
Abstract
Objective:
Retrograde intrarenal surgery is limited by the narrow caliber of the human ureter, resulting in both reluctance to deploy larger ureteral access sheaths and, at times, failed primary ureteral access, requiring placement of a ureteral stent and a delayed second procedure. In this study, we sought to evaluate the application of electromotive drug administration (EMDA) to deliver smooth muscle relaxants to the porcine ureter to facilitate acute ureteral dilation.
Methods:
Eighteen juvenile female Yorkshire pigs were randomized into three treatment groups (alfuzosin, aminophylline, or isoproterenol; n = 6 per group). Within each animal, one ureter received an intraureteral drug infusion with EMDA, while the contralateral ureter served as a control, receiving 0.9% normal saline (NS). Ureteral size was assessed before and after treatment by passing sequentially larger urethral dilators starting at 10 Fr, with a maximum insertion force of 3.5 N.
Results:
Only alfuzosin with EMDA increased ureteral size compared with NS alone (alfuzosin vs NS, 0.8 Fr vs 0.1 Fr, p = 0.031). Neither aminophylline nor isoproterenol with EMDA resulted in a significant increase in ureteral size compared with their respective NS controls (aminophylline vs NS, 0.3 Fr vs −0.6 Fr, p = 0.344; isoproterenol vs NS, 0.1 Fr vs −0.4 Fr, p = 0.125).
Conclusion:
In this first report, EMDA-mediated in vivo delivery of alfuzosin into the porcine ureter acutely increased ureteral distensibility.
Keywords
Introduction
Retrograde intrarenal surgery (RIRS) is the gold standard for treating kidney stones smaller than 2 cm. 1 Ureteral access sheaths (UAS) are commonly used in RIRS to provide safe, repeated ureteroscope passage into the kidney, thereby reducing surgical time, decreasing intrarenal pressure, improving visualization, and enhancing stone-free status.2–5 Despite these benefits, reluctance to utilize UAS persists due to concerns regarding the ureter’s fragile anatomy; low-grade ureteral injuries occur in almost half of cases, while a complete ureteral wall tear occurs in up to a fourth of patients. 6 Additionally, the ureter’s narrow caliber leads to a 15% failure rate of primary access, often requiring passive dilation with an indwelling stent and a delayed secondary procedure. 7
Given these challenges, there is growing interest in methods to acutely dilate the ureter intraoperatively to facilitate the safe passage of larger UAS and reduce failed primary access. Smooth muscle relaxants (SMRs) offer a potential solution due to the presence of alpha, beta, and muscarinic receptors in the ureter.8–15 To date, ureteral infusion of SMRs has yielded equivocal results.16–18 The urothelium, reinforced by a glycosaminoglycan layer, limits localized drug absorption, whereas peristalsis, urine dilution, and retrograde infusion challenges hinder efficient intraureteral drug delivery. 19
In order to deliver drug across the urothelium and into the ureteral smooth muscle, electromotive drug administration (EMDA) employs a low electrical current to enhance the delivery of charged drug molecules deep into tissues through electroporation, electrophoresis, and iontophoresis. 20 In Urology, EMDA has been utilized to treat non-invasive bladder cancer, overactive bladder, bladder pain syndrome, and radiation cystitis, as well as to deliver analgesics before transurethral procedures.20,21 To apply EMDA to the upper urinary tract (UUT), we developed novel EMDA ureteral and renal pelvis catheters.22,23 Initial studies in the porcine ureter and renal pelvis demonstrated safe and effective delivery of methylene blue into the lamina propria without significant urothelial damage.22,23
Based on these findings, we proceeded to evaluate the impact of EMDA on ureteral relaxation using three SMRs: alfuzosin, a nonselective alpha-1-adrenergic antagonist; isoproterenol, a nonselective beta-adrenergic agonist; and aminophylline, a competitive nonselective phosphodiesterase inhibitor.24–26 These drugs were selected for their small molecular weight (200–400 Da), chemically charged nature, and high water solubility, thereby increasing the likelihood of EMDA-induced urothelial penetration.
