
Abstract
Osteoarthritis (OA) affects more than half of all persons above age 65 (Felson & Zhang, 1998) and is the leading cause of late-life disability (Burns, Graney, Lummus, Nichols, & Martindale-Adams, 2007; Theis, Helmick, & Hootman, 2007). However, not all OA sufferers are equally affected by its characteristic pain and disability. A developing literature suggests that race and sex, in particular, may markedly affect the experience and effects of OA. Risk of OA is higher among women than men (Dunlop, Manheim, Song, & Chang, 2001; Verbrugge, 1995), and particularly among African American (Black) as compared with non-Hispanic White (White) women 1 (Felson & Zhang, 1998; Kington & Smith, 1997). The literature also fairly consistently indicates that, as with other pain syndromes (Fillingim, King, Ribeiro-Dasilva, Rahim-Williams, & Riley, 2009), women experience greater OA-related pain (Affleck et al., 1999; Keefe et al., 2000; Perrot, Poiraudeau, Kabir-Ahmadi, & Rannou, 2009; Theis et al., 2007) and disability (Axford, Heron, Ross, & Victor, 2008; Theis et al., 2007) than do men.
Research on racial differences in OA prevalence and symptoms is less plentiful and less consistent. As just noted, Black women appear to be at particularly high risk of at least some forms of OA, but there is little consensus beyond that. Some investigators have found no racial differences in OA pain intensity and disability (Ang, Ibrahim, Burant, Siminoff, & Kwoh, 2002; Burns et al., 2007; McIlvane, Baker, & Mingo, 2008); others report that Blacks experience significantly more severe symptoms (Allen et al., 2010; Burns et al., 2007). At least one study indicates that results may differ as a function of measurement approach, that is, self-report versus performance measures (Burns et al., 2007), suggesting a complicated interaction of objective symptoms and subjective experience.
Extant research on emotional effects of OA is similarly complex. OA is known to place older adults at heightened risk of depression 2 (Adams et al., 2008; Axford et al., 2008; Davis, Ettinger, Neuhaus, Barclay, & Segal, 1992; Lindesay, 1990; Machado, Gignac, & Badley, 2008; Parmelee, Harralson, Smith, & Schumacher, 2007; Stubbs et al., 2010). Emotional distress, in turn, interacts with physical symptoms in complex ways. An emerging literature suggests that OA pain is the root cause of both disability and depressive symptoms (Parmelee et al., 2007) and that it puts individuals at risk of more rapid functional decline (Dekker, van Dijk, & Veenhof, 2009). Indeed, recent evidence suggests that the causal effect of current pain on future disability may be at least partially due to depression (Machado et al., 2008). More general (non-OA-specific) research indicates that depression may exacerbate the association of pain with disability (Ullrich, Askay, & Patterson, 2009) and that there are mutually influential, “downward spiral” associations of depression with pain (Chou, 2007; Schieir et al., 2009) and functional disability (Lenze et al., 2001) over time.
Together, these findings highlight the importance of delineating how individual difference factors such as sex and race may interact with physical and psychological processes to affect long-term well-being of older adults with OA. For example, if Black women experience particularly severe OA symptoms, they may be more prone to depression—which, in turn, could put them at disproportionate risk of marked functional decline. Yet we know surprisingly little about how basic demographic factors interact in persons with OA. It is well established that women in general are more likely to experience significant depression (Weissman & Klerman, 1977), but there has been little exploration of how those differences manifest in associations with pain and disability. Existing work with varied (non-OA) populations suggests that the associations of pain with depression (Adams et al., 2008) and with disability (Hirsh, Waxenberg, Atchison, Gremillion, & Robinson, 2006) may be stronger among women than men; others, however, have found quite different results. For example, Geerlings, Twisk, Beekman, Deeg, and van Tilburg (2002) found a stronger association of pain with depression among men than in women. Haley, Turner, and Romano (1985), in contrast, found that pain was more strongly associated with depression in women but with activity impairment in men. Interestingly, one recent study of German primary care patients with OA (Rosemann, Laux, & Szecsenyi, 2007) reported that, despite women’s greater disability, they displayed no greater depressive symptomatology than did men.
Similarly, general population studies reveal few racial differences in rates of depression (Kessler et al., 2003). However, work with chronic pain populations has variously reported that, as compared with Whites, older Blacks report greater pain, disability, and depression (Green, Baker, Smith, & Sato, 2003); greater disability but equivalent pain and depression (Ndao-Brumblay & Green, 2005); equivalent pain but greater disability and depression (Riley et al., 2002); equivalent pain but more disability (McIlvane et al., 2008); and greater pain but less disability (Bruce, Fries, & Murtagh, 2007). The bulk of this work addresses simply prevalence of symptoms, but there is some evidence that pain and disability may be more strongly associated with depression among Blacks as compared with Whites (McIlvane et al., 2008; Riley et al., 2002).
