
Abstract
Due to advances in medical treatments, students with terminal illnesses are more likely to attend public schools, increasing the possibility that they may die on school property. However, educational health plans often fail to consider end-of-life care decisions. In the absence of federal or state statutes, school boards are left to navigate the issue of minors with Do Not Resuscitate Orders while at school. We examine state statutes and school board polices for minors with Do Not Resuscitate Orders attending or wishing to attend school. Themes from school district policies are discussed, and recommendations for federal, state, and local policymakers are made.
Medical advances are extending the lives of children with terminal illnesses, making it increasingly feasible for medically fragile children seeking “normal” educational experiences to attend public schools (Westbrook et al., 2020). 1 The education and participation of children with terminal illnesses in U.S. public schools is covered by Section 504 of the Rehabilitation Act (1973), which prohibits discrimination against individuals with disabilities. In some instances, the parents or guardians of children with terminal illnesses may wish for their children to experience a natural death without medical interventions that have a low probability of resuscitation and may cause physiological pain and unnecessary suffering (Adelman, 2011). 2 In such cases, the physician of a child with a terminal illness, in consultation with parents or guardians, will write a Do Not Resuscitate (DNR) Order, which directs medical responders not to provide unwanted medical interventions. 3
DNR Orders for minors attending public schools is an ideologically and emotionally charged topic that has been explored in research over the last 30 years (Kuehl et al., 1992). Efforts to develop and implement public policy on matters in which people and technological advances meet often defy the power of the classical scientific paradigm because problems exist in a social context (Rittel & Webber, 1973). Our topic raises questions about medical advances in the context of the right to die with autonomy and dignity, the well-being of classmates and teachers who may witness a death or attempted resuscitation, and the liability of local education agencies (LEAs) 4 and school personnel in whose care the child is entrusted. Because children with terminal illnesses may die on school properties, this possibility should be considered by state and local policymakers.
Some state legislatures have enacted statutes permitting or prohibiting minors from having DNR Orders. Similarly, some LEAs have adopted policies addressing minor students and DNR Orders, while many have not. If a LEA refuses to honor a DNR Order, school personnel are placed in the difficult situation of having to choose to follow LEA policy to administer cardio-pulmonary resuscitation (CPR) or risk the liability of knowingly administering CPR to a person with a DNR, which could be considered assault (Teno, 2008). School nurses are especially placed in a legal dilemma if LEA policy forces them refuse to follow a medical order (Begley et al., 2018). This issue is of critical importance to students with terminal illnesses and their educators, especially when viewed through an equity lens. For example, the findings reported in this study suggest that some LEA positions related to minors with DNR Orders wishing to attend public schools are forcing families to pursue court orders to have their wishes honored. Implicit in this finding is that only families with the financial means to do so would be able to secure the court order, which represents an equity barrier.
This study builds on our previous work on DNR Orders in public schools (Westbrook et al., 2020) which addressed a specific case study of a terminally ill high school student who possessed a DNR and the legal conflict his mother faced with the LEA regarding him attending school. We believe this is an important line of inquiry because it considers the intersection law, policy, medical ethics, and child welfare. This study focuses on two key factors that determine the treatment of minors with DNR Orders in public schools, state statutes and LEA policies. The guiding research questions for this study were:
How do state statutes address the issue of minors with DNR Orders?
How many LEAs have policies addressing minors with DNR Orders?
Do state statutes and LEA policies align?
What themes appear in LEA policies?
Answering our research questions will be particularly helpful for federal, state, and LEA policymakers and for future research on DNR Orders for minors in educational settings.
Do Not Resuscitate Orders
DNR Orders are medical orders written to address withholding CPR in the event that an individual’s heart stops or a person stops breathing, referred to as cardiac arrest and respiratory arrest (Lee, 2012). CPR is an attempt to restore the functions of the heart and lungs through the use of chest compressions or electric shocks to restart the heart and mouth-to-mouth or artificial ventilation (Jin et al., 2017; Lee, 2012). DNR Orders are controversial for terminally ill patients in medical settings, and health providers experience ethical dilemmas in deciding how to respond to the natural death of patients with terminal illnesses (Burns & Truog, 2016).
Since the widespread introduction of CPR in the 1960s as a treatment to a cardiac event that would otherwise result in death (Kouwenhoven et al., 1960), CPR has become a common response to a cardiac arrest even if when it is an often-futile effort to extend life (Blackhall, 1987). However, medical professionals have long disagreed about the ethics of performing CPR on patients with terminal illnesses (Tomlinson & Brody, 1988). Recognizing that performing CPR may actually cause physiological harm and unnecessary suffering to the terminally ill, health providers began implementing DNR Orders for patients whose illnesses are expected to result in a natural death (American Medical Association, 1974).
DNR Orders were formalized in the 1980s as a result of the work of the President’s Committee for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research (1983), which standardized recommendations for medical practitioners and resulted in state statues that provided both a means for patients to have autonomy over their end-of-life care and to provide legal liability protection to medical practitioners. Today, physicians routinely ask patients about their end-of-life care wishes and create documentation providing both patient autonomy and legal liability protection for health providers (Abba et al., 2019
The public has come to expect CPR to be administered in the event of a cardiac arrest in the absence of a clearly articulated DNR Order (Blackhall, 1987). In fact, all 50 states have “Good Samaritan” Laws that protect those attempting to render aide from liability claims (West & Varacallo, 2020). However, “Good Samaritan” Laws do not protect individuals who knowingly defy a DNR Order and perform CPR—which could be considered assault (Teno, 2008).
While competent adults may create advanced medical directives to address their wishes regarding CPR prior to having a medical condition or accident that leaves them incapacitated to speak for themselves, minors lack legal capacity to do so. Additionally, parents cannot simply create advanced directives for their children. A child who is terminally ill requires a physician’s order for a DNR. Optimally, the parents of the child should be fully informed and in agreement with the medical order. Parents cannot simply write a DNR Order for a child. They must request that their child’s physician write a DNR Order (Abuhammad et al., 2020).
Physicians determine the appropriateness of CPR and indicate that it is contraindicated in a child’s medical record by writing a DNR Order. CPR is not always in a terminally ill patient’s best interests and may be withheld when the benefits would not exceed the risk. A DNR Order provides for a natural death as a result of a terminal illness. A DNR Order does not prohibit providing comfort or palliative care such as suction for trouble swallowing or interventions during seizures or unconsciousness (Boston Children’s Hospital Ethics Advisory Committee, 2012).
The physicians of children with terminal illnesses have clear ethical standards on the appropriateness of CPR as a therapy for a child experiencing cardiopulmonary arrest (Boston Children’s Hospital Ethics Advisory Committee, 2012). CPR is only medically appropriate if the expected benefits exceed the risks. Children with terminal illnesses for whom CPR is deemed physiologically futile should not receive CPR and a DNR Order should be placed in their medical records (Boston Children’s Hospital Ethics Advisory Committee, 2012). In addition, CPR is not designed for use in patients for whom CPR in not therapeutic or cannot reverse the on-going dying process or will not provide benefits that outweigh the harms. In this case, administering CPR contravenes medical ethics and the principle of “do no harm,” and following the medical protocols which may involve a team of physicians and medical ethicists, a DNR Order is issued by the child’s physician and placed in the child’s medical record.
The Policy Issue
When children with terminal illnesses wish to attend public schools in an attempt to have a sense of “normalcy” in their schooling, school personnel are placed in the difficult position of acting according to laws and policies that may conflict with a physician’s medical order, disregard the wishes of the parents or guardians, and subject a dying child to actual pain and suffering. As of 2021, the federal government had not enacted statutes or established guidelines explicitly addressing minors with DNRs. As a result of this federal abdication, some state legislatures have enacted statutes on the issue.
