
Abstract
Past research has established that older adults can improve their cognitive abilities through interventions that target memory, reasoning, and speed of processing, as well as other domains (Ball et al., 2002; Edwards, Wadley, et al., 2005; Mozolic, Long, Morgan, Rawley-Payne, & Laurienti, 2011; O’Hara et al., 2007; Willis et al., 2006). However, little is known about how these interventions achieve improvements in the cognitive abilities of older adults or how individual characteristics are associated with responsiveness to such interventions. A prior study showed that higher self-efficacy is associated with larger reasoning training gains, and memory self-efficacy influences engagement and effort during this cognitive intervention (Payne et al., 2012). We investigated whether self-efficacy similarly serves as a predictor of responsiveness (e.g., moderation) to cognitive speed of processing training (SOPT). One previous study found that SOPT enhanced self-efficacy (Wolinsky, Vander Weg, et al., 2010). Thus, we also examined whether cognitive gains from SOPT can be attributed to improved self-efficacy (e.g., mediation).
Self-Efficacy
Self-efficacy is an individual’s perceived ability to produce and regulate life events (Bandura, 1977, 1989), and is a dynamic concept that results from the interplay of cognitive, social, and behavioral skills working together to serve a specific purpose (Bandura, 1989). Bandura (1977, 1989) posits that the types of activities people engage in, the level of effort they expend, and their emotional response to behavior are influenced by self-efficacy. For example, cognitive training gains can be related to a participant’s beliefs about the intervention, and participants may perform better based upon their beliefs (Morrison & Chein, 2011). Increases or decreases in self-efficacy may be causally related to maintenance of cognitive functioning or performance on cognitive tasks, as well as engagement in cognitive training (e.g., Payne et al., 2012; Seeman, McAvay, Merrill, Albert, & Rodin, 1996; Valentijn et al., 2006). Responsiveness to cognitive training could be affected by general self-efficacy, which is an individual’s perceived confidence in completing tasks (Bandura, 1977; Seeman et al., 1996) or specific self-efficacy, which is perceived ability to excel in a targeted cognitive task, such as memory (e.g., Beaudoin & Desrichard, 2011; G. J. McDougall, 2004; Valentijn et al., 2006; Wells & Esopenko, 2008). This study examined two indices of self-efficacy as moderators and mediators of SOPT gains.
Self-Efficacy and Cognitive Performance
The strongest relationships between self-efficacy beliefs and cognitive performance have been found with memory tests (G. J. McDougall, 2004; Payne et al., 2012; Rebok & Balcerak, 1989). Using data from the MacArthur Research Network on Successful Aging Community Study, Seeman et al. (1996) found that strong baseline general self-efficacy beliefs predicted better verbal memory performance at follow-up among men, but not among women. Similarly, Valentijn et al. (2006) found that memory-specific self-efficacy predicted verbal memory performance, as measured by the Visual Verbal Learning Task, at a follow-up interval of 6 years. Thus, both general and specific self-efficacy are related to cognitive performance.
Self-Efficacy and Responsiveness to Cognitive Training
Intervention studies observing the effect of self-efficacy on responsiveness to training provide further evidence of the potential influence of self-efficacy on the effects of cognitive interventions. The findings from a study of memory training (focusing on organization association, attention, and recall) indicated that individuals with higher specific self-efficacy scores had better overall performance on word recall and greater increases in memory post-training (West, Bagwell, & Dark-Freudeman, 2008). Similarly, Payne et al. (2012) found that baseline memory-specific self-efficacy beliefs predicted changes in inductive reasoning following reasoning training with basic (e.g., words, letters, and numbers) and everyday reasoning problems (e.g., completing a mail order form or answering questions about a bus schedule). While many authors have focused on the association between specific self-efficacy and memory training (e.g., Carretti, Borella, Zavagnin, & De Beni, 2011; Payne et al., 2012; West et al., 2008), none have examined the influence of either specific or general self-efficacy on responsiveness to SOPT. Thus, the relationship between self-efficacy and SOPT effects is unclear.