In short, although some consistent patterns are emerging, existing evidence regarding sex and race differences in associations among pain, depression, and disability is spotty. To help fill that gap, this research examines how race and sex affect the associations of pain and disability with depressive symptoms in a sample of older adults with OA of the knee. We first delineate basic race and sex differences in pain severity, extent of disability, and depressive symptoms both generally and with control for relevant covariates. We then explore how race and sex influence the associations of pain and disability with depression. We hypothesize, given literature just reviewed, that pain and disability will be greater among Blacks than Whites but that depression will be equivalent in the two groups. Women are expected to report more severe symptoms on all three variables. Previous research suggests that associations of pain and disability with depression will be stronger among women than men (Adams et al., 2008; Hirsh et al., 2006) and among Blacks than Whites (McIlvane et al., 2008; Riley et al., 2002). Finally, we hypothesize that effects of race and sex will be additive, such that the effects of pain and disability will be greatest for Black women and lowest for White men.
Method
Sample
Greater Philadelphia residents with knee OA were recruited from a university rheumatology clinic (N = 53, 14.6% of total sample), a Veterans Affairs Medical Center (VAMC; 44, 12.2%), two general geriatric outpatient clinics (44, 12.2%), persons who had completed a past psychoeducational study of OA (46, 12.7%), and through public service announcements in newspapers and on radio (PSAs; 175, 48.2% of total). Recruitment site information was missing for one participant. All participants had physician-confirmed knee OA, were able to respond to questions in English, and had no life-threatening or severely disabling medical conditions (e.g., cancer, chronic obstructive pulmonary disease).
Recruitment methods were approved by institutional review boards at participating institutions. At clinics where investigators were affiliated, eligible patients were identified through medical chart review; they then received a physician’s letter alerting them to an imminent telephone call from project staff. Elsewhere, study fliers were offered in the waiting room or by attending physicians; as for PSA respondents, interested individuals telephoned the research office. Initial phone contacts confirmed interest and eligibility and scheduled data collection. Respondent’s signed consent for physician confirmation of the knee OA diagnosis was a condition of participation. Confirmation was achieved either by review of the medical record at the treating clinic or by direct contact with the respondent’s physician. All respondents received US$25 for completing the baseline questionnaire and survey on which this report is based. Table 1 describes the final sample of 363 Black and White participants.
Characteristics of Study Participants as a Function of Race and Sex
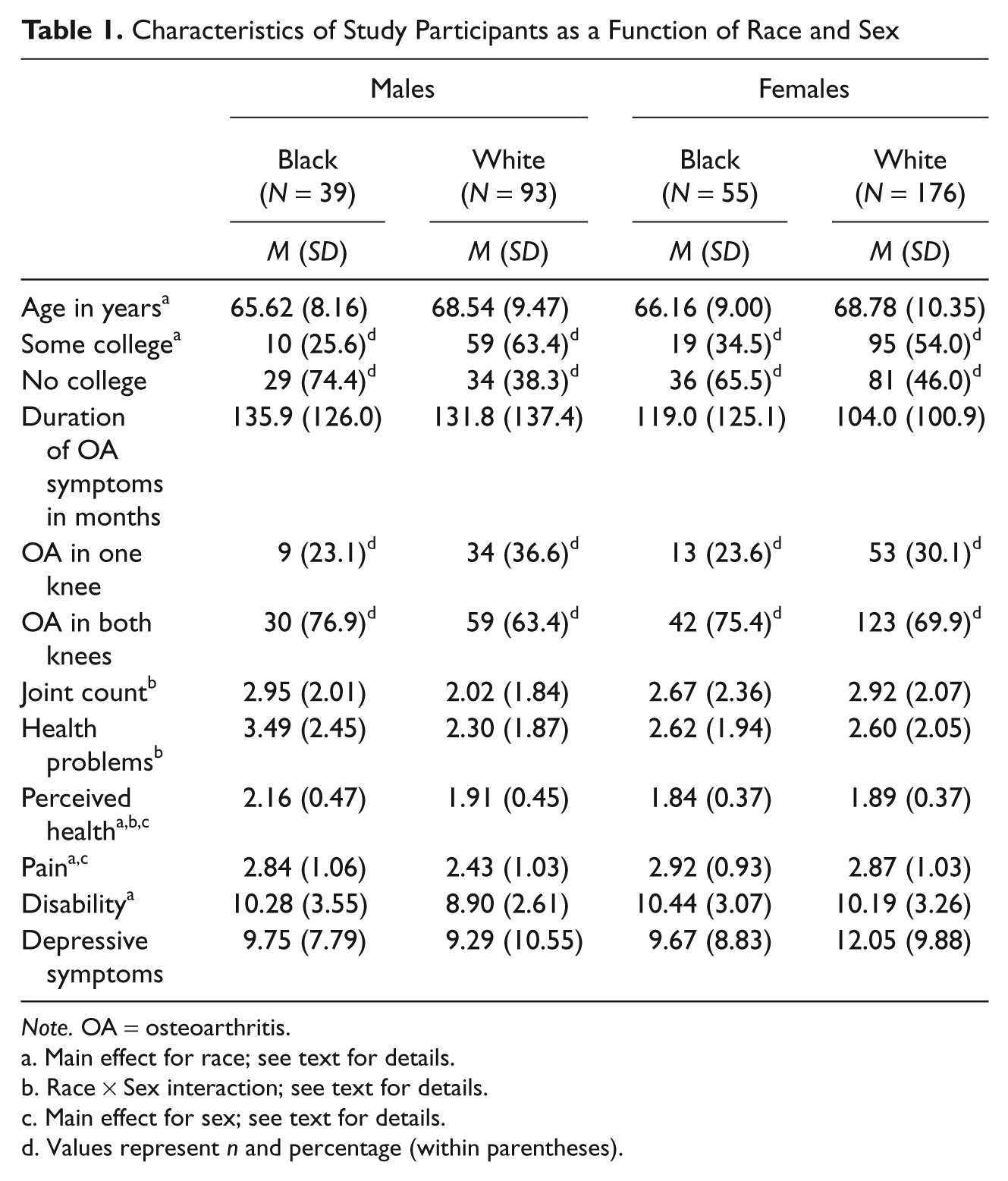
Note. OA = osteoarthritis.