The National Portable Medical Orders Organization, commonly referred to as POLST (2020), divides state statutes addressing DNRs for minors into one of three categories: (1) Authorizing minors to possess DNRs, (2) Not explicitly prohibiting minors from possessing DNRs, and (3) Prohibiting minors from accessing DNRs. In this sense, state policies embrace “courses of action (and inaction) that affect institutions and individuals in a health system” (Buse et al., 2005, p. 6). Because states often delegate the development of school policies and procedures to LEAs, the issue of DNR Orders for minors attending or wishing to attend school becomes a LEA policy issue.
When the parents of a minor enrolled in a public school present the LEA with a DNR Order, the LEA has three possible responses: (1) To honor the DNR Order as a medical directive written by physician and incorporate the DNR Order into the child’s Individual Health Plan (IHP) or 504 Plan, (2) To challenge the DNR Order by having a medical review by other physicians at the LEA’s expense (similar to challenging physician’s recommendations for special education services, a LEA may pay for its own medical review), or (3) To refuse to honor the DNR Order. In this study, we only consider the options of honoring or refusing to honor a DNR Order. A consequence of relying on individual LEAs to enact policy is the lack of uniformity related to minors with DNR Orders. The inconsistencies between LEA policies result in confusing messages to students with terminal illnesses, their families, and the educators who care for them. For children with terminal illnesses attending or wishing to attend public schools, this creates a difficult system to navigate.
Historically, LEA policies and procedures have resulted in children with terminal illnesses being placed on homebound services to be educated in their homes 5 —leaving the decisions for medical care up to the parents or guardians. Many children with terminal illnesses often become unable to engage in regular school activities due to their illnesses and related treatments. Children with terminal illnesses do not experience a sudden death, but a prolong decline that may result in respiratory depression that would prohibit their mobility and therefore their participation in schooling (Boston Children’s Hospital Ethics Advisory Committee, 2012; Rice & Gourley, 2003). Some students with terminal illnesses may continue to have the stamina to participate in schooling either in a full-time capacity or on a modified school day based on their physicians’ recommendations and in conjunction with an IHP or a 504 Plan. These are the children at risk of experiencing a sudden death while attending school.
Methodology
The discussion around the methodology is divided into five sections. In the first section, we present the conceptual framework for this study. We next explore the research design. Next, the theoretical framework for our analysis is explained. Then we identify the data sources used in this study and how they were collected. Finally, we describe the data analysis procedures.
Conceptual Framework
The two major elements considered in this study were state statutes addressing minors possessing DNR Orders and LEA policies on DNR Orders for students attending school. We developed the conceptual framework for this study as presented in Figure 1.
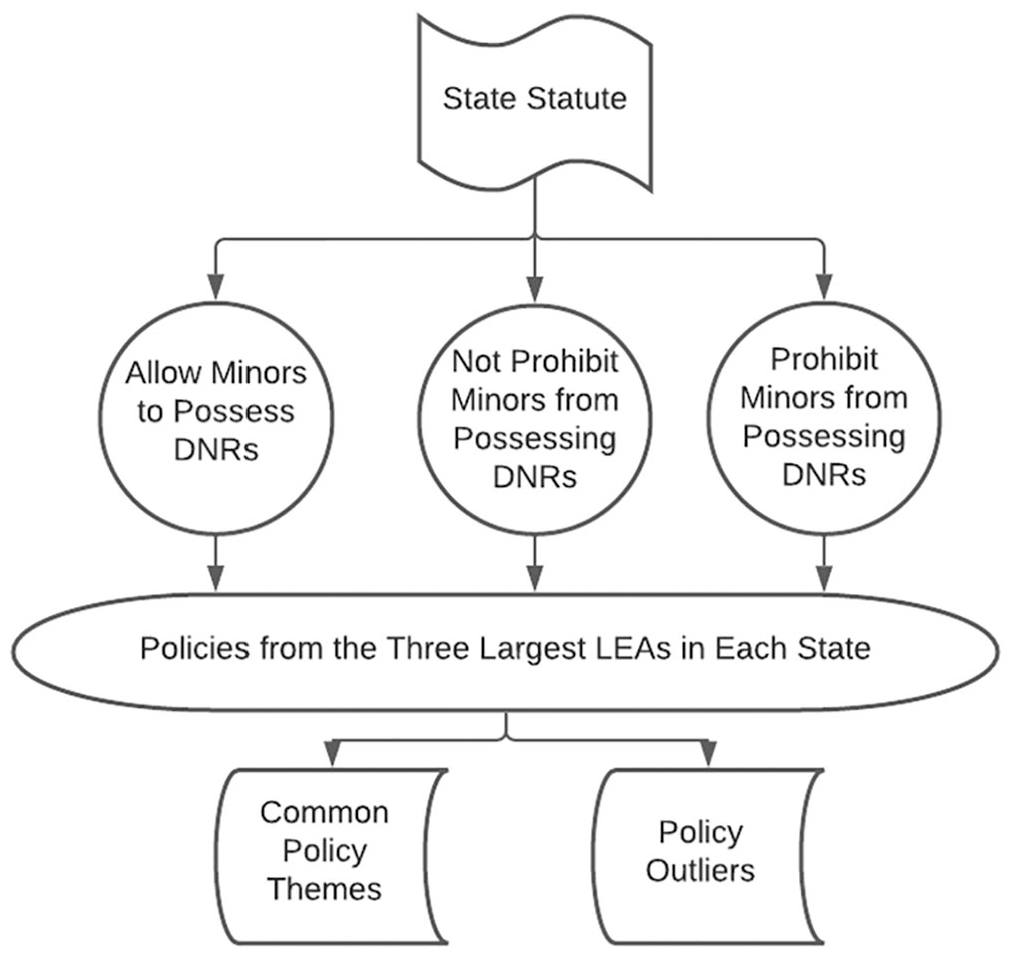
Treatment of minors with DNR Orders attending public school.
The conceptual framework for this study begins with an examination of statutes from each state on the topic of minors with DNR Orders. Specifically, we sought to determine if state statutes allow minors to possess DNR Orders. State statutes were divided into three categories, as described above. We then examined LEA policies addressing minors with DNR Orders attending or wishing to attend school in the three largest LEAs in each state. The policy examination included open coding of policy language, which resulted in the identification of common themes within the different types of LEA policies and outlier statements in policy language.
Pragmatic Research Design
This study used pragmatic philosophical and methodological approaches to explore the topic of LEA policies addressing minors with DNR Orders using several types of data and approaches to data analysis. Pragmatic approaches are ideal when researchers are focused on understanding socially situated data in an ever-changing context and are not attempting to resolve philosophical matters (Creswell & Plano Clark, 2007; Morgan, 2007). Pragmatic researchers generally select approaches that are most appropriate to address their guiding questions (Kaushik & Walsh, 2019). Our topic was socially constructed policies that address practical problems (Kaushik & Walsh, 2019; Maxcy, 2003).
This approach to research design focused on understanding existing policies by analyzing the text of the policies identified. This study and data collection were approached from both an iterative and sequential mindset as more was learned about the topic and the types of data available to answer the research questions (Irwin, 2003, p. 38). Throughout the data collection and analysis process, we moved between inductive and deductive reasoning in attempts to understand the DNR position based on state statutes and LEA policies (Kaushik & Walsh, 2019; Morgan, 2007). We discussed and explored numerous plausible explanations and patterns in an effort to reach understanding that addressed as many of the findings as possible.
Theoretical Framework
A top-down and bottom-up theoretical framework (Sabatier, 1999) was used to better understand the data within our conceptual framework (see Figure 1). We selected this theoretical framework because we examined this topic hierarchically and sought to understand policies and procedures that originated from the state, or the top, and LEAs, or the bottom. The top-down and bottom-up theoretical framework captures the role of both the state and the LEAs in the creation and oversight of existing statutes and policies related to minors with DNR Orders attending public schools.
