
Abstract
Purpose:
This study aimed to increase the consumption of home-cooked meals among employees at a large urban worksite through a fully subsidized Community Supported Agriculture (CSA) program.
Design:
Randomized trial.
Setting:
Worksite in a large northeast city.
Participants:
Employees were recruited through flyers, e-mail listservs, and outreach from departmental administrators (n = 60).
Intervention:
Intervention participants received 8 biweekly fresh food deliveries through a CSA program. They also received cooking education and support. Control participants received usual employee benefits.
Measures:
Consumption of meals prepared at home was the primary end point. Increased consumption of fresh fruits and vegetables was the secondary end point, and food insecurity was an exploratory end point.
Analysis:
Poisson regression was used to assess mean differences in weekly consumption of home-cooked meals. To assess differences in fruit and vegetable consumption and food insecurity, binary logistic regression was used to estimate odds ratios.
Results:
Compared to the control group, intervention participants consumed 29% more home-cooked meals per week (P < .01). Fruit and vegetable consumption also increased among intervention participants. The odds of at least twice-daily fruit consumption were 3.8 times higher among intervention participants than among controls, and the odds of at least twice-daily vegetable consumption were 6.2 times higher among intervention participants than among controls. Compared to control participants, intervention participants experienced a statistically significant 89% reduction in the odds of reporting food insecurity at follow-up, when controlling for baseline food insecurity. Participants reported perceived intervention benefits, including the opportunity to experiment with new, healthful foods without financial risk, as well as the social value of sharing recipes, food, and related conversation with colleagues.
Conclusion:
The study demonstrated the feasibility and potential positive effects of a subsidized workplace CSA program, augmented with cooking education and support.
Purpose
Most Americans consume too few fruits and vegetables and too many meals away from home, which tend to be more calorically dense and less healthful than home-cooked meals—contributing to the population burden of chronic disease. 1 -3 Over two-thirds of US adults are currently considered overweight or obese, 4 which has been linked to decreased workplace productivity. 5 Along with population health practitioners, employers are motivated to identify effective behavior change strategies to encourage healthier dietary practices. This article evaluates a worksite program designed to increase employees’ consumption of healthful home-cooked meals.
Approximately half of the US employers with 50 or more employees offer workplace wellness interventions. 6 Obesity prevention and weight loss programs—which are among the most common workplace wellness initiatives—have demonstrated variable effectiveness in achieving behavior change. A systematic review of dietary workplace interventions described a range of outcomes with regard to eating habits, diet quality, and weight loss, noting that interventions were most successful when they had leadership buy-in, incorporated social support, and addressed multiple behaviors versus diet alone. 7 Some interventions have successfully leveraged behavioral economics (BE) including financial incentives to shift dietary practices and promote weight loss. 8 -10
Multiple barriers stand between well-intentioned, well-informed consumers and the adoption of healthier dietary practices. Barriers include constraints on healthy food availability, cost, lack of familiarity with diverse fruits and vegetables and how to prepare them, and the alluring convenience of eating away from home. 11,12 More frequent consumption of foods prepared away from home—which account for more than half of all food dollars spent in the United States—has been associated with decrements in diet quality and higher body mass index (BMI). 2,13 Further, there is no assurance that provision or acquisition of healthful foods alone will lead to greater consumption of those foods. US households throw away nearly 27 million tons of food annually. 14 Fruits and vegetables are the most frequently discarded items, accounting for 42.5% of all US consumer food waste. 15 Interventions that aim to improve cooking skills may also help minimize food waste. 16
The authors hypothesized that offering healthful food deliveries to employees at the workplace, through a fully subsidized Community Supported Agriculture (CSA), in combination with cooking education and support, would increase participants’ consumption of home-cooked meals (primary end point) and lead to increased consumption of fruits and vegetables (secondary end point). The intervention was designed to address 3 barriers to cooking healthful meals at home: access to fresh fruits and vegetables, cost, and convenience. Thus, the authors of this study partnered with a nonprofit food distributor to conduct a mixed-methods randomized controlled trial (RCT) to simulate a potential workplace benefit of delivery of fully subsidized fresh healthful foods and cooking instruction to employees. This evaluation was designed to generate evidence to inform potential employer investments in workplace wellness policies.
