
Abstract
Introduction:
Surface lubricity is a desirable characteristic of ureteral access sheaths (UAS), allowing for atraumatic navigation of the urinary tract. This study aimed to characterize the surface lubricity of commonly available 14F UAS, as well as 14F ureteral and urethral dilators, using a tribometer and a novel ex vivo ureteral tissue holder.
Materials and Methods:
The surface lubricity of 12, 14F urological catheters (8 UAS, 1 urethral dilator, and 3 ureteral dilators) was tested in six ex vivo Yorkshire porcine ureteral segments. A tribometer, capable of measuring force in thousandths of a Newton (N), measured frictional force during insertion and retraction cycles under a 4.0 N normal force. The coefficient of friction (COF) was calculated. Individual and cumulative lubricity scores (ILS and CLS) were calculated based on COF percentiles, enabling a comparative evaluation of device performance. Surface roughness was assessed via white light interferometry.
Results:
The Cook Flexor® UAS consistently demonstrated the highest lubricity, as reflected in its CLS for both insertion and retraction phases, followed closely by the Wellead ClearPetra® UAS. Dilators, including the Cook AQ hydrophilic-coated ureteral and urethral dilators, exhibited higher COF values, correlating with greater surface roughness. COF values were significantly higher during retraction cycles than insertion cycles (p < 0.05). Variability in COF across devices underscored the influence of surface properties on lubricity.
Conclusions:
Among all the UAS/dilators tested, the Cook Flexor® AQ-coated UAS and Wellead ClearPetra UAS had the best lubricity. Catheter retraction resulted in higher COF than catheter advancement.
Introduction
Ureteroscopy (URS) is the gold standard for treating kidney stones <2 cm. Ureteral access sheaths (UAS) may improve stone clearance, reduce procedure costs, lower the risk of infection, provide for repeated safe passage of the ureteroscope, and reduce intrarenal pressure.1–3 However, concerns persist regarding UAS usage, especially regarding ureteral injury. Studies by Traxer and Thomas and Loftus et al. noted significant ureteral injury rates of 14% to 23% associated with passage of a 14F UAS.4,5 The consequences of high-grade injuries remain controversial. Stern et al. found that patients with high-grade ureteral lesions following UAS placement had a stricture rate comparable with UAS procedures with no visible injury, at 1.8%. 6 In contrast, in reviewing our database of over 700 URS procedures, we found that high-grade UAS-induced injuries (i.e., Post Ureteroscopy Lesion Scale [PULS] grade 3) were associated with ureteral strictures in 13% of patients. 7 Moreover, research by Tapiero et al. demonstrated that UAS deployment forces exceeding 8 Newtons (N) were associated with high-grade ureteral injury. 8 Together these findings underscore the critical need to find ways to optimize UAS deployment at a low insertion force and thereby improve patient safety.
Tribology is the science of studying friction between two surfaces that are in relative motion. It has only recently been applied to the field of biological surfaces and catheters. Specifically, Yang et al. evaluated the frictional properties of guidewires and hydrogel coatings using a reciprocating sliding test, measuring frictional resistance during insertion with wires, a silicone clamp, and lubricant. 9 Similarly, Røn et al. assessed the frictional forces of catheters inserted into a silicone-based urethral model via linear reciprocating motion by using a digital balance sensor. 10 A drawback to these studies is that silicone is not an accurate surrogate for human urothelial tissue. To overcome this shortcoming, Humphreys et al. created a synthetic urethral model using human urethral epithelial cells seeded within a synthetic polydimethylsiloxane (PDMS) matrix, thereby enabling more clinically relevant COF estimations. 11 Finally, Shi et al. further replicated urethral catheterization conditions by testing friction between the porcine urethra and polyvinyl chloride tubes coated with PDMS in order to compare various silicone-based lubricants. 12
Given the rise in URS and the usage of UAS, we sought to provide the first studies on the friction generated between ureteral tissue vs UAS and upper urinary tract dilators. Accordingly, we developed a novel ex vivo tribometry porcine ureteral model. Herein, we compare the friction between the porcine ureter and commonly available UAS as well as multiple ureteral and urethral dilators. In addition, we evaluated surface roughness using white light interferometry in order to further expand our understanding of how a UAS’s or urinary tract dilator’s surface characteristics might influence their lubricity when deployed in the porcine ureter.
