
Abstract
Introduction:
Holmium laser enucleation of the prostate (HoLEP) is an established surgical technique for treating benign prostatic enlargement with bladder outlet obstruction. Although HoLEP offers advantages such as reduced hospital stays and lower complication rates compared with traditional transurethral resection of the prostate, it presents a steep learning curve for surgeons. The number of procedures required to achieve proficiency remains debated, with estimates differing widely. This study aims to analyze the HoLEP learning curve beyond 200 cases, evaluating perioperative efficiency and complication rates in high-volume surgeons.
Materials and Methods:
A retrospective analysis was conducted on 1724 HoLEP procedures performed between 2015 and 2022 by six surgeons, three of whom had performed over 200 cases each. Key parameters assessed included operative time, enucleation efficiency, energy use, and complication rates. Statistical analyses included univariate and multivariate regression models to identify predictors of postoperative complications and efficiency improvements.
Results:
The mean patient age was 70.48 years, with an average prostate volume of 93.43 g. The mean operative time was 80.68 minutes, with significant efficiency improvements correlating with increased surgeon experience (p < 0.001). Complication rates, including bleeding necessitating coagulation (4.7%) and urinary retention (9.3%), decreased significantly beyond 350 cases. Learning curves demonstrated a nonlinear reduction in complications and a continuous increase in surgical efficiency, with operative proficiency plateauing after approximately 350 procedures.
Conclusion:
Contrary to previous studies suggesting HoLEP proficiency after 50 to 60 cases, our findings indicate ongoing improvements beyond 200 cases, with stable complication rates achieved after 350 procedures. Structured mentorship programs and simulation-based training could facilitate faster learning and enhance patient outcomes.
Introduction
Benign prostatic enlargement leading to bladder outlet obstruction (BOO) is a common condition with a prevalence that increases with age. 1 In most cases, surgical intervention remains the primary treatment modality. Historically, transurethral resection of the prostate (TURP) has been regarded as the gold standard for managing BOO. However, in recent years, holmium laser enucleation of the prostate (HoLEP) has gained prominence as the preferred technique because of its shorter hospitalization time, lower complication rates, and superior functional outcomes. 2 In addition, evidence suggests that HoLEP can be safely performed in patients undergoing anticoagulant therapy without compromising clinical outcomes. 3
Despite its advantages, HoLEP is often associated with a steep learning curve, which raises concerns among urologists. 4 Even experienced endourologists may encounter perioperative complications and long-term sequelae as they refine their technique. 5 Common perioperative complications include postoperative bleeding, urinary retention, and febrile episodes. Other key parameters used to assess the learning curve include operative time, procedural efficiency, enucleation ratio, and length of hospital stay. 6
Most studies evaluating the HoLEP learning curve are based on case series of fewer than 200 procedures. There is no consensus on the number of cases required to achieve surgical proficiency with acceptable complication rates and long-term outcomes. Estimates range from 20 to 60 cases, although significant variability in enucleation and morcellation efficiency has been observed even beyond 150 procedures. 7,8
Currently, limited data exist on the evolution of the HoLEP learning curve beyond 200 cases. This study aims to systematically assess and quantify perioperative factors and complications in surgeons with experience exceeding 800 procedures. By doing so, we seek to determine whether key parameters such as surgical efficiency and complication rates continue to improve over extended periods of practice.
Patients and Methods
We conducted a retrospective analysis of consecutive perioperative data from all patients who underwent HoLEP for BOO between September 2015 and October 2022, using our institutional clinical information system. A total of 1724 procedures were performed by six surgeons, three of whom conducted the majority (226, 470, and 820 procedures, accounting for ∼88%), whereas the remaining three performed 117, 49, and 42 HoLEPs. Thirteen cases with a resectate weight below 10 g were excluded.