Main effect for race; see text for details.
Race × Sex interaction; see text for details.
Main effect for sex; see text for details.
Values represent n and percentage (within parentheses).
Measures and Procedure
After assenting via telephone, respondents were mailed questionnaires and consent forms for independent completion. An in-person interview occurred within 2 weeks to review and clarify completed questionnaires, collect additional data, and obtain signed consent for physician confirmation of knee OA.
This report uses six classes of variables. Demographic characteristics include age, sex, race, and education.
Arthritis status included duration of symptoms, OA in one or both knees, and a count of other OA-affected joints.
Health was represented by (a) number of health problems endorsed on a 31-item checklist (Lawton, Moss, Fulcomer, & Kleban, 1982) and (b) perceived health, measured by a 3-item composite tapping overall health (4-point scale, excellent to poor), health now versus 5 years ago and versus others the same age (both rated “better,” “the same,” or “worse”). Higher scores indicate poorer perceived health; scores can range from 1 to 4.
The 20-item Center for Epidemiologic Studies Depression scale (CES-D; Radloff, 1977) tapped depressive symptoms, α for this sample = .89. Possible scores on this widely used scale can range from 0 to 60.
Pain was assessed with the 6-item Philadelphia Geriatric Center (PGC) Pain Scale (Parmelee, Katz, & Lawton, 1991); α = .84. Possible range of scores is 0.71 to 5.71. As this was a study of OA pain specifically, we felt it important to evaluate both generalized and OA-specific pain. We therefore computed a measure of OA pain by combining that scale, modified to reference OA pain, with the Pain subscale of the Arthritis Impact Measurement Scales–2nd edition (AIMS2; (Meenan, Mason, Anderson, Guccione, & Kazis, 1992). Both instruments used 5-point scales; hence, no transformation of scores was required. Alpha for the resulting composite was .89. The two pain measures correlated at r = .90.
Functional disability was assessed with AIMS2 subscales tapping mobility, walking and bending, hand and finger function, arm function, self-care, and household tasks (total of 28 items, each scored on a 5-point scale); scores were averaged to yield a single composite (α = .78). Possible range of scores is 6 to 36.
Analytic Plan
Analysis of variance (ANOVA) examined effects of race and sex on pain, depression, and disability, both alone and controlled for demographics, arthritis status, and general health. Selection of control variables was based on descriptive analyses depicted in Table 1. Specifically, variables that differed significantly as a function of race and/or sex were retained as covariates; these included age, education, joint count, and perceived and objective health. Duration of symptoms and whether OA was present in one or both knees were eliminated from further analysis. Ideally, one would use structural equations to test associations among race, sex, pain, disability, and depression, but this was precluded by small Ns for males and Blacks. Instead, we used ordinary least squares (OLS) regression, with hierarchical block entry of variable classes. The hierarchical analyses first examined demographic influences on depression. We then stepped in joint count and health status; pain and disability; and interactions of race and sex with covariates, pain and disability. Because of the strong collinearity of pain and disability (see Results) as well as problems accompanying use of multiple interaction terms, we examined the latter, interactive effects in separate analyses.
Analyses using general versus OA-specific pain measures were virtually identical. 3 As the OA-specific measure has not been validated, it is not reported here. To explore confounding of physical and mental health symptoms, we also reran analyses excluding CES-D items tapping somatic symptoms. Effects were identical.
