
Abstract
Asians were the fastest growing ethnic group in the United States during the last decade (U.S. Census Bureau, 2011). Among those 65 and above, the Asian population is projected to triple over the next four decades, from 3% presently to 9% of the population in 2050 (U.S. Census Bureau, 2010). This is the largest percentage increase among any racial/ethnic group in the United States.
In light of the growing size of this population, the present study develops a model of spiritual care for hospitalized Asians. More specifically, the study examines the relationship between addressing older Asians’ spiritual needs and their overall satisfaction with service provision, in tandem with the effects of eight potential mediators. It is widely recognized that spiritual needs emerge during hospitalization and that practitioners should address these needs to optimize satisfactory service provision (Koenig, 2012; Koren & Papamiditriou, 2013). Yet, little, if any, research has examined the process of meeting the spiritual needs of hospitalized Asians in the United States (Koenig, 2007). Toward this end, we review some relevant information about the Asian population in the United States, spiritual needs, and the relationship between addressing these needs and overall satisfaction with service provision. We conclude the section by delineating a hypothesized model of spiritual care, which is subsequently tested.
Literature Review
The term Asians is commonly understood to refer to people originating from the Far East, Southeast Asia, or the Indian subcontinent (U.S. Census Bureau, 2011). Included under this umbrella are people from nations such as China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, and Vietnam. Currently some 14.7 million Asians reside in the United States, accounting for over 5% of the American population (2011). As noted above, the population of older Asians is projected to increase dramatically over the course of the next few decades (Nandan, 2005).
Hospitalizations rates are generally lower for Asians relative to European Americans, although exceptions exist for certain health problems among some subgroups (Klatsky & Tekawa, 2005). Interestingly, Mui and Shibusawa (2008) found that higher levels of spirituality was related to greater hospital use among their sample (n = 407) of six older Asian subgroups living in New York City. They concluded that spirituality may give older Asians the necessary courage to obtain assistance with health-related problems.
A relatively substantial body of research links spirituality with a broad array of salutary health outcomes (Levin, 2010). For example, spirituality has been positively associated with optimism, social support, and life satisfaction, and inversely associated with anxiety, loneliness, and depression (Koenig, King, & Carson, 2012). Including among these positive outcomes is coping. People often draw upon their spirituality to help them cope with challenging situations (Pargament, 2007).
This includes coping with health-related challenges (Soenke, Landau, & Greenberg, 2013). For example, older Asians are as likely to pray for their health as their European American counterparts (Tait, Laditka, Laditka, Nies, & Racine, 2011). Consistent with other racial/ethnic groups, spirituality is a salient dimension of experience for Asians wrestling with medical concerns (Koenig et al., 2012; Pargament, 2007), although spirituality may be conceptualized in broader terms than is common among some European Americans (Lee & Chan, 2009; Leung & Chan, 2010).
Spiritual Needs
Various definitions of spirituality have appeared in the literature (Canda & Furman, 2010). Spirituality can be conceptualized as experiential aspects of human existence that transcend sensory phenomena (World Health Organization [WHO], 1990). Accordingly, spirituality is a universal human phenomenon that is expressed in both religious and secular forms (Crisp, 2010). In turn, spiritual needs flow from this innate spiritual drive (Nixon & Narayanasamy, 2010).
Spiritual needs are commonly understood to be universal in nature, a manifestation of an intrinsic and fundamental component of human nature that integrates and gives meaning to human existence (Narayanasamy, 2010). Spiritual needs include desires frequently expressed in religious spheres (e.g., connection with a Higher Power) as well as desires expressed in non-religious, secular spheres (e.g., hope, meaning, purpose, existential connection with other humans; Hermann, 2001; Murray, Kendall, Boyd, Worth, & Benton, 2004; Tanyi, Recine, Werner, & Sperstad, 2006). As such, spiritual needs are holistically intertwined with patients’ emotional, physical, and psychological needs (Clark, Drain, & Malone, 2003). Among hospitalized patients, such needs may manifest in terms of formal religious practices (e.g., visitation from clergy, receiving communion, etc.), or they may manifest in secular forms, apart from religion, such as searching for meaning in difficult experiences, achieving transcendence, or easing fear and loneliness (Hermann, 2001).
In turn, addressing these spiritual needs helps patients cope with the challenges associated with hospitalization (Koenig, 2013). In keeping with this view, many organizations recommend the administration of a spiritual assessment to identify and address patients’ spiritual needs. Included among these organizations are the Joint Commission (2012), the National Cancer Institute (2012), and the WHO (1990).