Materials and Methods
Regulatory approval and randomization
With Institutional Animal Care and Use Committee approval at the University of California, Irvine (Animal Use Protocol-21-131), 18 juvenile female Yorkshire pigs (Premier BioSource, Ramona, CA) were randomly assigned to three drug groups (n = 6/group): alfuzosin, aminophylline, or isoproterenol. Each ureter in each group had an EMDA catheter placed and was then randomized to receive either intra-ureteral medication in normal saline (NS) with activated EMDA or NS infusion only without medication or activation of the EMDA catheter.
Animal preparation and general anesthesia
Preanesthetic sedation was administered intramuscularly using xylazine (2 mg/kg) and Telazol (6–8 mg/kg). After endotracheal intubation, general anesthesia was induced with 4%–5% isoflurane and maintained at 1.5%–2.5%. A skin dispersive grounding pad (11.5 × 7.5 in.) was placed on the shaved flank between the costal margin and anterior superior iliac spine on the side randomized to EMDA-activated drug treatment. The pad was connected to the negative anode of the MINI 30N2 EMDA machine (Physion Srl, Mirandola, Italy).
Cystoscopy and ureteral access
Flexible cystoscopy (Karl Storz, Tuttlingen, Germany) was performed, and both ureteral orifices were individually cannulated with 0.035-inch straight hydrophilic Glidewires (Terumo Medical, Somerset, NJ) to provide renal pelvis access. A 5 French (Fr) open-ended ureteral catheter (Cook Medical, Bloomington, IN) was passed over both guidewires, followed by retrograde pyeloureterograms using 1:1 saline-diluted Omnipaque contrast (GE Healthcare, Chicago, IL). Subsequently, bilateral Amplatz Super Stiff guidewires were inserted, and the open-ended ureteral catheters were removed (Boston Scientific, Marlborough, MA).
Initial ureteral sizing
Ureteral sizing was performed bilaterally using sequential urethral dilators (Cook Medical), starting at 10 Fr and increasing in 2 Fr increments under low-dose fluoroscopy using a novel University of California, Irvine Force Sensor (Fig. 1). Dilator size and the location in the ureter (distal, middle, or proximal ureter) at which 3.5 N were reached were recorded.