Guided by the Easy, Attractive, Social, and Timely (EAST) framework, the intervention was designed to make cooking at home: (1) easy (ie, delivered to a convenient work location); (2) attractive (ie, attracted attention through tailored instructional cooking videos); social (ie, provided in-person and web-based supports); and timely (ie, delivered supports in sequence with food deliveries). 17 The EAST framework and other applied BE theories seek to influence human decision-making and are often leveraged by policymakers, public health practitioners, and employers to promote adoption of healthy behaviors. 18 The intervention also employed nudge theory, which incorporates positive reinforcement and choice architecture (ie, interventions that make the healthy choice the easy choice) as ways to shift behavior. Nudge theory informed messages and materials developed by study staff, including straightforward instructional materials and short videos that shared recipes, food storage tips, and recommendations regarding how to prepare items in upcoming CSA deliveries. 19
Methods
Design
The study was a 16-week, mixed-methods RCT.
Setting
This study was conducted at the worksite of one of Philadelphia’s largest employers. The intervention was conducted in winter 2017 to 2018 and was approved by the University of Pennsylvania's institutional review board.
Intervention
Intervention participants received free biweekly CSA deliveries for 4 months (a total of 8 CSA deliveries). The CSA box was delivered to a central worksite location and typically included 1 dozen eggs, 1 type of fruit (4 servings), and 5 types of vegetables (10+ servings). In addition to CSA deliveries, participants received intervention “enhancements,” which included curated content with recipe suggestions, instructional cooking videos, and food storage tips, as well as digital and in-person communication from study staff. These “enhancements” were designed to encourage the preparation and consumption of all the foods included in each CSA delivery and to minimize waste. Control group participants received usual care (ie, regular employee benefits).
Participants and Recruitment
The study sample included 60 adult employees. Participants were recruited through flyers, e-mail listservs, and outreach from departmental administrators. All participants provided written informed consent. Participants were randomized using block randomization into the intervention group or the usual care control group.
Hypotheses, Sample Size, and Power
The study team hypothesized that CSA participation would contribute to increases in weekly consumption of home-cooked meals (primary end point) as well as increases in consumption of fruits and vegetables (secondary end point). Food insecurity was an exploratory end point. Data were collected from 30 intervention participants and 30 controls, with the goal of informing the design of a larger RCT. The sample size was maximized based on funding available for the study. Sample size was therefore not based on estimates of power to detect between-group differences of a prespecified magnitude. The CSA cost was $29.99 per delivery per person or $239.92 for 8 deliveries. The CSA intervention was grant funded and intervention participants received the CSA deliveries free of charge. The study was registered with ClinicalTrials.gov.
Measurement
All 60 participants were invited to complete questionnaires at baseline and at the end of follow-up (March 2018). The survey included questions about frequency of cooking at home, a modified version of the US Department of Agriculture’s (USDA) Food Frequency Questionnaire to assess fruit and vegetable consumption, and a validated 6-question food insecurity screener from the USDA. 20
In addition, postintervention, semistructured qualitative interviews were conducted with a convenience sample of the intervention group to obtain program feedback as well as to understand current cooking habits, dietary practices, and food preferences (n = 7).
Data Analysis
Survey data were collected using REDCap version 8.9.0, a secure online resource for data collection and storage. 21 Quantitative data were analyzed using Stata 15.1 statistical computing software. Poisson regression was used to assess mean differences in weekly consumption of home-cooked meals comparing intervention and control members at follow-up. To assess differences in fruit and vegetable consumption and food insecurity, binary logistic regression was used to estimate odds ratios (OR) and 95% confidence intervals (95% CIs). Microsoft Excel 16 was used to perform block randomization and to conduct additional descriptive analyses.
Analyses only included participants who completed baseline and follow-up surveys, unless otherwise specified.