A number of quantitative studies have examined the relationship between addressing patients’ spiritual needs and various outcomes among diverse samples. More specifically, addressing patients’ spiritual needs has been linked with decreased depression (Ganatra, Zafar, Qidwai, & Rozi, 2008; Pearce, Coan, Herndon, Koenig, & Abernethy, 2012) and lower medical costs (Balboni et al., 2011). Furthermore, addressing patients’ spiritual needs has been associated with greater quality of care (Astrow, Wexler, Texeira, He, & Sulmasy, 2007), higher levels of spiritual meaning and peace (Pearce et al., 2012), and better quality of life (Balboni et al., 2007; Balboni et al., 2010; Kang et al., 2012).
Two of these studies were conducted with samples of older Asians. Ganatra and associates (2008) examined the relationship between spiritual needs and depression among individuals (n = 402) receiving services at a community health clinic in Pakistan. They reported that inadequately fulfilled spiritual needs were associated with higher levels of depression. Kang and associates (2012) examined the relationship between addressing spiritual needs and quality of life among a sample of inpatients receiving cancer treatment at palliative care centers in Korea. Among their spiritually diverse sample (n = 94), patients whose spiritual needs were addressed reported higher levels of quality of life.
Spiritual Needs and Overall Satisfaction
One particularly noteworthy outcome is overall satisfaction with service provision (Chandra et al., 2011). This variable—perceptions of global satisfaction—is widely used as a proxy for the quality of care provided during hospitalization (Jackson, Chamberlin, & Kroenke, 2001; Shea et al., 2008). Consequently, the overall quality of services provided in hospitals, as well as many other health care settings, is commonly assessed with measures of global satisfaction (Chandra et al., 2011; Gribble & Haupt, 2005; Press, 2002). In keeping with this perspective, the U.S. Patient Protection and Affordable Care Act (P. L. 111-148) links Medicaid reimbursements to patient satisfaction scores (Neuhausen & Katz, 2012). In other words, hospitals that record higher levels of patient satisfaction with service provision receive more funding (Rau, 2011).
A number of studies have examined the relationship between addressing patients’ spiritual needs and overall satisfaction with service provision (Astrow et al., 2007; Clark et al., 2003; Williams, Meltzer, Arora, Chung, & Curlin, 2011). Consistent with the prior research reviewed above, addressing spiritual needs has been positively associated with higher levels of satisfaction in all of these studies.
These findings lead us to posit that satisfaction with hospital staff’s efforts to address older Asians’ spiritual needs will be associated with higher levels of overall satisfaction with service provision. Patients typically report that they appreciate having their spiritual needs addressed during hospitalization (Koenig, 2013). Furthermore, the existing research suggests that older Asian Americans are just as likely to use spirituality to address health concerns as older European Americans (Tait et al., 2011). Thus, we expect that addressing spiritual needs in a satisfactory manner will be associated with higher levels of overall satisfaction among older Asian American patients.
Potential Mediators
Although prior quantitative research has documented a positive effect between satisfactorily addressing patients’ spiritual needs and overall satisfaction, no research appears to have identified mediators of this relationship. As alluded to above, this represents a significant gap in the literature since, by necessity, certain variables must mediate the relationship between spiritual needs and overall satisfaction. In other words, no research has examined possible mediating variables that may explain the relationship between spiritual needs and satisfaction. Ascertaining the variables that explain the relationship between spiritual needs and satisfaction is critical since identifying such variables is a necessary prerequisite for equipping hospital practitioners with the knowledge required to tailor services more effectively.
In keeping with Andersen’s (1995) behavioral model of health services use, a number of constructs likely influence perceptions of overall satisfaction with service provision. Included among these are demographic characteristics, perceptions of need, and organizational characteristics. In this study, we focus on organizational characteristics. Of the various factors that influence perceptions of the overall satisfaction, these organizational characteristics are perhaps the most malleable (Andersen, 1995).
Key organizational dimensions during hospitalization include the admissions process, room quality, meal service, nursing staff, tests and treatment administration, visitors, physicians, and the discharge process. These eight organizational characteristics span the hospitalization experience and are indicated as important by the health service quality literature and the National Library of Health Care Indicators (Kaldenberg, 2001). Service provision in these areas is highly adaptable and, in keeping with the behavioral model of health services use, holds important implications for program design and interventions (Andersen, 1995).
In addition to being highly malleable, these organizational dimensions meet the requirements necessary for mediation. For these organizational variables to mediate the relationship between spiritual needs and overall satisfaction, they must be related to (a) spiritual needs while also being related to (b) overall satisfaction (Baron & Kenny, 1986). Satisfaction with services in each dimension is frequently related to overall satisfaction, and qualitative research suggests that spiritual needs can emerge in each dimension (Press, 2002).
