
Abstract

Workplace health promotion practitioners have an opportunity to embrace a global movement focused on better understanding and supporting employees with mental health and substance abuse disorders. More than 1500 research articles and applied reports now exist on the topic of workplace mental health. 1 This article provides an overview of key findings from epidemiological and applied research. The prevalence rates and clinical nature of these disorders are briefly noted, followed by an examination of how the workplace can both contribute to and ameliorate the problem. A list is provided of organizations active globally in this area and their key resources. Finally, the growth of employee assistance programs (EAPs) around the world is recognized as they have evolved into a valued partner for employers interested in advancing workplace mental health. 2
Understanding Mental Health Disorders
Worldwide, common mental health disorders affect more than 300 million people and a majority (70%) of these people are employed. 3 Most mental disorders are mild or moderate in their level of impairment and clinical severity, which allows most of these people to work. This translates into about 15% of the total workforce who have a milder form of mental disorders and another 5% who have a more serious mental or psychiatric disorder. Epidemiological data from many developed countries on the prevalence rates in society indicate that about 1 in every 5 working adults have mental health disorders and substance abuse problems. This rate increases to more than a 1 in 3 people over a lifetime who will develop a behavioral health disorder. In addition, many of these disorders overlap as an individual can have more than 1 disorder or risk factor at the same time (called dual disorders or clinical comorbidity). Table 1 displays the annual prevalence rates for common disorders from countries and regions that have had the most success in workplace mental health, including the United States, 4 -6 Canada, 7 -13 Australia, 14,15 and Europe/the United Kingdom. 16 -19 For comparison, total global averages are also provided, which include data from both developed and underdeveloped countries. 20 -22 The rates in Table 1 were averaged by the author from multiple recent reports based on national and international studies.
Global Prevalence Rates per Year in Adult Populations for Common Mental Health Disorders and Behavioral Problems.
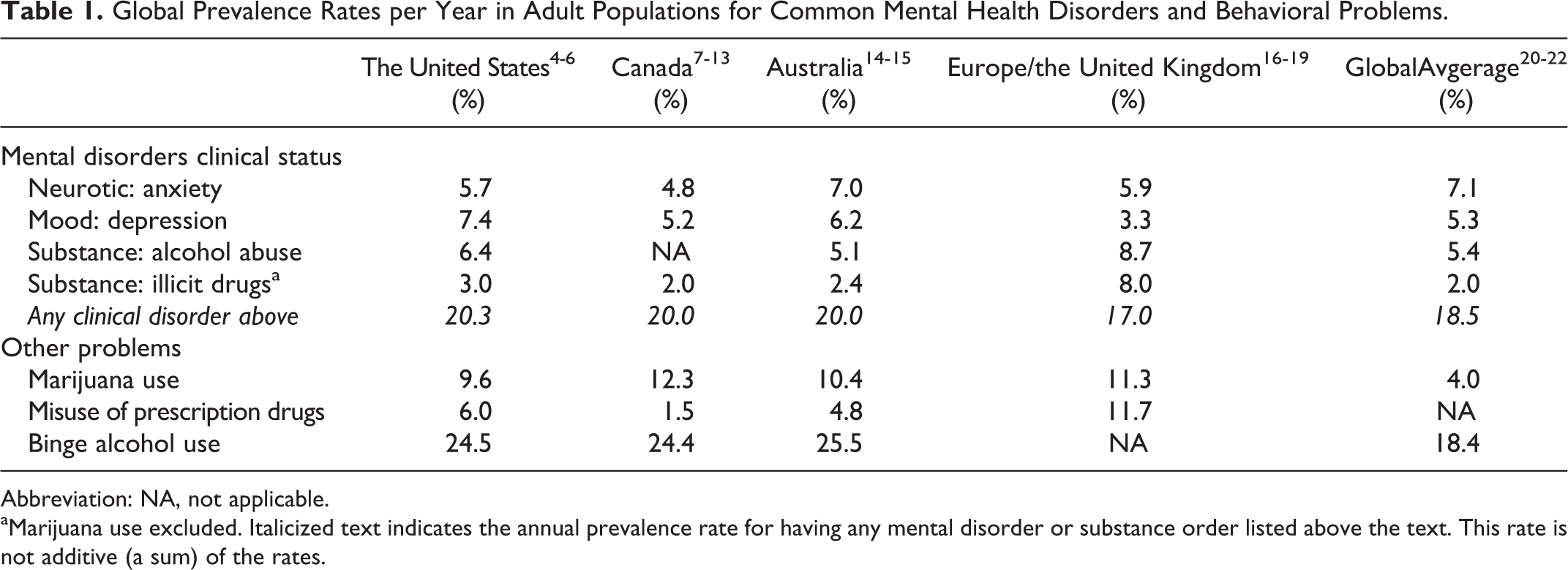
Abbreviation: NA, not applicable.