Data Collection
The starting point for data collection was POLST’s State Laws and Regulations spreadsheet and map (POLST, n.d.), which identified states by the following DNR Orders for minors categories: (1) permits, (2) does not explicitly prohibit, and (3) prohibits. A review of each state’s DNR statute or guidelines did not produce any useful information because actual DNR Order policies are addressed at the LEA level.
We next discussed how to sample policies that might provide us with the best data for understanding how LEAs address the issue of minors with DNR Orders. The decision was made to sample the policies in the three largest LEAs in each state because, statistically, these LEAs are more likely to have encountered terminally ill students with DNRs and to have the requisite resources to enact policies addressing this issue (Soifer, 2000). Therefore, the sample was purposeful.
The next step was to locate DNR Order policies from the three largest LEAs in each state. We were interested in the language LEAs used to justify their policies supporting or prohibiting minors with DNR Orders. This was accomplished primarily by searching each LEA’s online policy manual for key words such as do not resuscitate, DNR, CPR, resuscitate, and medically fragile. Data were collected between fall 2020 and spring 2021.
We next created a spreadsheet of the LEAs policies, organized by their state’s position concerning minors with DNR Orders (permits, does not prohibit, or prohibits). In several instances, LEA policies were identical. For example, in New York State, the three largest LEAs had the same policies. In other instances, LEAs in different states used nearly identical language in their policies leading us to believe that some LEAs are either using policy templates or are copying existing policies. Applying the search criteria, 36 LEAs were identified with DNR policies and 112 LEAs without DNR policies.
Data Analysis
We then reviewed each LEA policy by focusing on identifying the specific elements of the policies and their intentions. This process was both inductive and deductive as preliminary generalizations were developed from the policies. Policies were separated into three categories based on whether the LEA was in a state that permitted minors to possess DNRs, did not explicitly prohibit minors from possessing DNRs, or prohibited minors from possessing DNRs. We also sought to determine why school districts adopted the current policy, but we were unable to definitively determine the impetus for each LEA position. While causal or correlational relationships may exist, we were unable to identify it.
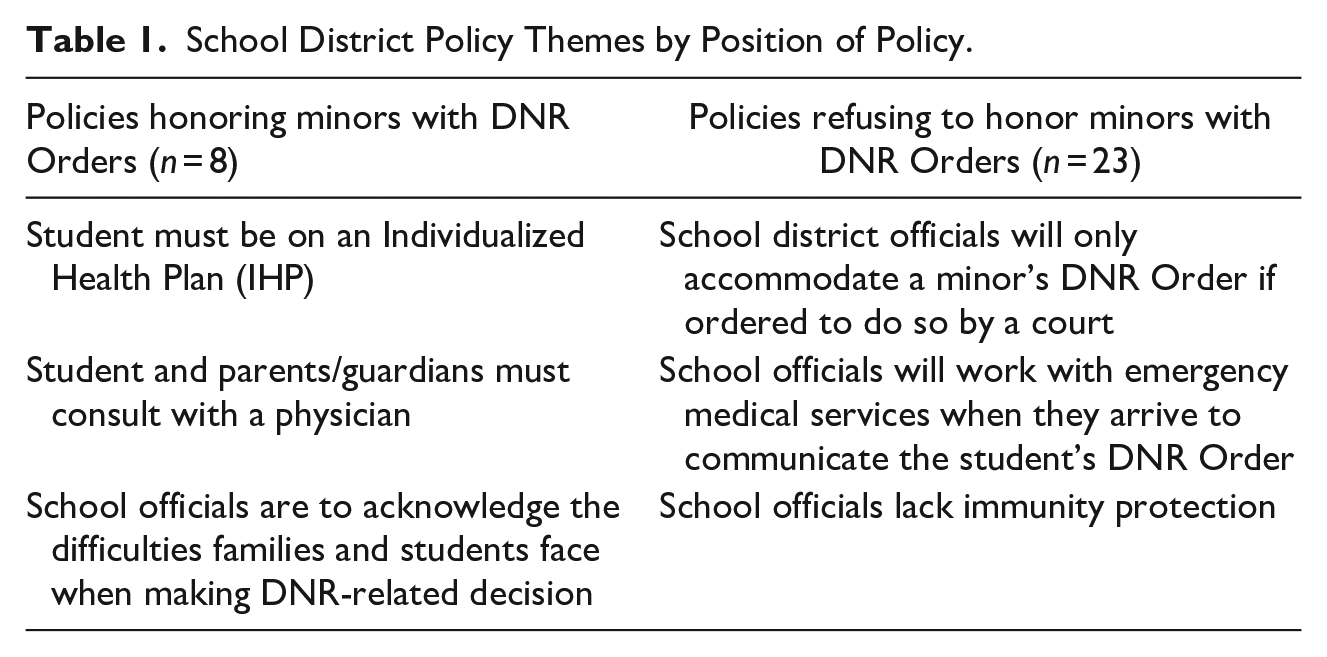
LEA policies were then open coded. We clustered passages around the following codes: conditions for honoring a DNR, justifications for having a DNR, key actors, and procedures for acting upon a DNR. This process was challenging due to the range of the language used in the policies and required a discussion of each policy for its actual meaning. To ensure greater accuracy, we collaboratively reviewed all the policies and reached consensus on their meanings. This approach permitted us to further interpret the content of each DNR policy holistically, or in context to the other policy statements, and then quantitatively compare policies according to the categories, which consisted of tallying the total number of policies in each category to include references to the themes. The quantitative comparison serves to provide the reader with a sense of how often a particular theme occurred in each stratification. 6 These reported tallies help the reader conceptualize the frequency of each theme within the stratifications. The themes that emerged from the analysis of school district policy are summarized in Table 1.
School District Policy Themes by Position of Policy.
Findings
The findings from this policy review are divided into three sections. The focus of the first section is to summarize each state’s position concerning minors with DNR Orders, which also serves to answers the first research question. In the second section, we analyze the distribution of LEA policies addressing minors with DNR Orders attending public schools. In the final section, we examine some of the themes that appear in LEA policies. The final two sections answer the remaining three research questions.