Cognitive SOPT
Consistent evidence demonstrates that SOPT enhances speed of processing for visual attention (Ball, Beard, Roenker, Miller, & Griggs, 1988; Ball, Edwards, & Ross, 2007; Willis et al., 2006). Unlike other cognitive training programs, SOPT transfers to improved performance efficiency for instrumental activities of daily living (IADLs), including driving (Ball, Edwards, Ross, & McGwin, 2010; Edwards et al., 2002; Edwards, Wadley, et al., 2005; Roenker, Cissell, Ball, Wadley, & Edwards, 2003). As examples, SOPT transfers to a 50% reduction in at-fault crash rates over 6 years (Ball et al., 2010) and protects against driving mobility declines over 3 years (Edwards, Myers, et al., 2009). Similarly, SOPT results in reduced rates of driving cessation over 3 years (Edwards, Delahunt, & Mahncke, 2009). There are also health benefits in that SOPT decreases the likelihood of developing depressive symptoms by 30% at 1 and 5 years post-baseline (Wolinsky et al., 2009), and protects against declines in health-related quality of life over 5 years (Wolinsky et al., 2006).
There are individual differences in the effectiveness of SOPT. However, little is known about what factors moderate SOPT gains. Prior studies have found that people with and without memory impairment benefit from training (Unverzagt et al., 2007), and longitudinal training gains do not vary by type of mild cognitive impairment (Valdes, O’Connor, & Edwards, 2012). Also, Ball et al. (2007) found significant weak correlations between training gains and education, age, and mental status. However, very little of the variance in training gains could be attributed to these variables. No prior study has examined whether higher self-efficacy is associated with greater SOPT gains (e.g., self-efficacy moderates SOPT gains).
Interestingly, Wolinsky, Vander Weg, et al. (2010) found that specific cognitive self-efficacy, as indicated by internal locus of control, was improved among older adults randomized to SOPT. As SOPT improved specific cognitive self-efficacy (Wolinsky, Vander Weg, et al., 2010), it is possible that other training-related gains could be attributed to such enhanced self-efficacy (i.e., self-efficacy may mediate SOPT gains). Also, given that Payne et al. (2012) found that memory-specific self-efficacy moderated gains from inductive reasoning training, it is also possible that self-efficacy may moderate SOPT gains. No prior study has examined this. The nature of these relationships was examined in secondary data analyses. Data from the Staying Keen in Later Life (SKILL) study and the Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) study, both of which randomized community-dwelling older adults into either a SOPT or a control group, were analyzed to examine whether baseline self-efficacy beliefs would serve as a moderator or mediator of SOPT gains.
Study 1: SKILL
Method
Participants
Participants included in analyses were obtained from the SKILL study, which randomized 228 community-dwelling older adults to training or an active control condition. Participants were recruited through community organizations and advertisements in community newspapers in the greater areas surrounding both Western Kentucky University and the University of Alabama at Birmingham (Edwards, Wadley, et al., 2005). In addition, older adults in Alabama received letters inviting them to participate. Finally, participants from past research studies conducted at both sites were contacted and invited to participate, and were also asked to refer others for potential participation (Edwards, Wadley, et al., 2005).
Eligibility for participation in this study was based on the following criteria: Mini-Mental State Examination (MMSE) score of 23 or higher, at least a fifth-grade literacy level, a far visual acuity score of 20/80 or better, and Useful Field of View (UFOV) combined subtests 3 and 4 score ≥ 800 or a subtest 2 score ≥ 150 (for further details, see Edwards, Wadley, et al., 2005). These criteria were chosen to ensure that participants could view testing and training stimuli, and potentially benefit from the intervention. The SKILL study initially screened 1,131 adults between the ages of 62 and 94 for participation. From this screened sample, 305 were eligible for training based on the aforementioned inclusion criteria; 77 refused to continue with the study largely due to time demands required for participation. Thus, 228 participants were randomized to training. On average, participants attended training sessions two times a week, with sessions held 1 to 5 days apart (Vance et al., 2007). Prior research has found that the timing interval between sessions can vary without affecting efficacy (Vance et al., 2007). Additional details on participant recruitment and sample characteristics of the SKILL study have been described elsewhere (Clay et al., 2009; Edwards, Wadley, et al., 2005).
The mean age of the 228 participants was 75.23 years (SD = 5.96 years, age range = 63-96 years), with a majority of participants being female (57.5%) and Caucasian (82%). The average years of education for included participants was 13.67 years (SD = 2.60 years). Descriptive characteristics of the study sample are summarized in Table 1 by training condition.