Interviews were recorded and transcribed verbatim. The study team developed a coding structure using line-by-line reading of transcripts to specify recurrent concepts. Trained research assistants coded the content of all interviews using NVivo 11, with 97% agreement. The research team summarized findings in memos that guided group discussions and iterative interpretation of the data to identify cross-cutting themes. 22 -24
Results
Description of Study Population
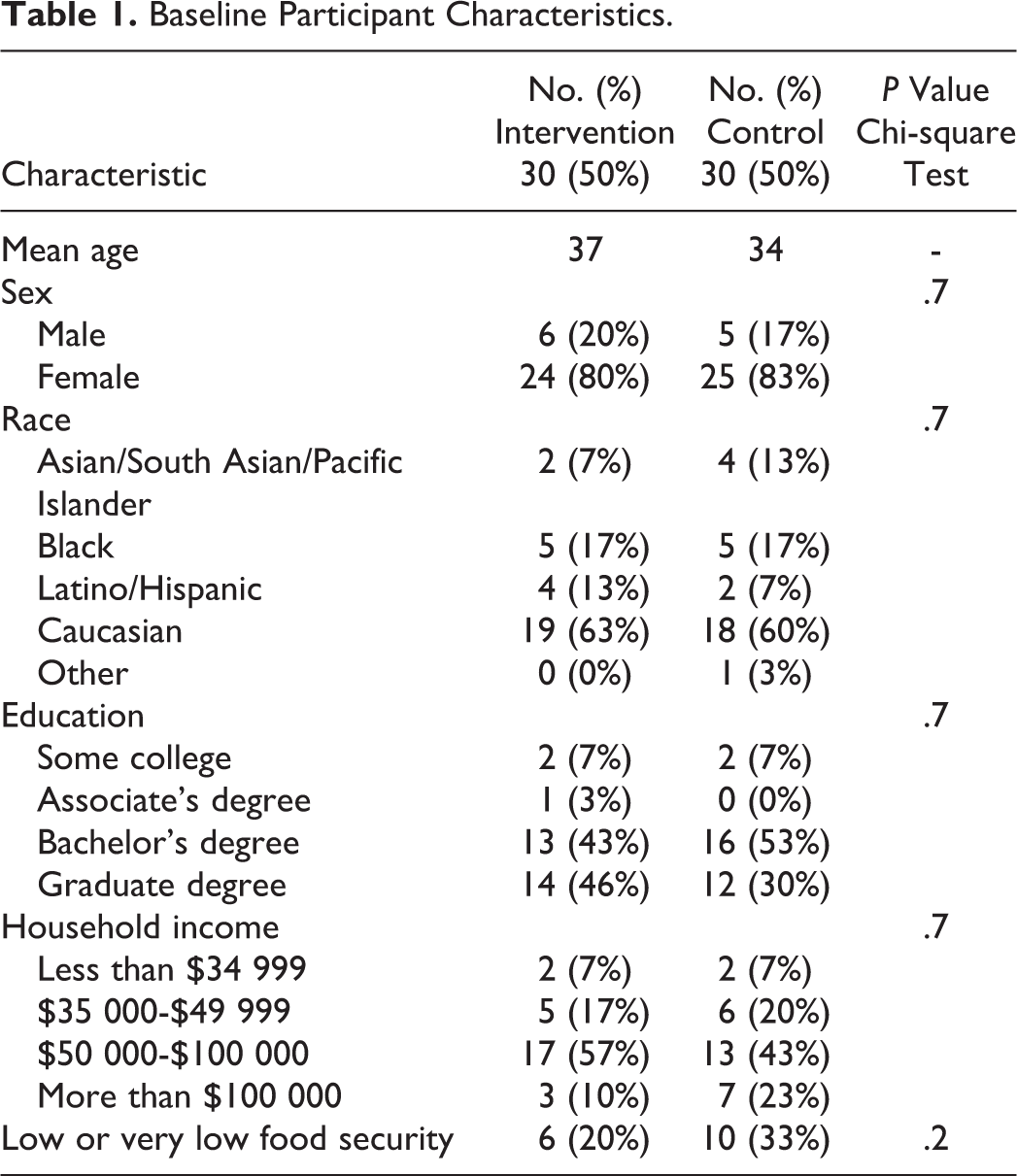
The study sample included adults employed by a large university and health system. Participants had varied job titles (eg, administrative assistant, research coordinator, associate director) in a wide range of departments (eg, alumni relations, student health services, school of education). As shown in Table 1, this sample of employed adults was diverse with regard to income, age, education, and race; and participants were predominantly female. The participants in the intervention and control groups were roughly similar, suggesting that randomization worked well to balance covariates or potential confounders in the 2 groups: 100% (n = 60) of participants completed the baseline survey; 100% (n = 30) of the intervention group and 80% (n = 24) of the control group (90% of total study population) completed the final survey.
Baseline Participant Characteristics.
Primary End Point: Consumption of Home-Cooked Meals
At the close of the intervention, compared to control group members, intervention participants ate, on average, almost 3 additional home-cooked meals per week (Table 2).
Mean Weekly Consumption of Home-Cooked Meals.