For instance, a number of researchers have examined nurses’ role in addressing patients’ spiritual needs (Conner & Eller, 2004; Koren & Papamiditriou, 2013; Nixon & Narayanasamy, 2010; Tanyi et al., 2006; Taylor, 2003). This qualitative work suggests that patients frequently look to nurses to respond to their spiritual concerns. Nurses convey warmth, courtesy, and information that directly meets the expressed spiritual needs of many patients while also responding to requests that address other needs (e.g., facilitating a quiet space to pray or mediate, access to information about tests and their ramifications for wellness, etc.). This research suggests the quality of care provided by the nursing staff may mediate the relationship between spiritual needs and overall satisfaction among older Asian patients.
Although less work has been done in the other key areas of service provision, some research indicates that spiritual needs can emerge in each of the other organizational dimensions mentioned above. For example, patients may express spiritual needs related to fear of the unknown during the admissions process (Jang et al., 2004; McBrien, 2010); a quiet, ascetically pleasing room that is conducive for prayer or mediation (Hermann, 2001); kosher or halal food that is respectfully served (Davidson, Boyer, Casey, Matzel, & Walden, 2008); the provision of timely information about tests and treatments in a courteous, caring manner (Hodge & Horvath, 2011); visits from friends, family, and clergy (Conner & Eller, 2004); physicians who express concern and respect regarding patients’ spiritual values as they intersect treatment decisions (Ellis & Campbell, 2004; Galanter, Dermatis, Talbot, McMahon, & Alexander, 2011); and discharge plans that process the existential sense of loss and grieving that emerged during hospitalization (Koenig, 2012; Meert, Thurston, & Briller, 2005). Furthermore, across the arc of hospitalization, patients often report a spiritual need for staff to be courteous, caring, informative, skillful, and supportive of their spirituality (Anderson, Anderson, & Felsenthal, 1993; Hodge & Horvath, 2011; Meert et al., 2005; Tanyi et al., 2006).
Thus, satisfaction in each of these areas may potentially function as a mediator in a manner analogous to nursing staff (Baron & Kenny, 1986). For example, some research suggests physicians may play an important role in addressing patients’ spiritual concerns as a result of their unique status on the health care team (Astrow et al., 2007; Ellis & Campbell, 2004; Hodge & Horvath, 2011). Other commentators indicate that social workers administering the discharge process are often instrumental in responding to the needs that have emerged during hospitalization but have not been adequately addressed during ever shorter stays (Koenig, 2012). It is important to reiterate, however, that less research exists on these seven organizational dimensions relative to nursing.
