
Abstract
Introduction
The combined impact of increasing life expectancy (LE) and declining fertility has brought the issue of population aging to the fore, all over the world. Globally, the elderly population is growing quickly, in both percentage and absolute numbers relative to the younger population. Populations are aging in developing countries faster than in the developed world (United Nations, 2009). Asia, Latin America, and the Caribbean are the world’s fastest aging regions, with the percentage of elderly in both regions projected to double between 2000 and 2030 (Kaneda, 2006; United Nations, 2009). Bangladesh is no exception to this; due attention should therefore be placed on the elderly as well as on elderly-oriented research in Bangladesh.
As people live longer, quality of life becomes a central issue (Liu, Chen, Song, Chi, & Zheng, 2009), and recognition of the growing impact of population aging has added the need for Disability-free Life Expectancy (DFLE) measures in particular and health expectancy measures in general (Bone, Bebbington, & Nicolaas, 1998; Robine, Romieu, & Cambois, 1997). Health expectancy measures have been developed to add a quality-of-life dimension to length of life (Sanders, 1964). They are very useful in monitoring the health status of the population (Saito, Qiao, & Jitapunkul, 2003; Stiefel, Perla, & Zell, 2010) and should be linked to policy making in the new era (Saito et al., 2003). Among the elderly in Bangladesh, however, very little is known about gender differences in disability and DFLE.
Gender differences in health and mortality have been of longstanding interest to researchers, and a number of studies have been devoted to this topic (Doblhammer & Hoffmann, 2010; Oksuzyan, Juel, Vaupel, & Christensen, 2008). Gender differences in disability and DFLE are also areas of interest, particularly in Bangladesh, where women are highly disadvantaged compared with men. In Bangladesh, there have been fluctuations in male and female LE at age 60; for example, in 1975, male LE at age 60 was 10.83 years, shorter than female LE at age 60 (female: 11.46). But in 1980, male LE at age 60 was 17.30 years, longer than female LE at age 60 (female: 16.40). However, since 1985, female LE at age 60 has been consistently longer than that of males (see Human Life-Table Database [HLD], 2013). In 2010, female and male LEs were 17.95 and 16.87 years, respectively (see Bangladesh Bureau of Statistics [BBS], 2011b). Whether greater LE implies better health and longer healthy life expectancy for elderly females is a critical question in Bangladesh.
Previous studies have demonstrated that although women live longer, they are more likely to report worse health, and to have a higher prevalence and incidence of disability, lower mobility, and decreased strength than men at old age (Case & Paxson, 2005; Drumond Andrade, Guevara, Lebrão, de Oliveira Duarte, & Santos, 2011; Oman, Reed, & Ferrara, 1999). In the United States, older women have been found to incur disabilities at earlier ages and experience higher incidence rates of impairment with longer retention rates of impairment compared with older men (Dunlop, Hughes, & Manheim, 1997). Older Bangladeshi women have also been found to have more limitations than men in self-reported activities of daily living and observed physical performance (Rahman & Liu, 2000). Although in terms of the number of expected years of remaining life, studies on health expectancy in several countries have shown that women can expect to live longer than men, with and without disability (Camargos, Machado, & Rodrigues, 2007; Jitapunkul, Kunanusont, Phoolcharoen, Suriyawongpaisal, & Ebrahim, 2003), in terms of proportion, women live a greater proportion of their later years with a disability than do men (Camargos et al., 2007; Crimmins & Saito, 2001; Jitapunkul et al., 2003; Reyes-Beaman et al., 2005). The current study, therefore, attempts to examine the gender differences in disability and DFLE for older Bangladeshi adults. To our knowledge, this is the first study of DFLE that attempts to estimate DFLE for the whole of Bangladesh.