aMarijuana use excluded. Italicized text indicates the annual prevalence rate for having any mental disorder or substance order listed above the text. This rate is not additive (a sum) of the rates.
Common Types of Mental Health and Substance Use Disorders
Anxiety disorders affect about 7% of adults. As a group, they include conditions such as generalized anxiety disorder, post-traumatic stress disorder, panic disorder, social phobias, and trauma. Next most prevalent, at about 5% of adults, are the various forms of mood disorders. Mild and moderate depressive disorders can contribute to personal suffering as well as poor productivity and work absence, but major depression can be disabling and increases suicide risk. Combining anxiety, depression, and related conditions, about 1 in 10 workers have a mental health disorder.
Considered together, substance abuse disorders involving alcohol, illicit drugs, and legal drugs affect between 10% and 20% of adults. Substance abuse disorders most commonly involve alcohol abuse or alcohol dependence. The use of illicit or illegal drugs is only about half as common as alcohol disorders. However, misuse of prescription drugs that are legally obtained (such as opiates initially prescribed for pain relief) is also a growing concern as far more people use legal drugs than illegal drugs. Additionally, about 10% of adults smoke marijuana, which is a more complicated concern for employers in locations where it has been legalized. Although technically not a clinical disorder, regular heavy regular drinking or binge drinking (called alcohol misuse) are also highly prevalent, affecting about 1 in 4 adults in most developed countries.
Age and Gender Considerations
One of the key characteristics of mental disorders is that they tend to start early in life. The median age of onset across all types of mental disorders is in the early teenage years, with 75% of all mental illnesses having developed by the mid-20s. Anxiety disorders start particularly early in life (high school age), substance abuse disorders typically begin in young adulthood (college years), whereas mood disorders shows more range across age groups and tend to start in the decades of the 30s and 40s. The implication is that many employees first entering the workforce or in the early stage of their career are at risk of behavioral health problems.
There are also consistent gender differences found in the global prevalence data. Women are about twice as likely as men to have mood disorders and anxiety disorders and to be the victims of sexual and domestic violence. In contrast, men are more likely than women to have substance abuse disorders (particularly for alcohol), antisocial (anger), and personality disorders; to experience violence; to suffer from loneliness; and to die from suicide. More women than men typically seek treatment for mental health problems in outpatient settings and also to use counseling services from EAPs. Workplaces can be a good place to start changing the fears and social stigma issues that hold many men back from getting the mental health and alcohol misuse support they need (see the Movember organization in Table 2).
Organizations With Workplace Mental Health Resources Available Globally.