Demographic Characteristics of SKILL Study Participants.

Note. SOPT = Speed of Processing Training; MMSE = Mini-Mental State Examination; SKILL = Staying Keen in Later Life.
Measures
Inclusion measures and assessments of self-efficacy and cognitive speed of processing were selected for data analyses. Further details and rationalization for the measures chosen for the SKILL study can be found elsewhere (Wood et al., 2004).
Mental status
The MMSE was used to assess mental status and diminish the likelihood of including participants with dementia. The MMSE is a staff-administered cognitive screening tool that assesses memory, attention, language, and orientation (Folstein, Folstein, & McHugh, 1975). Scores range from 0 to 30, with higher scores indicating better performance. Scores of 23 or higher were required for inclusion in the study.
Far visual acuity
Far visual acuity was measured using a standard Lighthouse Early Treatment Diabetic Retinopathy Study (ETDRS) chart and evaluated based on the traditional Snellen method with the participant’s available correction, if any (Good-Lite, 2010). All participants were required to demonstrate a Snellen acuity of 20/80 or better, when standing at a distance from the chart of 10 feet, for inclusion. Scores were assigned based on the ACTIVE method (Jobe et al., 2001), which credits each letter correctly identified by the participant, and ranges between 0 and 90 with higher scores representing better far visual acuity.
Self-efficacy
General self-efficacy was measured using a four-point Likert scale with a total efficacy score created by summing the responses in each of the following eight domains: health, transportation, relationships with family, relationships with friends, living arrangements, finance, safety, and productivity. The test–retest reliability of the self-efficacy scale ranges from .50 to .64 (Seeman et al., 1996). Participants rated each item from strongly agree (1) to strongly disagree (4), with lower scores representing greater self-efficacy and possible aggregate scores ranging between 8 and 32 (Rodin & McAvay, 1992). An example of the questions includes the following: (a) “I’ve been feeling this month that keeping healthy depends on things that I can do” (health), (b) “This month I’ve been feeling that it’s up to me to get transportation when I want it” (transportation), (c) “This month I’ve been feeling that I cannot have the relationships with my family I want” (relationships with family), (d) “This month I’ve been feeling that I cannot have the relationships that I want with my friends” (relationships with friends), (e) “This month I’ve been feeling that I do not have enough control over how good are my living arrangements” (living arrangements), (f) “This month I’ve been feeling that I could make my finances better if I wanted to” (finances), (g) “This month I’ve been feeling that there are things I could do to make myself feel safe” (safety), and (h) “I’ve been feeling this month that I cannot be as productive as I want to” (productivity; Rodin & McAvay, 1992).
Speed of processing
The UFOV test was used to measure cognitive speed of processing. The touch PC version of the test was administered to participants. Four subtests were included to evaluate the participants’ speed of processing under increasing cognitive demand at each subsequent subtest. Targets in each subtest were displayed from 16.67 to 500 ms in duration, and scores represented the display durations at which participants accurately performed each subtest 75% of the time (Edwards, Wadley, et al., 2005). The first subtest required participants to identify a central target (a car or truck) presented at a fixation point in the center of the screen. The second subtest required participants to identify both the central target and a simultaneously presented peripheral target (only a car). The third subtest repeats the second subtest with the addition of visual distractors. The fourth subtest presents two center targets and the participant must indicate whether these targets are identical or different. The test–retest reliability (r = .808) and validity of UFOV scores obtained from PC versions of the test are sufficient for use with older adults (Edwards, Vance, et al., 2005). Participants needed to exhibit a speed of processing deficit (combined UFOV subtests 3 and 4 score ≥ 800 or a subtest 2 score ≥ 150), allowing for potential improvement with training, for inclusion in the study (for further details, see Edwards, Wadley, et al., 2005). A composite score of performance across subtests was used in analyses as is standard practice.
Procedure
Participants eligible for training were randomly assigned to a SOPT group (n = 120) or a social contact-control group, which received Internet training (n = 108). Participants completed the training in groups of two or three persons and were led by a trainer in brief discussions and computer exercises. Over 6 weeks, participants completed 10 training sessions, which were 1 hr in duration (Edwards, Wadley, et al., 2005). Immediately following either training condition, cognitive abilities were reassessed for all participants.