Surgical techniques included the classical three-lobe approach or the three horseshoe incision with en bloc enucleation, as described by Miernik and Schoeb (2019). 9 A 26F continuous-flow laser resectoscope and a mechanical tissue morcellator (Richard Wolf GmbH, Knittlingen, Germany) were used. HoLEP was performed with a 100 W Holmium-YAG laser (520-µm fiber) at an energy of 3 J, frequency of 28 Hz, and pulse duration of 750 µs. Coagulation was achieved using a monopolar resectoscope with either a cutting loop or a roller probe (Richard Wolf GmbH, Knittlingen, Germany). Nearly all procedures were conducted under general anesthesia. Antibiotic prophylaxis was administered either 2 days preoperatively in case of a positive urine culture or as a single intravenous dose otherwise. Non-vitamin K antagonist oral anticoagulants were discontinued for 2 days, antiplatelet drugs (excluding aspirin) for 7–10 days, and vitamin K antagonists were bridged with low-dose heparins for 10 days preoperatively. Postoperatively, a three-way Foley catheter was inserted for continuous bladder irrigation and removed after 2 days, with postvoid residual volume (PVR) measured before discharge on postoperative day 2 or 3.
Preoperative parameters included patient age, prostate specific antigen (PSA) level, prostate volume, American Society of Anesthesiologists physical status classification system (ASA) score, anticoagulant/antiplatelet medication (AC/AP), and presence of an indwelling catheter. Postoperative outcomes assessed were bleeding, urinary retention, and fever (temperature >38.5°C). Urinary retention was only considered if unrelated to bleeding. Bleeding was further categorized into cases necessitating manual clot evacuation vs those necessitating transurethral coagulation. Manual clot evacuation was defined as the removal of intravesical clots via a transurethral catheter at the bedside without anesthesia, whereas transurethral coagulation referred to surgical hemostasis performed under general anesthesia in the operating room. Additional parameters included total energy used (Joules), resected prostate mass (g), operative time (minutes), hospital stay (days), and postoperative pain measured via the cumulative analgesic consumption score (CACS). 10 Postoperative complications were classified according to the Clavien–Dindo (CD) grading system to enable standardized assessment of complication severity.
Learning curves were evaluated by analyzing the relationship between the number of procedures performed and key efficiency and complication parameters. The following outcome variables were tested: enucleation efficiency (g/min), laser-to-prostate ratio (J/g), enucleation ratio, urinary retention, transurethral coagulation, clot evacuation, fever, overall complication rate, postoperative pain (CACS), and length of hospitalization (<4 days vs >4 days). Depending on the scale of the variable, either linear or logistic univariate regression was performed using the Scikit-learn package in Python.
For parameters with a statistically significant association with case number, learning curves were subsequently observed, and the number of procedures required for plateau formation was evaluated to illustrate the dynamics of performance stabilization over time.
Multivariate regression models were used to identify predictors of postoperative complications. Statistical significance was set at p < 0.05. The study was approved by the local ethics committee and conducted in accordance with the ethical standards of the Declaration of Helsinki.
Results
The mean age of patients undergoing HoLEP was 70.48 years (range: 47–92), with a mean prostate volume of 93.43 g (15–450) and a preoperative PSA level of 7.48 ng/mL (0.03–174). The mean ASA score was 2.26 (1–4), with 32.2% (n = 557) of patients requiring an indwelling catheter and 15.6% (n = 267) receiving AC/AP therapy beyond aspirin. The mean operative time was 80.68 minutes (23–322), with an average energy use of 54,779.31 J (4100–532,919) and a mean prostate resectate weight of 73.06 g (10–430). The mean CACS was 5.3 (0–45). A total of 29.5% (n = 510) of patients had prolonged hospitalization exceeding 4 days (Table 1).
Baseline Characteristics and Perioperative Parameters
Baseline characteristics of the patient cohort and perioperative parameters, presented as mean ± standard deviation (SD).
AC/AP = anticoagulant/antiplatelet medication; CACS = cumulative analgesic consumption score; PVR = postvoid residual volume.