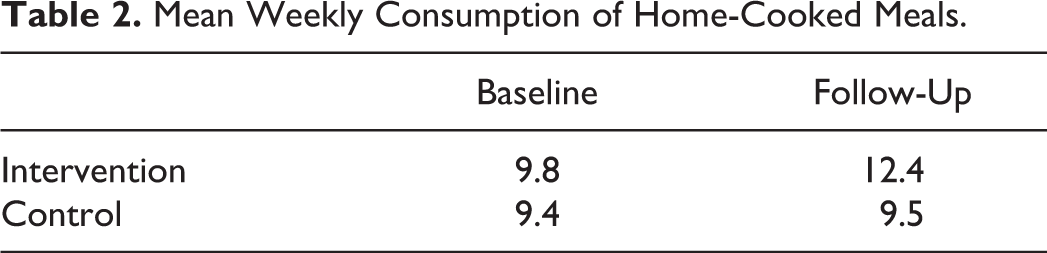
In a Poisson regression model, there was a 29% difference in mean consumption of home-cooked meals per week at follow-up in the intervention group versus the control group (P < .01). This difference was sustained after controlling for baseline number of home-cooked meals consumed each week.
The data from interviews with intervention participants offered additional insight regarding the impact of CSA participation on cooking at home. Many participants described ways in which they creatively approached cooking and meal preparation in order to use the contents of the CSA. They created self-assigned challenges to learn to prepare previously unfamiliar foods. As one participant said, “…it’s almost like I’m gamifying eating better,” by challenging themselves to learn new ways to prepare healthy food. Participants also reported that they were motivated to prepare fruits and vegetables to ensure that the CSA contents would not spoil.
Participants alternately used recipes provided by the study team as CSA “enhancements” or identified their own recipes, usually through Internet searches. One interviewee remarked that the enhancements were helpful because they focused on simple food preparation strategies, thereby demonstrating that home cooking need not be a lengthy process. As one participant said, “…your recipes and videos helped. I can take it from scratch. It doesn’t have to take four hours. I can do it quickly.” The study materials showed how to use basic approaches to preparing vegetables, including roasting and sautéing, which participants found to be easy to learn and appealing.
Secondary End Point: Fruit and Vegetable Consumption
As presented in Table 3, at follow-up, the odds of having consumed fruits and vegetables twice or more per day were significantly higher among intervention participants than among controls, taking into account baseline consumption. Specifically, the odds of at least twice-daily fruit consumption were 3.8 times higher among intervention participants than among controls. The odds of at least twice-daily vegetable consumption were 6.2 times higher among intervention participants than among controls.
Odds Ratio for Consumption of Fruit and Vegetables ≥2 Times Per Day at Follow-Up, Adjusting for Baseline Consumption.

Abbreviation: CI, confidence interval.
Interviews offered additional insights regarding fruit and vegetable consumption in the intervention group. In addition to increased overall fruit and vegetable consumption, participants reported increased consumption of new vegetables. As one participant said, “There were always new vegetables, things that I hadn’t eaten before whether it was the turnips or…honey nut squash…radishes. So because I had them, I had to use them.”
According to interviewees, the CSA deliveries exposed participants to new foods that they otherwise would not have purchased at a grocery store. After this initial introduction to new, healthful foods, some participants said they incorporated the new foods into their later grocery store purchases. As one participant explained, becoming familiar with new foods increased their confidence while purchasing vegetables at the grocery store.
Intervention participants also noted that they were more willing to take “risks” on new foods provided in the CSA, because the food was free. As one participant noted, “having the confidence to work with the raw vegetables and learning what they were and what to do with them…it just gave me the ability to try new things without [wasting money].” Some participants said that they tended to be reticent about purchasing new foods, since they cannot know in advance if they or their family members will like those foods, and they do not want to spend their grocery budgets on untested, unfamiliar items. Thus, according to participants, the CSA allowed for greater experimentation with healthy, fresh foods, without attendant financial risk.
Social Aspects of the CSA
A key finding from the qualitative interviews was the perceived social benefits of CSA participation. Several intervention group members reported that CSA participation stimulated workplace conversations around healthful cooking and promoted cooking accountability, particularly among coworkers. As one participant said, “So that was fun, too—the element of sharing it with other people. And two of my coworkers did it…we had a group thread of recipes that we made.” Other participants shared CSA items with curious colleagues who were not enrolled in the study. Another participant commented on the opportunity for CSA participation to promote equity among colleagues of varying seniority: “I can imagine say one of the younger—the newer people in our office did it, then that would be such a cool way for them to bond across a couple of levels where they might not ever get to interact…” In many ways, study participation seemed to generate active workplace conversations regarding cooking and health.
