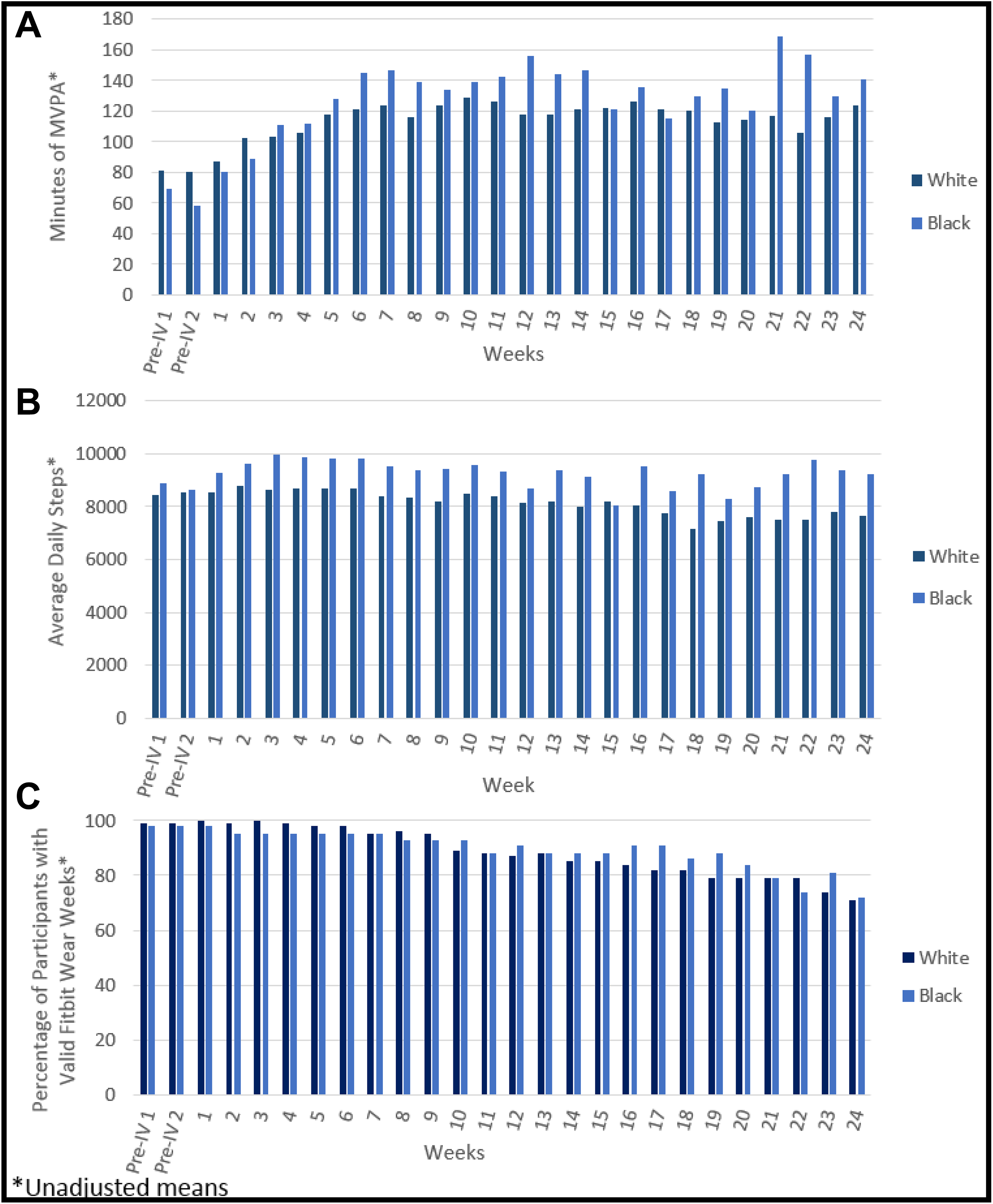
Moderate-to-vigorous physical activity (MVPA), average daily steps, and valid Fitbit wear across intervention weeks by race.
