
Abstract
Cognitive test performance is subject to a wide range of influences including demographic factors, health conditions, and mood. A complete accounting of cognitive performance requires knowledge of the interrelation of these factors. Demographic factors such as age, education, and gender have been well studied. For the most part, better scores on tests of new learning, problem solving, and psychomotor speed are seen among younger and better educated subjects (Samuels & Podbros, 1988; van Gorp, 1990). Women have slight advantages on some verbal memory tests (Van der Elst, Van Boxtel, Van Breukelen, & Jolles, 2005), while men have small advantages on some spatial processing tasks (Wiederholt et al., 1993). Race is a surrogate for many factors including disparities in education (Manly et al., 1998) and health (Schwartz et al., 2004). Years of education may be an inadequate measure of educational experience in multicultural elders (Manly, 2002), suggesting an interaction between race and education that may further complicate our understanding of the influence of these factors on cognitive performance. Finally, the deleterious influence of certain illness and medical disorders on cognitive performance is clearest when the pathology directly involves the brain (e.g., stroke and dementia). However, when illness or disease does not directly affect the brain, the influence on cognition may be less clear-cut (e.g., lung and cardiac disease).
A few studies have attempted to examine the independent role of these factors in cognition. The Health and Retirement Study (Masel & Peek, 2009) offered an opportunity to look at the role of several demographic factors (age, gender, marital status, income level, education, working status), self-reported health conditions (stroke, heart disease, diabetes, and hypertension), body mass index (BMI), and exercise in relationship to mental status and memory (immediate and delayed recall of a word list) in a nationally representative study of 7,944 White, African American, and Hispanic adults aged 51 years and older. After adjusting for age, ethnicity, gender, income, work status, chronic illness, BMI, and physical activity, education was positively correlated with memory. Regarding ethnicity, being African American or Hispanic was associated with a lower memory score. The strength of this study is that it looked at several variables in combination, but the study is limited by its use of a general marker of cognitive status and a one-trial word list memory test.
The Asset and Health Dynamics of the Oldest-Old (AHEAD) study (Zelinski & Gilewski, 2003) examined the relationship between cognition and demographics and health in 6,663 non-institutionalized older adults. The cognitive tests included immediate and delayed memory using a word list and Mini-Mental State Examination (MMSE). Participants also completed an abbreviated Center for Epidemiologic Studies–Depression Scale (CES-D). Self-reported history of heart disease, diabetes, lung disease, or stroke was also taken. Demographic variables were most strongly related to cognitive performance, while the self-reported illnesses were only weakly related to cognition. Education had some of the largest affects across tasks. White participants performed better across cognitive tasks independent of age or education. Women performed better than men on recall but worse on a task of working memory. Depression, similar to the demographic variables, consistently predicted performance on recall and cognitive score. Stroke predicted lower performance on recall, mental status, and the overall cognitive score. The main limitation of this study was the small number of cognitive tests and the relatively few cognitive domains studied.
The Correlates of Cognitive Function in an Elderly Community Population study looked at 3,682 older community-dwelling adults in East Boston (Scherr et al., 1988). Cognition was measured with tests of immediate memory, delayed memory, attention, and orientation. They found an association between lower scores on cognitive measures and increasing age, fewer years of formal education, and less prestigious occupation; this was maintained even after adjusting for other variables (Scherr et al., 1988). They also inquired whether participants had a history of stroke or diabetes. Those with a history of stroke performed worse on tests of delayed memory and mental status than those who did not after adjusting for age and gender. A history of diabetes was not found to be related to test performance on any of the measures. Although large, this area sample is geographically homogeneous, which limits the generalizability of findings.
In this article, we examine baseline data from the ACTIVE study to determine independent affects of demographic and health factors on composite measures of memory, reasoning, and speed of processing in a large, diverse sample of older adults. Based on prior research, we expected large independent affects for age and education, smaller affects for gender, and smaller affects still for certain health conditions with direct impact on brain structure and function (e.g., stroke and depression).