Results
Race and Sex Differences
Table 1 presents sample characteristics by race and sex. It is important to note that those factors were confounded to some extent with recruitment site. Specifically, Blacks comprised 25.6% of the total sample but were disproportionally represented among VAMC (47.7% of site total) and rheumatology clinic (47.2%) subsamples. Conversely, they were underrepresented among geriatric outpatient clinic (18.2%) and PSA (13.1%) groups, χ2(4) = 41.73, p < .001. Similarly, the 132 men in our sample (36.4% of total) were drawn disproportionately from the VAMC (88.6%); women were more likely to have been sampled from geriatric outpatient (84.1%) and rheumatology clinics (73.6%), χ2(4) = 64.20, p < .001. Importantly, however, there were no interactive patterns of recruitment of Black and White men and women within sites. Thus, for example, of the 44 VAMC participants, 19 were Black men and 20 were White men; among PSA respondents, men comprised 31.6% of Whites and 30.4% of Blacks. 3
Whites were older than Blacks, F(1, 359) = 5.39, p < .03, and more likely to have attended college, χ2(1) = 19.42, p < .001. We found no main effects of race and sex for duration of symptoms, joint count, or involvement of one versus both knees. A Race × Sex interaction for joint count, F(1, 359) = 5.42, p < .02, reflected relatively low counts among White men.
Black men reported the highest number of health problems and White men the lowest, Sex × Race interaction, F(1, 359) = 5.42, p < .02 (Table 1). Men self-reported significantly poorer health than did women, F(1, 359) = 11.77, p < .001, and Blacks than did Whites, F(1, 359) = 4.09, p < .045. A Race × Sex interaction, F(1, 359) = 9.89, p < .002, stems primarily from Black men’s disproportionately poorer perceived health.
Women reported greater pain intensity than did men, F(1, 359) = 4.19, p < .042, and marginally greater disability, F(1, 359) = 3.57, p < .06. Blacks were significantly more disabled than Whites, F(1, 359) = 4.58, p < .035, and reported marginally greater pain, F(1, 359) = 3.49, p < .062. Interactions of race and sex were not significant for either pain, F(1, 359) = 2.10, or disability, F(1, 359) = 2.19. There were no group differences in depression, all Fs < 1.5; variances were also comparable, Levene’s F(3, 358) = 1.38.
Reanalyses controlling age, education, joint count, health problems, and perceived health eliminated effects of race for both pain and disability. The sex difference for pain remained significant, and the marginal effect for disability was strengthened, F(1, 354) = 9.37, p < .002. For depression, control of covariates yielded a significant effect of race, F(1, 354) = 4.68, p < .035, due to a slight lowering of scores for Blacks (adjusted M = 8.54, vs. raw M = 9.70) but not for Whites (11.12 vs. 11.17).
Associations of Pain and Disability With Depression
Based on these analyses, OLS regression analyses predicting depression used age, education, joint count, health problems, and perceived health as covariates, along with pain, disability, race, and sex. In initial analysis, tolerance statistics indicated collinearity of disability with health problems (r = .439) and pain (r = .548) and of health problems with perceived health (r = .395). As disability and pain are of primary interest, we retained both. We dropped health problems, retaining perceived health based on its established impact on well-being of older adults beyond effects of objective health (Idler & Benyamini, 1997). Parallel analyses comparing the two health variables yielded indistinguishable results. 3