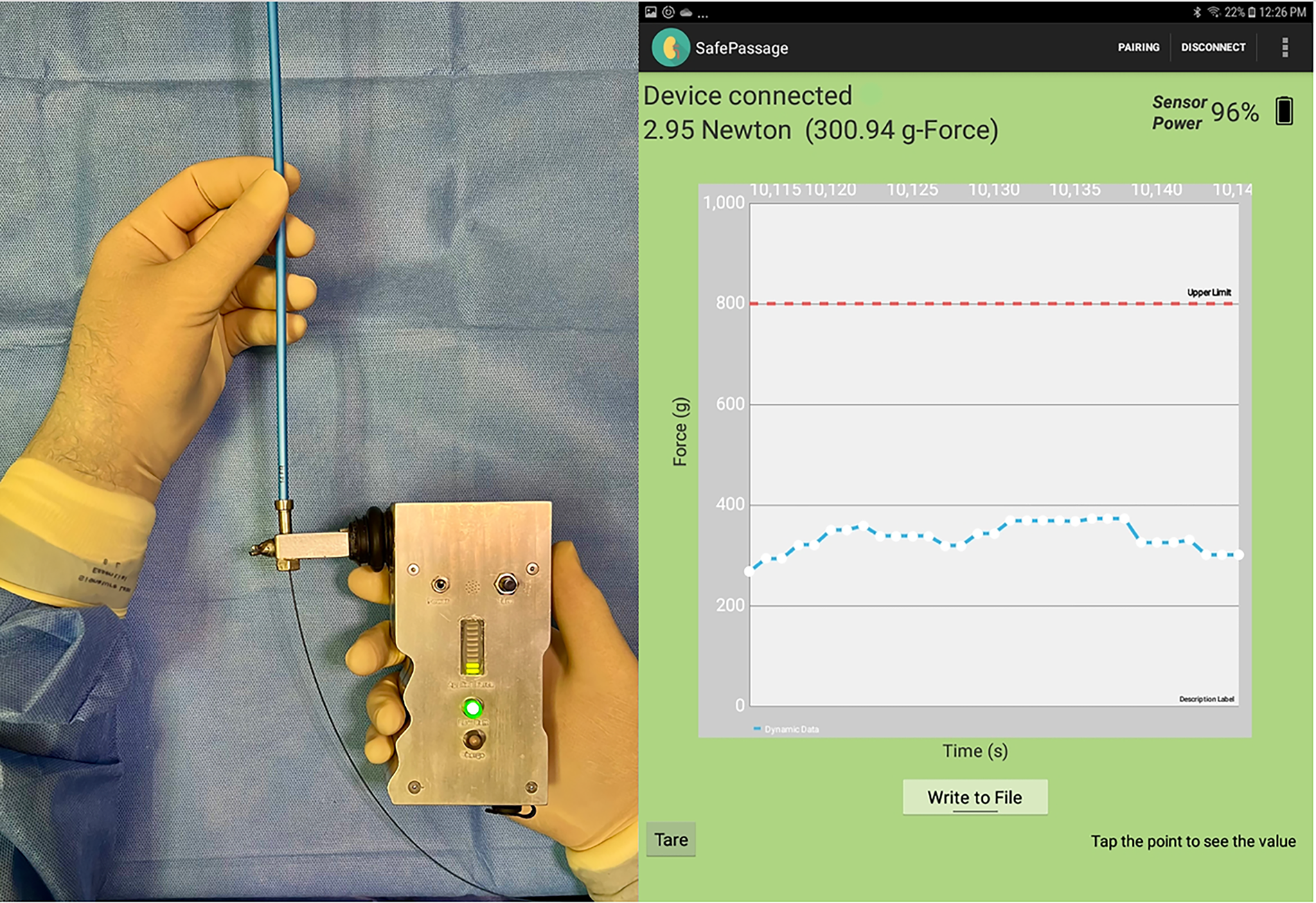
The UCI force sensor. Passage of a 14 Fr urethral dilator (Cook Medical, Bloomington, IN) over a guidewire with the UCI force sensor (left) with an example force reading (right). UCI = University of California.
Drug infusion and EMDA
After ureteral sizing, Amplatz Super Stiff guidewires were exchanged for EMDA catheters. Catheters were fabricated by modifying the distal 20 cm of 35 cm, 11 Fr Navigator obturators from a 13 Fr UAS (Boston Scientific); 1.0 mm fenestrations were placed 0.5 mm apart in three equidistant longitudinal rows (Fig. 2). Polytetrafluoroethylene-insulated 22 AWG 99.9% pure silver wires (Tempo Electric, Saratoga Springs, NY) with a 0.5 mm insulated tip were inserted into each catheter, providing 20 cm of exposed wire (Fig. 3). A three-port adaptor was connected to the EMDA catheter.

Schematics of custom catheters for EMDA.

The silver wire anode was connected to the EMDA generator via one port. Drug solutions (isoproterenol 1 mg/100 mL, aminophylline 500 mg/100 mL, or alfuzosin 10 mg/100 mL prepared in sterile water) were infused through a second port at 5 mL/min. Of note, due to the insulated enlarged tip of the silver wire, no drug could exit the tip of the EMDA catheter; as such, the infused drug was localized to the ureter. The third port was connected to a central venous pressure column to maintain intrarenal pressure below 40 cm H2O and prevent pyelovenous/lymphatic/sinus backflow. No current was applied to the EMDA catheter on the NS control side. A drug infusion on the control group without EMDA was avoided due to earlier studies suggesting that the topical ipsilateral ureteral application of an SMR may induce relaxation in the contralateral ureter. 18
Based on prior human skin studies on safe electrical current density (0.5 mA/cm2) and an estimated juvenile porcine ureteral lumen surface area in contact with our EMDA catheter of roughly 24 cm2, a pulsed direct current of 10 mA was selected. 27 On the experimental side, EMDA was applied for 20 minutes, with concurrent drug infusion at a rate of 5 mL/min. For the control side, no current was applied, and saline was infused at 5 mL/min for 20 minutes (Fig. 4).