Method
Design and Participants
ACTIVE is a multisite, randomized, controlled clinical trial of the effectiveness of cognitive interventions in maintaining and promoting cognitive health and daily function in older adults (see Ball et al., 2002; Jobe et al., 2001, for details). Recruitment occurred in six metropolitan areas using a variety of sampling strategies. Community-dwelling adults aged 65 years and older were eligible. Persons were excluded if they had significant cognitive dysfunction (score <23 on the MMSE; Folstein, Folstein, & McHugh, 1975); functional impairment (dependency or regular assistance in ADL on Minimum Data Set Home Care [Morris et al., 1997]); self-reported diagnoses of Alzheimer’s disease, stroke within the last 12 months, or certain cancers; current chemotherapy or radiation therapy; or poor vision, hearing, or communicative ability that would have interfered with the interventions assessments. Eligible participants (n = 2,802) were randomly assigned to one of three treatment arms (memory, reasoning, or speed training) or a no-contact control group, although group assignment is not relevant to the pretreatment baseline analyses presented in this study.
Procedures
Eligibility and demographic data (age, gender, race, and education) were gathered in telephone and in-person screening. Health history, mental status (MMSE; Folstein et al., 1975) and cognitive measures (see below) were gathered via in-person examinations in individual and small-group formats. Health history consisted of self-reported hypertension, diabetes, high cholesterol, lung disease (defined as asthma, bronchitis, or emphysema), myocardial infarction, stroke or transient ischemic attack (TIA), or cancer. Depressive symptoms were measured with a 12-item version of the CES-D, a self-report measure of depressive symptoms (Radloff, 1977). Short versions of the CES-D such as the one used in ACTIVE have been shown to have comparable factor structure, internal consistency, precision, and score distributions to the original (Kohout, Berkman, Evans, & Cornoni-Huntley, 1993; Radloff, 1977; Wolinsky et al., 2009). A cut score of 16 or more on the full length CES-D has commonly been used to identify cases of suspected clinical depression (Kohout et al., 1993). We adopted this cutoff score for our analysis aware that it will result in a slightly more stringent threshold for suspected clinical depression.
Cognitive Measures and Formation of Composites
Three tests were administered for each cognitive domain. Memory tests included the Rey Auditory Verbal Learning Test (Rey, 1941), a 15-item, five-trial word list learning test; the Hopkins Verbal Learning Test (Brandt, 1991), a 12-item, three-trial word list learning test consisting of three sets of four semantically related words; and the Rivermead Behavioral Memory Test Paragraph Recall (Wilson, Cockburn, & Baddeley, 1985), a test of prose recall of a four- to five-sentence paragraph containing 21 distinct bits of information. All tests were administered by audiotape for standardized presentation.
Reasoning was assessed with the Letter Sets (Ekstrom, French, Harman, & Derman, 1976), requiring participants to identify which set of letters out of four letter sets does not follow the pattern of letters; the Letter Series Sets (Thurstone & Thurstone, 1949), requiring participants to identify the pattern in a series of letters and circle the letter that comes next in the series; and the Word Series Test (Gonda & Schaie, 1985) that presents 5 to 15 words in a pattern with the objective of determining the next word in the series from among five choices.
Processing speed was assessed with the Useful Field of View (UFOV), a computerized measure of visual information processing speed for divided and selective attention tasks consisting of four subtests that increase in complexity (Owsley et al., 1998). There are four tasks with different levels of difficulty and the goal is for the participant to perform the task correctly 75% of the time as quickly as possible. The speed composite is composed of UFOV Tasks 2 to 4.
Composite measures of memory, reasoning, and processing speed were formed by first transforming each subject’s raw test scores into z-scores based on the baseline mean and standard deviation and then calculating the average of the z-scores’ contribution to a domain. This was designed to represent the “ability” rather than results for a single test.
Statistical Analyses
The analytic sample consisted of participants with complete baseline data for measures of interest. In addition, because of the small number, participants reporting race other than White or African American were excluded (n = 20). Therefore, the analytic sample is 2,782. Analyses were conducted using R version 2.12.0 (Team, 2010). Descriptive statistics were presented as mean ± standard deviation for continuous variables and number of subjects (percentage) for categorical variables.