Materials and Methods
Preparation of porcine ureters
Ureters were harvested from female juvenile Yorkshire pigs of similar size and weight (mean age: 92 days, mean weight: 43 kg), skeletonized, detubularized, sectioned into 25 × 20 mm segments, and stored at −20°C. The ureteral segments were thawed for 45 minutes prior to Figure 1A.
Sample selection and testing methodology
A total of 12 14F upper urinary tract devices were tested, consisting of eight unused UAS (Cook Flexor®, Boston Scientific Navigator™ HD, Dornier Magellan™, Coloplast ReTrace®, Bard Proxis™, RocaMed Bi-Flex EVO™, Wellead ClearPetra®, and Applied Forté®), three ureteral dilators (Cook AQ-hydrophilic coated ureteral dilator, polyethylene ureteral dilator, and polytetrafluoroethylene [PTFE] ureteral dilator), and one urethral dilator (Cook AQ-hydrophilic coated urethral dilator). Each device was assessed against six different porcine ureteral segments. 0.9% saline (NS) was applied to activate the hydrophilic coating of all sheaths and dilators prior to testing.
Ureteral tissue holder design and implementation
A custom-designed 3D-printed ureteral tissue holder was developed to secure porcine ureteral segments. The ureteral holder was engineered to minimize tensile stress on the tissue while using a curved contour that aligns with the natural lumen of the ureter to maintain a consistent saline film at the urothelial-UAS/dilator interface. The model ensured that the ureteral specimen would remain securely in place throughout the testing period. Both the distal and proximal ends of each ureteral segment were marked, simulating the antegrade and retrograde direction of the Figure 1B.
Testing parameters and procedure
The frictional interaction between the ureteral wall and UAS/dilator was quantified using a tribometer (MFT-5000, Rtec Instruments, San Jose, CA). An additional 2.0 mL of NS was applied to the ureteral mucosa prior to initiating each test to maintain lubrication and prevent tissue desiccation. A saline film was visually confirmed before each trial.
A tension load cell was used to employ a constant normal force of 4.0 N to the UAS/dilator holder at the point of contact with the Figure 1C. The 4.0 N value was previously identified in our in vivo porcine ureteral work as the non-injurious threshold for UAS passage. 13 Each ureter–UAS/dilator interaction was conducted with motion alternating between insertion and retraction.
Based on a prior UAS study showing that the time necessary to insert a UAS was 23 to 29 seconds, we divided our testing into 3 × 10-second intervals. 5 During each cycle, the UAS/dilator was moved along the ureteral surface in one direction for the full length of the ureteral segment. In cycle 1, the UAS/dilator was inserted from the distal to the proximal end of the ureteral segment, simulating retrograde access. In cycle 2, the UAS/dilator was moved in the opposite direction, simulating device retraction. Figure 1D cycle 3 represented a retrograde reinsertion along the same path as cycle 1.
Lubricity Assessment—Coefficient of friction (COF) calculation
The COF serves as a valuable metric that quantifies both the lubricity of the UAS/dilator as well as the frictional resistance between the UAS/dilator and the ureteral segment, directly impacting ureteral catheter insertion and retraction. The COF was calculated as the ratio between the measured frictional force and the applied normal force. As the COF is a relative lubricity metric, all devices under investigation were tested against the same ureter. To mitigate potential cumulative tissue damage, the UAS/dilator testing order was randomized.