Schematics of the in vivo experimental setup with EMDA in a female pig. Bilateral EMDA catheters are positioned in the porcine ureters, with the distal ends terminating in the renal pelvis. On the control side (right), the EMDA catheter is only connected to an infusion of normal saline without EMDA. On the experimental side (left), the EMDA catheter is connected to an infusion of smooth muscle relaxant (alfuzosin, aminophylline, or isoproterenol) with pulsed direct current EMDA at 10 mA. Both sides are connected to a CVP line to maintain intrarenal pressure below 40 cm H2O. CVP = central venous pressure.
Ureteral sizing post-treatment
After treatment, EMDA catheters were removed, and ureteral sizing was repeated. Flexible ureteroscopy was performed to assign a Post-Ureteroscopic Lesion Scale (PULS) grade. Ureters exhibiting high-grade PULS 3 ureteral injuries (i.e., full-thickness splitting of the ureteral wall with visualization of periureteral fat) were excluded. Animals were euthanized using intravenous pentobarbital sodium and phenytoin sodium.
Ureteral sizing measurement and data analysis
The ureteral size was determined in two ways: (1) recording the maximum dilator size (Fr) that could be advanced to the renal pelvis while maintaining insertion forces ≤3.5 N and (2) noting the furthest ureteral segment reached at the time of dilator failure at ≤3.5 N. Ureteral dilation was quantified using a ureteral size scale (USS): 3 points for each 1 Fr increase in dilator size successfully passed to the ureteropelvic junction, starting from 10 Fr (e.g., 10 Fr = 3 points, 11 Fr = 3 additional points). Additionally, 1–3 points were awarded for the furthest ureteral segment (distal, middle, and proximal) reached by the largest dilator at 3.5 N (Supplementary Appendix).
Descriptive statistics were conducted for porcine demographics, USS, and dilator size. A Kolmogorov–Smirnov test assessed data normality. Parametric data were analyzed using analysis of variance with Tukey post hoc tests, while nonparametric data were analyzed using the Kruskal–Wallis test with Dunn’s post hoc analysis. A generalized estimating equation model, followed by Bonferroni adjustment, was employed to conduct pairwise comparisons between intra- and inter-treatment groups for pre- and post-treatment USS and dilator French size. For the purposes of this study, dilator size was treated as a continuous variable.
Additionally, mean differences in pre- and post-infusion USS within the same ureter and changes in pre-infusion and post-infusion USS between experimental and control ureters within the same drug group were assessed using the Wilcoxon signed-rank test. Statistical analyses were performed using GraphPad Prism for macOS, Version 10.1 (GraphPad Software, Boston, MA) and IBM Statistical Package for the Social Sciences Statistics for Windows, Version 29.0.0.0 (241) (IBM Corp., Armonk, NY). Biostatistical support was provided by the Chao Family Comprehensive Cancer Center Biostatistics Shared Resource at UCI.
Results
Demographics
The average swine age was 88.5 ± 13.1 days. Swine in the isoproterenol group were significantly older compared with those in the aminophylline group (98.3 days vs 79.5 days; p = 0.027). (Table 1). The average weight of the swine was 41.11 ± 8.52 kg, with no significant differences observed between any groups (p > 0.999 for alfuzosin vs aminophylline or isoproterenol; p = 0.701 for aminophylline vs isoproterenol) (Table 1).
Mean, Standard Deviation, and Mean Comparison of Age and Weight of Female Juvenile Yorkshire Swine in Each Drug Group

The bolded values indicate a significant p-value of less than 0.05.
SD = standard deviation.
Pretreatment ureteral size (baseline)
The mean baseline ureteral size, measured by dilator French size and USS, showed no significant differences across all treatment groups (p > 0.999) (Tables 2 and 3).
Mean Ureteral French Size in Normal Saline Infusion Only Control Groups and Drug Administration with Electromotive Drug Administration Experimental Groups

EMDA = electromotive drug administration; NS = normal saline.