Ordinary least squares (OLS) regression was used to examine bivariate associations between demographic and health variables with cognitive domain composite scores. Three multivariable models were sequentially constructed: (a) demographic characteristics, (b) race × education interaction, and (c) health conditions. The race × education interaction was carried forward into subsequent models only if statistically significant. The amount of variance explained, R2, and information criteria measures (Akaike information criterion [AIC] and Bayesian information criterion [BIC]) were used to compare the models. Cognitive domain composite scores were standardized in all regression models such that regression coefficients indicate the change in the cognitive domain composite score measured in standard deviation units. In addition, cognitive domain composite scores were coded such that higher scores indicate better performance. Model residuals were examined to assess deviation from normality and dependence with independent variables.
Results
Demographic and health characteristics of the analytic sample are displayed in Table 1. Participants had an average age of 73.6 years and were predominantly female (75.9%), with just over a quarter (26.2%) African American. Years of education ranged from 4 to 20 years with a mean of 13.5 years. Hypertension (51.2%) and high cholesterol (44.7%) were the most frequently reported health conditions with lung disease present in 14.9%, diabetes in 12.8%, heart attack in 11.1%, stroke in 7.0%, cancer in 5.6%, and suspected clinical depression in 4.8%.
Characteristics of the Study Population.
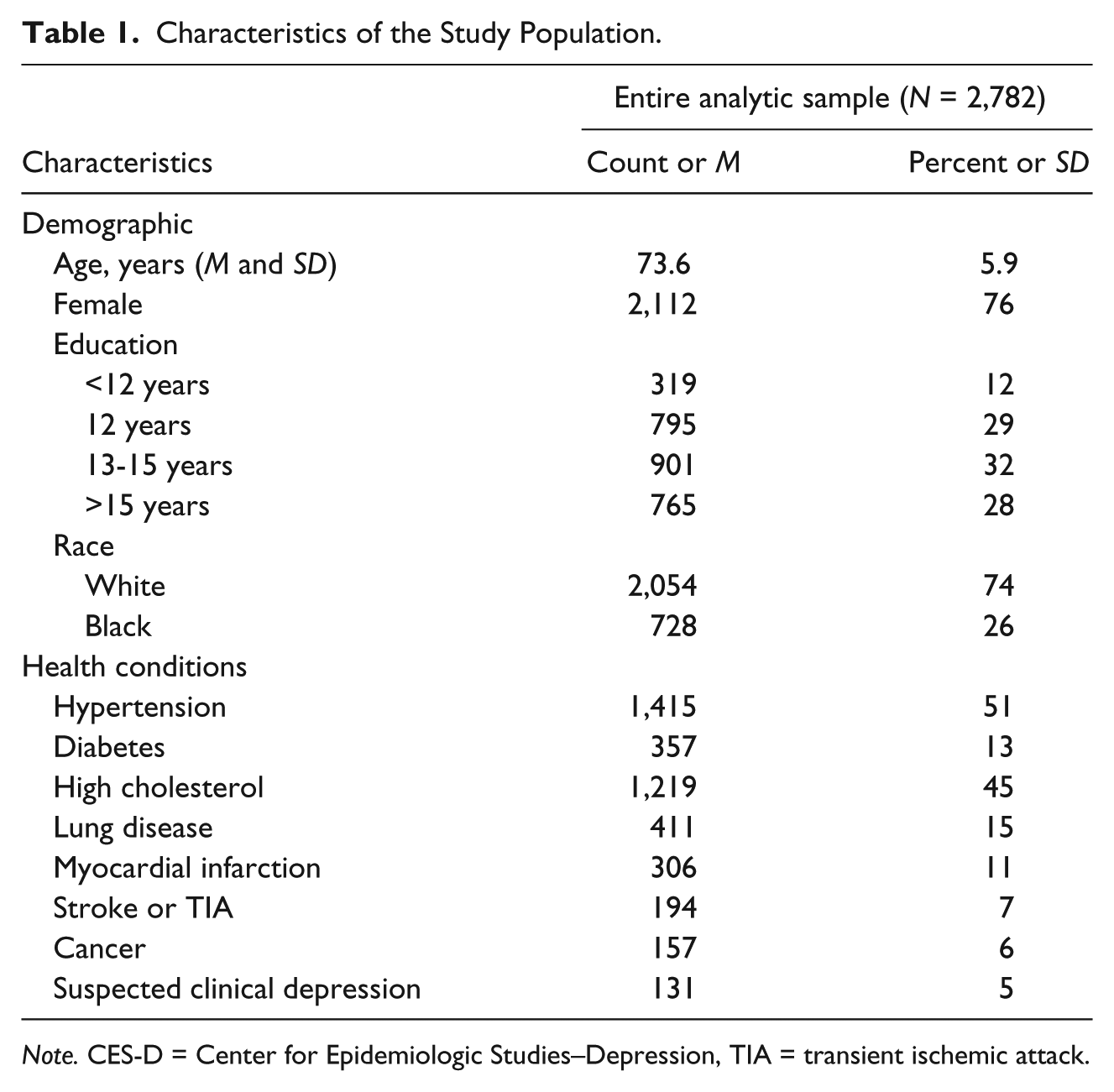
Note. CES-D = Center for Epidemiologic Studies–Depression, TIA = transient ischemic attack.