Results of the hierarchical regression analysis appear as Table 2. Step 1 regression of depression onto race, sex, age, and education yielded a significant effect driven largely by education, with marginal contributions of sex and race. Step 2 addition of joint count and perceived health significantly increased variance explained due to the strong significant association of perceived health with depressive symptoms. This also intensified effects of race on depression, yielding a significant coefficient for that variable. Pain and disability were entered at Step 3, again significantly improving prediction of depression. Pain, but not disability, was significantly associated with depression.
Hierarchical Regression Predicting Depressive Symptoms as a Function of Demographic, Arthritis History, General Health, Pain, and Disability
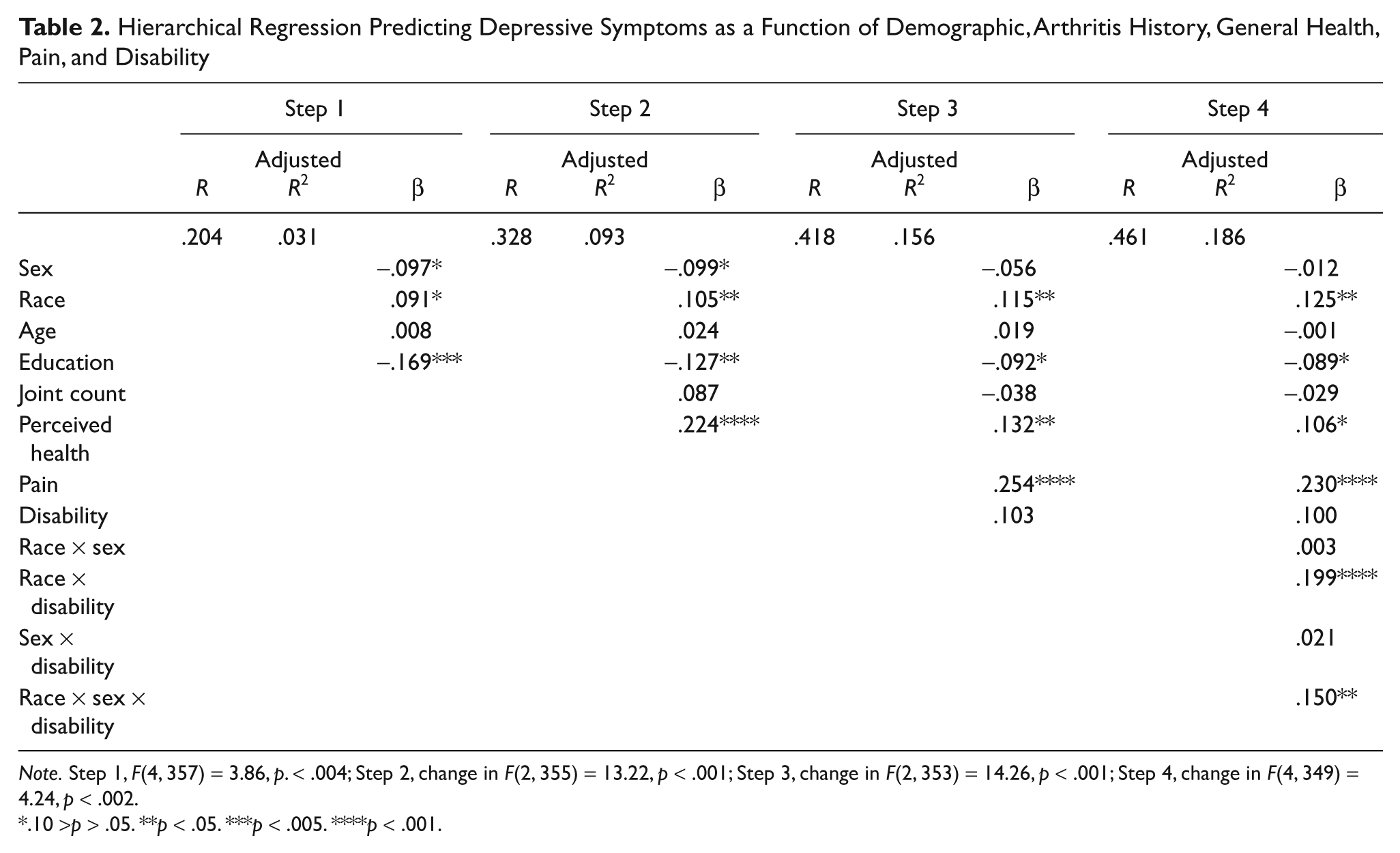
Note. Step 1, F(4, 357) = 3.86, p. < .004; Step 2, change in F(2, 355) = 13.22, p < .001; Step 3, change in F(2, 353) = 14.26, p < .001; Step 4, change in F(4, 349) = 4.24, p < .002.
.10 >p > .05. **p < .05. ***p < .005. ****p < .001.
Interactions Among Race, Sex, Pain, and Disability
To determine how race and sex influence associations of pain and disability with depression, we computed interaction terms by centering all variables and then computing cross-products. Because of the strong collinearity of pain and disability noted earlier, we ran the Step 4 analysis separately for the pain and disability interaction terms. For each, we added to the Step 3 model interactions of sex and race, sex and disability/pain, race and disability (or pain), and the three-way interaction of sex, race, and disability/pain.
For pain, the overall change in F was not significant, ΔF(4, 349) = 1.63, p > .10. For disability, however, a significant overall effect (Table 2, Step 4) was driven by the interaction of race with disability and the three-way interaction of race, sex, and disability.
We explored the Race × Disability interaction by replicating the regression separately for Blacks and Whites. Whereas Whites displayed a positive association of disability with depression, β =.238, F = 9.69, p < .002, Blacks showed an opposite trend, β = -.253, F = 5.53, p > .052. When covariates (age, education, joint count, perceived health) and pain are removed from the equation, the positive effect among Whites is exacerbated, β = .370 (vs. .202 originally), F = 41.04, p < .001. Among Blacks, however, the negative depression–disability linkage is attenuated, β = .086, F < 1.
Figure 1 depicts the Race × Sex × Disability effect as presented in Table 2. Separate regressions for men and women yielded comparable main effects of race (β = .124 for women, .118 for men) and disability (.078 and .105), both zs for difference between b coefficients < 1. However, the Race × Disability interaction was quite strong in men, β = .309, F = 15.22, p < .001, but not in women, β = .052, F < 1, z for difference between b coefficients = 3.09, p < .001. Reanalyses omitting controls for age, education, joint count, perceived health, and pain are presented in Figure 2. The triple interaction was unchanged, men’s Race × Disability β = .372, F = 23.04, p < .001, women’s β = .032, F < 1, z = 2.53, p < .006.