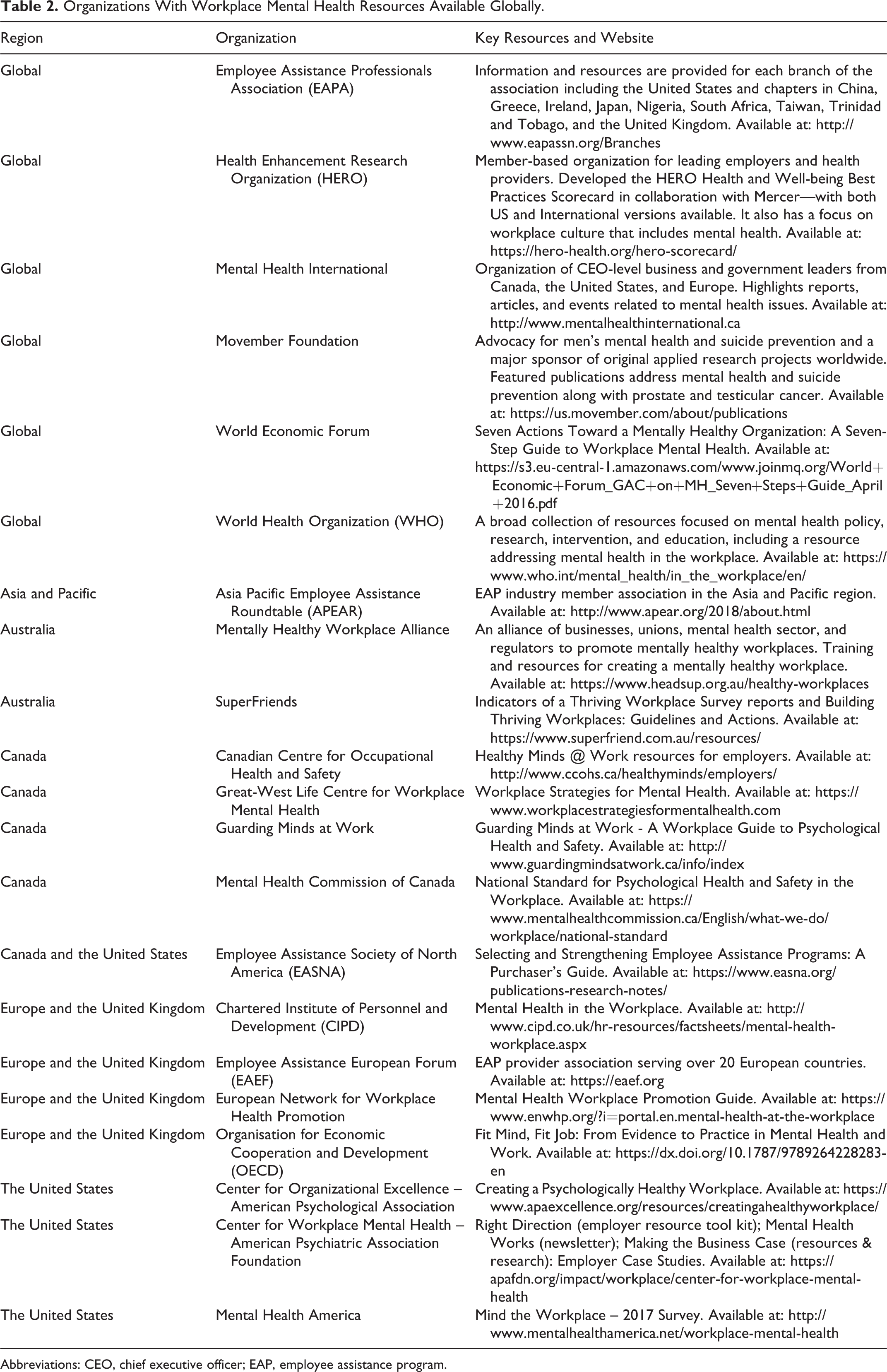
Abbreviations: CEO, chief executive officer; EAP, employee assistance program.
Role of Work and Workplace in Mental Health Disorders
There is now substantial evidence linking work design, certain working conditions, and the larger workplace culture to employee mental health and job performance. 23 Highlights from this research are now presented.
Nature of Work and Mental Health
Poor-quality jobs can contribute to mental health problems. 24 Workers with mental disorders are more likely to work in jobs that do not match well with their skills. They are also more likely to work in low-skilled and low-wage occupations (clerical work, sales and service work, elementary occupations). These occupations tend to combine high psychological demand with low decision latitude—a combination likely to lead to job strain, which is an unhealthy form of work-related stress. Jobs with high workload, time pressure, and low levels of autonomy and authority increase stress and the risk of making mental health disorders worsen.