Materials and Method
Data
This study uses data from a large nationally representative sample survey, Bangladesh’s Household Income and Expenditure Survey (HIES)-2010, collected by the BBS, the only national statistical institution responsible for collecting, compiling, and disseminating statistical data on all sectors of the Bangladesh economy. The objectives, sampling design, and methodologies of HIES-2010 are described elsewhere in detail (BBS, 2011a). In brief, HIES-2010 provides valuable data on household income, expenditure, consumption, savings, housing conditions, as well as individual-level data on education, employment, health, disability, and so on. A two-stage stratified random sampling technique was used in drawing the sample for HIES-2010. Interviewers entered all information collected during interviews into their laptops at the end of each day. If they noticed any inconsistency in the data, they went back to the relevant households and made the required changes to remove the discrepancy (BBS, 2011a). Consequently, for the variables we used, there are no missing values in the dataset. Data collection was completed in 1 year (February 1, 2010, to January 31, 2011). In all, 12,240 households were selected, with 7,840 from rural areas and 4,400 from urban areas. All individuals from selected households were interviewed, for a total of 55,580 individuals. Of these, 27,533 (49.54%) were male and the rest were female. Our analyses were focused at the individual level, and we restricted our sample only to those who were 60 years of age and above. Our sample, thus, consisted of 4,189 elderly men and women; 2,149 (51.30%) were men and the rest were women.
Measures
Disability
Information on six types of disabilities was collected through the disability module in HIES-2010. These were (a) vision; (b) hearing; (c) walking and climbing; (d) difficulty in remembering and concentrating; (e) self-care; and (f) speaking and communicating. To assess these disabilities, every member of the household was asked the following questions: (a) Does (name) have difficulty seeing, even if he or she is wearing glasses? (b) Does (name) have difficulty hearing, even if he/ or she is wearing a hearing aid? (c) Does (name) have difficulty walking or climbing steps? (d) Does (name) have difficulty remembering or concentrating? (e) Does (name) have difficulty with self-care, such as washing all over or dressing, feeding, or toilet chores? and (f) Does (name) have difficulty communicating, for example, understanding or being understood? Each question has four response categories: (a) no difficulty, (b) yes, some difficulty, (c) yes, severe difficulty, or (d) yes, can’t see/hear/walk/remember/self-care/communicate at all. We categorized having each disability into two groups as no (no difficulty) and yes (yes, some difficulty/yes, severe difficulty/yes, can’t see, hear, walk, remember, self-care, communicate at all). Finally, to obtain the disability prevalence, that is, at least one disability, we combined the six categories of disability into one measure, where individuals with at least one of the six disabilities were considered disabled.
Estimation of DFLE
The Sullivan (1971) method was used to compute DFLE. It partitions total life expectancy into disabled and disability-free LE based on the prevalence of the disability within a representative sample at a single point in time. To compute the DFLE in 2010, we obtained age-specific mortality information from the standard period life table of 2010 and the proportion of the population with disability from the cross-sectional survey for the year 2010. Age- and sex-specific standard period life tables for the year 2010 were obtained from BBS (BBS, 2011b). The data on disability prevalence by age came from HIES-2010. By combining the published life tables and disability prevalence rates, we estimated DFLE for our study population. For more details on computation of DFLE and confidence intervals using the Sullivan method, see Jagger, Cox, Le Roy, and EHEMU (2006).
Analysis plan
After a description of the study sample by sex and age group, we analyzed prevalence of disability by sex. We used STATA/SE 12.1 (StataCorp LP, College Station, Texas, United States of America) to perform a two-sided test for equality of proportions in disabilities. Estimates of DFLE are then obtained using the Sullivan (1971) method. Finally, as an intuitive step, the estimates of DFLE and disabled LE (DLE) are plotted in graph form. No sampling weights are provided by HIES-2010, and we did not apply sampling weights in any estimation procedure.
Results
Table 1 shows the sample population by sex and age group. The mean age of the elderly was 69 years, which is similar for both males and females. The percentage distribution of the sample population across age groups is also similar for both males and females.
Sample Population by Sex and Age Group.

Note. The figures are sample proportions that do not take into account sampling weights. M = mean; CI = confidence interval.
Gender Differences in Disability
Table 2 shows gender differences in disability prevalence. For elderly Bangladeshis, difficulties with eyesight were reported in higher percentages, followed by difficulties with walking and climbing, hearing, remembering and concentrating, self-care, and speaking and communicating. Elderly females reported each of the difficulties and at least one disability in higher percentages compared with males. Between elderly males and females, the percentage differences in each difficulty as well as in at least one disability are found to be statistically significant. It can easily be said that elderly females were more likely to have each difficulty or at least one disability than elderly males.
Percentage of Elderly Having Each Disability by Sex, and At Least One Disability by Sex and Age Group in Bangladesh.