During the course of the intervention, black participants averaged 102 minutes of MVPA per week and 9312 steps per day, an increase of 38 minutes of MVPA per week and 558 steps per day. White participants averaged 90 minutes of weekly MVPA and 8159 steps per day, an increase of 9 minutes of MVPA per week and a decrease of 333 steps per day. All white participants and 98% of black participants wore their Fitbits during the first week of the intervention. This declined steadily over time with 87% of white and 91% of black participants wearing their Fitbits during week 12 of the intervention and 71% of white and 72% of black participants wearing their Fitbit during the final week of the intervention.
Table 2 presents the results of the race (black vs white) by team ANCOVAs for each outcome. Because no demographic and health-related variables were associated with both black versus white race and study outcomes, none were included as covariates in the models. The following results included estimated marginal means from ANCOVA models. Our data did not provide evidence that team formation modified the relationship between black versus white race and PA. Therefore, final models did not include interaction terms of team formation and black versus white race. We found that white participants walked an average of 7826 steps per day while black participants averaged approximately 1300 more steps each day (P < .01) with 9128 average daily steps. Participants who self-selected their teams walked 9029 steps on average each day approximately 1100 more steps (P < .05) than those who were assigned into teams, who averaged 7925 daily steps. Our data did not provide evidence for significant black versus white race or team-formation differences in average weekly MVPA, total Fitbit wear days, valid weeks of Fitbit wear, or number of weeks meting personal goals or the Guidelines. Results of sensitivity analyses including demographic and health-related covariates (ie, gender, age, education, income, BMI, and delay discounting) did not differ from the parsimonious models presented above.
Results of Race by Team Formation ANCOVAs on Weekly MVPA, Average Daily Step Count, and Fitbit Adherence.

Abbreviations: ANCOVA, analysis of covariance; CDC: Centers for Disease Control and Prevention; CI, confidence interval; MVPA, moderate-to-vigorous physical activity.
Discussion
We examined the impact of black versus white race and team formation on PA uptake during a financial incentive-based workplace wellness intervention aimed at increasing PA among insufficiently active employees. Results indicated black participants and those who formed their own teams accumulated more steps each day of the intervention than did white participants and those assigned to groups, respectively. However, we did not find black versus white race differences in average weekly MVPA, Fitbit adherence, or meeting of personal goals or the Guidelines. Likewise, the data did not suggest team formation-related differences in MVPA, Fitbit adherence, or meeting of goals.
Prior research has demonstrated that black individuals engage in less PA than white individuals.9 Indeed, this was the case during with our sample where black participants engaged in less MVPA per week than white participants at baseline. Black participants did walk more steps per day on average at baseline (262 steps per day, on average); however, this was a nonsignificant difference from white participants. In contrast, our study found that black participants walked 1000 steps more per day, on average, than white participants during the course of the intervention. Furthermore, while black participants’ engagement in MVPA peaked later than white participants’ (week 21 vs week 10, respectively), black participants averaged 169 minutes of MVPA per week at their peak while white participants only averaged 129 minutes during their peak. Black participants also showed a greater increase in MVPA from baseline than did white participants, more than doubling their average weekly MVPA during the intervention when compared to baseline.
Together, these results indicate that black individuals demonstrated similar, if not greater, benefit than white participants from a financial incentive-based workplace wellness program aimed at improving PA. In fact, they showed greater benefit for increasing low intensity walking, which is also associated with a decreased risk of diabetes and all-cause mortality, as well as improved self-reported and performance-based measures of physical function, quality of life, and depression. 34 –36 Black participants also showed a greater increase in time spent engaging in MVPA. It is possible that black participants, who were of lower socioeconomic status than white participants in our sample, may have been motivated by the financial incentives provided in this program and thus were more likely to engage in PA throughout the intervention. Because the data did not provide sufficient evidence that health or demographic factors, such as income, were associated with PA and adherence outcomes at the bivariate level, we did not include them in the multivariate models. However, we conducted sensitivity analyses including possible covariates (ie, age, sex, education, income, delay discounting, and BMI) that may affect outcomes, which did not change the pattern of our results. Furthermore, black participants did not differ from white participants regarding the average weeks meeting personal goals or the Guidelines. Thus, it remains unclear why black participants demonstrated greater improvement in PA. Regardless, greater levels of MVPA are associated with better health related outcomes and quality of life. 1,3 –5,37 Thus, similar interventions may be particularly helpful for African Americans who are less likely to be physically active and are at higher risk for chronic health problems.10
In previous work, group-based wellness interventions have shown to be more effective than individual interventions. 19,21,22 However, even among group-based interventions there is considerable heterogeneity. In one study, researchers found that providing a combination of individual- and team-based financial incentives was most effective in improving PA.19 In this study, however, all teams were self-selected. In other studies that used financial incentives to improve health behaviors, teams were assigned by the researchers. In another study, teams worked together to earn a potential bonus,22 while in another teams were assigned by researchers but members did not know the identity of others on their team.21 This study capitalized on competition between group members as only those who were successful shared a monetary reward. In each case, those in teams were more successful than those who participated individually.