Food Insecurity
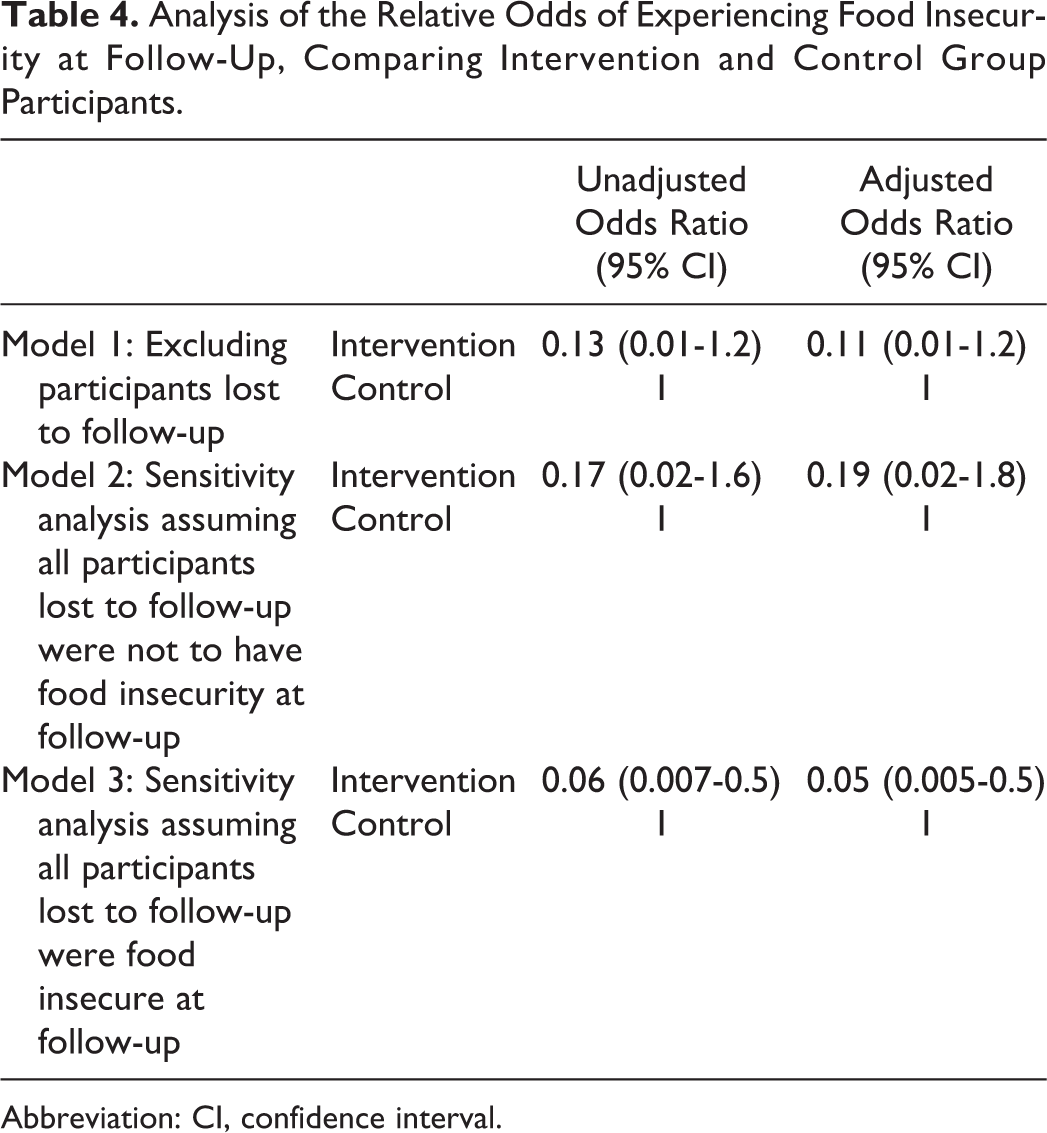
At baseline, more than a quarter of the employed adults enrolled in this study (27%) reported either low or very low food security, referred to subsequently in this study as “food insecurity.” Table 4 presents analyses of food insecurity at follow-up among intervention versus control participants. Overall, the analyses show markedly lower levels of food insecurity among intervention participants than among controls. In model 1, compared to control participants, intervention participants experienced a statistically significant 89% reduction in the odds of reporting food insecurity at follow-up, when controlling for baseline food insecurity. Model 1 excludes 6 participants who were lost to follow-up, all of whom were control group participants, yielding an analytic sample of n = 54.