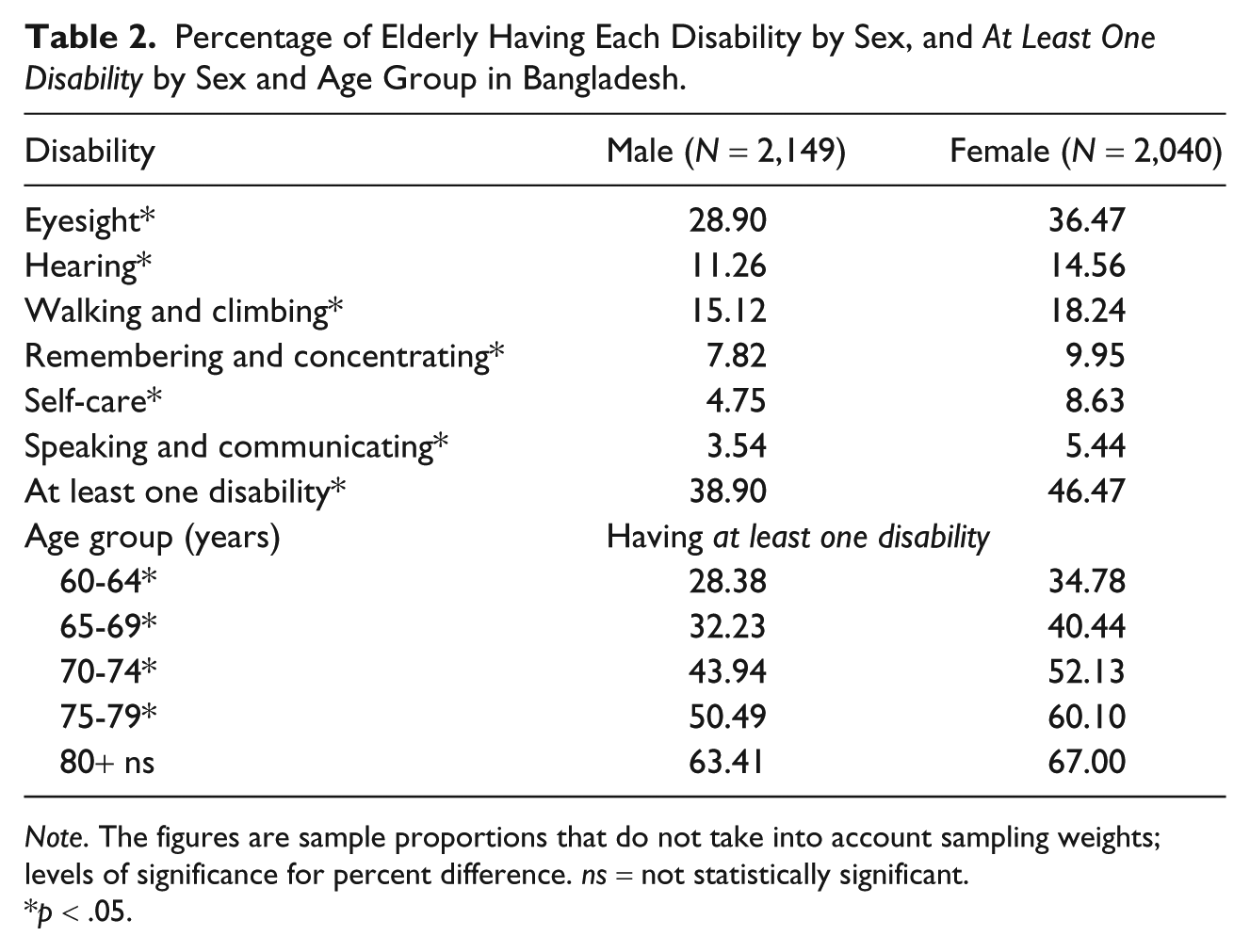
Note. The figures are sample proportions that do not take into account sampling weights; levels of significance for percent difference. ns = not statistically significant.
p < .05.