Regression analysis was used to test the association of self-efficacy at baseline with responsiveness to SOPT. The primary outcome of SOPT is UFOV performance. As an indicator of responsiveness to SOPT, we computed the difference in UFOV composite scores between baseline and post-test (Ball et al., 2007). An interaction term between baseline general self-efficacy and training condition was added to the model to determine whether general self-efficacy moderates training gains. Thus, training condition, self-efficacy, and an interaction between these conditions were examined as indicators of change in UFOV from pre- to post-training. All analyses were performed using IBM SPSS Statistics Version 20.
Results
Two hundred eleven participants completed training and post-test. There were 17 participants not included in analysis due to dropout and 1 participant did not complete UFOV at post-test. Of the 18 participants not included in the final analyses, 13 participants were randomized to the control group and 5 to the experimental group. To examine if there were any differences between participants included in the final analyses and those excluded, baseline self-efficacy and UFOV scores were compared between the groups utilizing Multivariate Analysis of Variance (MANOVA). The MANOVA revealed no significant differences between participants across baseline measures of interest, Wilks’s Λ = .985, F(2, 225) = 1.66, p = .19, partial η2 = .02. Participants (n = 210) who had no missing data for their baseline self-efficacy or UFOV scores were included in analyses. Approximately 72% of participants completed all 10 training sessions. On average, participants in both training conditions completed 9.3 sessions.
To examine if there were any baseline differences between the control and SOPT conditions in self-efficacy, UFOV baseline score, age, education level, MMSE score, or far visual acuity, the groups were compared utilizing a MANOVA. The MANOVA revealed no significant differences between the two groups across baseline measures, Wilks’s Λ = .003, F(5, 222) < 1, p = .978. At baseline, participants in the control group had an average self-efficacy score of 15.41 (SD = 2.85) and participants in the SOPT group had an average of 15.02 (SD = 3.29). A chi-square test of independence was conducted to analyze potential differences in gender or race between the two training groups at baseline. Results showed that the groups did not differ in gender, χ2 (1, N = 228) < 1, p = .989, or race, χ2 (2, N = 228) = 3.454, p = .178.
Results of the regression analyses are presented in Table 2. In both models, the dependent variable was responsiveness to SOPT as modeled by the change in pre- to post-test UFOV scores. In the base model (Model 1), only training condition (SOPT vs. control) was entered as an independent variable, R2 = .344, F(1, 208) = 108.839, p< .001. In this model, training group was a significant predictor of responsiveness to SOPT, β = −.586, p< .001, indicating that UFOV improves following SOPT. In Model 2, two additional independent variables, baseline general self-efficacy and an interaction term between baseline general self-efficacy and training condition, were added to the base model. A significant interaction would indicate that general self-efficacy moderates gains from training. Results indicated, however, that the addition of self-efficacy and the self-efficacy by training group interaction did not reliably improve the model, R2 = .346, F(3, 206) = .463, p = .630. This pattern of results suggests that approximately a third of the variability in responsiveness to SOPT is predicted by training group assignment. Baseline general self-efficacy and the interaction between self-efficacy and training group do not significantly contribute to participants’ responsiveness to SOPT. General self-efficacy does not moderate SOPT gains.
Hierarchical Regression Analysis Results for Variables Predicting Responsiveness to Speed of Processing Training in SKILL Study (N = 228).