The lubricity was assessed qualitatively by ranking the UAS using the Individual Lubricity Score (ILS) for each ureter and the Cumulative Lubricity Score (CLS) across all ureters. These qualitative findings may, however, overemphasize small differences between statistically similar devices. As such, the UAS lubricity ranking was then validated quantitatively using analysis of variance (ANOVA), followed by Tukey’s Honest Significant difference (HSD) post hoc test to identify UAS/dilator pairs with significantly different COF.
Qualitative lubricity assessment—ILS
Once all UAS/dilators were tested against the same ureter, their lubricity was ranked on a point scale from 1 to 7 based on their percentile lubricity ranking. If the catheter was the most lubricious out of the 12 tested medical devices (i.e., 99th percentile), an ILS of 7 was allotted. However, if the catheter was on the opposite end of the lubricity spectrum (i.e., 1st percentile), an ILS of 1 was given. For catheters that had lubricities between the 2nd and 98th percentile, an ILS from 2 to 6 was assigned (Table 1). The ILS was calculated once for the insertion phase (average of cycles 1 and 3) and once again for the retraction phase (cycle 2), corresponding to the individual insertion lubricity score and the individual retraction lubricity score (IRLS), respectively.
Lubricity Percentile to Individual Lubricity Points Correlation
Qualitative lubricity assessment—CLS
As the same UAS/dilator could display different friction patterns when tested against different ureters due to interindividual biological variation as well as allotted catheter randomized testing order, we calculated the CLS for each UAS/dilator as the sum of the ILS across the six different ureters. Both a cumulative insertion lubricity score (CILS) and a cumulative retraction lubricity score (CRLS) were determined. This resulted in a maximum possible CLS of 42 points and a minimum of six points for each catheter.
These were graphically presented as hexagonal radar plots with the ILS corresponding to the individual points of the geometrical shape and the area of the radar plot representing the CLS (Fig. 2). Catheters with higher CLS and larger areas were more lubricious, while those with lower CLS and smaller areas had lower lubricity.
Radar plot interpretation key with individual lubricity score (ILS) and cumulative lubricity score (CLS) significance.
Quantitative lubricity assessment—statistical analysis
The COF values of the 12 different UAS/dilators were analyzed using a one-way ANOVA. Following a significant ANOVA result, Tukey’s HSD post hoc test was performed to identify which specific UAS/dilator pairs differed significantly in COF. In addition, COF values between insertion and retraction across all UAS/dilator tests were compared using multiple unpaired sample t-tests with Welch corrections accounting for unequal variances. Statistical analyses were performed using SPSS Statistics version 29.0.0.0 (IBM Corp, Armonk, NY).
Surface analysis techniques
White light interferometry is a noncontact optical technique that permits capture of interference patterns created by light reflecting off surface irregularities. 14 These patterns are processed to generate a detailed 3D surface topography map.
Surface roughness of the sheaths and dilators was assessed using a white light interferometer camera on the Rtec Tribometer MFT-5000. This analysis was of particular interest for the UAS/dilators with identical AQ hydrophilic coatings (14F Cook Flexor® UAS, Cook Ureteral Dilator, and Cook Urethral Dilator). The average roughness (Ra) was calculated to quantify deviations from the mean surface level, providing insight into the texture and detection of any UAS/dilator surface irregularities. With this approach, surface roughness could be correlated with observed frictional characteristics.
Results
Out of a total of 216 tests, consisting of 12 different UAS, urethral dilators, and ureteral dilators, assessed during three cycles (insertion–retraction–reinsertion) across six different ureters, 97% of tests displayed a coefficient of variability (calculated as the ratio between standard deviation and sample mean) of less than 20% when comparing the same access sheath/dilator across different ureters (Supplementary Table A1).