Having at least one disability by age group gives us an idea of which age group has a higher prevalence of disabilities. And it is obvious that older individuals have a higher possibility of getting at least one disability than their younger counterparts. The current study also reveals that the percentage with at least one disability increases with increasing age. Between elderly males and females, the percentage differences in having at least one disability are found to be statistically significant across all age groups except the 80+ years age group. In other words, across all age groups, elderly females have at least one disability in significantly higher percentages than do elderly males. The prevalence rates of having at least one disability for elderly males and females over 80 years old are about twice as those of individuals who are 60 to 64 years of age. Although females have higher prevalence levels than males, males have a much higher rate of increase in disability prevalence by age. For instance, the prevalence of having at least one disability is 2.23 times higher among males aged 80+ years than among those aged 60 to 64 years, whereas among females this ratio is only 1.93.
Sex Differences in LE and DFLE
Table 3 presents LE and DFLE, proportion of expected life without disability, and the sex difference in DFLE by age for elderly Bangladeshis in 2010. Women live longer than men; at each age they have a longer LE compared with men. Elderly females at age 60 could expect to live 17.95 years, which is 1.08 years longer than males. The difference in LE between elderly males and females decreases as age increases. At age 80+, elderly females could expect to live about 4 months longer than males of the same age.
Life Expectancy, Disability-Free Life Expectancy, and Proportion of Expected Life Without Disability by Age and Sex in Bangladesh, 2010.
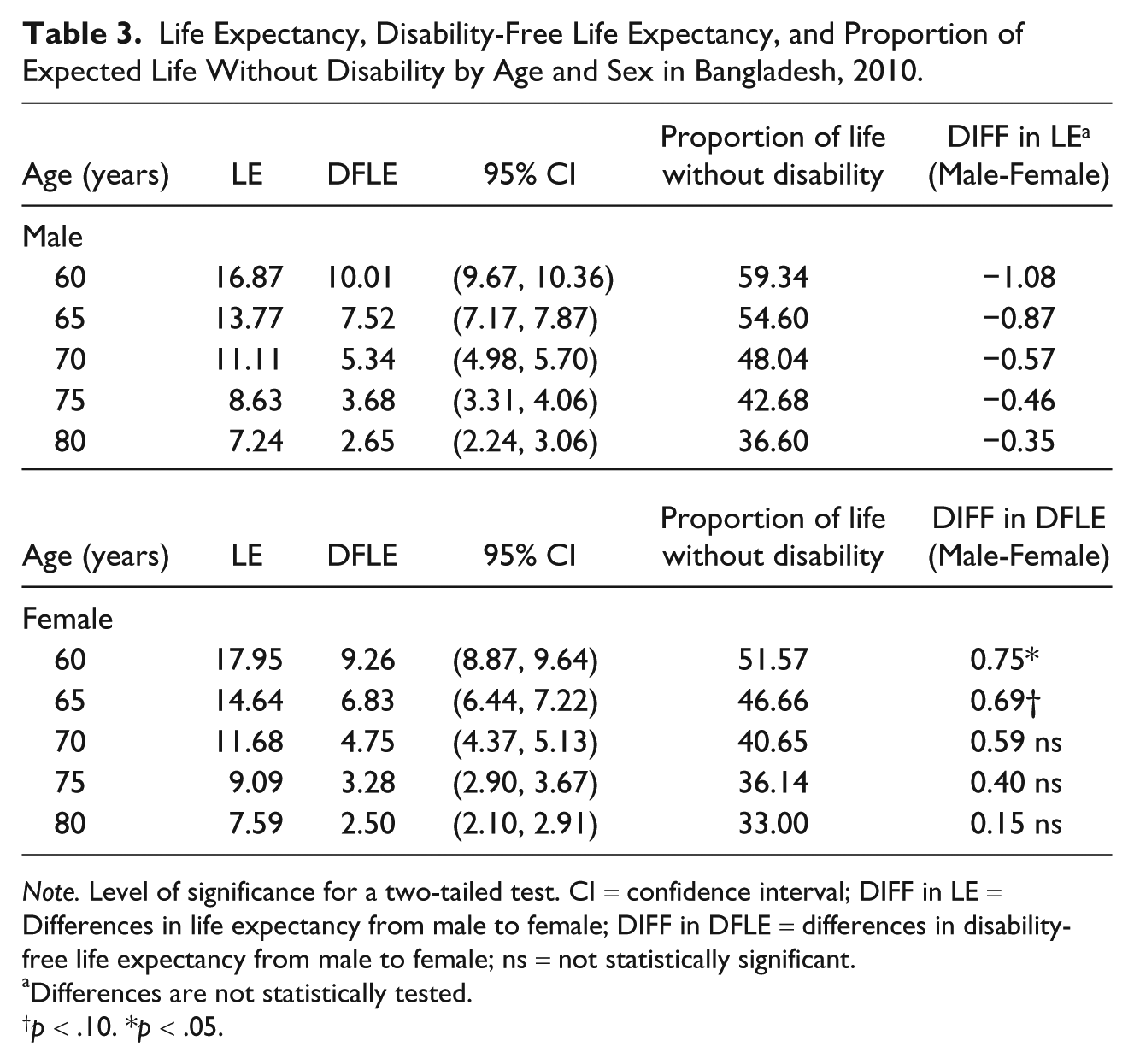
Note. Level of significance for a two-tailed test. CI = confidence interval; DIFF in LE = Differences in life expectancy from male to female; DIFF in DFLE = differences in disability-free life expectancy from male to female; ns = not statistically significant.