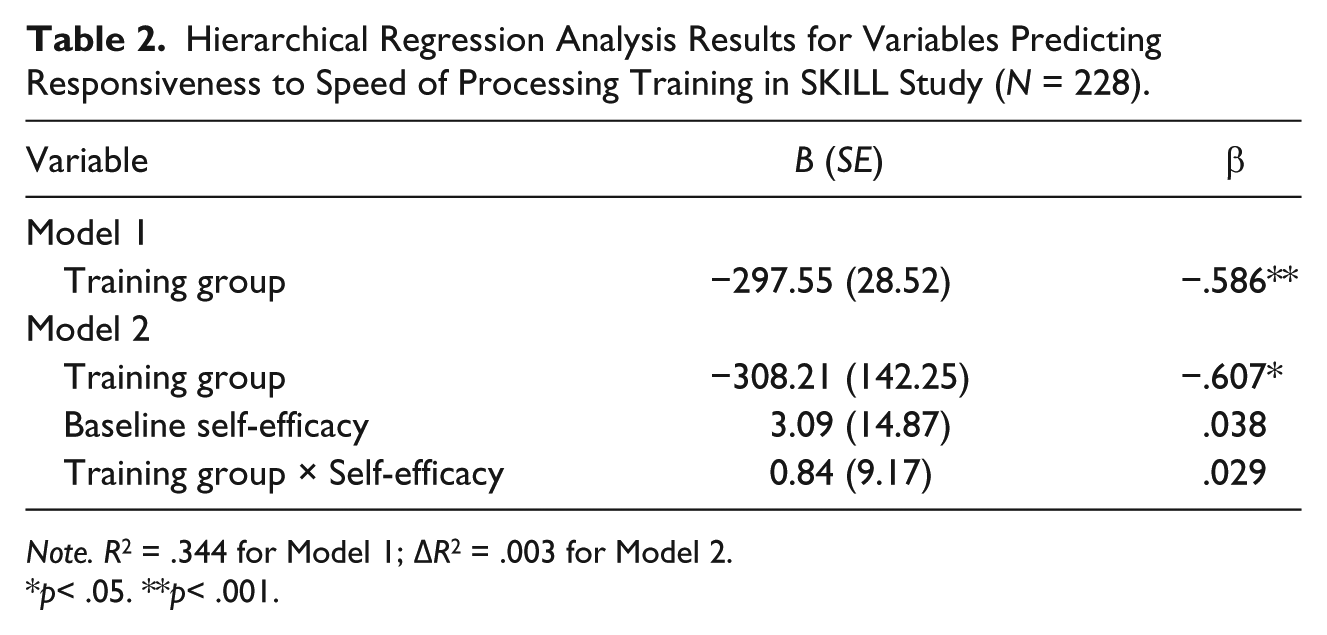
Note. R2 = .344 for Model 1; ΔR2 = .003 for Model 2.
p< .05. **p< .001.
Study 2: ACTIVE
Method
Participants
Participants for analyses were obtained from the ACTIVE study, which included 2,802 non-institutionalized older adults in training. Participants were recruited from six different field sites: the University of Alabama at Birmingham, the Hebrew Rehabilitation Center for Aged in Boston, Indiana University, John Hopkins University, Pennsylvania State University, and Wayne State University (Jobe et al., 2001). The strategies employed for recruitment varied by site, and included the use of on-site presentations, newspaper advertisements, letters, and follow-up phone calls for interested older adults (Jobe et al., 2001).
Inclusion for participation in this study was based on the following criteria: a MMSE score of 23 or higher, the ability to perform activities of daily living (ADLs), visual acuity score of 20/50 or better, no present medical conditions preventing completion of all phases of the trial, no recent cognitive training, and availability to complete all testing and training phases of the study (for further detail, see Ball et al., 2002). The aforementioned criteria were chosen to ensure ability to participate in training interventions and potentially benefit from the study. The ACTIVE study initially randomized 2,832 individuals between the ages of 65 and 94 for participation in three training groups (memory training, reasoning training, and speed training) and one control group (Jobe et al., 2001). For the purpose of this study, 1,400 participants included in the speed training (n = 702) and the control (n = 698) groups were used for analysis.
The mean age of the 1,400 included participants was 73.73 years (SD = 5.92, 65-94 years), a majority of participants were female (75.1%) and Caucasian (73.1%). The average years of education for included participants was 13.51 (SD = 2.70). From these groups, attrition of participants was due to death, withdrawal from study, and incompletion of assessments, providing a final sample for analysis comprised of 1,383 participants (Jobe et al., 2001). Descriptive characteristics of the study sample are summarized in Table 3 by training condition.
Demographic Characteristics of ACTIVE Study Participants.