Figure 1 depicts a hypothesized mediation model. In this model, satisfaction with hospital staff’s efforts to address older Asians’ spiritual needs is posited to exhibit a direct and positive effect on overall satisfaction with service provision. This relationship between satisfactorily spiritual needs and overall satisfaction is mediated by eight areas of service provision: the admissions process, room quality, meal service, nursing staff, tests and treatment administration, visitors, physicians, and the discharge process.
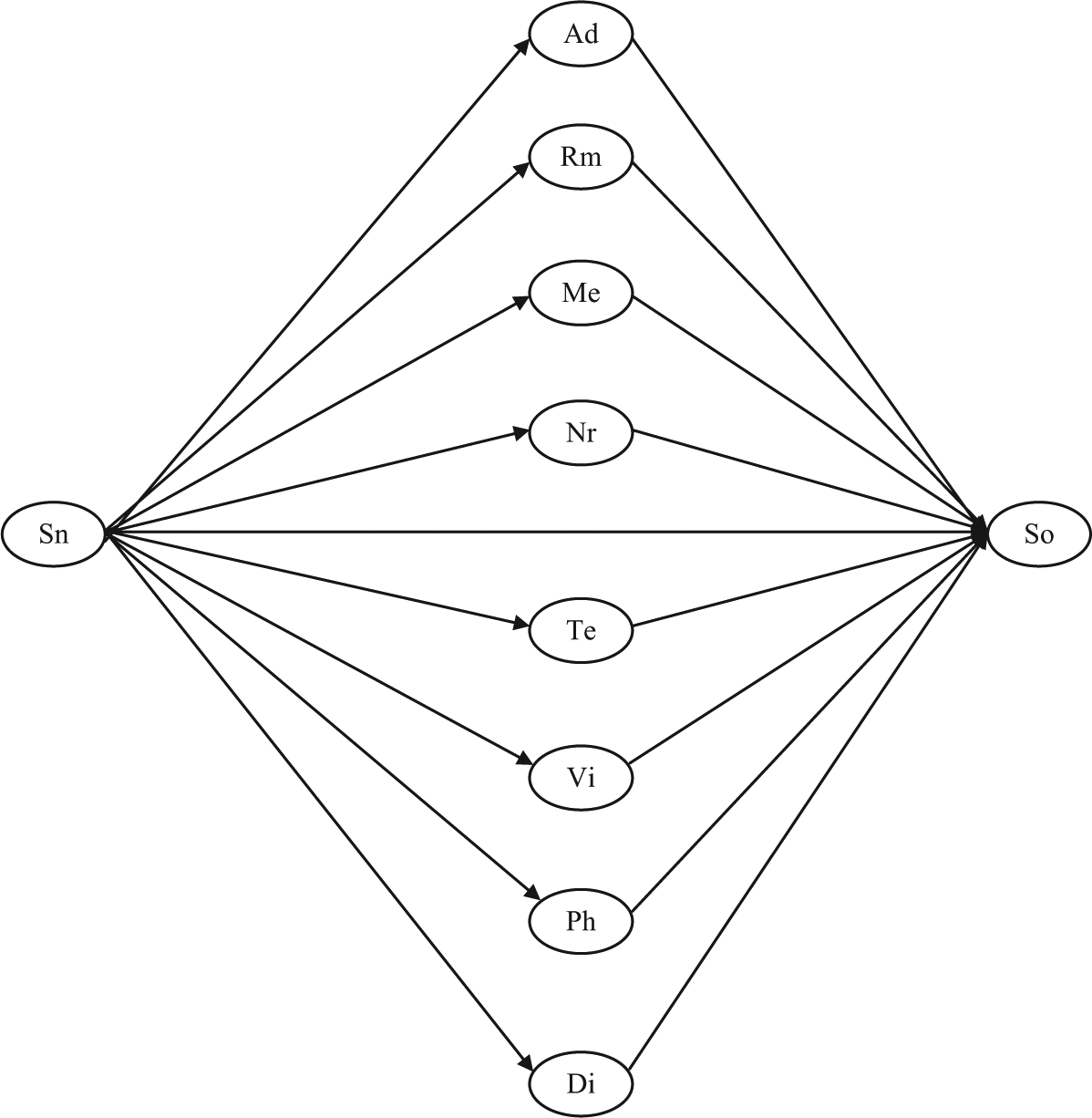
Theoretical model of the relationship between spiritual needs and overall satisfaction with eight potential mediators.
Method
To test this model, a secondary data analysis of hospital inpatient satisfaction data was conducted. The data were obtained from Press Ganey Associates, Inc., a health care consulting firm that specializes in patient satisfaction measurement and management. As noted above, hospitals typically measure patient satisfaction as a means to assess service quality (Chandra et al., 2011). This task is frequently delegated to outside organizations. Of these organizations, Press Ganey is the largest (Press Ganey Associates, 2011). De-identified data were provided for the present study, which was conducted with the approval of a university Institutional Review Board.
Sample
The sample consisted of 805 Asians, aged 50 and above, who were consecutively discharged over a 12-month period from hospitals from four geographic regions. The 50-year mark is commonly used to delineate older adults since this is the decade with health-related problems often begin to manifest (Tait et al., 2011). Just over half the sample (50.8%, n = 409) was female. In terms of age, 42.4% (n = 341) of respondents were between 50 and 64 years old, 40.1% (n = 323) were between 65 and 79 years old, and 17.5% (n = 141) were 80 and older. Regarding their geographic location, 24.1% (n = 194) were from the Northeast, 30.2% (n = 243) from the South, 14.2% (n = 114) from the Midwest, and 31.6 (n = 254) were from the western region of the United States.
Measures
Spiritual needs
Respondents’ perceptions of how well hospital staff addressed their spiritual needs were operationalized with a single item. More specifically, individuals were asked to indicate the “degree to which hospital staff addressed your spiritual needs” on a 5-point, Likert-type response key that ranged from “very poor” (1) to “very good” (5). This item is similar to one used in prior research examining the relationship between spiritual needs and overall satisfaction (Astrow et al., 2007). For the purposes of the present study, this exogenous variable was assumed to be measured without error.
Overall satisfaction
The latent construct of overall satisfaction with the services provided during hospitalization was measured with three items (see Table 1). The same 5-point, Likert-type response key described above was used with these items. A Cronbach’s alpha of .94 was obtained in this study. This alpha is similar to the level of reliability recorded in previous research using this scale (Kaldenberg, 2001).
Factor Loadings and Measurement Error Coefficients for Multiple Item Measures.