Differences are not statistically tested.
p < .10. *p < .05.
But men have longer DFLE than women. The positive differences between male and female DFLE are statistically significant at ages 60 and 65. At later ages as well, men have longer DFLE than their female counterparts, but these differences are not statistically significant at standard p values. Although women at age 60 have 1.08 years longer LE than men at 60 years, their DFLE is 9 months shorter than that of men. And the differences between male and female DFLE range from about 9 months to 2 months for ages 60 to 80+ years.
Proportionally, LE without disability decreases as age increases. Most interestingly, despite higher LE, women spend a smaller proportion of their life without disability compared with men. It is also clear from Figure 1 that women have a longer LE but a shorter DFLE in numbers and proportion than do men. Women and men expect about 48% and 41% of their life in a disabled state at age 60. Men and women, 70 years old and above, can expect more than half of their expected life with disability. And at age 80+, LE with disability for both sexes is between 63% and 67%, which means only about 33% to 37% of their expected life, on average, is disability-free.
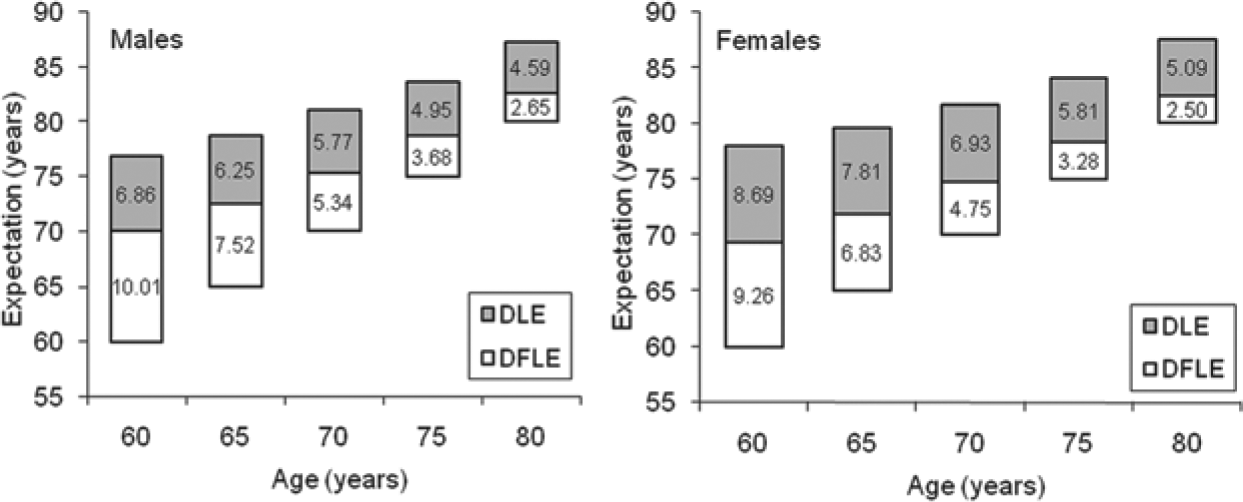
DFLE and DLE by age in Bangladesh.