Table 2 shows model results for the memory composite. Bivariate analyses revealed that younger age, female gender, more years of education, and White race were associated with better memory performance. Presence of hypertension, diabetes, suspected clinical depression, and heart attack were all associated with poorer memory performance. The multivariable model examining demographics contingently (Model 1) showed that age, gender, education, and race were all independently associated with performance. The race × education interaction was nonsignificant (Model 2). The model examining demographics and health conditions showed that diabetes and suspected clinical depression (in addition to all demographic factors) were related to poorer memory performance (Model 3). Heart attack, which was associated with memory performance in the bivariate analysis, was no longer significant in the multivariable model. Notably, the magnitude of affect for all demographic factors was not attenuated after the inclusion of health conditions.
Models Predicting Memory Composite.
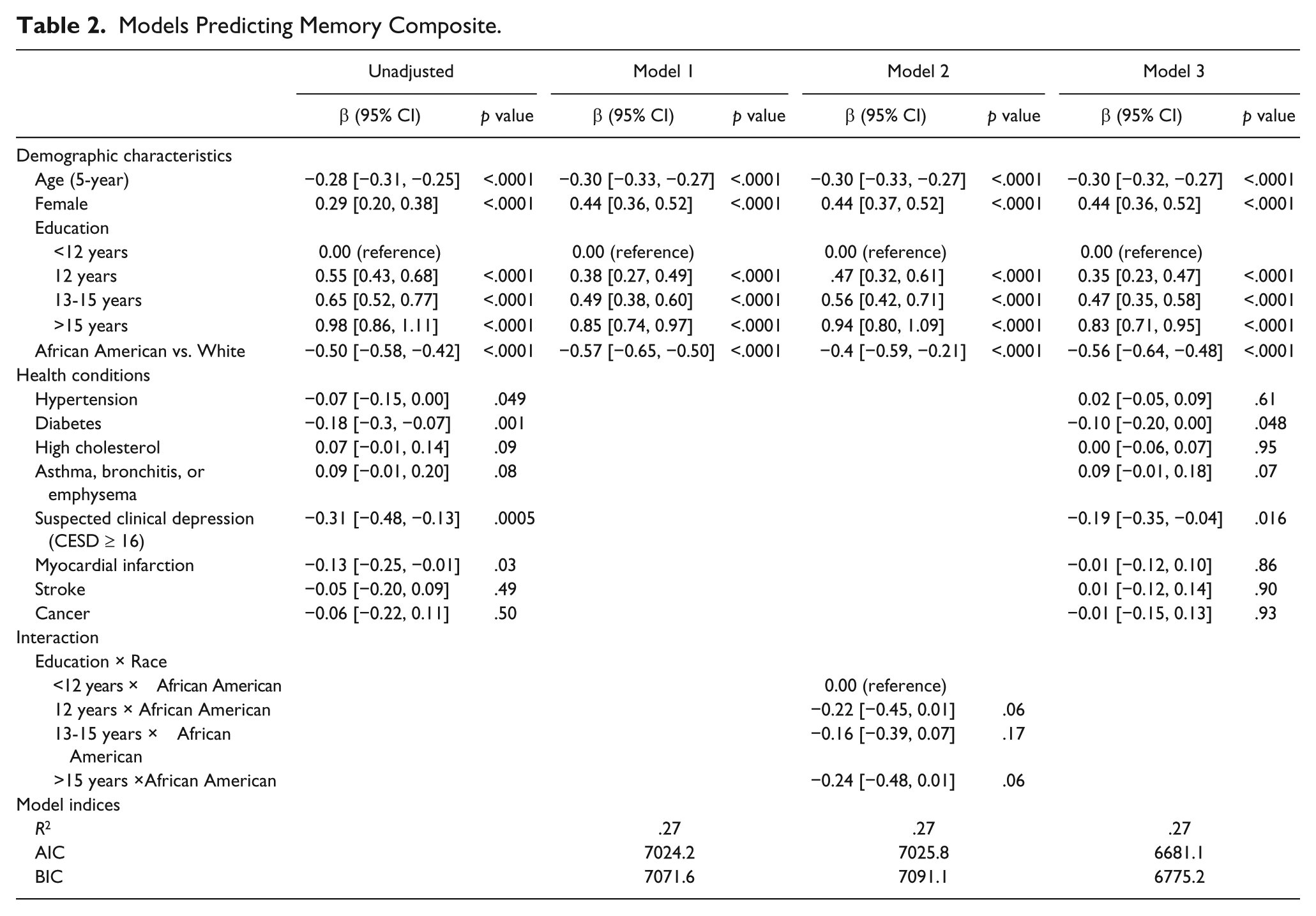
Table 3 shows model results for the reasoning composite. Bivariate analyses revealed that younger age, male gender, more years of education, and White race were associated with better reasoning performance while presence of hypertension, diabetes, suspected clinical