Postoperative complications included urinary retention in 9.3% (n = 160, CD I), clot retention in 7.8% (n = 134, CD I), bleeding requiring transurethral coagulation in 4.7% (n = 82, CD IIIb), and fever in 3.0% (n = 52, CD II). Less frequent complications, such as capsule perforation (1.4%, n = 24, CD I), bladder wall injury (1.4%, n = 23, CD I), blood transfusion (0.8%, n = 14, CD II), and Double J (DJ) stent placement (0.5%, n = 8, CD IIIa), were not further analyzed because of their low incidence (Fig. 1). DJ stents were placed because of injuries to the ureteral orifice, which led to a significant increase in serum creatinine levels. Mean values for key efficiency parameters were also calculated, with an enucleation ratio efficiency of 0.76 (0.11–2), operative efficiency of 0.91 g/min (0.06–5.41), and a laser-to-prostate ratio of 892.36 J/g (32.03–9662.4).
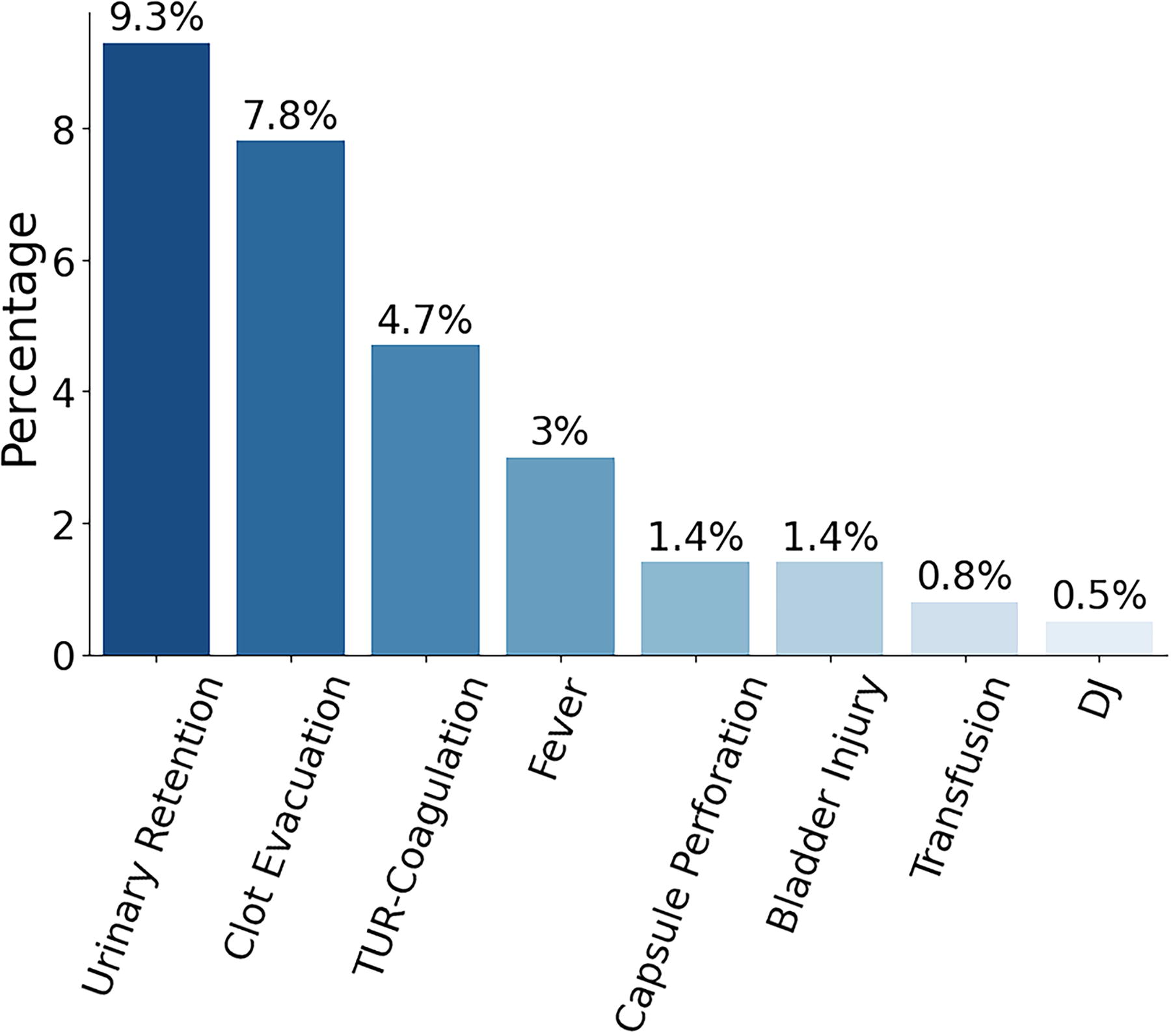
Perioperative complications after holmium laser enucleation of the prostate (HoLEP): Incidence of perioperative complications (%) within 30 days postoperatively in our cohort after HoLEP.