Mean Ureteral Size Scale in Normal Saline Infusion Only Control Groups and Drug Administration with Electromotive Drug Administration Experimental Groups
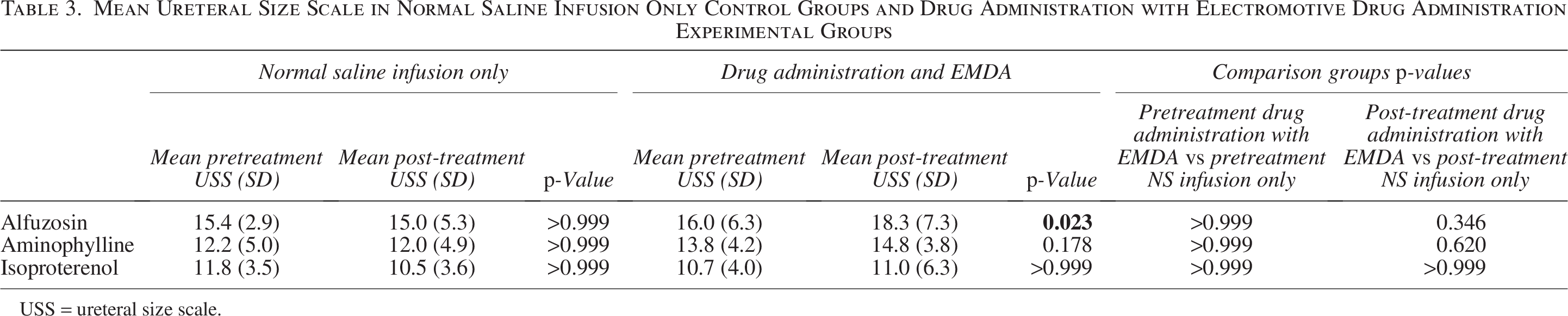
USS = ureteral size scale.
Effect of ureteral dilator passage on ureteral size
The mean pretreatment ureteral size was compared with the mean post-treatment ureteral size in the three NS control groups to assess the effect of ureteral dilator passage on ureteral size.
There was no difference in French size before and after ureteral dilator passage with NS infusion alone (alfuzosin 14.3 ± 0.82 F vs 14.3 ± 2.0 F, p > 0.999; aminophylline 13.3 ± 1.6 F vs 13.3 ± 1.6 F, p = not calculable; isoproterenol 13.3 ± 1.0 F vs 13.0 ± 1.1 F, p > 0.999) (Table 2).
Similarly, there was no difference in USS before and after ureteral dilator passage with NS infusion alone (alfuzosin 15.4 ± 2.9 vs 15.0 ± 5.3, p > 0.999; aminophylline 12.2 ± 5.0 vs 12.0 ± 4.9, p > 0.999; isoproterenol 11.8 ± 3.5 vs 10.5 ± 3.6, p > 0.999) (Table 3).
Effect of SMR administration with EMDA on ureteral size
The mean pretreatment ureteral size was compared with the mean post-treatment ureteral size in the three experimental groups (SMR administered with EMDA).
There was no difference in ureteral French size before and after SMR and EMDA administration in all three experimental groups (alfuzosin 14.7 ± 2.1 F vs 15.3 ± 2.4 F, p > 0.999; aminophylline 14.0 ± 1.3 F vs 14.0 ± 1.3 F, p = not calculable; isoproterenol 13.0 ± 1.1 vs 13.0 ± 2.1, p > 0.999) (Table 2).
Alfuzosin with EMDA administration significantly increased USS (16.0 ± 6.3 vs 18.3 ± 7.3, p = 0.023). No significant changes were observed with aminophylline or isoproterenol administered with EMDA (aminophylline 13.8 ± 4.2 vs 14.8 ± 3.8, p = not calculable; isoproterenol 10.7 ± 4.0 vs 11.0 ± 6.3, p > 0.999) (Table 3).
Effect of SMR administration with EMDA vs NS infusion alone
The mean change in USS (post-treatment minus pretreatment) was compared between experimental groups and their respective NS control groups.
For alfuzosin animals, the mean change in USS was −0.3 ± 2.6 for NS infusion alone and 2.3 ± 1.8 for alfuzosin with EMDA (Table 4). The change in USS between the NS infusion group and the alfuzosin with EMDA group was statistically significant (p = 0.031) (Fig. 5).