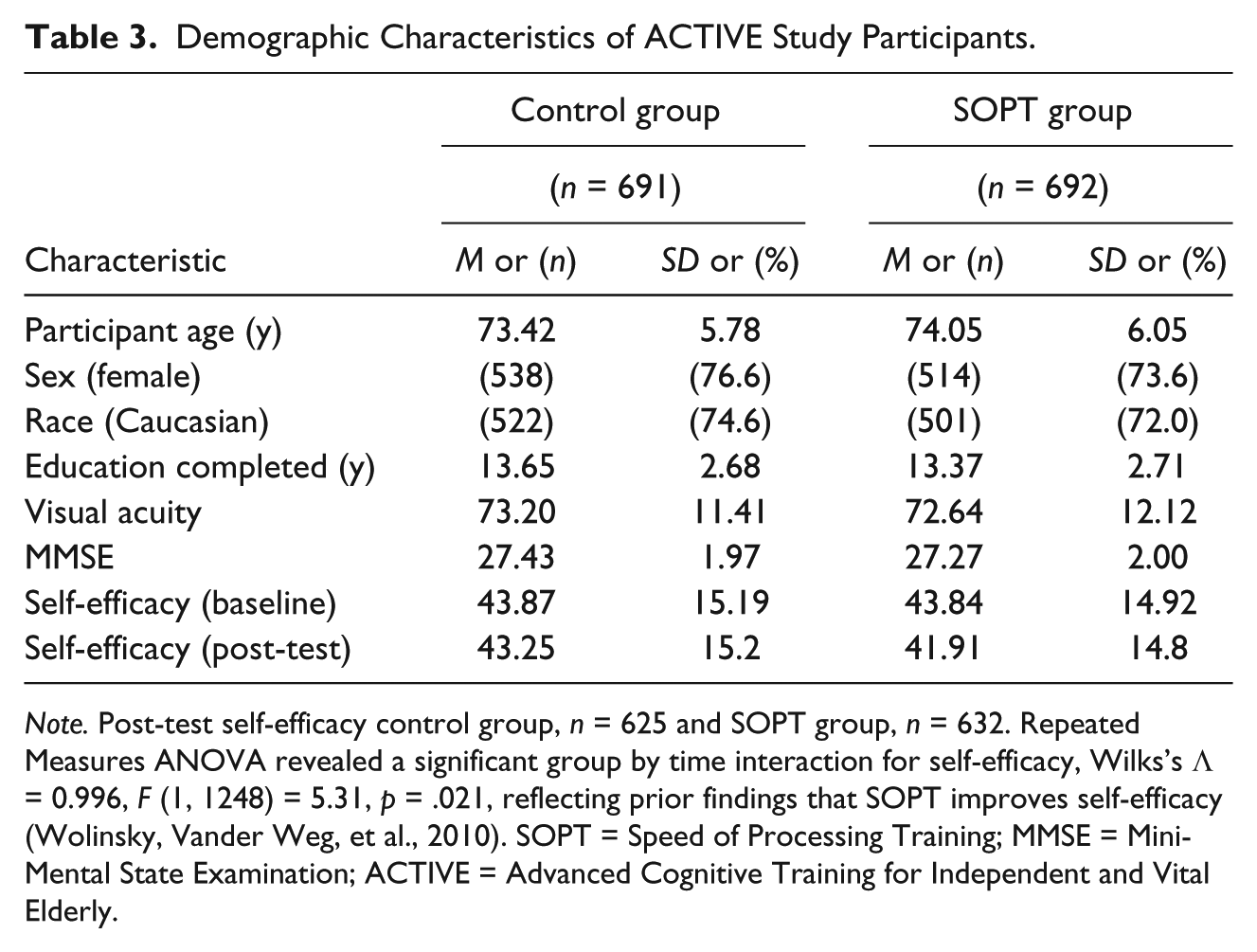
Note. Post-test self-efficacy control group, n = 625 and SOPT group, n = 632. Repeated Measures ANOVA revealed a significant group by time interaction for self-efficacy, Wilks’s Λ = 0.996, F (1, 1248) = 5.31, p = .021, reflecting prior findings that SOPT improves self-efficacy (Wolinsky, Vander Weg, et al., 2010). SOPT = Speed of Processing Training; MMSE = Mini-Mental State Examination; ACTIVE = Advanced Cognitive Training for Independent and Vital Elderly.
Measures
Inclusion measures and assessments of self-efficacy and cognitive speed of processing were selected for data analyses. Further details and rationalization for the measures chosen for the ACTIVE study can be found elsewhere (Jobe et al., 2001).
Mental status
The MMSE was used to assess mental status, and decrease the potential of including participants with substantial declines in cognitive function as described in Study 1. Scores of 23 or higher were required for inclusion in the study.