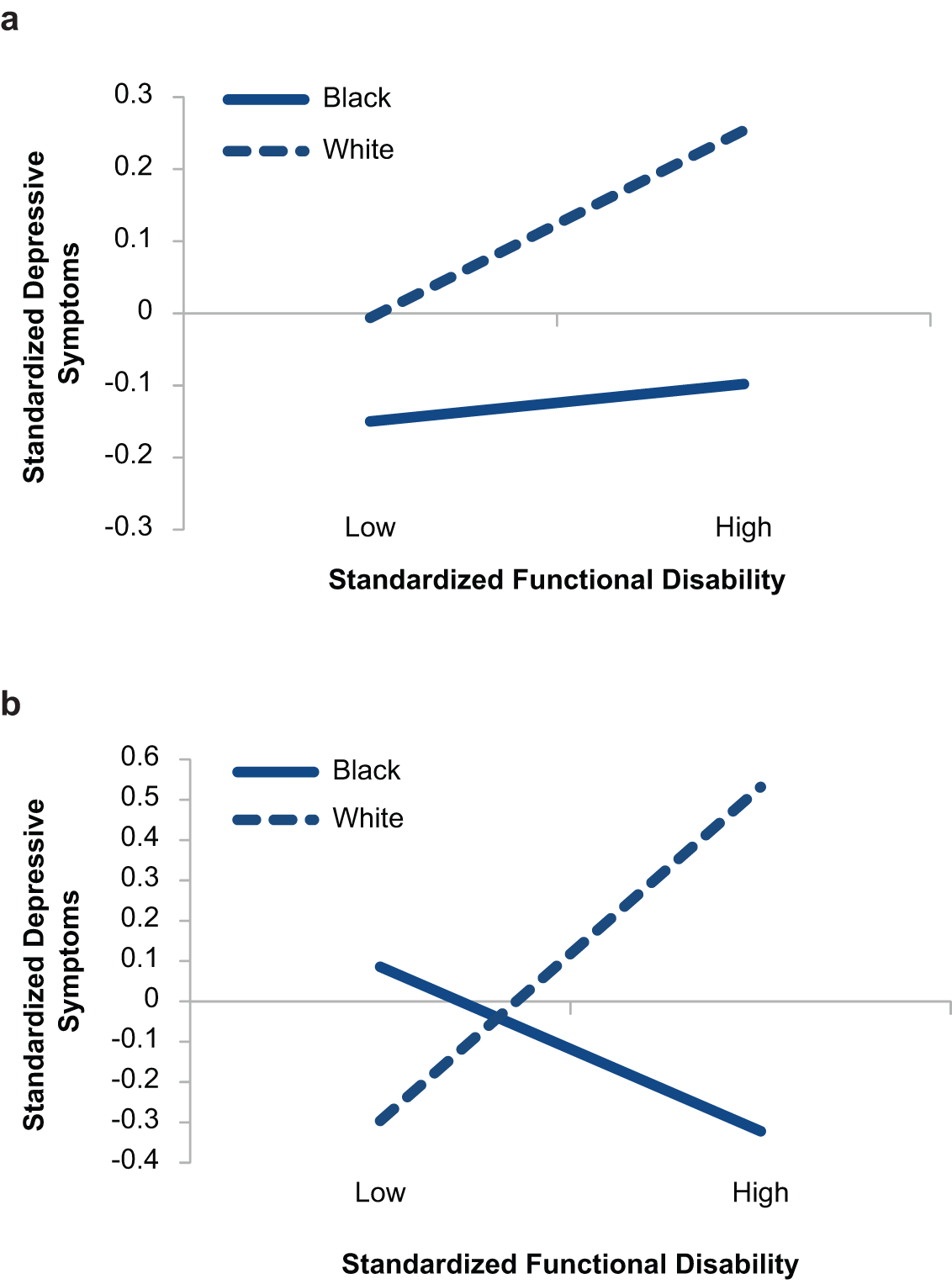
Interaction of race, sex, and functional disability on depressive symptoms, adjusted for covariates: (a) Women, adjusted for covariates; (b) Men, adjusted for covariates

Interaction of race, sex, and functional disability on depressive symptoms, unadjusted: (a) Women, unadjusted; (b) Men, unadjusted
Raw correlations (Table 3) further illustrate this effect. Whereas Black men displayed virtually no association of depression with pain or disability, correlations for White men were moderate to strong; women of both races were intermediate. In contrast, there were no group differences in the association of pain with disability.