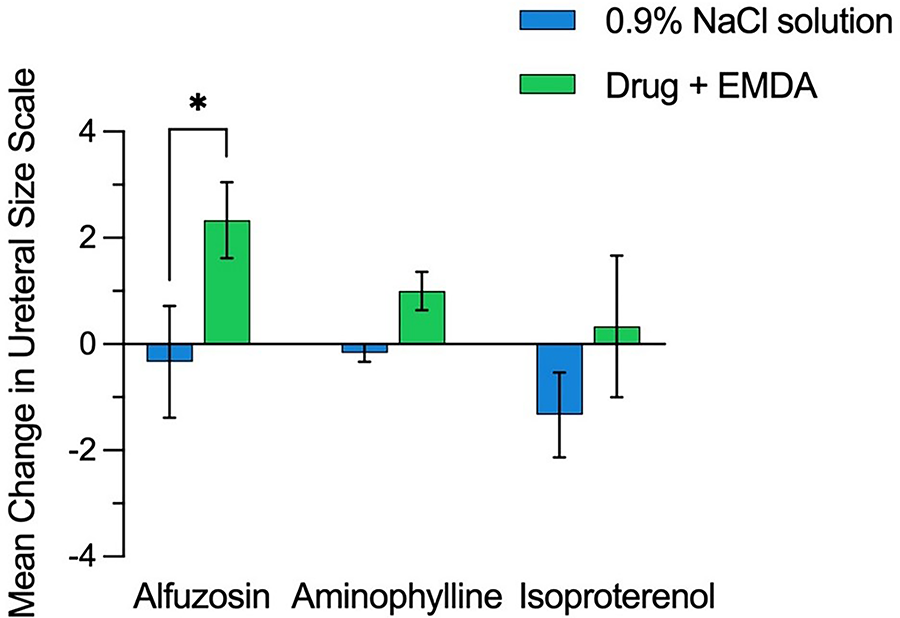
Mean change in ureteral size (post-treatment to pretreatment). Treatment groups include alfuzosin, aminophylline, and isoproterenol with EMDA compared with the contralateral ureter with 0.9% sodium chloride infusion only.
Mean Ureteral Size Scale and Change in Mean Ureteral Size Scale in Normal Saline Infusion Only Control Groups and Drug Administration with Electromotive Drug Administration Experimental Groups

For aminophylline animals, the mean change in USS was −0.2 ± 0.4 for NS infusion alone and 1.0 ± 0.9 for aminophylline with EMDA (Table 4). No significant difference was observed (p = 0.125) (Fig. 5).
For isoproterenol animals, the mean change in USS was −1.3 ± 2.0 for the NS infusion alone and 0.3 ± 3.3 for isoproterenol with EMDA (Table 4). No significant difference was observed (p = 0.344) (Fig. 5).
Ureteral injury assessment post-treatment: PULS grade evaluation
With adherence to a threshold of 3.5 N, no PULS 3 injuries were observed in any experimental or control ureter (Table 5).
Post-Procedure Ureteral Post-Ureteroscopic Lesion Scale Grade for All Control and Experimental Groups

PULS = Post-Ureteroscopic Lesion Scale.
Discussion
Intraoperative, atraumatic acute ureteral dilation may add to the safety, efficiency, and efficacy of ureteroscopic lithotripsy. To date, local delivery of SMRs to the ureter has yielded inconsistent results, likely due to the impermeable ureteral urothelium and limited SMR contact time caused by drainage and urine flow. Accordingly, we investigated whether EMDA could enhance SMR delivery to facilitate acute ureteral dilation. Alfuzosin, aminophylline, and isoproterenol were our SMRs of choice based on their small molecular weight and molecular charge potentials, which would be favorable for EMDA.
Only alfuzosin administered with EMDA at 10 mA for 20 minutes increased USS when compared with its control contralateral ureter and when compared with its pretreatment baseline (Fig. 4). Although statistically significant, the clinical relevance of this increase is slight, as a USS of 2.3 from pretreatment to post-treatment equals only a 0.8 Fr increase. Nonetheless, this level of dilation may enable ureteroscope passage in cases of failed primary access or facilitate the insertion of a slightly larger UAS higher in the ureter. Existing methods for ureteral dilation rely on either acute traumatic intervention, such as balloon dilation, or delayed passive dilation requiring pre-stenting for a week or more.28–30 Of note, in our study, limiting the applied force to 3.5 N prevented PULS 3 injuries that would have resulted in a false positive effect.