State Statutes
According to POLST, there are 29 states that allow minors to possess DNR Orders, 17 states where statutory language does not explicitly prohibit minors from possessing DNR Orders, and four states that prohibit minors from possessing DNR Orders. All states are identified below:
States that allow minors to possess DNR Orders: California, Connecticut, Delaware, Hawaii, Idaho, Indiana, Iowa, Kentucky, Louisiana, Maine, Massachusetts, Minnesota, Mississippi, Nevada, New Hampshire, New York, North Carolina, Oklahoma, Oregon, Pennsylvania, Rhode Island, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming
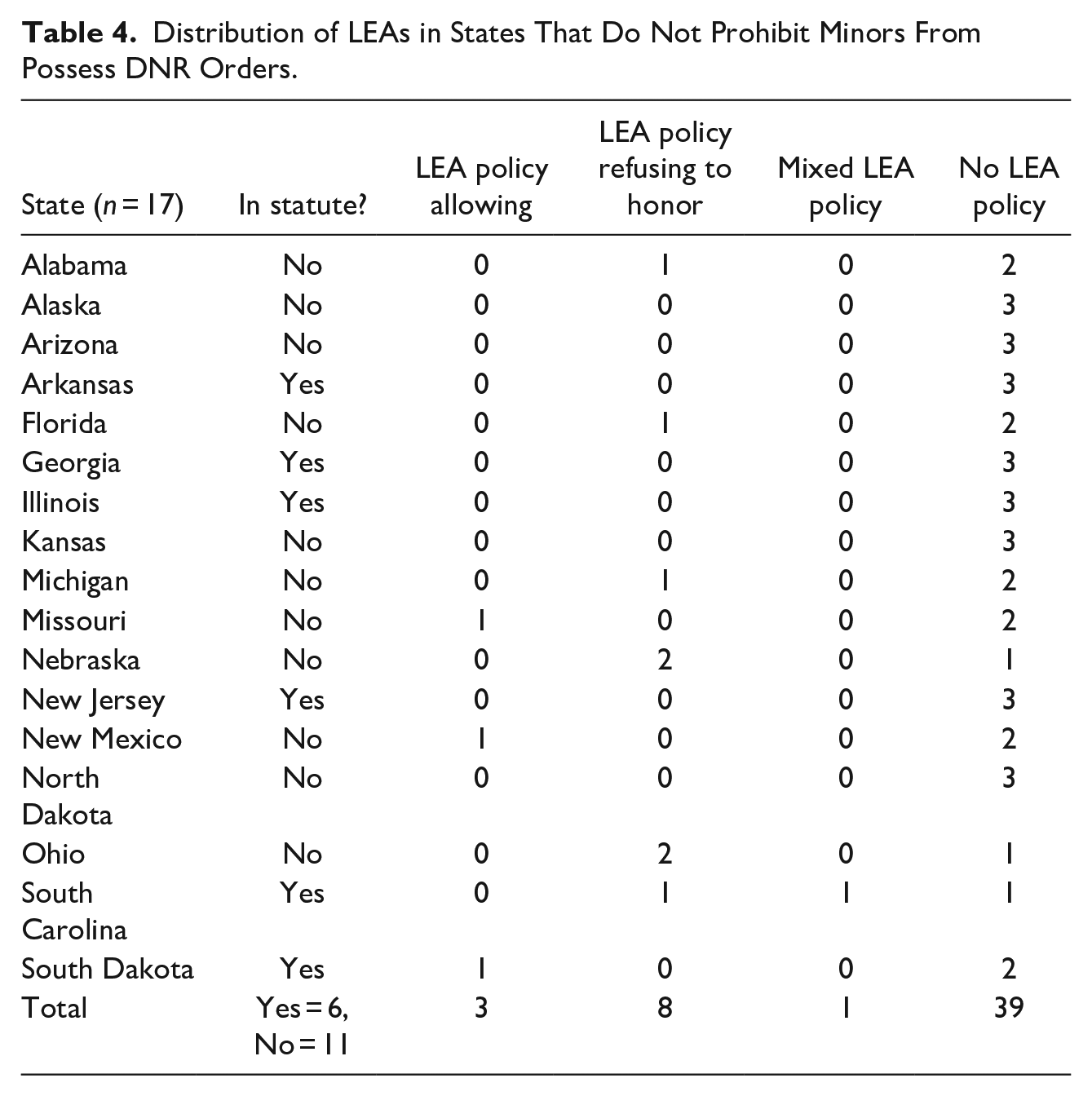
States that do not explicitly prohibit minors from possessing DNR Orders: Alabama, Alaska, Arizona, Arkansas, Florida, Georgia, Illinois, Kansas, Michigan, Missouri, Nebraska, New Jersey, New Mexico, North Dakota, Ohio, South Carolina, and South Dakota
States that prohibit minors from possessing DNR Orders: Colorado, Maryland, Montana, and Vermont
In addition, the review of POLST data determined that not all states have codified into statutes their positions concerning minors with DNR Orders. There are 33 states that have enacted statutes and 17 states that have non-statutory DNR statements, such as state guidelines, administrative procedures, or recognized practices. All are identified below:
States with DNR Rules in Statutory Language: Arkansas, California, Colorado, Connecticut, Delaware, Georgia, Hawaii, Idaho, Illinois, Indiana, Iowa, Kentucky, Louisiana, Maryland, Mississippi, Nevada, New Hampshire, New Jersey, New York, North Carolina, Oklahoma, Oregon, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, Washington, West Virginia, and Wyoming
States with DNR Rules in Non-statutory Language: Alabama, Alaska, Arizona, Florida, Kansas, Maine, Massachusetts, Michigan, Minnesota, Missouri, Montana, Nebraska, New Mexico, North Dakota, Ohio, Pennsylvania, and Wisconsin
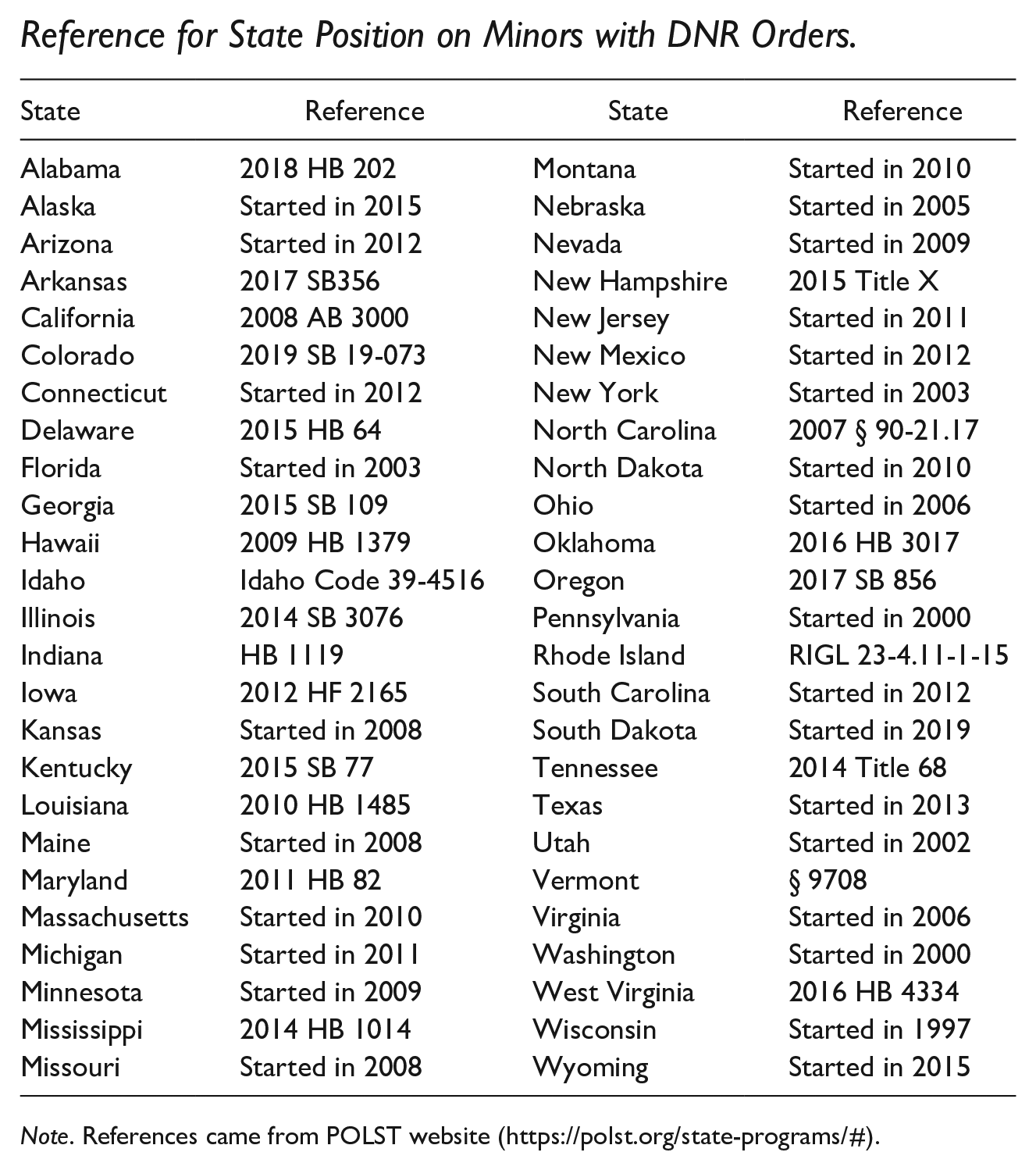
The location of each state’s statement regarding minors with DNR Orders is identified in the Appendix. In summary, the answer to the first research question (How do state statutes address the issue of minors with DNR Orders?) is that minors in most states are either authorized to possess DNR Orders (29 states) or not explicitly prohibited from possessing DNR Orders (17 states). There are only four states that explicitly prohibit minors from possessing DNR Orders.