Intercorrelations Among Key Study Variables as a Function of Race and Sex
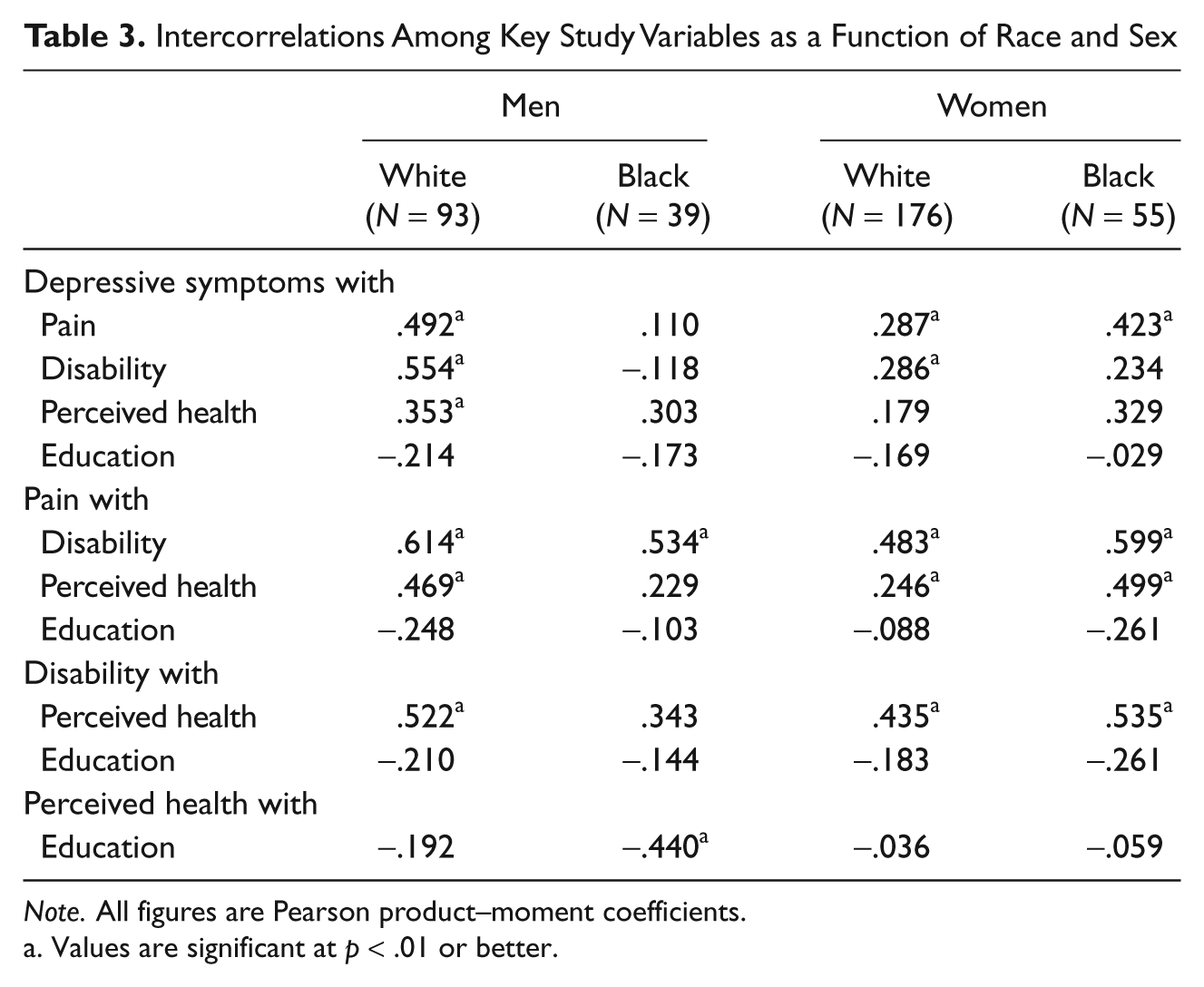
Note. All figures are Pearson product–moment coefficients.
Values are significant at p < .01 or better.
Discussion
Although our hypotheses were only partly confirmed, these data yield some intriguing insights into the effects of sex and race on older OA sufferers’ affective reactions to pain and disability. As predicted, women in our sample reported greater pain than did men. A parallel, marginally significant effect for disability was intensified by control for demographic, arthritis, and health status variables. Interestingly, however, we observed no sex differences in depressive symptoms. Black respondents reported significantly greater disability and marginally greater pain than their White counterparts. These effects, however, washed out when controlled for age, education, joint count, and perceived and objective health. As with sex, we found no evidence that depression is more prevalent among Blacks than Whites. A marginal effect did emerge when covariates were introduced, representing slight reduction of depressive symptoms among Blacks but not Whites.
Obtained sex differences in pain and disability are not particularly surprising as they conform to previous research (Axford et al., 2008; Fillingim et al., 2009; Keefe et al., 2000; Stubbs et al., 2010). Our data are also consonant with the bulk of existing evidence indicating that there are minimal differences in prevalence of depression between Blacks and Whites (Kessler et al., 2003). In contrast, our failure to confirm established findings regarding women’s greater depression (Weissman & Klerman, 1977) is somewhat puzzling. White women did report somewhat greater depression than White men, but the effect was not statistically significant. However, the much less pronounced difference between Black men and women confirms previous work on the epidemiology of depression in that ethnic group (Brown, Ahmed, Gary, & Milburn, 1995). Further work with larger samples of African Americans is needed to explore possible moderating effects of race and sex on depressive symptomatology. Of course, it is equally important to continue exploring measurement equivalence of standard approaches to assessing depressive symptoms across different ethnic groups (Kim, Chiriboga, & Jang, 2009).