In no case was urothelial damage noted throughout the testing period in any of the ureteral segments. Among the 12 UAS, ureteral dilators, and urethral dilators tested, the Cook Flexor® UAS consistently demonstrated the highest lubricity, with both CILS and CRLS outperforming other devices (Fig. 3). This performance was reflected in its overall CLS, indicating that the Cook Flexor® encountered the least friction during both insertion and retraction with the ureteral mucosa. The Wellead ClearPetra® demonstrated a CLS comparable with that of the Cook Flexor®. In contrast, the Cook AQ-, polyethylene-coated, and PTFE-coated Ureteral Dilators and the Cook Urethral Dilator demonstrated lower lubricity, as indicated by their higher COF values and lower CLS.
Relative lubricity of ureteral access sheaths (UAS), ureteral dilators, and urethral dilators across six porcine ureters.
A one-way ANOVA was performed to compare mean COF values among the 12 UAS/dilator devices. The analysis revealed statistically significant differences among the devices (Table 2; F = 79.37, p < 0.0001). Post hoc Tukey comparisons indicated that the Cook Flexor® showed significantly lower COF values compared with the Boston Scientific (p < 0.0001), Coloplast ReTrace® (p < 0.0001), Bard Proxis™ (p < 0.0001), Applied Forté® (p < 0.0001), Dornier Magellan™ (p = 0.0388), and RocaMed Bi-Flex EVO™ UAS (p = 0.0337). No significant difference in COF values was observed between the Cook Flexor® and Wellead ClearPetra®.
Pairwise Comparisons of the Coefficient of Friction (COF) Between Ureteral Access Sheaths (UAS), Ureteral Dilators, and Urethral Dilators During Insertion Cycles

Each cell represents the mean difference in COF between the device in the row and the device in the column (row–column). Bolded values indicate statistically significant differences (p < 0.05)
PTFE = polytetrafluoroethylene.
The results of the quantitative lubricity analysis were largely concordant with the qualitative lubricity rankings. Devices that demonstrated lower COF values in ANOVA testing, such as the Cook Flexor® and Wellead ClearPetra® UAS, also consistently received the highest ILS and CLS. Conversely, devices with significantly higher COF values, including the ureteral and urethral dilators, correspondingly received lower CLS values (Fig. 4). This alignment between statistical and scoring-based assessments reinforces the robustness of the lubricity ranking system and supports the validity of using CLS as a surrogate for comparative performance.

Quantitative lubricity ranking based on UAS/urethral dilator/ureteral dilator COF analysis of variance. Circles represent catheter groupings with statistically equivalent lubricity, while overlapping circles indicate UAS devices that belong to multiple statistically distinct lubricity groups. COF = coefficient of friction; UAS = ureteral access sheaths.
Interestingly, despite having the same AQ hydrophilic coating, the Cook Flexor® UAS, the Cook AQ Hydrophilic-coated Ureteral Dilator, and the Cook Urethral Dilator demonstrated different COF values. Of note in this regard, upon white light interferometry analysis, the Cook Flexor® demonstrated the smoothest surface, correlating with lower COF values and superior lubricity, while the Cook Ureteral Dilator and the Cook Urethral Dilator exhibited rougher surfaces and had higher COF values (Fig. 5). COF values during the retraction phase were significantly higher than those observed during insertion across all UAS/dilators (Fig. 6).

Head-to-head surface roughness comparison by white light interferometry for three urological catheters all with AQ Hydrophilic coating. Despite having the same coating, the surface roughness had a significant impact on the lubricity of the catheters, with rougher catheters displaying higher friction forces at the catheter-urothelial interface.