Discussion
Disability among the elderly is an important public health concern (Liu et al., 2009). The incidence and development of disability has a negative impact on the lives of elderly individuals and those who assist these individuals with daily living activities. This situation affects thousands of people and, consequently, constitutes a public health problem in the society. An abundance of research has been conducted by developed countries on DFLE or health expectancy, whereas only a handful of literature exists on this issue for developing countries. There is no study on gender differences in DFLE that represents the whole of Bangladesh. This study examines gender differences in the prevalence of disability and DFLE among older Bangladeshi adults.
It provides notable results in terms of the prevalence of disability in old age. For example, in Bangladesh, eyesight disability has a higher prevalence than other types of disabilities. Programs aimed at reducing eyesight disabilities in old age could be given highest priority in Bangladesh because this type of disability significantly affects other routine living activities, such as walking, self-care, and communicating. Self-care ability is shown to be crucial as a health resource in older people, and it may be the decisive factor for managing daily life in their own homes (Høy, Wagner, & Hall, 2007). Reduced self-care ability is found to reduce life satisfaction in older people in different settings (Borg, Hallberg, & Blomquist, 2006). However, self-care problems are very low compared with eyesight problems among elderly Bangladeshis. Empirical data on living and care arrangements of elderly people in the country reveal dependence of older persons on their younger family members for physical and emotional care (Abedin, 2003). However, it is unclear how long the tradition of young family members taking care of the elderly in their family can continue. Because of rural poverty, many adults move in search of employment to urban areas. Women are also joining the urban work force in increasing numbers, and they have less time to take care of elderly family members than they did in the past. Therefore, policies and programs aimed at reducing disabilities in old age, particularly eyesight disabilities, are recommended as a way to greatly improve the quality of life of the elderly in Bangladesh.
The study also reveals that the number of elderly with at least one disability increases as age increases. Although women have a lower rate of increase in disability prevalence by age than men, they have each disability and at least one disability in significantly higher percentages than men; at each age group women are also found to have significantly higher percentages of at least one disability than men. In line with other research findings (Drumond Andrade et al., 2011; Rahman & Barsky, 2003), older individuals are more likely to report poor health than their younger counterparts, and women report significantly worse health than their male counterparts at each age group. In old age, women report suffering more from disability than do men. Part of the reason for this greater prevalence of disability among older women could be due to the less than adequate care and services for pregnant and delivering mothers. During their reproductive years, women probably encounter some lasting health problems, which, for cultural reasons, remain undisclosed, and subsequently, lead to frequent ailments at older ages. In addition, the lower status of women in Bangladesh means that many are deprived of basic things in life, including food, good nutrition, health care, a secure life, a respectable living, mental peace, freedom from abuse, and so on, and this may contribute to their bad health in old age. The female disadvantage in each of the disabilities in this study needs attention, and special care should be given to older women. Older women suffer from multiple disadvantages, resulting from biases on gender and widowhood, and experience ill health, social isolation, and poverty more than older men (Munsur, Tareque, & Rahman, 2010). Women, particularly widows, who are without living sons or who live alone, are considered to be particularly at risk of economic destitution, social isolation, poor health, and death (Abedin, 2003). In our study, a high percentage of elderly females were widows. There are two possible reasons for having such a large number of elderly widowed women in Bangladesh: one is the higher LE for women compared with men and the other is the difference in age between the bride and the groom at the time of marriage.
Our study is also in line with a study by Barford, Dorling, Smith, and Shaw (2006) indicating that women outlive men even in poorer countries. Bangladeshi women have longer LE but shorter DFLE in both numbers and proportion when compared with men. Although at standard p values the difference in DFLE between males and females is not significant at ages 70, 75, and 85+, the decrease in the positive difference across age groups is a strong indication that the difference is nonetheless robust. The current study also found that Bangladeshi women expect a smaller proportion of life without disability compared with men, which is also in line with findings that women spend more time in disabled states than do men (Camargos et al., 2007; Crimmins & Saito, 2001; Dunlop et al., 1997; Reyes-Beaman et al., 2005; Sauvaget, Jagger, & Arthur, 2001). At 60 years of age, women and men can expect about 48% and 41% of their LE, respectively, to be in a disabled state. But at 70 years of age and later, women and men can expect more than half of their expected life with disability. During more than half of their expected life, the elderly need help performing daily living activities, such as walking, self-care, communicating, and so on. Thus, to create a healthy aged society, the elderly, particularly those 70 years of age and over, should receive special attention.