Far visual acuity
Visual acuity was evaluated as in Study 1. Visual acuity was used to assess the severity of sensory losses, which would limit the ability to effectively complete the various study measures (Jobe et al., 2001). All participants were required to demonstrate a Snellen acuity score of 20/50 or better.
Self-efficacy
Cognitive specific self-efficacy was measured using the Personality in Intellectual-Aging Contexts (PIC) inventory. The PIC inventory measures self-assessments of cognitive competence and beliefs about intellectual functioning (Lachman, Baltes, Nesselroade, & Willis, 1982). The PIC inventory examines six dimensions of personality in cognitive contexts, including locus of control (internal, chance, and powerful others), achievement, anxiety, and morale (Lachman et al., 1982). The test–retest reliability of all PIC scales ranges from .74 to .88 (Lachman et al., 1982). In efforts to reduce participant burden, the ACTIVE study used a modified version of the PIC inventory, with three dimensions including six cognitively specific items, which were scored using a six-point Likert scale (Sartori et al., 2012). A prior study utilized the locus of control dimension of personality (e.g., internal, chance, powerful others) to examine an individual’s capabilities and beliefs about control over intellectual processes for everyday situations (Sartori et al., 2012). Participants rated each item from strongly agree (1) to strongly disagree (6), with scores on each scale having a possible range of 6 to 36. Higher scores represent lower self-efficacy (Sartori et al., 2012), except for the internal scale, in which higher scores reflected higher self-efficacy. The internal scale was reverse scored and a composite score was then computed by summing the scores from the three scales. Prior studies have similarly used composites of these scales (Lachman, Steinberg, & Trotter, 1987; Miller & Gagne, 2005). Examples of the questions provided include (a) “I know if I keep using my memory I will never lose it” (internal), (b) “My problem solving ability depends on how healthy I am” (chance), and (c) “I would have to ask a salesperson to figure out how much I’d save with a 20% discount” (powerful others; Lachman, 1986).
Speed of processing
Cognitive speed of processing was assessed with the same measure, the UFOV Test, used in Study 1. This is the primary outcome that SOPT is designed to improve (Ball et al., 2007). Unlike Study 1, UFOV difficulties were not inclusion criteria.
Procedure
Participants included individuals randomized to the SOPT group (n = 692) or no-contact control group (n = 691). Participants completed SOPT in groups of three or four persons as in Study 1. Over 6 weeks, participants completed 10 training sessions, which were between 60 to 75 min in duration (Jobe et al., 2001). Following either condition, cognitive abilities and self-efficacy were reassessed for all participants.
Statistical analyses
As in Study 1, regression analysis was used to test the association of self-efficacy at baseline with responsiveness to SOPT. The outcome of interest was UFOV gain, which was computed by the difference in UFOV scores between baseline and post-test. Independent variables were training group, self-efficacy, and the interaction between training group and self-efficacy. A significant interaction would indicate that general self-efficacy moderates gains from training.
Mediation analysis was also conducted to determine whether change in self-efficacy from pre- to post-test mediated responsiveness to SOPT as determined by the change in pre- to post-test UFOV scores. Bootstrap analysis was used to test a simple mediation model of X→M→Y (where X was training condition—SOPT or control, M was the change in self-efficacy scores from pre- to post-test, and Y was the change in UFOV scores from pre- to post-test). Bootstrapping was used, which is a powerful method for testing mediation because inferences are based on the indirect effect and are not influenced by the sampling distribution (Hayes, 2009). Bootstrap estimates were based on 5,000 bootstrap samples (Hayes, 2009). The mediation model utilized is displayed in Figure 1. The results of the analysis show the total effect of the model indicated by path c predicting X→Y. The direct effect of training is shown by path c’ (Hayes, 2009). In the mediation model, path a reflects the model prediction for X to M, whereas path b shows the model prediction for M to Y (Hayes, 2009). All analyses were performed using IBM SPSS Statistics Version 20.
