
Abstract
Purpose:
To examine how interpersonal factors are associated with family, peer, and partner social support among urban female adolescents in sexual relationships.
Design:
Secondary data analysis of cross-sectional data.
Setting:
Two urban health clinics and community sites in Baltimore, Maryland.
Participants:
One hundred sixteen female adolescents (ages 16-19) with 131 heterosexual relationships from the Perceived Risk of Sexually Transmitted Diseases cohort.
Measures:
Interpersonal factors included parental monitoring, friend–partner connectedness, and feelings of intimacy for partner. Social support was measured using the Multidimensional Scale of Perceived Social Support with family, peer, and partner subdomains.
Analysis:
Multivariable linear regression models using baseline data and accounting for clustering of partners.
Results:
Adolescents perceived high levels of family, peer, and partner support, with the greatest coming from partners (range: 1-5; family mean: 4.0 [95% confidence interval, CI: 3.83-4.18]; peer mean: 4.2 [95% CI: 4.05-4.33]; partner mean: 4.5 [95% CI: 4.36-4.60]). Parental monitoring and friend–partner connectedness were significantly associated with greater family (b = 0.11, standard error [SE] = 0.03, P = 0.001; b = 0.15, SE = 0.06, P = .02) and peer support (b = 0.06, SE = 0.02, P = .01; b = 0.29, SE = 0.07, P < .001). Feelings of intimacy for partner was significantly associated with greater partner support (b = 0.08, SE = 0.03, P = .02).
Conclusion:
Feeling connected to one’s social network and having a connected network is an important contribution to social support for urban female adolescents in sexual relationships. Future research targeting interpersonal factors is warranted, as it may result in increased social support and promote positive sexual health behaviors in an urban female adolescent population.
Purpose
Social support promotes adolescent well-being and is protective in adolescent health. 1 An adolescent’s social network can serve as social capital for those in disadvantaged communities by providing social support and health education. Research has linked the presence or absence of social support to sexual health behaviors and outcomes for urban adolescents. 2 Interventions can target social networks to increase social support and subsequently promote positive sexual health behaviors and healthy relationships among adolescents. However, factors that contribute to perceived social support for urban adolescents are not well understood. Traditionally, focus has been on family serving as the safety net, despite peer and romantic relationships being highly valued by adolescents. 3,4 The purpose of this study was to examine social support from all 3 sources (family, peer, and partner) and how interpersonal factors (parental monitoring, friend–partner connectedness, and feelings of intimacy for partner) are each associated with family, peer, and partner social support among urban female adolescents in sexual relationships.
Methods
Design and Sample
Baseline data from female adolescents aged 16 to 19 years enrolled in the Perceived Risk of Sexually Transmitted Diseases (PRSTD) study was used for this secondary data analysis. Briefly, PRSTD was a longitudinal observational study conducted between December 2009 and August 2011 examining sexually transmitted infection (STI) risk in the context of adolescent sexual relationships. Adolescents, engaging in heterosexual vaginal or anal intercourse in the previous 3 months, were recruited from 2 urban health clinics and community sites all serving predominantly low-income African Americans in Baltimore, Maryland. 5 The current analysis was restricted to 116 participants who provided data on at least 1 male partner at baseline. A total of 131 sexual relationships were reported on from these 116 participants.
Measures
Interpersonal factors
Parental monitoring was assessed with 3 questions regarding parental knowledge of whereabouts at night, afternoon, and during free time. 6 Response options were on a 5-point Likert-type scale from 1 (not at all) to 5 (most they can). These questions were summed to reflect a total parental monitoring score ranging from 3 (lowest monitoring) to 15 (highest monitoring).
To capture friend–partner connectedness, participants were asked, “How many of your close friends know this partner?” Response options were on a 4-point Likert-type scale from 1 (a few/none) to 4 (all). This question was partner-specific as it was queried for each reported partner.
Feelings of intimacy for their partner was assessed by asking adolescents partner-specific questions on closeness, trust, and love within the relationship in the past 4 weeks. Response options were on a 4-point Likert-type scale from 1 (not at all) to 4 (very). A “feelings of intimacy for partner score” 7 was derived from the sum of these 3 questions, ranging from 3 (lowest feelings of intimacy) to 12 (highest feelings of intimacy).
Social support
Social support was measured using the validated Multidimensional Scale of Perceived Social Support, 8 which includes family, peer, and partner subdomains. Response options for each subdomain were on a 5-point Likert-type scale from 1 (strongly disagree) to 5 (strongly agree).