Previous studies have found that females have longer LE and longer DFLE, but a smaller proportion of DFLE to LE (Camargos et al., 2007; Jitapunkul et al., 2003). Although varied methods and measures used in the existing literature make it difficult to compare patterns of DFLE, a study with similar methods to our study (Liu et al., 2009) reports that in 2006, in China, females had higher LE (LE at age 60: female = 20.7 years vs. male = 17.3 years) and DFLE in numbers, but proportionately lower DFLE than males (DFLE at age 60: female = 14.9 years [72.1 percent of LE] vs. male = 17.3 years [74.3 percent of LE]). Nguyen, Saito, Phan, and Nguyen (2012) report similar results for Vietnam. Females have higher LE (LE at age 60: female = 20.4 years vs. male = 18.1 years) and DFLE in numbers, but proportionately lower DFLE than males (at age 60: female = 11.4 years [55.8% of LE] vs. male = 11.1 years [61.1% of LE]). However, a very interesting finding from the current study is that females, when compared with their male counterparts, on average have longer LE but shorter DFLE and a smaller proportion of DFLE to LE. For example, females have higher LE (LE at age 60: female = 18.0 years vs. male = 16.9 years), but lower DFLE in both numbers and proportion than males (at age 60: female = 9.3 years [51.6% of LE] vs. male = 10.1 years [59.3% of LE]).
DFLE data are invaluable for predicting future needs, evaluating health programs, and identifying trends and inequalities, and planning health and social services, long-term care, and pensions. These data should get due attention in Bangladesh. DFLE by sociodemographic characteristics also provides insight about which group needs special care and attention. Because of the unavailability of life tables by sociodemographic characteristics (e.g., by education, marital status, religious groups, rural-urban), we were unable to estimate the DFLE by sociodemographic characteristics. Data collection for longitudinal aging studies is necessary in Bangladesh to provide a better understanding of DFLE and disability transitions.
Limitations
The study has a few limitations. First, the data used in the study are self-reported. Although this could be a possible source of bias, studies have shown that self-reported data on functional disability were consistent with medical diagnoses (Zunzunegui, Alvarado, Béland, & Vissandjee, 2009). Second, the survey (HIES-2010) mentions nothing about proxy interviews; in cases where elderly people were unable to respond to the interviews, some proxy respondents may have been interviewed. Third, the data do not provide any weights for individuals to account for the complex sampling design. This could be a source of bias for the representativeness of the sample by urban-rural areas. And fourth, the institutionalized population was not taken into account due to unavailability of data. If individuals living in institutions have more disabilities than individuals residing in the community, not taking into account the institutionalized population might overestimate the DFLE, especially at older ages (Yong & Saito, 2009). Here, we assume the number of elderly people living in institutions is negligible and that they exhibit the same distribution of health conditions and disabilities as the elderly living in the community at large. Notwithstanding these limitations, the most recent and reliable nationally representative data give a clear picture of gender differences in disability and DFLE for older adults in Bangladesh. Addressing these limitations in future research is vital for a clearer scenario for elderly Bangladeshis and DFLE.
Conclusion
The findings of the current study have important implications for risk of disability and the need for, and use of, long-term care services. Eyesight disability is the main disability in old age and one that is preventable by providing eyeglasses, facilitating the availability of affordable and high quality cataract surgical services, providing affordable pricing, making surgical supplies available, and so on. Women have higher percentages of disabilities and lower DFLE compared with men. At age 70 and above, both men and women can expect more than half of their expected life with disability. Thus, the elderly should receive due attention, and special care should be given to women. The knowledge that disabilities faced by older persons are the result of a number of past life-time experiences related to education, health care, housing conditions, hygiene practices, and so on can serve as a guide for public policies in the country.
Footnotes
Authors’ Note
Md. Ismail Tareque originated the study and contributed to the study design, statistical analysis, and the writing of the article. Sharifa Begum contributed to the conception and design of the study, and helped access and analyze the data. Yasuhiko Saito participated in the conception and design of the study, helped analyze data, and critically revised the article. All authors were involved in the development of the manuscript and approved the final version. As the de-identified data for this study came from secondary sources, this study does not require ethical approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and /or publication of this article.