Summary of LEA Policies
To answer the second research question (How many LEAs have policies addressing minors with DNR Orders?), we identified the three largest LEAs in each state, reviewed each LEA’s online policy manual, and, in certain cases, reached out to LEA personnel to confirm the absence of policy concerning minors with DNR Orders. The data for the 148 LEAs related to students with DNR Orders attending school in each state are summarized in Table 2.
Distribution of LEAs.
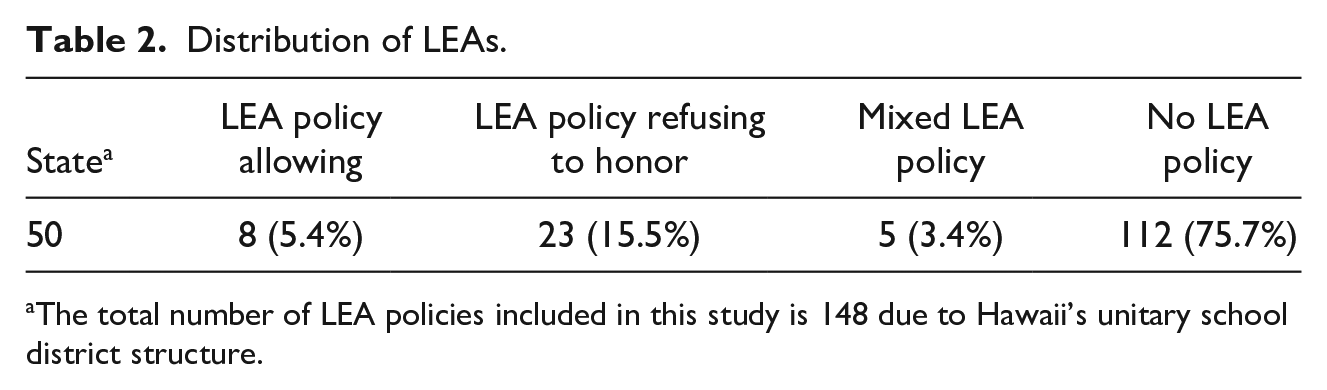
The total number of LEA policies included in this study is 148 due to Hawaii’s unitary school district structure.
As reported in Table 2, over 75% of LEAs sampled had not enacted policies addressing minors with DNR Orders attending or wishing to attend school. Of the 36 LEAs with policies, only eight honored DNR Orders. Assuming the findings reported in Table 2 are representative of all LEAs throughout the nation, these findings help to answer our second research question (How many LEAs have policies addressing minors with DNR Orders?).
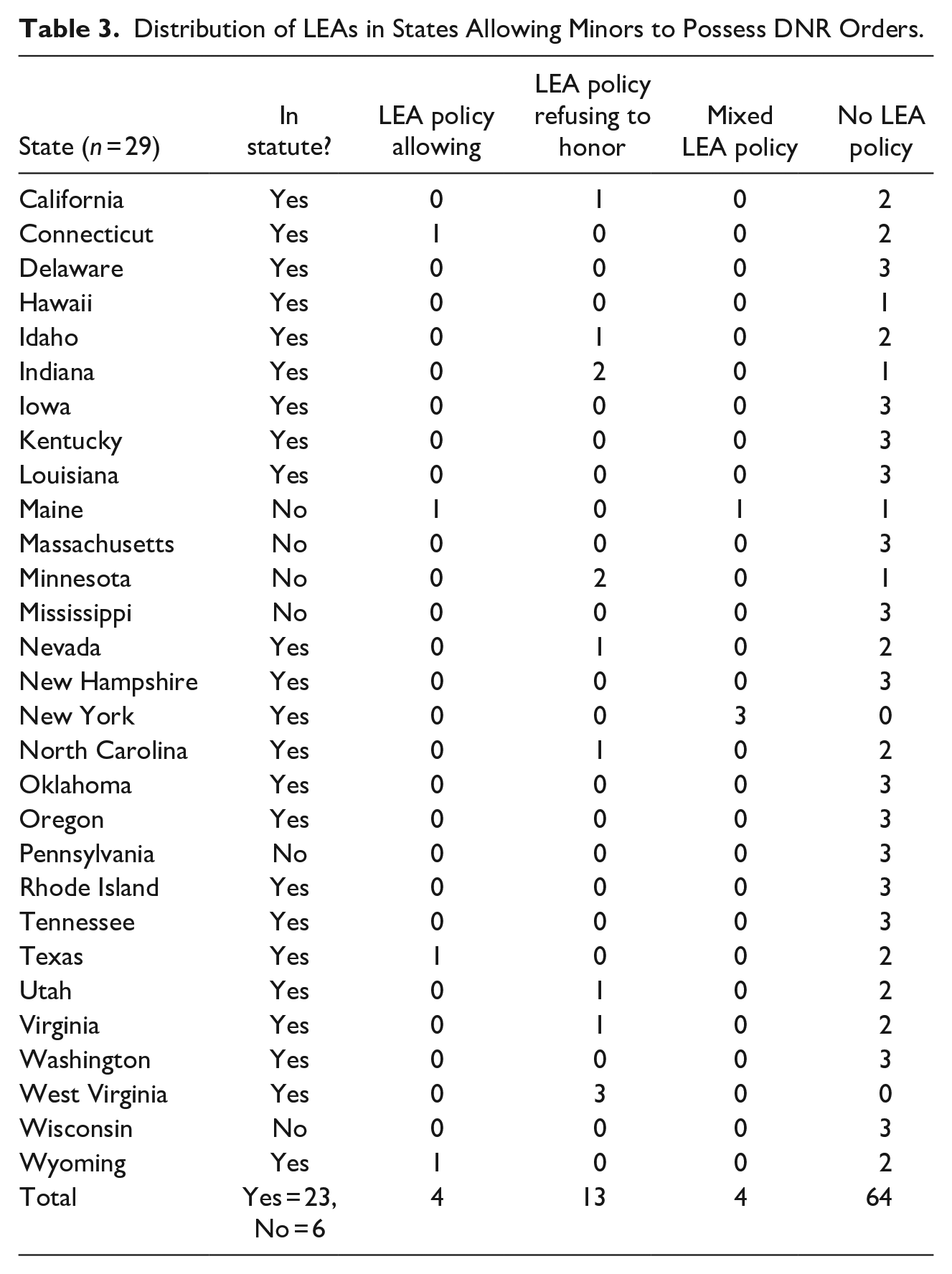
The data presented in Tables 3 to 5 disaggregate the distribution of LEA policies based on the state’s position on the issue of minors with DNR Orders.
Distribution of LEAs in States Allowing Minors to Possess DNR Orders.
Distribution of LEAs in States That Do Not Prohibit Minors From Possess DNR Orders.
Distribution of LEAs in States Prohibiting Minors to Possess DNR Orders.

Note. The LEA in Maryland with a policy allowing minors to possess DNR Orders and attend school last amended its policy in 2010, a year before the current state statute was enacted.
The significance of the findings reported in Tables 3 to 5 is summarized in Table 6.
Percent of LEAs Based on State Position Concerning Minors With DNR Orders.