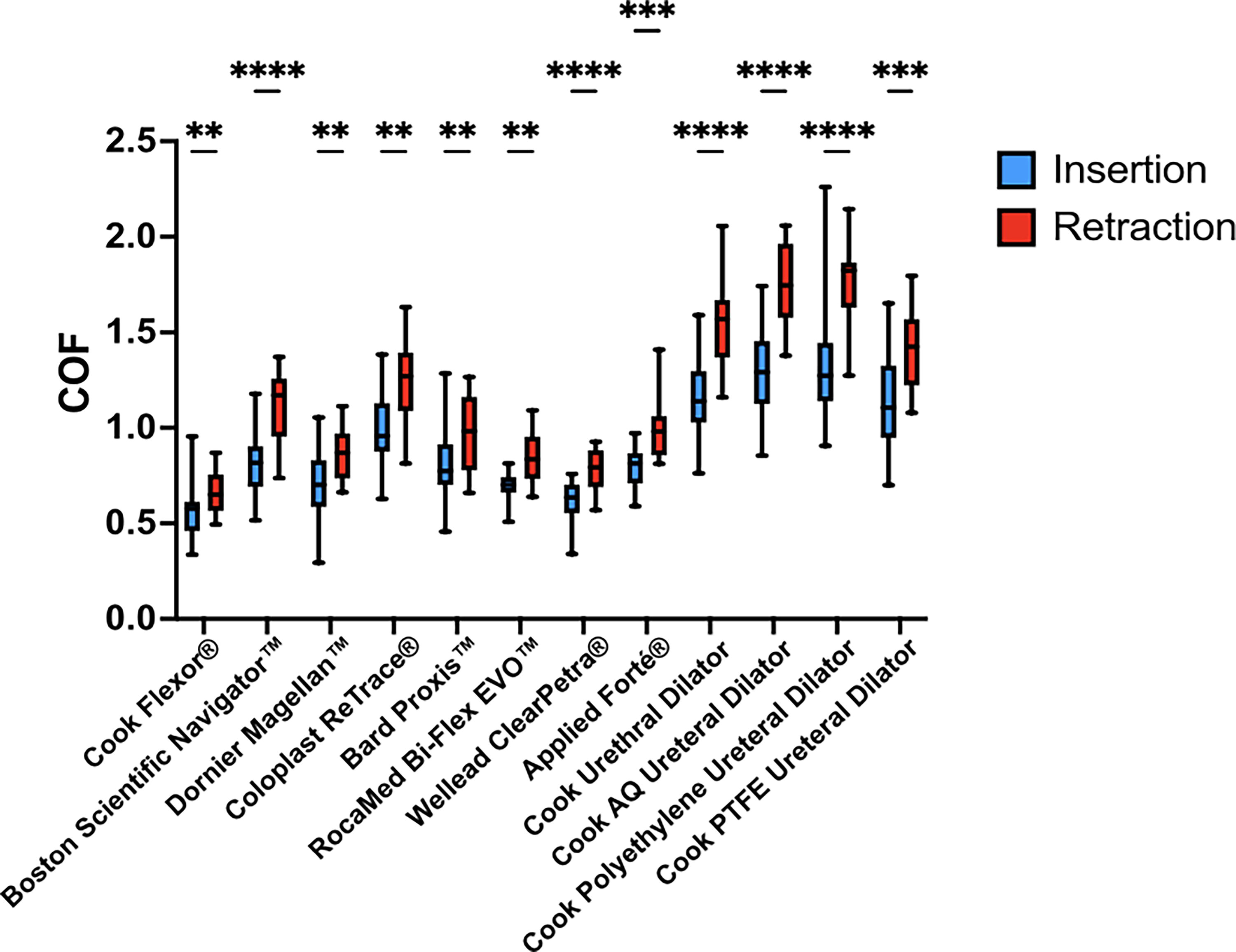
Comparison of coefficient of friction values between insertion vs retraction across 14F UAS, ureteral dilators, and urethral dilator. Multiple unpaired sample t-tests with Welch corrections were employed for comparative analysis to account for unequal variances between groups. *, **, ***, and **** correspond to p values <0.05, 0.01, 0.001, and 0.0001, respectively. UAS = ureteral access sheaths.