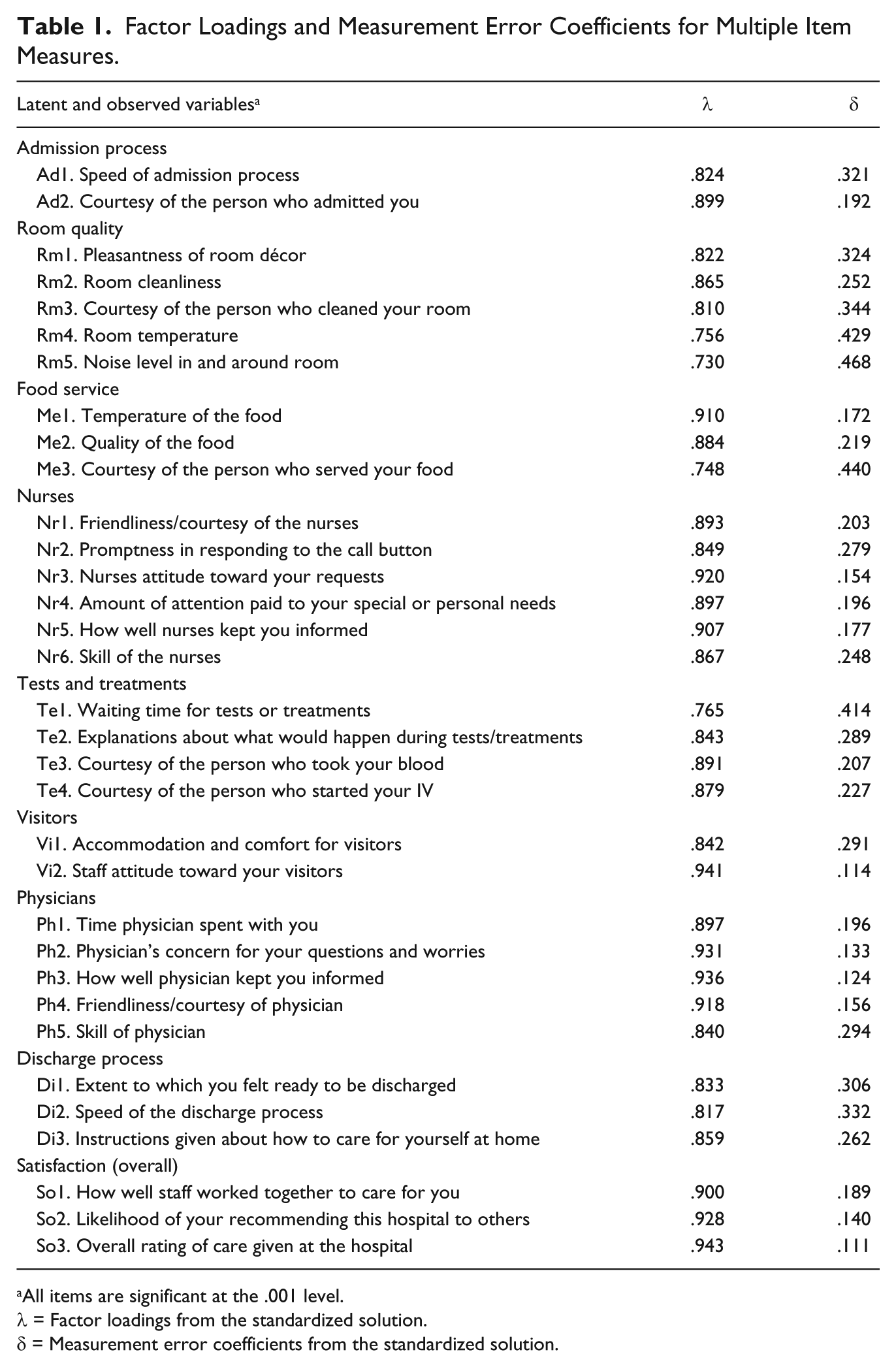
All items are significant at the .001 level.
λ = Factor loadings from the standardized solution.
δ = Measurement error coefficients from the standardized solution.
Potential mediators
The study included eight variables that potentially mediate the relationship between spiritual needs and overall satisfaction. These variables were developed by Press Ganey to assess the major organizational dimensions of service provision across the hospitalization experience. As noted above, these areas capture the key areas of service provision articulated in both the service quality literature and the National Library of Health Care Indicators (Kaldenberg, 2001).
The indicators for these eight latent constructs are listed in Table 1. Each indicator was paired with the 5-point, Likert-type response key described above. The alphas obtained in this study for each scale are listed as follows: admission process (α = .83), room quality (α = .89), food service (α = .88), nurses (α = .96), tests and treatments administration (α = .90), visitors (α = .88), physicians (α = .96), and the discharge process (α = .87). These values are similar to the reliability coefficients recorded in previous research using these scales (Kaldenberg, 2001).