Univariate regression analysis demonstrated a significant correlation between surgeon experience and the overall complication rate (p = 0.009). When evaluating individual complications, a significant association was found between experience and bleeding necessitating transurethral coagulation (p = 0.001), as well as urinary retention (p = 0.007). However, no significant correlation was observed for clot retention (p = 0.467) or fever (p = 0.181). The surgeon’s experience did not influence the duration of hospitalization (p = 0.382). Operative efficiency improved significantly with increasing case numbers (p < 0.001), and laser energy usage per gram of resected prostate tissue decreased accordingly (p < 0.001). In contrast, the proportion of resected tissue relative to prostate size (p = 0.871) and postoperative pain perception (CACS) (p = 0.278) remained unchanged with increasing experience.
Multivariate regression analysis identified several predictors of postoperative complications. No independent predictors were found for the development of fever. Bleeding necessitating transurethral coagulation was significantly associated with larger prostate volume (p = 0.035, odds ratio (OR) = 1.004), AC/AP therapy (p = 0.005, OR = 2.31), and lower surgeon experience (p < 0.001, OR = 0.9976). Clot retention was predicted by increasing patient age (p = 0.008, OR = 1.033) and AC/AP therapy (p < 0.001, OR = 2.68). Several factors influenced the likelihood of urinary retention, including higher ASA scores (ASA 2: p = 0.039, OR = 2.958; ASA 3: p = 0.003, OR = 4.97), as well as increasing patient age (p = 0.002, OR = 1.036). Conversely, larger prostate volume (p = 0.008, OR = 0.9939) and greater surgeon experience (p = 0.009, OR = 0.9988) were associated with a reduced likelihood of urinary retention. The overall complication rate increased with advancing patient age (p < 0.001, OR = 1.034) and AC/AP therapy (p < 0.001, OR = 1.92), whereas increasing surgeon experience significantly reduced the probability of complications (p = 0.003, OR = 0.9991). Prolonged hospitalization (>4 days) was independently associated with higher ASA scores (ASA 2: p = 0.042, OR = 1.601; ASA 3: p = 0.015, OR = 1.82), older age (p < 0.001, OR = 1.036), AC/AP therapy (p = 0.008, OR = 1.52), and larger prostate volume (p < 0.001, OR = 1.004).
Visual analysis of learning curves demonstrated that complication rates decreased with experience, but not in a strictly linear manner. The incidence of urinary retention declined to a consistently lower level after approximately 175 procedures, whereas bleeding requiring transurethral coagulation showed a delayed decrease, stabilizing only after 350 procedures, despite an earlier phase with minimal cases. The overall complication rate followed a similar pattern, decreasing significantly after 350 procedures. In contrast, operative efficiency exhibited a nearly linear improvement, doubling after approximately 600 procedures compared with initial cases. The laser-to-prostate ratio also showed a steady decline, stabilizing after 100 procedures, despite an initial dip around 50 cases (Fig. 2). No clear correlation was observed between the number of procedures performed and other perioperative outcome measures.

Learning curves for key parameters in relation to surgeon experience. Observation of learning curves for significant perioperative parameters plotted against the number of HoLEP procedures performed by the surgeon.
Discussion
This study presents the learning curves of three surgeons with extensive HoLEP experience, having performed 226, 470, and 820 procedures. Previous studies have primarily analyzed case numbers ranging from 20 to 250, often concluding that HoLEP has a steep learning curve, with a plateau occurring after 30 to 50 cases. 11 Although a systematic review supports this estimate, it applies primarily to a selected patient cohort. 6 However, Sie and colleagues (2022) observed ongoing improvements beyond 60 cases, suggesting that this threshold may be insufficient for achieving consistent surgical outcomes. 12 Our findings align with this perspective, demonstrating that learning continues beyond 200 cases, as reflected in parameters such as laser utilization and operative times. In addition, perioperative complication rates, occurring in at least 2% of cases, were evaluated as part of the learning curve.