Lack of social support or friends at work can also contribute to poor mental health of workers. Some workers also face trauma in the workplace from bullying, mobbing, or having an abusive manager or boss. In addition, when employees perceive that rewards are not commensurate with the effort they invest in work, the risk of poor mental health increases. The perception of fair processes and justice in the workplace—notably, accuracy of assessment, inclusion in decision-making, and respectful treatment by supervisors—also influences mental health. 25
Workplace and Mental Health
Certain industries and workplaces also have more inherent health risks and stressors for employees with mental health disorders. High stress occupations can lead some employees to use alcohol and drugs as an ineffective coping mechanism. Some industries and jobs with high rates of regular contact with the public can sometimes involve incidents of customer-to-employee violence. The impact of larger “shared” workplace traumatic events, such as accidents, suicides, deaths, and even natural disasters, also can create situations of extreme distress for some workers. Those affected by these kinds of critical incidents often benefit from immediate psychological first aid, group debriefing provided onsite after the event, and individual counseling afterward (if needed). Industries with frequent but unpredictable violent or traumatic events (ie, railways, airlines, banking, retail, police) often have implemented a “peer support” program, in which more experienced employees volunteer to help identify and refer other employees who witness or experience a traumatic incident as part of their work. 26
Positive workplaces for mental health often embrace 3 key components. 27 Foremost is a vision for the organization that recognizes that operational excellence and business success requires a psychologically healthy workplace. This is followed by comprehensive strategies and company policies that are sustainable over time and which operate at the employee, workplace, and organizational levels. Prevention and treatment referral services for mental health conditions should also be available company-wide for both employees and their family members. Even as the social stigma against mental health and addiction has lessened to some extent, it remains a major barrier to enacting significant change in workplace mental health. 28 That is why the single most important workplace context factor is when senior leadership at an organization recognizes and personally gets involved to help develop a work culture that is accepting and supportive of employees who are struggling with mental health issues. 29
Executives at leading employers in Canada consider supporting workplace mental health as part of their corporate civic duty. For example, Bell Canada has spent over $100 million dollars on its annual “Let’s Talk” antistigma campaign that is designed to get people talking about mental health issues. 30 The Great-West Life Centre for Workplace Mental Health recently sponsored a major research project that resulted in a white paper 31 and a book 32 that together document how the landscape of workplace mental health in Canada has dramatically changed over the past decade. Two of these milestones were the establishment in 2007 of a National Mental Health Commission and the creation in 2013 of the “first in the world” National Standard for Psychological Health and Safety in the Workplace (see Table 2). Many employers and health promotion professionals are now being trained in how to implement and advance this new exciting standard. See the lessons learned from case studies of 40 organizations across Canada who were early adopters of the Standard between 2014 and 2016. 33
Practical Resources for Supporting Workplace Mental Health
Numerous resources for employers are now available from a wide range of nonprofit and government organizations. 34 Table 2 lists a sampling of 21 organizations from the same countries and regions featured in Table 1. All of these organizations offer rich content and resources aimed at professional and business audiences with most of the resources available at no cost. Many of these resources were only developed in the past decade and represent significant collaborations between business leaders, clinicians, and applied researchers on how to most effectively use the power of the workplace to support employee mental health. Most of these resources have been sponsored by government, nonprofit organizations, and even businesses themselves, which shows a recognition of the importance of mental health issues that was often lacking in the past. On this list are the 4 major industry associations that support professionals in the EAP profession (see Table 2).
Global Trends in EAPs
In addition to the job design, work policy, and organizational culture approaches already discussed, there has been tremendous growth in offering EAP in many countries. 35 Employee assistance programs are employer-sponsored programs designed to help individuals resolve acute but modifiable behavioral health issues. Review of industry-wide data representing more than 80 vendors shows that most individuals only need a few sessions with an EAP counselor to get relief and rebound to a more normal level of work performance. 36 The roughly 15% of EAP cases that have more serious or chronic mental health and substance abuse disorders (such as in Table 1) are provided referrals to qualified treatment providers.