depression, and heart attack were associated with lower performance. Model 2 revealed a significant race × education interaction such that the difference in reasoning composite scores between African Americans and Whites was slightly larger for those with the highest education level (Figure 1). However, inclusion of this interaction did not change the pattern of results in that or subsequent models. In Model 3, all demographic factors except for gender retained significance. Suspected clinical depression was the only health condition that remained significantly associated with reasoning performance after accounting for demographics.
Models Predicting Reasoning Composite.
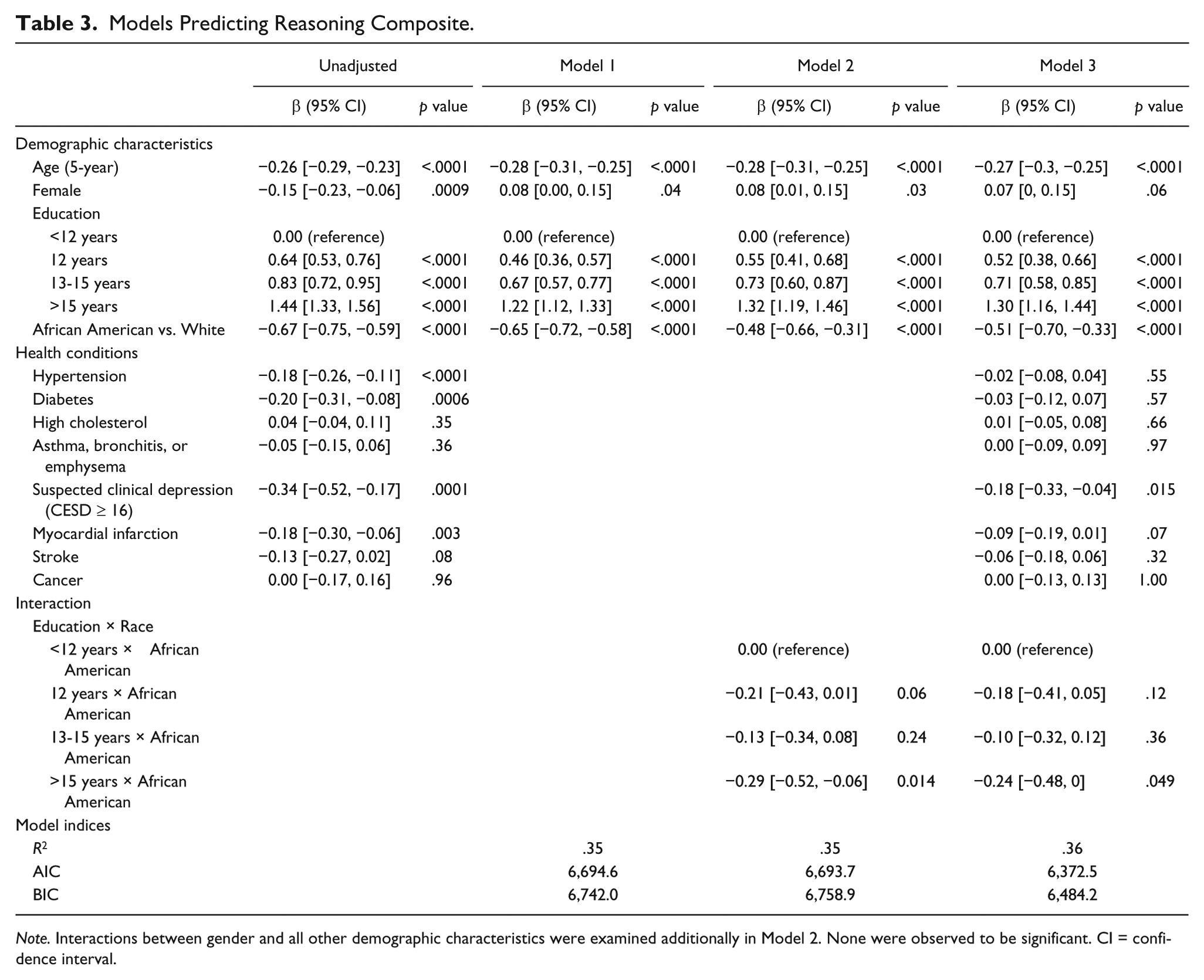
Note. Interactions between gender and all other demographic characteristics were examined additionally in Model 2. None were observed to be significant. CI = confidence interval.
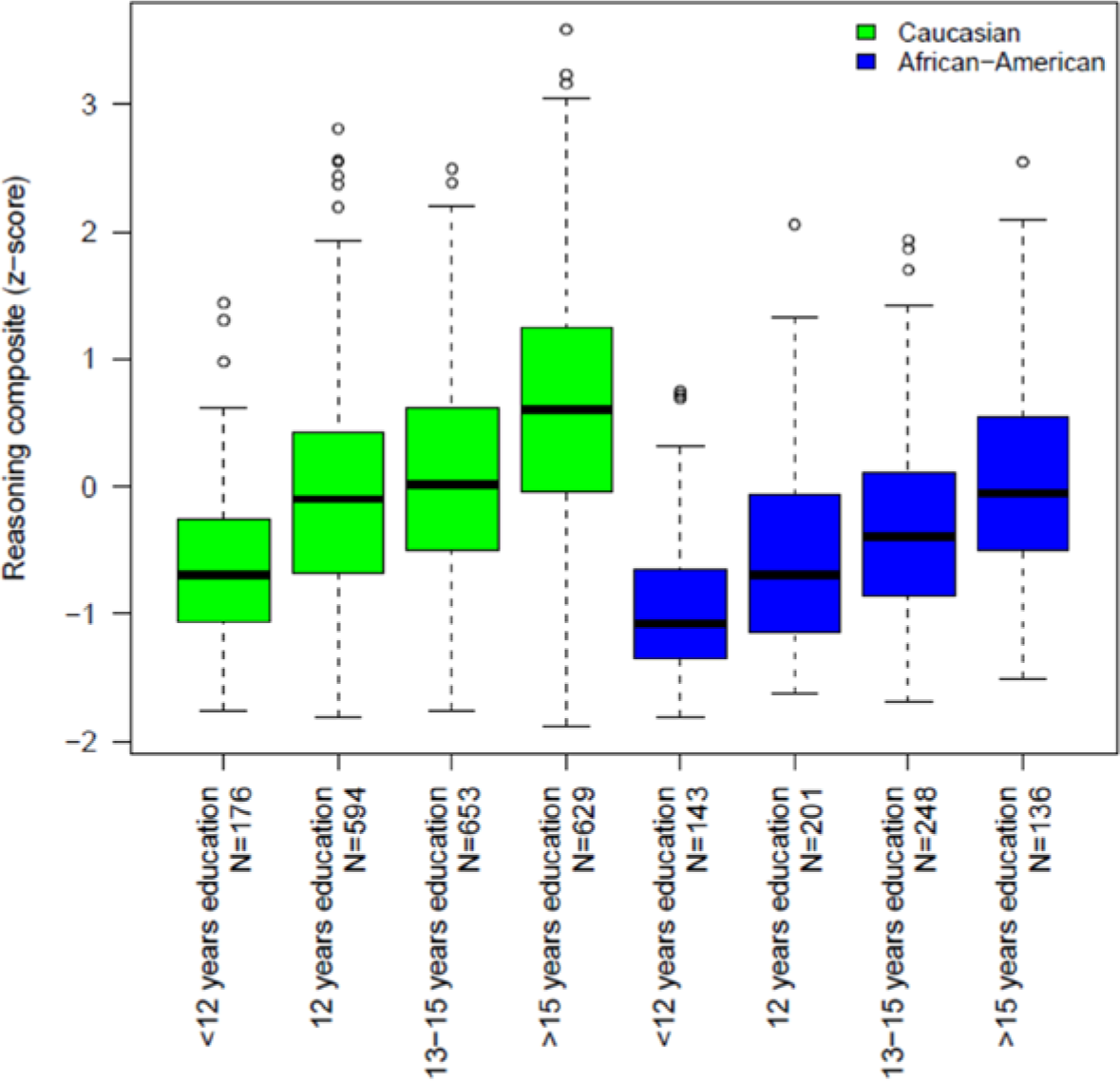
Reasoning composite by race and education.
Table 4 shows model results for the speed of processing composite. Bivariate analyses revealed that younger age, more years of education, and White race were associated with better speed performance, while presence of hypertension, diabetes, suspected clinical depression, stroke, and heart attack were associated with poorer speed performance. The multivariable model looking at all demographics