In the current study, participants could either form a team or be assigned by the research team. While team formation did not impact MVPA, Fitbit adherence, or meeting of goals, those in self-selected teams did average approximately 1100 more steps each day than those who were assigned to teams, or nearly half a mile. 38 Because forming one’s own team may be a barrier for participation (eg, if required to establish their own team in order to participate, employees with a limited social network may be at a disadvantage), workplace wellness interventions should allow for both options—self-selection and matching. Indeed, self-selection may prove to increase the effectiveness of workplace wellness interventions due to social desirability (ie, wanting to please others they are friendly with) 39 and accountability (ie, not wanting to disappoint a teammate who you know). 40 -42 Participants who self-select teammates may also be more motivated and may choose peers who are also highly motivated to join their team. However, assigned teams performed similarly across most outcomes within the B-Well intervention.
These results should be interpreted in the context of several limitations. First, this study is limited geographically. All participants are employees from one hospital in Boston, Massachusetts, and the sample was comprised predominantly of white females. Furthermore, we excluded individuals of racial and ethnic backgrounds other than white or black. Therefore, our results may not generalize to other populations, particularly those of other racial and ethnic backgrounds, a greater proportion of males, or other geographic areas. Our study provides novel information about the use of a financial incentive-based wellness program in the workplace among black and white employees. However, future research is needed to generalize these findings to a larger, more diverse workforce, especially those of other racial and ethnic backgrounds. Additionally, we excluded data based on nonwear activity; thus, our estimation of PA using less data may not be robust and could lead to an overestimation of PA. Moreover, the Fitbit accelerometer does not measure nonwalking PA. Thus, we cannot detect any black versus white race or team formation-based differences in PA that occurred on invalid days and weeks as well as nonambulatory PA. Finally, providing financial incentives based on meeting personal goals that were below the Guidelines, we may have inadvertently lowered expectations for participants. However, for insufficiently active employees, a goal of meeting the Guidelines may have been overwhelming. Given the evidence suggesting small, manageable goals are more attainable and lead to larger future goals, these smaller personal goals were meant to motivate ongoing behavior change. 43,44
Our results indicate that a financial incentives-based workplace wellness intervention aimed at improving PA among insufficiently active employees was effective at increasing PA among both black and white employees. Indeed, this may be especially true for blacks who walked an average of 1000 steps more than white employees each day of the intervention. By increasing PA using similar programs, employers may help in reducing the cost and burden of chronic illness, particularly for blacks who have higher rates of many chronic conditions. Further, allowing participants to either self-select or be assigned to teams may help improve the effectiveness of the intervention by capitalizing on the use of teams 19,21,22 while also removing the barrier of forming a team on one’s own.
So What?
Although regular physical activity (PA) has been demonstrated to reduce the risk of chronic health conditions, many Americans do not meet the Guidelines for PA. Moreover, there are racial disparities in PA with black individuals engaging in less physical than white individuals. We examined differences in the uptake of PA between black and white employees enrolled in a financial incentives-based workplace wellness intervention to determine whether this type of intervention would be useful in eliminating disparities in PA. We found that although black and white participants engaged in similar amounts of MVPA during the intervention, black participants walked more steps per day and showed a greater increase than white participants in both MVPA and daily steps, compared to baseline. Together this suggests that financial incentives-based workplace wellness programs may work to reduce the black versus white race disparities in PA, which may help to reduce overall disparities in chronic health conditions between these racial groups.
Footnotes
Authors’ Note
The data that support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. All authors are employees of Brigham and Women’s Hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the National Institutes of Health under award numbers T32 AR055885 and K24 AR057827-09 and Brigham and Women’s Hospital. B-Well is registered at ![]() (NCT02850094).
(NCT02850094).