Data Analysis
Structural equation modeling was preformed with AMOS 20.0. Across the data set, 3.41% of values were missing. No values were missing from the categorical or the outcome variables. Although most continuous variables had a minimal number of missing values, three items were missing more than 6% of their values (Ad2, 9.7%; Te2, 6.8%; Te1, 6.2%).
The Expectation-Maximization (EM) algorithm procedure in SPSS was used to impute missing values for the continuous indicators (Peng, Harwell, Liou, & Ehaman, 2007). EM estimation and the Full Information Maximum Likelihood (FIML) procedure are among the most commonly recommended methods for dealing with missing data (Byrne, 2010). The FIML procedure offers the advantage of making use of all the available data without resorting to imputation, but limits the number of indices available for assessing model fit (Blunch, 2008). Given the relatively minimal amount of missing data, the EM estimation procedure was used to retain the full sample and to access all fit indices (Kline, 2011).
Preliminary examination of the continuous variables revealed evidence of non-normality. To improve normality, the continuous variables were transformed using the normal scores function in PRELIS (du Toit, du Toit, Mels, & Cheng, 2006). This procedure resulted in skew and kurtosis values of, respectively, < 0.865 and < 1.120, across the continuous variables. Despite improvement in the univariate skew and kurtosis values, Mardia’s test of multivariate normality was not supported. This is a concern since the widely used Maximum Likelihood (ML) method of estimation assumes multivariate normality.
Alternative estimation techniques exist, such as weighted least squares (WLS), that make no assumptions about multivariate normality (i.e., asymptotically distribution-free techniques). Such estimators, however, typically require large small sizes (e.g., 5,000 cases) to work satisfactorily (Lei & Wu, 2012). Conversely, ML estimation is commonly considered to be relatively robust (Schumacker & Lomax, 2010). For instance, Finney and DiStefano (2006) recommend the use of ML estimation with data that exhibits up to moderate non-normality (i.e., skew < 2 and kurtosis < 7). Under such departures from non-normality, the use of ML estimation may result in attenuated parameter estimates (Finney & DiStefano, 2006). However, given that the data in the present study fell well within Finney and DiStefano’s criteria, ML estimation was used for all models.
The models adjusted for the effects of demographic variables. This was accomplished by incorporating the control variables directly into the model by allowing them to covary as exogenous predictors (Mueller & Hancock, 2010). Accordingly, the structural models in the following section controlled for the effects of gender, age, and geographic region.
To test the hypothesized mediation model, a standard two-phase procedure was used (Mueller & Hancock, 2010; Schumacker & Lomax, 2010). In the first phase, the measurement model is validated. After validating the measurement model, the hypothesized structural model is tested.
Results
Measurement Phase
Initially, a measurement model was constructed consisting of the eight mediators, overall satisfaction, and their associated indicators. Table 1 displays the standardized factor loadings and measurement error coefficients for all the multiple item measures. The factor loadings function as validity coefficients, indicating how accurately the indicator measures the latent construct (Joreskog & Sorbom, 1993). Values > .70 indicate relatively high loadings (Kline, 2011). For this initial model, factor loadings ranged from .730 to .943 suggesting the items are psychometrically valid indicators of the underlying construct.
A number of indices have been developed to assess the fit between the hypothesized model and the data. These fit indices can be classified into three different classes: (a) absolute indices that appraise the overall discrepancy between the implied and observed covariance matrices, (b) parsimonious indices that assess the overall discrepancy between the implied and observed covariance matrices while taking into account the model’s complexity, and (c) incremental indices that evaluate absolute or parsimonious fit relative to a baseline model, typically the null model or a model that specifies no relationships among the observed variables (Mueller & Hancock, 2008).
Since absolute, parsimonious, and incremental fit indices use modally different approaches to assessing fit, they can yield inconsistent results. Consequently, Mueller and Hancock (2010) recommend reporting fit results from all three classes. Within each class, they recommend using the best performing index. In keeping with their recommendations, we report the results of the Standardized root mean square residual (SRMR) in the absolute class, the root mean square error of approximation (RMSEA) with 90% confidence intervals in the parsimonious class, and the Comparative Fit Index (CFI) in the incremental class. As might be expected, these three indices are widely recommended by various authorities (Byrne, 2010; Garson, 2012; West, Taylor, & Wu, 2012).
We also report the results of the chi-square test, one of the first (absolute) indices to gain widespread popularity. Subsequent empirical work, however, has demonstrated that this test is sensitive to departures from multivariate normality and sample size (Schumacker & Lomax, 2010). For example, if the sample is sufficiently large (e.g., >200), good fitting models are frequently rejected (Blunch, 2008). Consequently, while it is common practice to report the chi-square value, this test is not particularly helpful in assessing model fit in many instances, including the present study (West et al., 2012).