Employers should be cautious though about a recent trend in the North American region to provide a stripped down version of services that are bundled as “Free EAP” into other health insurance and benefit offerings. 37 The lack of promotion and workplace integration of these kinds of minimal EAPs often yield very low utilization (ie, <2% of employees use it for counseling in a year) and very little if any resources for the work organization. 36 In contrast, a full service EAP goes beyond just counseling for troubled employees to provide a more comprehensive suite of services. 38 The more comprehensive approach usually includes support for individual managers and work teams with expert consultation and supports the larger work organization with trainings, educational resources, and risk screening tools. Moreover, full-service providers often seek to build strategic alliances with other employee benefits and family support services for a more proactive approach to finding and treating at-risk employees. Advance planning and professional response to critical incidents affecting the workplace are also a very specialized and highly valued component of EAP core services. When these full-service EAPs are embraced by health promotion, wellness, safety, and company leadership, they can be more effectively integrated into other parts of the larger organization. 39 One result of greater integration is much higher level of utilization of individual counseling services (ie, at 2 or 3 times the industry average of 4.5%) and also greater use of other EAP services, such as work/life, financial or legal, and manager consulting and training. 40 Employer case study examples of this enhanced EAP effect are provided on the websites of many of the organizations listed in Table 2.
Employee Assistance Program in North America
Employee assistance programs first started in the 1930s in the United States as employer-sponsored internal support programs to help restore work function for alcoholic employees in manufacturing industries. In the 1980s and early 1990s, only one-third of employers in the United States offered an EAP. Today, in the United States, all federal and state government workers and a vast majority of employees in large- and medium-sized employers in the private sector have access to EAP. 41,42
Like the United States, Canada is a mature market for EAP services, which are called Employee and Family Assistance Programs (EFAP). Although recent national market statistics are not available, EFAPs are offered by the national government, all of the provincial governments and by most large- and medium-sized employers in Canada. The substantial growth in EFAPs has been driven largely by employers who recognize the role of workplace mental health as contributing to business success.
Employee Assistance Programs Globally
In other regions of the world outside North America, EAP is not as mature a product offering as it has only been active in the past 20 years or so. In many parts of the world, the concept that an employer should even get involved in employee personal or mental health issues has been challenged. In 2016, the international EAP provider Chestnut Global Partners conducted a survey to determine how many external EAP vendors there were in the world. 43 The survey identified a total of 839 EAPs. Of these, approximately 70% were based in the United States, with about 250 different EAP vendors operating outside the United States. The list was further broken into 3 market segments based on geographic reach. Global EAPs are tasked with building local relationships that allow services to be delivered in each country and are increasingly focusing on the use of technology as a service delivery platform. Only 6 vendors were identified as global providers of EAP. The next segment includes EAPs that serve multiple countries within the same geographic region. There are 56 of these kinds of EAPs. For example, Asia has about 4 regional EAPs and Latin America has 7, while the country of Australia has 20 EAPs. Finally, the single-country national market segment has the most EAPs with 777. Table 3 lists a series of brief articles that profile the state of EAP services in 10 different countries internationally.