Covariates
The following covariates were selected for multivariable analysis: age, living independently, number of close friends, type of partner at last sex (eg, main versus causal) for each partner, and condom use at last sex for each partner.
Analysis
Initial descriptive statistics were performed to examine baseline demographic and sexual relationship characteristics as well as the distributions of social support and the interpersonal factors. To examine the unique levels of social support within the adolescent’s social network, means for each social support subdomain (family, peer, and partner) were calculated separately. Parental monitoring, friend–partner connectedness, and feelings of intimacy for partner were all modeled as continuous variables in the analyses. Bivariate associations between each social support subdomain and (1) parental monitoring, (2) friend–partner connectedness, and (3) feelings of intimacy for partner were assessed by linear regression models accounting for clustering of partner data within a participant. Subsequently, a total of 9 adjusted multivariable linear regression models were performed for each social support subdomain. All analyses were conducted using Stata version 15.
Results
Baseline Demographics and Sexual Relationship Characteristics
Participants were on average 17.9 (standard deviation [SD] 1.0) years old, 94% were African American, 20% lived alone or with peer(s), and had 3.2 (SD 2.6) close friends. Over half (54%) of participants self-reported a positive STI history with an average age at first sex of 14.6 (SD 1.7).
Participants reported having an average of 1.9 (SD 2.7) sexual partners in the past 3 months. Most participants reported on a single sexual partner (range 1-3) at baseline. For the 131 reported sexual relationships, sexual partners were on average 19.9 (SD 3.6) years old, and the majority (95%) were African American. Most (60%) adolescents met their sexual partner on their own; however, 18% were introduced through relatives and 22% were introduced through close friends. Of the reported sexual relationships, 73% were identified as main partners and 47% of participants reported using a condom at last sex with that partner.
Social Support and Interpersonal Factors
Table 1 describes the baseline interpersonal factors and social support reported by female adolescents in the PRSTD study. Each social support subdomain had high internal reliability (family subdomain 4 items, α = .90; peer subdomain 4 items, α = .86; and partner subdomain 4 items, α = .84). Overall, levels of family, peer, and partner social support were high: family mean: 4.00 (95% confidence interval [CI]: 3.83-4.18); peer mean: 4.19 (95% CI: 4.05-4.33); and partner mean: 4.48 (95% CI: 4.36-4.60). Parental monitoring showed high internal reliability (3 items, α = .86). On average, the parental monitoring score was 10.2 (SD 3.2). Almost half (48%) of participants’ close friends knew their sexual partner, while 19% participants reported that only a few or none of their close friends knew their sexual partner. The feelings of intimacy for partner score showed high internal reliability (3 items, α = .87). Overall, participants reported high feelings of intimacy for specific partners with a mean score of 10.1 (SD 2.3).
Interpersonal Factors and Social Support for Female Adolescents in PRSTD.
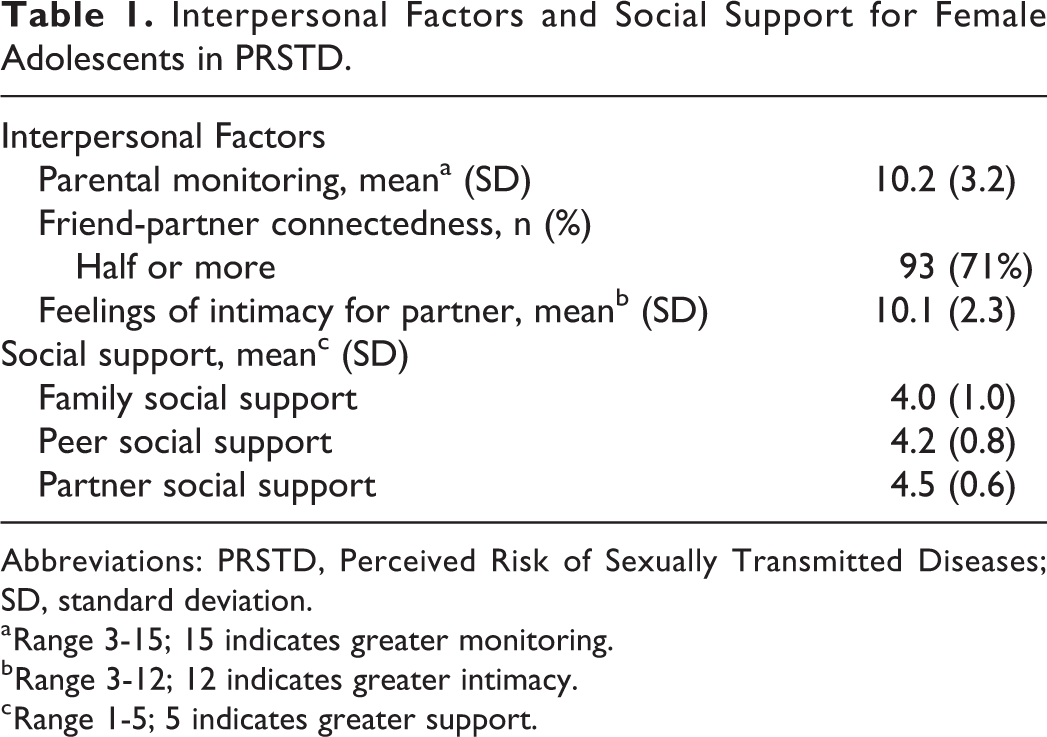
Abbreviations: PRSTD, Perceived Risk of Sexually Transmitted Diseases; SD, standard deviation.