To evaluate model fit using the SRMR, the RMSEA, and the CFI, the following guidelines are commonly used. For the SRMR, values < than 0.09 represent a good fit between the proposed model and the data (Mueller & Hancock, 2008). For the RMSEA, values < .08 represent a reasonable fit and values < .05 represent a good fit (Byrne, 2010), with values > .10 indicating a poor fit (Garson, 2012). For the CFI, values > .90 indicate a marginal fit while values > .95 indicate a good fit (Byrne, 2010).
The fit statistics for the measurement model were as follow: χ2 = 1,890.115 (df = 459, p < .001), SRMR = .040, RMSEA = .062 (90% CI = [.059, .065]), and CFI = .947. Although the model fit values might be considered acceptable, the CFI value fell just below the .95 value commonly viewed as denoting a good fit (Byrne, 2010). An examination of the modification indexes suggested adding a measurement error covariance between Te3 and Te4 would improve the model fit. This recommendation may stem from the use of the same language in these two items—that is, “courtesy of the person who . . . ” The use of similar language can cause a method effect which, in turn, can be addressed through the application of an error covariance (Byrne, 2010). The addition of the error covariance resulted in an acceptable model fit across all indices: χ2 = 1,654.280 (df = 458, p < .001), SRMR = .039, RMSEA = .057 (90% CI = [.054, .060]), and CFI = .956.
Structural Phase
After validating the measurement model, a structural model was constructed in which the eight areas of service provision mediated the relationship between spiritual needs and satisfaction. The fit statistics for the hypothesized structural model were as follows: χ2 = 1,910.187 (df = 626, p < .001), SRMR = .034, RMSEA = .051 (90% CI = [.048, .053]), and CFI = .955. As can be seen, the fit indices suggested the fit of the hypothesized model was acceptable.
Table 2 depicts the parameter estimates for hypothesized relationships in structural model. Specifically, this table reports each relationship, along with its corresponding standardized regression estimate, the unstandardized estimate, the standard error, and level of significance. As depicted in the table, five variables appeared to mediate the relationship between spiritual needs and overall satisfaction. Sobel tests using Preacher and Leonardelli’s (2013) online calculator confirmed the existence of mediation for these five variables: the administration process (z = 2.548, p = .011), nursing staff (z = 9.104, p = < .001), visitors (z = 2.719, p = .006), physicians (z = 5.168, p = < .001), and the discharge process (z = 2.735, p = .006). These five variables fully mediated the relationship between satisfactorily addressing older Asians’ spiritual needs and respondents’ perceptions of overall satisfaction with service provision.
Parameter Estimates for Hypothesized Relationships in Structural Model.

Indirect effects—which are estimated as the product of the direct effects that comprise the paths—were calculated for each of the five mediators (Kline, 2011). For example, the standardized indirect effect of spiritual needs on satisfaction through the admissions process is .048 (.557 × .087). These values are interpreted like path coefficients. An examination of the indirect effects for each mediated path indicated that nursing staff played the most prominent role in explaining the relationship between spiritual needs and satisfaction (.256), followed by physicians (.114), the discharge process (.082), visitors (.069), and the admissions process (.048).
Discussion
In light of the growing Asian population, this study sought to develop a model of spiritual care for use with older hospitalized Asians. Toward that end, the study examined the relationship between addressing older Asians’ spiritual needs and perceptions of overall satisfaction with service provision in tandem with the effects of eight possible mediators. Identifying the variables that explain the relationship between spiritual needs and overall satisfaction assists practitioners develop and provide more effective, culturally relevant services to Asian patients.
The results suggest that the relationship between satisfactorily addressing patients’ spiritual needs and overall satisfaction with service provision is fully mediated by five variables. In decreasing order of magnitude these five variables consist of nursing staff, physicians, the discharge process, visitors, and the admissions process. Satisfaction with services in these five organizational areas fully explained the relationship between spiritual needs and overall satisfaction with service provision among the study’s sample of older Asian patients.
This finding is consistent with prior quantitative research that has documented a positive relationship between spiritual needs and overall satisfaction (Astrow et al., 2007; Clark et al., 2003; Williams et al., 2011). The magnitude of the path coefficients indicated that nurses played the most prominent role in explaining this relationship, a finding consistent with the results of a number of qualitative studies that suggest nursing staff play an important role in addressing patients’ spiritual needs (Conner & Eller, 2004; Koren & Papamiditriou, 2013; Nixon & Narayanasamy, 2010; Tanyi et al., 2006; Taylor, 2003).
Similar comments can be made about the other identified mediators. For example, some scholarship has highlighted the role of family support and positive attitudes toward physicians as enabling factors for formal service use among older Asian adults (Mui & Shibusawa, 2008). In short, nurses, physicians, social workers administering the discharge process, the facilitation of visitors, and admissions personnel all helped to explain the positive association between spiritual needs and overall satisfaction.