Articles Profiling the EAP Market in Different Countries.a
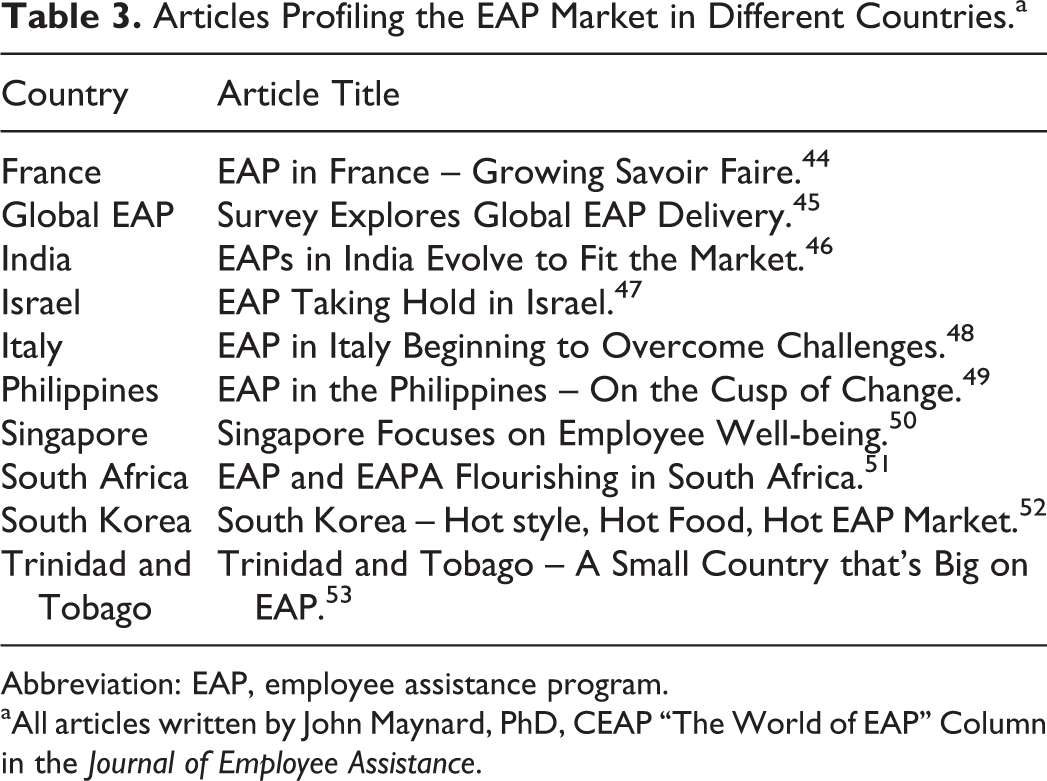
Abbreviation: EAP, employee assistance program.
aAll articles written by John Maynard, PhD, CEAP “The World of EAP” Column in the Journal of Employee Assistance.
Employee Assistance Program Counseling and Workplace Outcomes
A recent study examined the workplace outcomes for employee users of EAP counseling. 54 It was based on a sample of more than 24 000 total cases with longitudinal data on the Workplace Outcome Suite 55 from pre- and postuse of counseling. The data were collected during a 9-year period from more than 30 different EAP vendors and internal programs in 28 countries. Overall results demonstrated that use of workplace counseling was associated with improvements in employee work presenteeism, absenteeism, workplace distress, work engagement, and overall life satisfaction. The statistical effect sizes were largest for the outcomes of work presenteeism and life satisfaction. Moreover, the impact of brief counseling on workplace outcomes was found to be consistent across client age and sex, sources of referral into the EAP, types of clinical issues, employer industry, and the EAP delivery business model (ie, external vendor, internal staff program, or hybrid of both). Of interest to the present article, the EAP usage profile and the level of improvement over time in these outcomes was quite similar between cases from different countries. These findings are highlighted in Table 4. The results demonstrate the general effectiveness of brief counseling regardless of where the employee was working around the world.
Improvement After Use of EAP Counseling on Workplace Outcome Suite (WOS-5) Measures by Country.a

Abbreviation: EAP, employee assistance program.
aTotal sample size is 24 363 counseling clients. Listed in the relative change (as % improvement) from average score on measure at start of counseling to the average score at 3-month follow-up after counseling.
Conclusion
Employer interest in understanding and supporting workplace mental health is increasing worldwide. The prevalence rates globally reveal that common mental health and substance abuse disorders affect at least 1 in 5 workers, with many more affected depending on which problems are considered. Key aspects of how work is designed and the workplace context itself can all influence mental health. Fortunately, knowledge transfer guides and major reports for how to promote a psychologically healthy workplace are now available from a range of advocacy organizations in many countries. Employers are encouraged to use these practical resources for their employee education, manager training, company policies, and organizational-level activities. Global trends in EAPs show they continue to grow in popularity beyond their genesis in North America. New research using standardized outcomes measures provides evidence that the use of brief counseling from EAPs is associated with improvements in clinical and work performance domains. Importantly, these outcomes were found consistently for cases in different countries. Employee Assistance Programs can be a strategic partner for health promotion professionals to collaboratively advance a range of worthy workplace mental health initiatives.