Discussion
The UAS was first introduced by Takayasu in 1974 as a conduit for atraumatic introduction of a ureteroscope into the ureter and renal collecting system for stone removal. 15 This first generation UAS was not universally adopted due to high complication rates. 16 In 1999, Clayman, in collaboration with Applied Medical Resources (Rancho Santa Margarita, CA, USA), developed a kink-resistant UAS that significantly reduced complication rates, resulting in a more efficient device.1,17 When properly deployed, the UAS enhances surgical efficiency, efficacy, and safety by lowering intrarenal pressure, improving visualization, increasing stone-free rates, and reducing operative times.18,19
Despite these advantages, the adoption of UAS into clinical practice remains inconsistent. A survey of 216 endourologists revealed that UAS was used in only 46% of ureteral stone cases and 76% of renal stone cases. 20 Although UAS design has evolved significantly, the risk of ureteral injury and subsequent stricture formation persists.6,21–26
Previous studies conducted by Loftus et al. and Elsaga et al. comparing the Cook Flexor® and the Boston Scientific Navigator™ HD noted no significant difference in ureteral injury rates.5,26 However, in neither study was the force of UAS placement measured, and both studies were marred by relatively small sample sizes.
In contradistinction to the two foregoing studies, Patel and Monga investigated three types of UAS, focusing on the safety, positioning, lubricity, and radio-opacity. However, the study found minimal differences in frictional forces, leaving the impact of lubricity unclear. 27 Indeed, in this ex vivo benchtop study, bologna served as the biological model for the ureter; no data were presented to establish its status as a reasonable substitute for the ureter. To avoid this limitation, we selected porcine ureteral tissue, which more closely resembles human ureteral mucosa.28,29 Using a reciprocating tribometer calibrated to record frictional forces in thousandths of a Newton, we were able to detect variations in lubricity, allowing for a comparative analysis of commonly used ureteral catheter devices.
The fragility of the human ureter has only recently been defined, with studies concerning ureteral distensibility showing that UAS insertion forces as low as 8 N (2 pounds of force) are sufficient to cause a transmural ureteral wall tear.8,13 This stimulated our interest in catheter lubricity as we sought to identify a UAS that would possibly glide up the ureter with the least amount of deployment force. We hypothesize that a more lubricious UAS or dilator would pass easier and with less trauma up the ureter; this hypothesis is the subject of a planned porcine study. Although no injuries were assessed in this ex vivo study, the rationale stems from clinical reports of ureteral injury. For instance, Traxer and Thomas reported that 13% of patients undergoing URS with a 14F UAS sustained ureteral injuries graded ≥24. Loftus et al. further corroborated this risk, documenting injury rates of 23% to 26% (TISG ≥2) using 14F sheaths. 5 Similarly, Schoenthaler et al. observed a 24% incidence of PULS ≥2 injuries. 30 These findings underscore that clinically substantial mucosal disruption is not uncommon even with sheaths traditionally considered within safe diameter ranges. In contrast, at our institution, 16F UAS are deployed in upwards of 50% of our patients without ureteral injury, provided that the 16F sheath is deployed using a real-time force sensor capable of detecting insertion force variations in hundredths of a Newton such that the insertion force does not exceed 6 N. This is crucial, as the reported cumulative stricture rate following URS, though relatively low at 0.3% to 3%, increases markedly with the severity of the injury—rising from 1.1% for superficial urothelial splits to as high as 13% in cases of full-thickness transmural ureteral injuries in our experience. 7
Our results revealed variability in COF values across different ureters and different UAS/dilators, highlighting the heterogeneity of urothelial and UAS/dilator surface properties. With regard to the ureteral segments, randomizing testing order minimized any impact on mucosal wear and tear, reducing test order dependence. To the best of our ability, all possible confounders were tightly standardized (testing order, contact force, time of contact, tissue hydration) for each test. While all parameters were controlled, minor inter-ureteral biological variability may still exist. Among the six ureters tested, the Cook Flexor® consistently had the lowest COF values, indicating superior lubricity and smoother interactions with ureteral mucosa. In contrast, both the Cook Ureteral and Urethral Dilators showed higher COF values.