Analysis of the Relative Odds of Experiencing Food Insecurity at Follow-Up, Comparing Intervention and Control Group Participants.
Abbreviation: CI, confidence interval.
Sensitivity analyses were conducted to evaluate how loss to follow-up among controls may have affected our estimate of the intervention’s impact on food insecurity. Hypothetical outcomes were also assessed under 2 different assumptions about the prevalence of food insecurity at follow-up among the 6 control group participants who were lost to follow-up. (Five of those 6 participants had reported food insecurity at baseline.) The most extreme circumstances were also modeled, in which none of the lost controls (model 2) or all of the lost controls (model 3) experienced food insecurity at follow-up.
Model 2 incorporates the “optimistic” assumption that none of the lost controls were experiencing food insecurity at the close of the study period. This model—a “best-case” scenario that assumes that all 6 of the missing controls were food secure at follow-up—offers a conservative estimate of the impact of the CSA intervention on the odds of reporting food insecurity at follow-up. In this model, the intervention was associated with a nonsignificant 81% reduction in the odds of food insecurity in the intervention group versus the control group (adjusted OR = 0.19, 95% CI = 0.01-1.4).
Model 3 assumes that all control participants who were lost to follow-up were experiencing food insecurity at the end of the study period. This model would be expected to amplify the observed preventive effect of the intervention on food insecurity. In this model, controlling for baseline food insecurity, the CSA intervention was associated with a statistically significant 95% reduction in the odds of food insecurity in the intervention versus the control group (adjusted OR = 0.05, 95% CI = 0.005-0.5).
Program Feedback From Participants
Intervention group participants provided overwhelmingly positive feedback about their experience with the CSA plus enhancements. Most intervention participants (93%) indicated that they would participate in a CSA if it were offered as an employee benefit. In this trial, there was no cost to receive the CSA, but participants were asked how much they would be willing to contribute in order to continue to receive the food deliveries at work. On average, they were willing to contribute approximately $18 per delivery. The actual cost of the CSA used in this program was $29.99 per participant per delivery, suggesting that employee contributions and employer subsidies should be further explored in a larger trial.
A small number of participants who were interviewed described challenges associated with CSA participation, which they generally described as manageable and found ways to overcome. The primary challenge was how to transport the CSA contents from work to home. Despite this transportation challenge, there was consensus among intervention group participants that they preferred to have the CSA delivered to work. Overall, they reported that this was a strength of the intervention. Some individuals—particularly those with fewer household members—had trouble initially figuring out how to use the foods provided in the CSA. As the study progressed, however, they reported becoming more adept at using the items and more willing to experiment with unfamiliar foods. Participants reported having developed new skills and confidence throughout the study duration, and wasting or discarding less food as the study progressed.
Ultimately, participants described some successes and some failures in their experimentation with new foods. In good humor, one participant described her quest to use the varied and sometimes unfamiliar greens in her CSA: “…I tried the pea shoots, and they were really long and stringy…This was my only major, major fail. I put them in spaghetti thinking they would just twirl up along with the spaghetti noodles, and it would be delicious, and I tried one bite, and…it was really gross.” In reference to the ample quantities of vegetables in her CSA, another participant explained, “that’s a good problem to have and not a bad problem to have.”
Discussion
In this small RCT with employed adults, the study team observed several possible benefits of receiving healthy fresh food deliveries, plus cooking instructional resources, and support, at the workplace. Compared to the control group, the intervention group consumed significantly more home-cooked meals as well as more fruits and vegetables. Participants also reported that they valued the social aspects of sharing food and recipes and the convenience of having the food delivered to work. Finally, there was compelling preliminary evidence, requiring further exploration, to suggest that CSA participation reduced the odds of experiencing food insecurity. Taken together, these findings suggest possible beneficial effects of workplace CSA deliveries on meal preparation at home, consumption of fresh fruits and vegetables, and food insecurity. To assess longer-term sustainability of these changes and impact on health outcomes, as well as barriers and facilitators to implementing similar programs at other worksites, further study is merited. Such information would be useful to employers considering implementing similar worksite wellness efforts. Below, the authors pose questions this study raises for a future larger scale RCT.