Drug-specific physicochemical and electrochemical properties most likely explain the differences in the observed results under EMDA conditions. Alfuzosin, a positively charged and moderately lipophilic molecule at physiological pH, demonstrated effective delivery, likely due to its redox stability, favorable electrophoretic mobility, and high receptor affinity.31,32 In contrast, isoproterenol, although highly potent, contains a catechol moiety that is readily oxidized at low potentials, making it susceptible to redox-mediated degradation.33–35 Aminophylline, whose active component is theophylline, is neutral charged at physiological pH, therefore exhibits minimal electrophoretic mobility. Furthermore, theophylline also undergoes irreversible degradation upon oxidation of its xanthine ring. 36 Additionally, dissociation of the aminophylline complex or oxidation of the ethylenediamine component may have reduced drug stability or solubility under EMDA conditions. 37 Of note, all compounds were delivered through a silver-containing catheter, which may have further promoted oxidation, particularly for redox-labile molecules. Collectively, these findings suggest that intrinsic drug properties, especially redox stability, are critical determinants of EMDA efficacy and, in future studies, need to be considered when selecting compounds for electromotive delivery.
More importantly, this investigation represents the first purposeful application of EMDA in the UUT. Previous EMDA use in Urology has been limited to bladder applications. 21 Administering SMRs in the ureter with EMDA establishes an initial framework for optimizing EMDA parameters and advancing techniques to deliver other medications intraureterally safely and effectively via electromotive forces. Future research will focus on optimizing delivery parameters, refining drug formulations, and exploring additional therapeutic agents (i.e., antibiotics, analgesics, and chemotherapeutic agents).
There are several limitations to this initial study. First, although alfuzosin administration demonstrated a statistically significant effect, we can only hypothesize that this was secondary to alfuzosin delivery deep into the urothelium. Ongoing efforts, including matrix-assisted laser desorption/ionization imaging mass spectrometry, aim to accurately assess drug presence and the depth of drug penetration into the porcine ureter. Second, the control group consisted solely of saline infusion without drug administration and without EMDA, rather than drug administration without EMDA. This control was chosen based on prior porcine studies showing that topical SMRs can cause relaxation in the contralateral ureter. 18 Additionally, the small sample size in each group may have limited the power to detect more subtle intra- and intergroup differences. To address this, our institution is currently conducting further studies to evaluate alfuzosin administration via the activated and inactivated EMDA catheter since this was the only molecule that, despite the small sample size, provided a positive effect.
Furthermore, we did not go beyond the short-term assessment of the treatment. We thus cannot comment on either its durability beyond a few minutes or any delayed adverse effects. Last, initial drug selection was based on molecular size, charge, solubility, and known receptor affinity; however, we did not fully account for additional electrochemical properties such as redox susceptibility, which we now recognize as another key determinant of drug performance under EMDA conditions. These insights are guiding ongoing compound selection for future studies.
Conclusion
In vivo, alfuzosin EMDA infusion in the porcine ureter may result in an acute increase in ureteral distensibility. In contrast, aminophylline EMDA infusion, isoproterenol EMDA infusion, and NS infusion alone in the control ureter resulted in no significant increase in ureteral distensibility.
Authors’ Contributions
B.M.G.: Conceptualization, methodology, formal analysis, writing—original draft, and writing—review and editing. Y.X.W.: Methodology, formal analysis, writing—original draft, and writing—review and editing. S.H.H.S.: Methodology and writing—review and editing. S.A.M.L., S.S., M.S.H., and V.P.: Investigation and writing—review and editing. E.M.-C., O.D., A.A., Z.E.T., and P.J.: Data curation and writing—review and editing. R.M.P.: Formal analysis and writing—review and editing. J.L. and R.V.C.: Conceptualization, resources, supervision, and writing—review and editing. All authors have read and approved the final article.
Footnotes
Author Disclosure Statement
J.L. serves as Editor-in-Chief of the Journal of Endourology. The other authors declare no conflicts of interest.
Funding Information
The project described was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through Grant UL1 TR001414. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. Provision of urethral dilator sets was supplied by Cook Medical. The company did not participate in the study’s design, conduct, data collection, analysis, interpretation, article preparation, review, or approval.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.