Despite sharing the same AQ Hydrophilic coating, the Cook Flexor® UAS, Cook AQ Hydrophilic-coated Ureteral Dilator, and Cook Urethral Dilator exhibited markedly different COF values, suggesting that factors beyond advertised coating may significantly influence friction. To better understand these differences in lubricity, we performed white light interferometry to assess surface roughness. The Cook Ureteral and Urethral Dilators exhibited greater surface roughness than the Cook Flexor® UAS, likely explaining the higher friction and reduced lubricity with both dilators. This analysis confirmed that, even with identical coatings, surface properties are also important, as they clearly impact catheter performance; rougher surfaces reduce lubricity. In addition to surface roughness, other device-level properties such as cross-sectional geometry, material composition, temperature, speed of passage, and compliance may impact COF values and merit further exploration in future studies.
Overall, COF was higher during retraction, consistent with clinical experience, where retracting the UAS/dilator at times feels more resistant than inserting it. The higher COF observed during retraction may be attributable to partial degradation or redistribution of hydrophilic coatings during initial passage. In addition, anisotropic features of the catheter surface or the ureteral mucosa itself may contribute to increased resistance in the reverse direction. Future studies are needed to elucidate the underlying mechanisms and their clinical relevance.
Our study is not without limitations. While detubularization provided a controlled and uniform mucosal surface for testing, we acknowledge that this setup does not fully replicate in vivo conditions. Also, the frictional resistance under perpendicular force may not directly replicate axial insertion force in vivo. Regardless, the described experimental setup allows for controlled comparison of lubricity across devices under a standardized load. Furthermore, it is unclear whether hydrophilic coatings are applied uniformly by the manufacturer across the entire length of each UAS/dilator, as we focused only on the end of the UAS or dilator that would first encounter the ureter. Future in vivo porcine laboratory studies are needed in order to assess the relevance of our findings and their potential application in clinical practice.
Conclusions
A reciprocating tribometer enabled quantitative investigations into the mechanical interactions among 14F UAS, 14F ureteral dilators, a 14F urethral dilator, and the ureter. Among all the UAS/dilators tested, the Cook Flexor® AQ-coated UAS and Wellead ClearPetra UAS had the best lubricity.
Authors’ Contributions
B.C.: Methodology, data acquisition, data curation, and formal analysis. A.D.C.: Conceptualization, methodology, data acquisition, data curation, and formal analysis. K.M.-R.: Methodology, data acquisition, data curation, and formal analysis. T.N.V.: Data acquisition and data curation. Z.E.T.: Methodology, data curation, and formal analysis. J.A.: Methodology, data acquisition, and formal analysis. A.R.H.G.: Methodology, data acquisition, and formal analysis. A.A.: Methodology and supervision. B.M.G.: Methodology, data curation, and supervision, P.J.: Methodology, data curation, and supervision. R.M.P.: Methodology, data curation, and supervision. J.L.: Conceptualization, methodology, and supervision. A.M.: Conceptualization, methodology, supervision, data curation, and formal analysis. R.V.C.: Conceptualization, methodology, supervision, data curation, and formal analysis.
Footnotes
Acknowledgment
Portions of this current article were previously published (https://www.auajournals.org/doi/10.1097/01.JU.0001109956.38240.97.20), and some results were previously presented as a poster at American Urological Association Annual meeting in Las Vegas, NV, April 26–29, 2025. ![]() .
.
Author Disclosure Statement
J.L. is coeditor-in-chief of the journal, and R.V.C. is founding coeditor-in-chief. All other authors have no conflicts of interest to declare.
Funding Information
This research did not receive any specific grant from funding agencies. Funded through the Curiosity and Innovation laboratory funds.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.