simultaneously (Model 1) showed that age, education, and race, but not gender were independently and significantly associated with performance. There was no evidence of a race × education interaction (Model 2). When demographics and health conditions were considered jointly, age, education, and race remained significant among the demographic factors but only diabetes and stroke among the health conditions continued to have a significant negative influence on speed of processing performance; heart attack, which was related to poorer speed performance in the bivariate analysis, was no longer significant.
Models Predicting Speed Composite.

Note. CI = confidence interval.
Discussion
The results of these analyses partially support our hypotheses. Age, education, and race were related to performance in all the three cognitive domains, but the affects were not attenuated by health conditions. Based on prior studies, we expected to find relationships between cognitive performance and cardiovascular conditions, as well as suspected clinical depression. These relationships were detected but were not as strong as demographic characteristics. In addition, we observed variability in associated demographic characteristics and health conditions across the three cognitive domains. Younger age, more education, and White race were consistently related to better performance in all the three domains. However, gender was related only to memory performance, with females performing better than males. In terms of the health conditions considered in these analyses, suspected clinical depression was associated with poorer memory and reasoning performance but not with processing speed, whereas diabetes was associated with poorer performance in memory and processing speed but not with reasoning performance.
Our findings are generally consistent with those of other studies that have examined the relationship of demographic characteristics and health factors with cognitive performance. Others have reported the relationship of depression with declining cognitive status on the MMSE (Crowe et al., 2010) and with incident mild cognitive impairment (Arvanitakis, Wilson, Bienias, Evans, & Bennett, 2004; Luchsinger et al., 2007), as well as of diabetes with memory and reasoning (Brands et al., 2007). Two meta-analyses of the relationship between depression and memory functions (Burt, Zembar, & Niederehe, 1995; Veiel, 1997) reported some support for this relationship. Interestingly, the results of the latter meta-analysis suggest that it is likely that depression affects certain aspects of memory and only in particular subsets of depressed persons. However, both the analyses included younger populations, precluding a direct comparison with the ACTIVE sample.