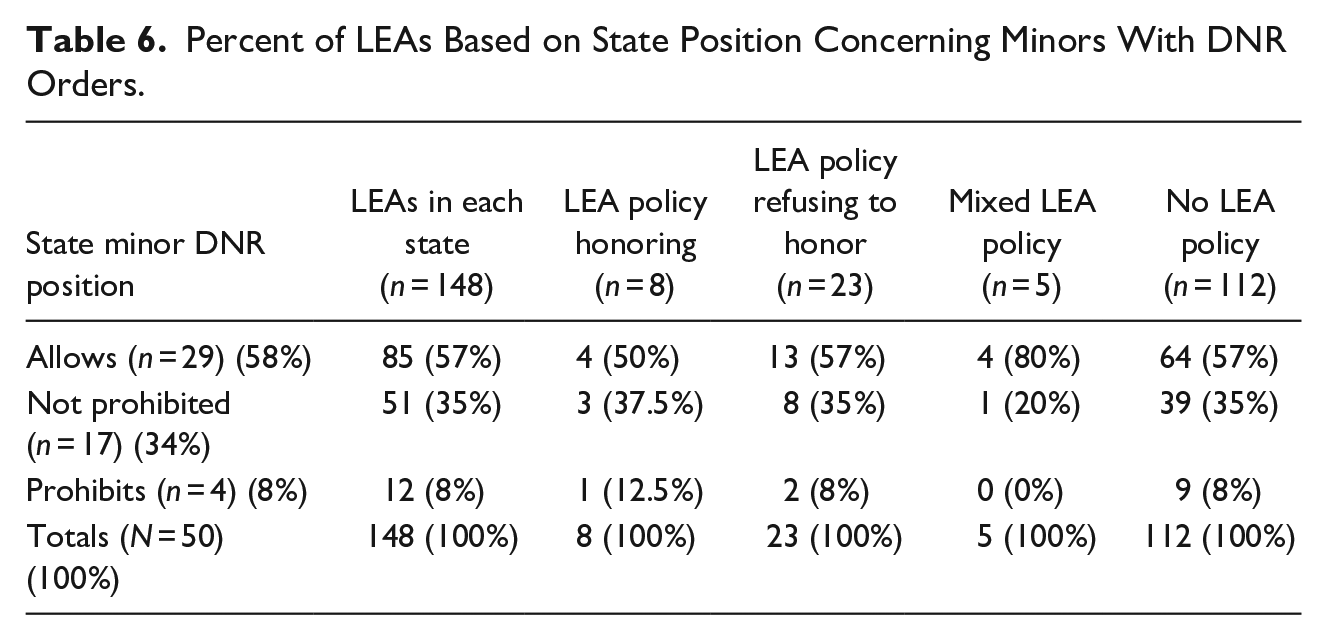
The distribution of states and LEAs, as measured by percentages, in each of the three rows closely aligns. The data reported in Table 6 seem to suggest that a state statute related to minors with DNR Orders may not influence LEAs when enacting policies on the issue.
The data reported in Tables 3 to 6 help to answer our third research question (Do state statutes and LEA policies align?). Our answer is that state statute and LEA policy appear to be created independently of one another. The top-down and the bottom-up perspectives of this issue currently lack alignment.
LEA Policies
To answer our fourth research question (What themes appear in LEA policies?), we identified themes within LEA policies addressing minors with DNR Orders. A total of 36 policies were reviewed and clustered around the three possible positions.
Themes in LEA policies that honor DNR Orders for minors
The review of the eight LEA policies honoring a minor’s DNR Order produced three overarching themes (the themes are reported in Table 1 and explained below). In addition, we identified three outliers that appeared in three or less policies but still hold potential significance for LEAs considering adopting similar policies.
Prior to exploring the specific themes, examples of the wording from these eight policies will be presented. Although the wording of policy differs among LEAs, the overarching message from these eight policies is clear—LEA officials are to honor minors’ DNR Orders. The policy for Laramie County School District (Wyoming) read, “upon receiving a written do not resuscitate order (DNR) [school district officials] will develop an individual health care plan for the student to address the medical needs stipulated within the order.” A second example comes from Lewiston School District (Maine), which stated, “The Team shall not approve a parental request to deny all life-sustaining emergency care for a student but may specify that only certain types of interventions are appropriate in a particular situation.”
All eight LEA policies required students with DNR Orders to be on an IHP. Rockwood School District’s (Missouri) policy offered the most detailed definition of an IHP for students. “An Individual Health Plan (IHP) will be developed in conjunction with the student’s parents or guardians and physician; appropriate school personnel. . .; and when appropriate, the student. This team will consider the best interests of the student.” The IHP details the protocols and procedures school personnel are to follow regarding the student’s health issues.
In addition, all eight LEAs required parents or guardians to consult with a physician before honoring the minor’s DNR Order at school. The Sioux Fall School District (South Dakota) policy required parents to submit “a written statement from both parents/guardians stating that they have discussed the possible interventions with the ordering physician and agree with the order.” A second example comes from Albuquerque Public Schools (New Mexico), which identified forms that must be completed and then states, “These forms shall be completed by the physician and the parent(s)/guardian(s).”
Five of the LEA policies acknowledged the difficult situation minors and their parents or guardians are in when they ask LEA officials to honor DNR Orders. The New Haven School District (Connecticut) policy offered this compassionate statement, “The District appreciates the difficult medical and emotional decisions that must be made when families choose to limit resuscitative efforts for these students.” These five policies provide parents or guardians clear directions on how they can go about receiving the desired support from the LEA related to the medical care of minors.
In addition to those three themes, there are three considerations referenced in less than half of these eight policies that LEAs should explore if adopting policies that allows minors with DNR Orders to attend school. In three LEA policies there were specific guidelines provided to LEA employees. These guidelines ensure employees are directed to act appropriately when supporting a student with a DNR Order. In addition, there were two LEA policies that explore the protocols and procedures addressing what is to happen when a student with a DNR Order experiences a sudden death. Finally, only three of the LEA policies explain how the DNR Order can be revoked.
Themes in LEA policies that refuse to honor DNR Orders for minors
We reviewed 23 LEA policies that prohibited school personnel from honoring a minor’s DNR Order. These policies require CPR be administered to all students, including terminally ill students, until medical personnel arrive at school. There is one overarching theme within these policies—that DNR Orders will not be honored. However, the discussion of these policies examines some of the reoccurring themes within these prohibitive policies.
One of the most succinct policies on the topic of minors with DNR Orders attending school comes from Mobile County Public Schools (Alabama). The entire policy is as follows, “No DNAR (Do Not Attempt Resuscitation) requests from parents or guardians will be honored under any circumstance.” Dearborn City School District’s (Michigan) policy offered a similar degree of clarity on the school district position, “Whenever it is necessary for staff members to use emergency procedures in order to care properly for a student, they are to follow the procedures described in the Superintendent’s administrative guidelines and are not to abide by any ‘Do Not Resuscitate’ (DNR) agreement that may exist for a student.”
We found it interesting that LEA policy refusing to honor a minor’s DNR Order provided additional direction beyond the LEA’s overarching position because these added policy statements were unnecessary given the LEA had stated that any DNR Order would not be honored. As an example of these superfluous statements, nine LEA policies required parents or guardians to consult with physicians even though a minor’s DNR Order is a directive from a physician. LEAs also often used language such as request, agreement, or wishes rather than acknowledging the DNR Order as a medical directive. LEAs implied in policy that they are the ultimate decision maker regarding the DNR Order and the parents and physicians are simply making a request or expressing their wishes.
There were nine school board policies that specifically stated the only way a minor’s DNR Order will be honored by the LEA is by a court order. As an example, the Hillsborough County Public Schools’ (Florida) policy read, “Staff members are not to abide by any ‘Do Not Resuscitate’ (DNR) agreement that may exist for a student unless ordered to do so by a court of law.” In effect, school district officials are directing parents or guardians of students with terminal illnesses to commit time and resources toward a legal battle while also caring for the child.
Within the 23 LEAs with policies refusing to honor minors’ DNR Orders, there was evidence that LEA personnel will attempt to work with the students and their families. Horry County Schools (South Carolina) offered this statement, “When EMS arrives at the school, the school will present to the EMS employees a copy of the DNR Order for their review and consideration. The EMS personnel may take into account the order as they assist the student.” A second example of this accommodation came from Minneapolis Public Schools (Minnesota), which read, “Upon arrival of emergency medical responders, the person’s DNAR or DNI [Do Not Intubate] order shall be delivered to the responders by the principal or the principal’s designee.”