A closer examination of perioperative complications reveals low rates of intraoperative adverse events in our cohort, such as capsule perforations (1.4%) and bladder wall injuries (1.4%), with no cases requiring conversion to TURP. Transfusion rates (0.8%) and postoperative fever rates (3%) were comparable with those reported in the literature. Notably, the incidence of urinary retention (9.3%) in our study was higher. 13 However, it must be considered that our analysis included four surgeons who had not yet completed their learning curves. Studies evaluating multiple surgeons similarly reported elevated rates of postoperative urinary retention during the early phases of training. 14 Regarding postoperative bleeding events, our cohort demonstrated relatively higher rates compared with the study by Capogrosso and associates who observed lower rates of bleeding complications, likely because of the fact that only 2% of their patient population was on anticoagulant therapy.
The impact of surgical experience became evident after approximately 350 cases, particularly through reductions in transurethral coagulation rates and urinary retention, whereas clot retention and postoperative fever remained unaffected. This contrasts with Brunckhorst and coworkers (2016), who found no statistically significant learning effect regarding complication rates over 253 consecutive cases performed by a single surgeon. They proposed that either complications are not an appropriate metric for learning curves or that the time to plateau (TTP) is longer than previously assumed. 7 Our data support the latter hypothesis, highlighting the extensive experience required to achieve consistently low complication rates. Similarly, Soto-Mesa and colleagues (2015) found no difference in complication rates between a surgeon’s first and subsequent 50 cases. 15
Multivariate regression analysis confirmed that surgical experience significantly reduces the likelihood of transurethral coagulation and urinary retention, whereas hospitalization duration, clot retention, and postoperative fever were independent of case numbers. Some studies contradict this finding, arguing that prostate size and ASA status, rather than case volume, are the primary determinants of complications. 16,17 A frequently cited risk factor for postoperative complications is patient age. 18 Our data confirm that age and prostate volume influence hospitalization duration, with age increasing overall complication rates, whereas prostate size primarily affects transurethral coagulation and urinary retention without altering total complication rates. A higher ASA score was only associated with an increased risk of urinary retention. Therefore, early-stage HoLEP surgeons should prioritize moderate-sized prostates, as this allows for faster technical mastery and independent practice within a manageable number of cases. 19,20
Another key predictor of complications was AC/AP medication, which primarily increased the risk of clot retention and transurethral coagulation, consequently prolonging hospital stay. Most studies confirm the general safety of HoLEP in patients on bridged AC/AP therapy while acknowledging higher overall complication rates. 21,22 Despite an increased need for transurethral coagulation in our cohort, our findings align with this conclusion. However, continuous AC/AP therapy without bridging would substantially elevate bleeding risk, even though studies with smaller prostates suggest feasibility and safety under such conditions. 3
Surgical efficiency, particularly laser-to-prostate ratio and operative efficiency, showed a clear correlation with experience. Operative efficiency demonstrated a linear improvement, continuing even after several hundred procedures. Placer and associates (2009) analyzed enucleation and morcellation efficiency separately, demonstrating a linear increase in enucleation speed over the first 125 cases, which is consistent with our findings. 23 However, some studies report a plateau in operative efficiency after 50 to 60 or even 25 cases. 7,8 Sie et al. (2023) estimated the TTP for operative efficiency to be between 30 and 50 cases, but acknowledged that learning was still ongoing at the end of their observation period, particularly for certain surgeons. 12 Although a direct comparison with our study is limited because of differences in monthly case density, our findings reinforce the notion that learning continues beyond 60 cases. Kosiba et al. also reported progressive improvements in enucleation speed beyond 200 cases, supporting this interpretation. 16
Regarding laser efficiency, our data suggest that the learning curve reaches a plateau after approximately 150 cases. Prior studies have similarly demonstrated a progressive reduction in laser time with experience. Dusing et al. (2010) reported a statistically significant decrease in laser time in later cases, independent of prostate size, and found a negative correlation between laser use and case numbers. 24 Elshal et al. (2017) also described a linear decline in laser use, reaching a plateau after approximately 20 cases. 25 Although our data exhibit some variability, the overall trend supports continued improvement, with a later plateau at 150 cases.