a Range 3-15; 15 indicates greater monitoring.
b Range 3-12; 12 indicates greater intimacy.
c Range 1-5; 5 indicates greater support.
Several interpersonal factors were significantly associated with multiple social support subdomains in unadjusted models. Effect estimates were essentially unchanged after controlling for covariates; therefore, only the adjusted estimates are provided in Table 2. After controlling for covariates, greater parental monitoring was significantly associated with greater family (b = 0.11, P = .001) and peer (b = 0.06, P = .01) social support. Greater friend–partner connectedness was significantly associated with greater family (b = 0.15, P = .02) and peer (b = 0.29, P < .001) social support. Finally, greater feelings of intimacy for a specific partner were significantly associated with greater partner (b = 0.08, P = .02) social support.
Adjusted Regression Coefficients.
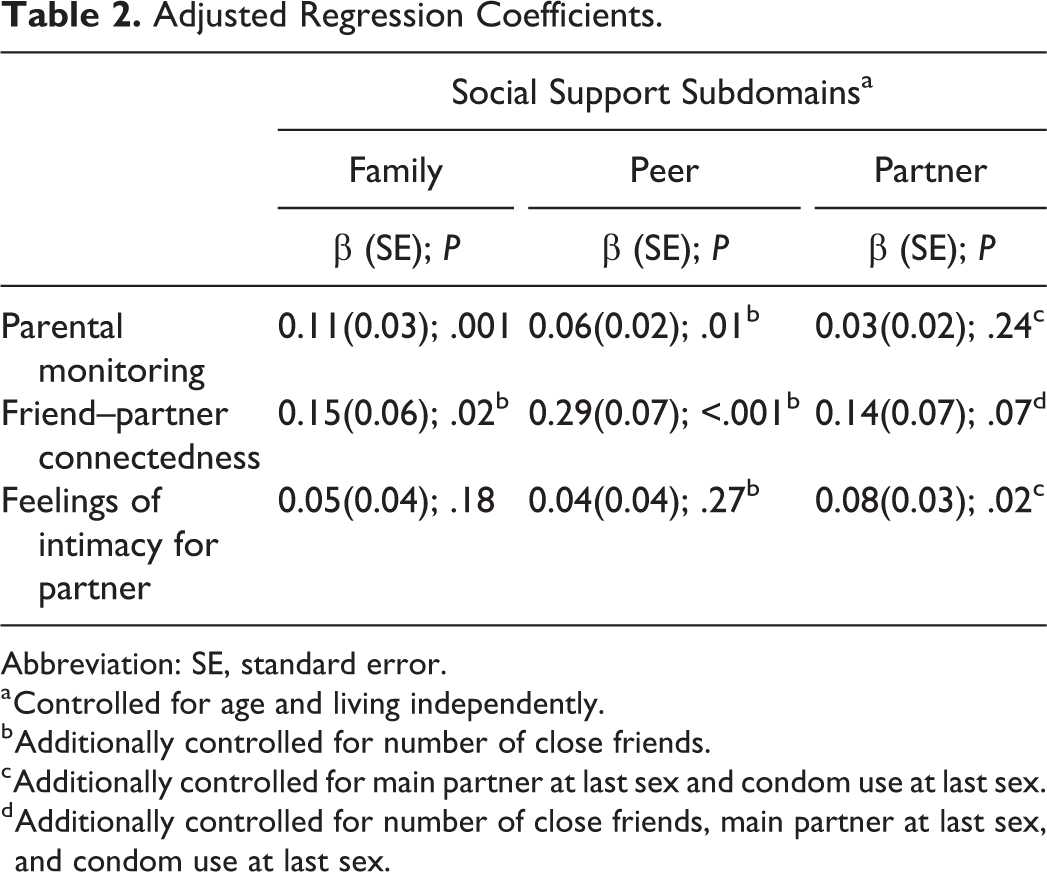
Abbreviation: SE, standard error.
a Controlled for age and living independently.
b Additionally controlled for number of close friends.
c Additionally controlled for main partner at last sex and condom use at last sex.
d Additionally controlled for number of close friends, main partner at last sex, and condom use at last sex.