The final point related to these policies comes from Horry County Schools (South Carolina). This was the only policy accessed that provided an explanation for refusing to honor a minor’s DNR Order. The policy stated that South Carolina law “does not provide school officials with immunity from civil or criminal liability for good faith compliance with a DNR Order, as is provided to EMS personnel and health care providers.”
Themes in policies with mixed guidance
The final grouping consisted of LEA policies that sent mixed messages regarding minors with DNR Orders attending school. These policies may overlap with the policies that honor a minor’s DNR Order, but they also overlap with the policies refusing to honor a minor’s DNR Order.
These five policies established their uniqueness by clearly stating a minor’s DNR Order will not be honored at school, but then offered an exception to the prohibitive policy. An example of this mixed policy was found in Bangor School Department (Maine), which read, “It is the policy of the Bangor School Department not to comply with directives from parents or others that life-sustaining emergency care should not be provided to any particular student in need of such care while under the control and supervision of the school. . . For those students who may present an ongoing need for medical interventions at school, including a need for life-sustaining emergency care, school personnel shall convene a team. . . The Team shall not approve a parental request to deny all life-sustaining emergency care for a student but may specify that only certain types of intervention are appropriate in a particular situation.” Finally, all five LEA policies stated students would need to be placed on an IHP.
Discussion
Our discussion is divided into five sections. In the first section, we discuss the unique nature of this issue. Then we explore the implications of the findings through the perspectives of a top-down and a bottom-up theorical framework. Next, we identify issues of equity embedded in the current practice of LEAs when it comes to educating students with DNR Orders. Finally, we examine the implications of LEAs enacting policy that refuse to honor DNR Orders.
Wicked Problem?
We began our study with the intention of identifying an underlying logic explaining why some states and LEAs have developed prohibitive DNR Order polices while others have permissive policies. We initially applied Elazar’s Political Culture Theory (Elazar, 1966) to understand the context in which DNR Orders are developed but this proved unfruitful as there seemed little underlying logic connecting a state’s approach to DNR Orders for minors. We also attempted to understand states’ adoption of DNR Order policies using policy diffusion, but this also failed to enhance our understanding of the issue. Finally, we attempted to determine if specific events or an instance of a child dying on school grounds shaped state adoption of DNR policies. However, a search of school board minutes, legal cases, and public legislative agendas found only one occurrence (ABC School v. Mr. and Mrs. M, 1997).
While causal or correlational relationships may exist, we were unable to identify them. We believe that when our topic is viewed as a public policy issue, it takes on some elements of being a “wicked problem”—an issue that does not to yield to rational problem solving (Rittel & Webber, 1973). Wicked problems are generally open-ended, complex, and intractable with the nature of the “problem” and the preferred “solution” are strongly contested (Head, 2008). Because actual deaths occurring on school grounds are extremely rare, there is no opportunity to develop evidence-based solutions. As a result, trial-and-error approaches yield to often conflicting stakeholder preferences (Head, 2008; Head & Alford, 2013; Rittel & Webber, 1973). Parents, school leaders, teachers, lawyers, and healthcare professionals frame the nature of the problem and possible solutions in value-laden interpretations, sometime grounded in competing ethical frameworks.
If the wicked problem explanation for each state’s approach to addressing our topic is plausible, then each policy is perhaps understood as a temporary political accommodation informed by whatever stakeholders consider the best available evidence and the quality of leadership in defining shared goals. It seems likely that specific and tragic circumstances helped initiate state and LEA level policy on our topic, but we were unable to find enough evidence to substantiate this assumption. We arrived at our top-down bottom-up approach because efforts to explain why states and LEAs have permissive or prohibitive policies were unsuccessful.
Top-down Theorical Framework
The data analyzed in this study included a review of state statutes concerning minors with DNR Orders. While there were 29 states that had clear statutory language allowing minors to possess DNR Orders, there were 17 states with statutes that did not explicitly prohibit minors from possessing. Implicit in this finding is that these 17 states lack clarity in enacted statutes. This lack of clarity within statutory language could be contributing to the conflicting policy positions passed by LEAs within the same state.
The review of state statutes addressing minors possessing DNR Orders suggests that from the top-down perspective, states primarily limit their policies to achieve one of the three possible positions (allows, does not prohibit, and prohibits) without addressing many of the ethical and logistical issues. Pragmatically, states must also consider who is required to administer medical aid in an emergency and, therefore, adopt liability protections and directives about who must give aid in an emergency. Only four states explicitly prohibit minors from having DNR Orders. However, we were unable to identify an explanation for why these four states prohibit minors from having DNR Orders.
Another point of consideration related to the top-down perspective of minors with DNR Orders attending public school is that 17 states have not enacted statutes on this topic. Instead, these states rely on guidelines, administrative procedures, or recognized practices to inform action at the local level. The lack of clear state statutes concerning minors with DNR Orders leaves LEAs on their own to create policies. LEAs may prioritize fear of litigation over doing what is best for a student with a terminal illness. The LEA administrators creating the policies may lack a clear understanding of a DNR Order as a medical directive issued by a physician, how DNR Orders are written, and the ethical considerations for children with terminal illnesses.
Finally, when examining the issue of minors with DNR Orders attending public school, the data presented in Table 6 illustrate that state statute fails to consistently influence LEA policy. This conclusion is based on the distribution of states and LEAs in each of the three rows (allow, not prohibited, and prohibited). If the state, or the top, was consistently influencing LEA policy, there would be evidence of this influence in the distribution of policy positions across the three rows. The findings included in this study suggest a breakdown in LEA policy when it comes to educating a minor with a DNR Order and this breakdown could be contributable to the fact that state statute is sometimes failing to influence LEA policy and practices.
Bottom-up Theorical Framework
The data presented in this study illuminate a disconnect between state statute and LEA policy on the issue of minors with DNR Orders attending schools. This disconnect is the reason the top-down, bottom-up theoretical framework helps add meaning to the findings. It is as if the states and the LEAs are working independently. And, given that LEA policy is governing the actions of school personnel, the bottom-up perspective of the theoretical framework currently enjoys the greatest degree of influence on minors with DNR Orders attending or wishing to attend public schools. Weatherly and Lipskey (1977) referred to this grass-roots form of policy development as “street-level bureaucracy,” or bureaucracy from the lowest organizational level. In this study, the LEA would be the lowest bureaucratic level of policymakers.
As was reported in Table 2, over 75% of LEAs do not have policies addressing the issue of minors with DNR Orders attending public schools. While the reasons for this policy omission are unknown, a future examination may determine why LEAs developed policies on the topic of students with DNR Orders. LEAs without policies addressing students with DNR Orders will be forced to develop such policies when faced with a minor with a DNR Order. Of concern is that LEAs may create a reactive policy in response to fear of liability related litigation and, consequently, prohibit minors with DNR Orders from attending public schools (Volante, 2015).
To support the suggestion that LEAs will only develop reactive policy when forced to consider the issue, the data in Table 2 also reported that 64% of LEAs with policies on the issue refuse to honor a minor’s DNR Order. In effect, these prohibitive policies are failing to acknowledge the professional expertise of the physician(s) who signed the DNR Order. As a result, these students are being forced to choose between a “normal” educational experience at the end of their lives without having their DNR Order honored or a home-bound educational experience where the DNR Order will be honored.
The remaining LEA policies honor students’ DNR Orders (5.4%) or have mixed guidance (3.4%). We recommend that the LEAs with mixed guidance work on revising existing policy to enhance clarity and provide children with terminal illnesses the educational services to which they are entitled. The current structure which relies on the goodwill of the LEA does not serve the best interests of students with terminal illnesses.