After the initial implementation of the HoLEP technique by two experienced endourologists, surgical training was gradually expanded to include additional trainees. During their first 30 procedures, trainees received close supervision and progressively took over individual steps of the operation. After this initial phase, senior surgeons were present on call only. This structured teaching approach may have influenced perioperative outcomes in the early learning phase and could partially explain the initial drop in urinary retention rates observed in the learning curves. To promote earlier independence from close supervision, future training could benefit from preclinical rehearsal using realistic phantom models. Recent studies have demonstrated the feasibility and educational value of such simulations in replicating various enucleation techniques. 26
Despite its strengths, this study has several limitations. As a monocentric retrospective study, the findings may have limited generalizability, particularly as most surgeons had prior endourological experience. In addition, our cohort included patients with prostate cancer, AC/AP therapy, and indwelling catheters, which are often excluded in other studies. Given this heterogeneity, we did not assess functional outcomes, such as PVR, uroflow, or International Prostate Symptom scores. A common benchmark for evaluating HoLEP learning curves is the trifecta or pentafecta concept. 4 However, because of the large prostate sizes in our cohort and the absence of continence assessment, these criteria were not applicable in our analysis.
Conclusions
Most studies suggest that the HoLEP learning curve plateaus between 20 and 60 cases. However, our findings indicate that learning continues far beyond this range. Although surgeons may gain confidence and operate independently after 50 to 60 procedures, achieving optimal efficiency and minimal complication rates requires significantly more experience. Based on our data, we propose that the learning curve reaches completion after approximately 350 cases, as complication rates stabilize at a low level despite further improvements in operative efficiency. Given the prolonged learning process, structured mentorship programs and simulation-based training should be encouraged to enhance surgical proficiency, minimize complications, and optimize patient outcomes.
Footnotes
Authors’ Contributions
M.G.: Article writing, data collection, data analysis, and project development. A.M., A.S., and M.S.: Protocol development. M.F.v.B.: Data management. A.Ö., D.S.S., K.W., and C.G.: Article editing.
Author Disclosure Statement
A.M. receives research funds from the German Federal Ministry of Education and Research, Berlin (D). He receives support for his travel activities from the European Society of Urology, Arnhem (NL) and the German Society of Urology, Düsseldorf (D). Furthermore, A.M. is consulted for the following: KLS Martin, Tuttlingen (D), Avateramedical, Jena (D), LISA Laser Products GmbH, Katlenburg-Lindau (D), Schoelly fiberoptics GmbH, Denzlingen (D), Dornier MedTech Systems GmbH (D), Medi-Tate Ltd. (IL, USA), and (B) Braun New Ventures GmbH, Freiburg (D). A.M. is a speaker for the companies Richard Wolf GmbH (D) and Boston Scientific (USA). In addition, he performed expert activities for the Ludwig Boltzmann Gesellschaft, Wien (A). A.M. is involved in numerous patents and inventions in the field of medical technology. C.G. is an adviser for Astellas Pharma GmbH, DE, IpsenPharma GmbH, DE, Steba Biotech S.A., LUX, Bayer Pharma, DE, Olympus Winter & Ibe GmbH, DE, Medi-Tate Ltd., IL, MSD, DE, Astra-Zeneca, UK, and Roche, CH. He receives speaker fees from Amgen, USA, Astellas Pharma GmbH, DE, Ipsen Pharma GmbH, DE, Janssen-Cilag GmbH, BEL, Bayer Pharma, DE, Takeda Pharmaceuticals, JPN, and medac GmbH, DE. M.G., A.S., M.F.v.B., M.S., A.Ö., D.S.S., and K.W. declare to have no conflicts of interest.
Funding Information
No funds, grants, or other support were received.