First, while employers may be highly motivated to deploy worksite dietary interventions to advance weight loss, employees may be motivated by alternative factors, such as well-being or social engagement. This intervention explicitly did not employ language, or espouse goals, related to weight loss or obesity prevention—based on the assumption that increased consumption of home-cooked meals and fresh fruits and vegetables is recommended regardless of one’s BMI. Tapping into employees’ motivations may be important to the success of health interventions. Based on results from this study, such additional motivators could include the social component of sharing food and recipes with coworkers, including those across different levels of the employee hierarchy. Researchers have shown how some interventions may be more successful if they are explicitly designed to be social, so that participants can bolster one another’s motivation to adhere to a new behavior. 25 Interventions may also be designed to amplify the enjoyment of learning new skills or experiencing an expanded repertoire of foods and recipes. By emphasizing social components of the intervention in the program design, employers may be more likely to shift their workplace environments toward a culture of health. 26
Second, this article highlights the presence of food insecurity among employed adults who elected to participate in this study. At baseline, more than a quarter of study participants reported food insecurity—over twice the 2017 national average of 11.8%. 27 Food security was an exploratory end point, and the study team did not anticipate such a high prevalence in this employed population. The study team also did not expect that the amount of food provided in the CSA intervention would appreciably influence food security status. Nonetheless, there was a strong association observed between intervention participation and decreased odds of food insecurity at follow-up. The adverse health effects of food insecurity are well documented and include higher rates of chronic disease and decrements in physical functioning and mental health. 28,29 Other studies of working age adults have demonstrated a range of food insecurity prevalence estimates and associated negative health and social outcomes—such as diabetes, kidney disease, and hypertension. 30 Given the small sample size, our interpretation of the data should be tempered and should be explored in a larger scale trial. Thus, further study of food as an employee benefit should include measures of food (in)security as an outcome.
Third, it is important to consider how this intervention might operate differently at other worksites or among different populations. For example, women are more likely to cook at home than men (70% vs 46%), and spend more time daily preparing food (50 min/d vs 20 min/d). 31 Further, college-educated people are more likely to cook than those with a high school degree or less (61% vs 53%). Given that a majority of our participants were women with Bachelor’s degrees or higher, the program may have different effects or face different implementation challenges at a predominately male worksite or with a less educated population. Nonetheless, such populations may stand to benefit most from an enhanced CSA program to encourage consumption of home-cooked meals.
Limitations
The study sample was small and predominantly female, and the study was limited to one worksite. In addition, participants in this study self-selected into an RCT that they knew to be about encouraging healthy eating, and thus participants were inclined to engage in diet and lifestyle behavior change. Given the high rate of food insecurity in this sample, it is possible that people who were food insecure were particularly motivated to join the study. The study also relied on self-reported measures. Furthermore, the intervention period was short, lasting only 16 weeks, with 8 CSA deliveries, and therefore it is unknown if the benefits would be sustained over a longer intervention period, or if behavior change would be sustained after termination of the CSA deliveries.
So What?
What Is Already Known on This Topic?
Diet-related programs are among the most popular workplace wellness interventions, however, their effectiveness in promoting behavior change is varied.
What Does This Article Add?
This study evaluates the impact of employee participation in a fully subsidized CSA program. Findings suggest that compared to employees who received standard benefits, employees who received biweekly food deliveries consumed more home-cooked meals, ate more fruits and vegetables, and experienced decreased incidence of food insecurity.
What Are the Implications for Health Promotion Practice or Research?
Employers should invest in studying the health-enhancing potential of provision of fresh, healthful foods, along with culinary education and supports.
Footnotes
Acknowledgments
The authors would like to thank The Common Market for their practical and financial support of the work. They would like to thank Haile Johnston, Sam Arnold, and Sarah Padva from The Common Market for their contributions. The authors would also like to thank Abby Dolan and Eliza Whiteman for their assistance with survey design and data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics statement
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the University of Pennsylvania Institutional Review Board (protocol number: 827780). Written informed consent was obtained from all subjects. Clinical trial registration: NCT03277040.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Common Market, a 501(c)(3), mission-driven regional food distributor. The Common Market received support to evaluate the behavioral health effects of The Common Market Farm Share program from the Independence Blue Cross Foundation and the Kresge Foundation. The Common Market and the outside funders played no role in the study design, study procedures, or data analysis.