Discussion
Summary
Importantly, despite living in communities often characterized as disadvantaged, urban female adolescents in this study perceived high levels of family, peer, and partner social support. This speaks to the strength of relationships’ capacity to promote member well-being and act as a safety net. We also note that partner social support had the highest mean which is consistent with normative developmental transitions in an adolescent’s social network in which intimate partners and peers become more proximal in the network, while family becomes less proximal although still critical. 9 This provides a compelling argument to include partners in health promotion interventions.
Furthermore, this study demonstrated that several interpersonal factors are associated with social support from various sources. First, adolescents with greater parental monitoring had greater family and peer support. These findings are consistent with literature that describes how parenting practices (eg, parental monitoring) should be viewed in the context of parent–child relationship qualities (eg, parental support) as opposed to viewing these as separate entities. 10 Furthermore, monitoring may aid in the selection of supportive peers through facilitating, mediating, and supervising these relationships. 11 Second, adolescents with greater friend–partner connectedness had greater family and peer support. This is likely as African American adolescents describe how close friends provide access to and vetting of partners and play a role during the relationship by providing advice on initiation and maintenance of these relationships. 12 Furthermore, friend–partner connectedness has been further associated with condom use for female adolescents in sexual relationships. 13 Finally, female adolescents who report greater feelings of intimacy for their partner report greater support from their partner. Prior research supports this finding as romantic adolescent relationships have been found to be important in providing support and intimacy. 14 Thus, overall social support has the potential to make a significant impact on adolescent sexual health.
Limitations
The findings from the current study should be interpreted in the context of several general limitations. This is a cross-sectional analysis of data; therefore, we cannot infer causality and report only on associations. Second, we had a small sample size from mostly African American heterosexual adolescent girls from a single urban community, which can limit generalizability. Finally, there is no measure of parent–partner connectedness that could provide another examination of connectedness within the social support network.
Significance
Although exploratory, these findings provide important knowledge regarding the correlates of social support for urban female adolescents. Feeling connected to one’s social network and having a connected network is important in social support for urban female adolescents in sexual relationships. Future research targeting interpersonal factors, such as those explored in this study, have the potential to increase social support and subsequently promote positive sexual health behaviors. The study’s findings may be applied to health promotion work seeking to utilize social network-based interventions, specifically focusing on the role of family, peers, and sexual partners in promoting adolescent well-being and positive sexual health behaviors. Past research has further provided evidence for this approach as urban adolescents’ social networks are routinely involved in educating adolescents about sex. 15
SO WHAT?
What is already known on this topic?
Social support is important in promoting adolescent sexual health.
What does this article add?
Feeling connected to one’s social network through parental monitoring and intimacy with a partner as well as having a connected network is an important contribution to social support for urban female adolescents in sexual relationships.
What are the implications for health promotion practice or research?
Targeting interpersonal factors in future research and/or interventions, especially ensuring appropriate parental monitoring, facilitating connecting friends and partners, and involving partners in interventions, may increase social support and subsequently promote positive sexual health behaviors in an urban female adolescent population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Maria Trent: Consultancy: Trojan Sexual Health Advisory Council [Church and Dwight, Inc].
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Maria Trent received funding from National Institutes of Health and an Unrestricted Research Grant from Hologic, Inc to Johns Hopkins University. This work was supported by a National Institute of Child Health and Human Development (NICHD) funded R01 [R01HD058309]. Camille A. Robinson was supported in part by a NICHD funded Adolescent Health Training grant [T32HD052459] and a US Health Resources and Services Administration (HRSA) Leadership Education in Adolescent Health (LEAH) Training grant [T71MC08054]. Pamela A. Matson was supported on an NIDA funded career development award [K01DA035387]. Everyone who contributed significantly to this work has been listed as an author. The study’s funding source did not have any involvement in study design, data analysis, or in the writing of the manuscript.