Implications for Practice
In discussing the implications for practice, it is important to emphasize the preliminary nature of the findings. As perhaps the first study of its kind, replication with other samples of older Asian Americans is needed before firm conclusions can be drawn from the data. Bearing this caveat in mind, the results do suggest a number of implications for practice with older hospitalized Asians.
Although the population of older Asians in the United States is highly diverse, the more than 30 ethnic subgroups that comprise this population share some common challenges (e.g., language proficiency, lack of health insurance) as they experience aging-related health issues in a country where most were not born (Mui & Shibusawa, 2008). For example, one third of Chinese elders in the United States immigrated after age 60 (Mui & Shibusawa, 2008). When faced with the prospect of hospitalization, one common challenge is navigating a hospital system that is often very different from their experiences in their country of origin (Torsch & Ma, 2000).
Spiritual needs inevitably emerge in such circumstances (Narayanasamy, 2010). Accordingly, assessing older Asians spiritual needs is the first important step in practice (Koenig, 2007). Given the diverse cultural backgrounds among this population, practitioners might start by exploring their spiritual preferences during the intake process to ensure that subsequent services are tailored appropriately to ensure as much cultural congruence as possible.
During such an assessment, it is important to be familiar with the diverse expressions of spirituality common in Asia, which may differ in character from those widely affirmed among European Americans (Lee & Chan, 2009; Leung & Chan, 2010). An older Chinese immigrant, for example, might report no formal religious affiliation. Yet, this same individual may strongly affirm belief in the importance of a transcendent healing power (Mui & Shibusawa, 2008). Thus, it is helpful to be cognizant of common expressions of spirituality among the Asian subgroups commonly encountered so that the presence of such beliefs can be explored during the assessment process.
The results may also have implications for medical interventions. More specifically, interventions that incorporate efforts from both informal support systems (e.g., relatives, friends, or other visitors) and formal support networks (e.g., nurses, physicians, social workers) may be helpful in addressing patients’ spiritual and health needs. Due to language and other cultural barriers, older Asians often rely on family members to link them with formal services. Having access to such visitors can help older Asians address anxieties and other spiritual needs that arise from adjusting to the hospital environment. They also help ensure that medical interventions are understood and implemented appropriately.
Accordingly, practitioners might consider including family members as part of their multi-disciplinary service delivery team. Empowering family members to educate their older relatives regarding the hospital service procedures and the roles of different practitioners can address both spiritual and medical needs. Such collaborative efforts can result in better service provision.
Limitations
Some limitations exist that should be considered when interpreting the results and implications. As noted previously, Andersen’s (1995) behavioral model of health services use suggests a number of variables may also be relevant. For example, perceptions of need stemming from the severity of the patients’ illness may influence the relationship between spiritual needs and overall satisfaction. Due to unavailability of specific illness variables in the data set, the influence of these and other variables could not be tested in the model.
Additional limitations include the cross-sectional nature of the data, the use of self-report measures, and the possibility of various types of response set bias. For instance, the spiritual needs question is an optional item that must be requested by hospitals. It is possible institutions that requested the inclusion of this item may be particularly committed to addressing patients’ spiritual needs relative to hospitals that did not request its inclusion.
The use of a geographically diverse sample may help to counter some of biases observed in studies conducted in specific geographic areas (Pearce et al., 2012; Williams et al., 2011). Nevertheless, the use of a non-random sampling design precludes generalizing the resulting model to other samples of older hospitalized Asians. While this study provides an initial understanding of the relationship between spiritual needs and overall satisfaction, and the variables that mediate this relationship, further research is needed with other samples of Asians to replicate the results obtained in this study.
Conclusion
This study helps address calls that have appeared in the literature citing the need for increased training in the provision of spiritual care to Asians (Nagai, 2008). As the first study to develop and test a model of spiritual care for use with older hospitalized Asians inpatients, the findings may assist practitioners tailor services to this population. By identifying key domains in the process, they can facilitate the provision of more effective, culturally relevant services.
The results suggest that the relationship between older Asians’ spiritual needs and overall satisfaction with service provision is fully mediated by five variables: nurses, physicians, the discharge process, visitors, and the admissions process. This suggests that nurses, physicians, and social workers administering the discharge process play a critical role in the process of effectively addressing older Asians’ spiritual needs. Furthermore, these formal providers can enhance service provision by working collaboratively with family members and other visitors. Such collaborative relationships can address patients’ spiritual and medical needs, helping to optimize service provision to members of this population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article was supported by a grant from the John A. Hartford Foundation.