Issues of Equity
The review of LEA policies found potential equity issues that merits further examination beyond the scope of this research project. Many of the LEA policies are either ambiguous or even contradictory. For a minor to have a DNR Order requires consultation with physicians and potentially attorneys. LEAs that require court orders are creating barriers for families that may not have the time or the additional finances for the legal assistance to seek a court order to force an LEA to honor a DNR Order. Therefore, the ability to develop a DNR Order for minors in states which permit them may be difficult for poorer families.
Implications of Refusing to Honor a DNR Order
LEAs who refuse to honor DNR Orders have no clear vested legal authority to do so. In states with statutes that provide for DNR Orders for minors, we find it illegal for a LEA, as an extension of the state, to refuse to follow a state statute. LEAs who refuse to allow children with DNR Orders to attend traditional schools are potentially engaging in an act of discrimination. Forcing children with terminal illnesses into homebound services without considering their individual educational needs or IHPs is a violation of Section 504 and a form of discrimination. LEAs whose policies require a court order to force them to honor a DNR Order are knowingly placing an undue burden on parents and students. Additionally, the actions of LEA personnel who knowingly perform CPR and the administrators who direct them to do so in violation of an authorized DNR Order could be judged as having committed an act of assault on a dying child. These intentional violations of a child’s DNR Order are not actions made in good faith as defined under “Good Samaritan” Laws, but a blatant disregard of consent—a primary component of the law (West & Varacallo, 2020).
LEAs with policies refusing to honor DNR Orders may be governed by a lack of clear understanding of the appropriateness of CPR as a therapy for child with a terminal illness, a fear of liability, or the social and psychological pressure to ignore the reality that children with terminal illnesses experience a natural death. Regardless of the motives and intentions of LEAs, refusing to honor the DNR Order or allow a child with a DNR Order to attend school has both potential ethical and legal implications.
Recommendations for Policymakers
Based on the findings and discussion included in this study, we offer recommendations to federal, state, and LEA policymakers.
Recommendation for Federal Policymakers
We believe the U.S. Department of Education could issue a “Dear Colleague” Letter interpreting the application of Section 504 of the Americans with Disabilities Act and other pertinent federal law to the issue of minors with DNR Orders attending or wishing to attend public schools (Petersen, 2005). Such a letter may offer support to students with DNR Orders and provide liability protection for school personnel who, in good faith, follow its direction. If the federal government provided such guidance based on federal law, the states would not need to have 50 different statutes that conflict or contradict one another on this issue. The response to a DNR Order should not be state specific but based on ethical and medical considerations that should not change regardless of the locale.
Recommendations for State Policymakers
State policymakers should ensure that the state position concerning minors possessing DNR Orders allies with medical ethics, considers medical advancements, aligns with other laws regarding privacy and consent in medical care, and respects the rights of individuals. The state position should be codified in statutory language. In addition, state policymakers should work closely with LEAs to ensure that the latter has policy on the issue of students with DNR Orders attending school and that the enacted policy aligns with state statutes. Finally, states need to acknowledge the fear of litigation that LEA officials may have and extend to them liability protections so that students with DNR Orders are afforded the opportunity to experience a “normal” school experience. Additionally, state policymakers should provide school personnel with clear guidance and training on this sensitive and emotional issue, including the consequences of failing to follow the student’s IHP.
Recommendations for LEA Policymakers
LEA policymakers, like state policymakers, should ensure that the LEA position concerning minors possessing DNR Orders allies with medical ethics, considers medical advancements, aligns with other laws regarding privacy and consent in medical care, and respects the rights of individuals. LEAs should also ensure their policies align with state statutes and proactively enact policy on this issue (Adelman, 2011).
Based on our analysis of the factors related to students with DNR Orders attending or wishing to attend school, we recommend LEAs should honor such orders. Given that a DNR Order is a physician’s medical directive and is a legal document, LEA officials who refuse to honor such a document could be placing themselves, their personnel, and the LEA in precarious situations. As the likelihood of terminally ill students attending school increases, LEAs with prohibitive policies could face litigation from students or their parents or guardians for being denied access to a “normal” educational experience and other possible legal challenges.
The National School Board Association and other groups that create model school board policies should provide guidance and policy recommendations for their members. Additionally, school superintendents, school board attorneys, and other school administrators should be educated and informed on this issue. Proactively addressing this topic is in the best interests of all involved.
Limitations and Conclusion
Despite efforts to secure LEA policies for the three largest school districts in each state, it is possible that more policies exist and were not located, that policies were either enacted or revised and the new policy statement was not yet available on the LEA’s website, or that procedures or guidance regarding minors with DNR Orders appeared in administrative handbooks or other documents outside of policy manuals. In addition, there is a possibility that policies were misinterpreted. While most policies were very clear, a few were ambiguous. To guard against this potential error, each state statue and LEA policy was reviewed by all three authors to reach consensus on the meaning of the policy statements.
As medical advancements further permit terminally ill minors to attend schools in traditional settings, it seems plausible that the issue of students with DNR Orders will need to be addressed more widely. While Section 504 of the Rehabilitation Act (1973) would suggest terminally ill students have certain educational rights, there is a lack of federal guidance related to the rights of these children to have their DNR Orders honored on school premises. Some states authorize minors to possess DNR Orders but do not address the relevant pragmatic issues. At least a third of states do not provide clear language on the topic, leaving LEAs to address the issue on their own. Still others continue to prohibit minors from possessing DNR Orders.
We conclude that the range of state statutes and LEA policies appears inconsistent and filled with contradictions. We are left asking how these different responses to a minor’s DNR Order can both be socially acceptable and legally defensible? These inconsistencies create confusion over an issue that needs clear guidance from policymakers. Children with terminal illnesses deserve not only society’s compassion but are entitled to legal protections concerning their DNR Orders.
Footnotes
Appendix
Reference for State Position on Minors with DNR Orders.
| State | Reference | State | Reference |
|---|---|---|---|
| Alabama | 2018 HB 202 | Montana | Started in 2010 |
| Alaska | Started in 2015 | Nebraska | Started in 2005 |
| Arizona | Started in 2012 | Nevada | Started in 2009 |
| Arkansas | 2017 SB356 | New Hampshire | 2015 Title X |
| California | 2008 AB 3000 | New Jersey | Started in 2011 |
| Colorado | 2019 SB 19-073 | New Mexico | Started in 2012 |
| Connecticut | Started in 2012 | New York | Started in 2003 |
| Delaware | 2015 HB 64 | North Carolina | 2007 § 90-21.17 |
| Florida | Started in 2003 | North Dakota | Started in 2010 |
| Georgia | 2015 SB 109 | Ohio | Started in 2006 |
| Hawaii | 2009 HB 1379 | Oklahoma | 2016 HB 3017 |
| Idaho | Idaho Code 39-4516 | Oregon | 2017 SB 856 |
| Illinois | 2014 SB 3076 | Pennsylvania | Started in 2000 |
| Indiana | HB 1119 | Rhode Island | RIGL 23-4.11-1-15 |
| Iowa | 2012 HF 2165 | South Carolina | Started in 2012 |
| Kansas | Started in 2008 | South Dakota | Started in 2019 |
| Kentucky | 2015 SB 77 | Tennessee | 2014 Title 68 |
| Louisiana | 2010 HB 1485 | Texas | Started in 2013 |
| Maine | Started in 2008 | Utah | Started in 2002 |
| Maryland | 2011 HB 82 | Vermont | § 9708 |
| Massachusetts | Started in 2010 | Virginia | Started in 2006 |
| Michigan | Started in 2011 | Washington | Started in 2000 |
| Minnesota | Started in 2009 | West Virginia | 2016 HB 4334 |
| Mississippi | 2014 HB 1014 | Wisconsin | Started in 1997 |
| Missouri | Started in 2008 | Wyoming | Started in 2015 |
Note. References came from POLST website (https://polst.org/state-programs/#).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.