It is difficult to compare these results to existing research because, net of a few studies (Affleck et al., 1999; Keefe et al., 2000), there has been relatively little work done specifically on sex and race differences in OA-related pain, disability, and affective distress. Functional disability is known to increase risk of depression in men as well as women (Bruce, Seeman, Merrill, & Blazer, 1994), but it is doubtful that the effect would eliminate sex differences that are well established in the general population. It is more likely that, by recruiting at a VA rheumatology clinic, we oversampled male OA treatment seekers versus a greater proportion of female general geriatric clinic patients for whom OA may not have been a primary concern. In other words, our sample of men may have been skewed, if not toward more severe arthritis symptoms, at least toward greater perceived need for treatment and concomitant affective distress. It is thus important that future work explore those associations in large sample studies drawing male and female, Black and White participants from the same sites and sources.
By far, the most intriguing results of this study are the interactive influences of race, sex, and disability on depressive symptoms. We had hypothesized that both race and sex would exacerbate the impact of pain and disability on emotional well-being, placing Black women at particularly high risk of depression consequent to OA-related pain and disability. In fact, however, after adjustment for covariates, Blacks displayed lower levels of depressed affect at higher levels of disability. The significant three-way interaction indicated further that this effect was driven by Black men, for whom there was virtually no raw correlation of disability with depression (r = -.118 vs. .554 for White males), and a negative association after taking into account education, perceived health, and pain. In contrast, Black and White women displayed similar raw and adjusted slopes, the primary difference being White women’s overall slightly greater depression.
It is also notable that disability, but not pain, interacted with sex and race to influence (or be influenced by) depression. To be sure, pain bore a significant independent association with depression—in fact, a stronger one than disability. However, the relationship of pain to depression appears to be uniform for men and women of both races. The affective concomitants of functional disability, however, appear to be somewhat blunted for African Americans generally and particularly for Black men.
This effect is particularly striking, given the fact that Black men were in generally poorer health than others in our sample, reporting significantly more OA-affected joints, more general health problems, and poorer perceived health. Logically, this should predispose them to greater rather than less emotional distress. It may be that effects of health were buffered by stronger coping strategies or pain-related cognitions; it is also possible that our older Black men were simply more reluctant than others to acknowledge symptoms of depression. An interesting third possibility is that differential work roles may play a part, especially in this cohort of older persons. Our Black men, less well educated than their White counterparts, likely also worked at lower paying, physically more demanding jobs. For these men, disability may have heralded release from physically stressful job demands and, consequently, have positive as well as negative emotional implications.
Of course, all these explanations are, at this point, speculative. Cautious interpretation is recommended due to several limitations of this research. Foremost are sampling concerns, particularly the relatively small number of Blacks and men in the sample. Although obtained effects are statistically quite robust, confirmation in larger and less select samples is needed to confirm this pattern. It is also difficult in the current study to disentangle effects of race and sex from those of recruitment site. The majority of men in the study were enrolled through a VAMC clinic; women were more likely to have been contacted through primary care or rheumatology clinics. Similarly, outpatient clinic and PSA respondents were more likely than other groups to be White. Our diverse sampling strategy was designed precisely to avoid possible biases due to reliance on specialty clinic enrollment; however, that very diversity introduces questions this study cannot answer due to demographic differences in service utilization at clinical recruitment sites. Importantly, however, there were no differences within sites in proportions of Black and White men and women, lending some credence to the overall pattern of findings. For example, although VA clinic referrals were overwhelmingly male, they comprised equal proportions of Blacks and Whites. Hence, differential patterns of associations between disability and depression for Black and White men cannot be explained purely on the basis of recruitment site.
Another limitation of this research is its cross-sectional nature, which precludes exploration of how observed difference developed and how pain, disability, and depression interact over time. As this literature develops, it will be important to conduct longitudinal analyses that will permit some explication of the (likely reciprocal) causal associations among these variables and how they may differ as a function of race and sex.
Despite these limitations, our findings regarding interactive effects of race and sex on the association of disability with depression are intriguing. Further research is clearly needed to replicate these effects and explore factors that may be driving them. Such work is especially important given the clinical implications of the current work and its various interpretations. For example, if findings represent a true (relative) invulnerability of Black men to the affective concomitants of OA pain and disability, closer study of that group may help identify ways to improve resilience of other groups. If, however, we are observing denial or minimization of symptoms and their effects, very different strategies will be needed effectively to reach this group of OA sufferers.
In sum, the current data offer confirmation, albeit somewhat weak, of previous findings regarding sex differences in the pain–disability–depression dynamic. This work perhaps does more to fuel than to resolve ongoing questions about racial/ethnic differences in these processes, but it does raise intriguing possibilities for future research. In particular, more intensive work is needed with African American men—a previously understudied group—to elucidate their unique experience and expression of this very common age-related disorder.
Footnotes
Acknowledgements
The authors thank Lori Smith for project management, James Hollander, Meredith Olderman, and Beth Chmar for collecting the data as well as Elaine Benoff, Susan Gallagher, Hui Wu, Yunqi Zhang, and others who assisted with the project.
An earlier version of these analyses was presented at the 2009 scientific meeting of the Gerontological Society of America.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Institute of Mental Health Grant 1-R01-MH51800 to the first author for research conducted at the Philadelphia Geriatric Center and the University of Pennsylvania.