Two studies have considered the association of demographic and health factors with cognitive function. Similar to our findings, Zelinski et al. (Zelinski & Gilewski, 2003) studied 6,663 non-institutionalized age 70 to 103 and found younger age, White race, and more education to be the most predictive of cognitive function with health factors having a smaller affect. Depression consistently affected memory, global cognitive status, and, to a lesser degree, working memory. After controlling for demographic variables, stroke negatively affected recall, mental status, and the overall cognitive score, while high blood pressure was associated with an improved mental status. Cognitive performance was not predicted by the presence of heart disease, diabetes, or lung disease.
Our findings also are generally consistent with those of the Baltimore Memory Study although that sample of 1,140 subjects was younger (age 50-70). The Baltimore Memory Study found that cognitive performance was related most strongly to demographic factors (race and SES) and to health factors (diabetes, taking medications for hypertension or anxiety, tobacco use, history of stroke, alcohol consumption, blood lead, and BMI) to a lesser degree.
Strengths of the ACTIVE study include a large, racially and geographically diverse sample of community-dwelling older adults. While African Americans have often been underrepresented in cognitive aging studies, they comprise 26% of the ACTIVE sample. The sample characteristics are similar to national averages in many ways. For example, the prevalence of ischemic heart disease, stroke, and diabetes are all within 3% and hypertension is within 6% of the national prevalence rates (Benson, 1998; Cohen, 1995; Federal Interagency Forum on Aging Related Statistics, 2000). Finally, using a composite score for tests of memory, reason, and speed of processing helped assure that the results measured an “ability” rather than the results for a single test.
We also note some limitations. The sample used by ACTIVE was made up of healthy volunteers without functional decline or cognitive impairment as assessed by their score on the MMSE. The sample was also well educated, and the range of cognitive ability was somewhat restricted. This may have limited our ability to detect associations with cognitive domains, though it should be noted that several such associations were found. First, we used a convenience sample of volunteers that specifically excluded subjects with significant cognitive dysfunction, self-reported diagnosis of Alzheimer’s disease, and recent stroke. The self-selection aspect in combination with the specific exclusion criteria could have the affect of minimizing the range and severity of health conditions in our sample and, as a result, could bias the results toward a smaller affect for health conditions and illnesses on cognition. In addition, the list of health factors in this study did not include all conditions that may affect cognitive functioning such as head injury or epilepsy. Similarly, another potential limitation is that all health conditions were self-reported, and information was not collected as to the severity of the health conditions. There is some question in the literature as to how accurate the self-report of health conditions is. Some articles reveal that self-report is a reasonable method of gathering this information, and one even showed self-report to be better than physician evaluation from a prognostic sense (Baumeister, Kriston, Bengel, & Haerter, 2010; Ferraro & Farmer, 1999). Others have argued that self-report is not always accurate and is instead related to the participant’s understanding of what the health condition is, how severe it is, and which conditions are being inquired about (Beckett, Weinstein, Goldman, & Lin, 2000). This was true in a study by Okura and colleagues that revealed high agreement between medical records and self-report for diabetes, hypertension, myocardial infarction, and stroke (kappa 0.71-0.80), but not for heart failure (kappa 0.46). Specificity was greater than 90% for all these diseases (Okura, Urban, Mahoney, Jacobsen, & Rodeheffer, 2004). Finally, our results likely overestimate the affect of race on cognition, as we were unable to fully account for relevant disparities that overlap with race.
In conclusion, we have provided an overview of some of the factors that influence cognitive function in community-dwelling older adults. Demographic factors have relatively strong independent influences on cognition, while health conditions such as diabetes, suspected clinical depression, and stroke have an independent but weaker relationship to cognitive function. Future research should examine whether duration and severity of health conditions might have a larger role in affecting cognition in older adults.
Footnotes
Authors’ Note
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Rebok is an investigator with Compact Disc Incorporated for the development of an electronic version of the ACTIVE memory intervention. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Nursing Research, National Institute on Aging, or the National Institutes of Health. Representatives of the funding agency have been involved in the review of the manuscript but not directly involved in the collection, management, analysis, or interpretation of the data.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs. Unverzagt and Marsiske have received research support from Posit Science, Inc., in the form of site licenses for cognitive training programs for different research projects.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Nursing Research (U01 NR04508 and U01 NR04507) and the National Institute on Aging (U01 AG14260, U01 AG14282, U01 AG14263, U01 AG14289, U01 AG014276, and R01 AG026096).