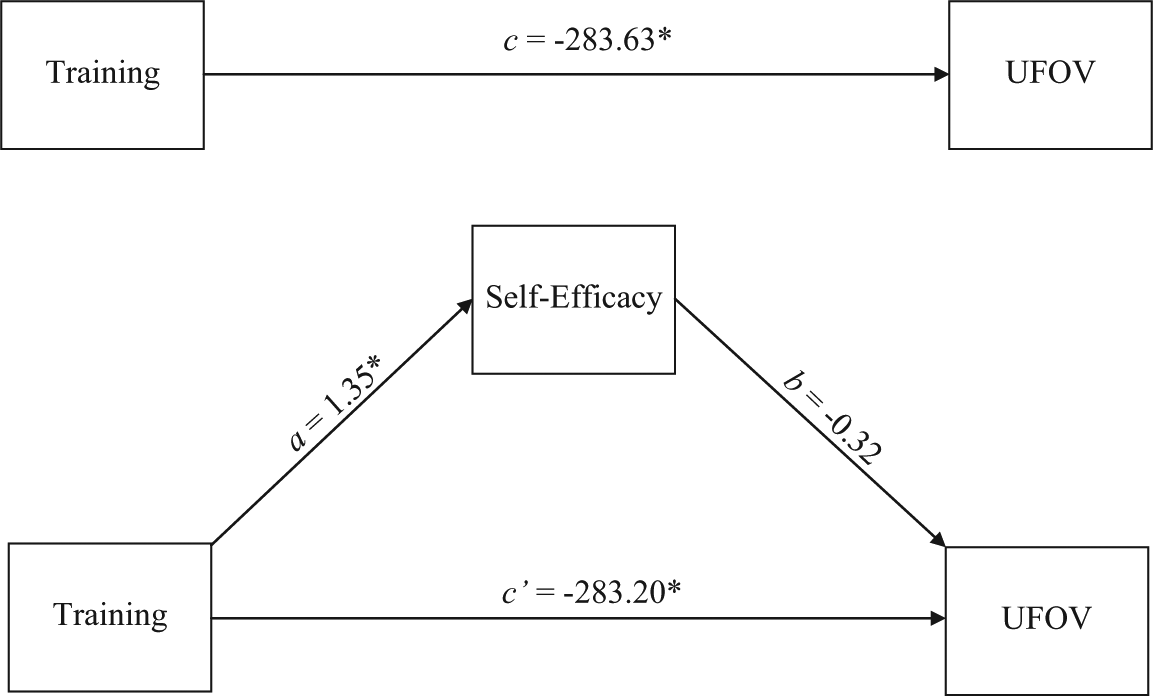
Simple mediation model with self-efficacy as the mediator.
Results
Baseline differences in self-efficacy, UFOV, age, education, MMSE score, and visual acuity between the control and SOPT conditions for the ACTIVE participants were examined using MANOVA. The MANOVA revealed no significant differences between the two groups across baseline measures, Wilks’s Λ = .007, F(6, 1356) = 1.657, p = .128. The reported average self-efficacy for participants in the control group was 43.87 (SD = 15.19) and the SOPT condition was 43.84 (SD = 14.92). A chi-square test of independence was examined to analyze potential differences in race or gender between the two conditions at baseline. Results indicated that the groups did not differ in race, χ2 (4, N = 1,396) = 3.554, p = .470, or gender, χ2 (1, N = 1,400) = 1.686, p = .194.
Results of the regression analyses to examine self-efficacy as a moderator of SOPT gains are presented in Table 4. Consistent with the analysis from Study 1, the dependent variable was the responsiveness to SOPT as determined by the change in pre- to post-test UFOV scores. In Model 1 (base model), only training condition (SOPT vs. control) was entered as an independent variable, R2 = .340, F(1, 1236) = 637.77, p< .001. In this model, training group was a significant predictor of responsiveness to SOPT, β = −.583, p< .001, reflecting that UFOV improves following SOPT. In Model 2, baseline self-efficacy and an interaction term between baseline self-efficacy and training condition were added. Results indicated that the addition of self-efficacy and the interaction term did not reliably improve the model, R2 = .346, F(3, 1234) = .323, p = .724. These results suggest that baseline self-efficacy and the interaction between self-efficacy and training group do not significantly contribute to participants’ responsiveness to SOPT. Approximately a third of the variability in responsiveness to SOPT is accounted for by training. Self-efficacy at baseline does not moderate SOPT gains.
Hierarchical Regression Analysis Results for Variables Predicting Responsiveness to Speed of Processing Training in ACTIVE Study (N = 1,237).
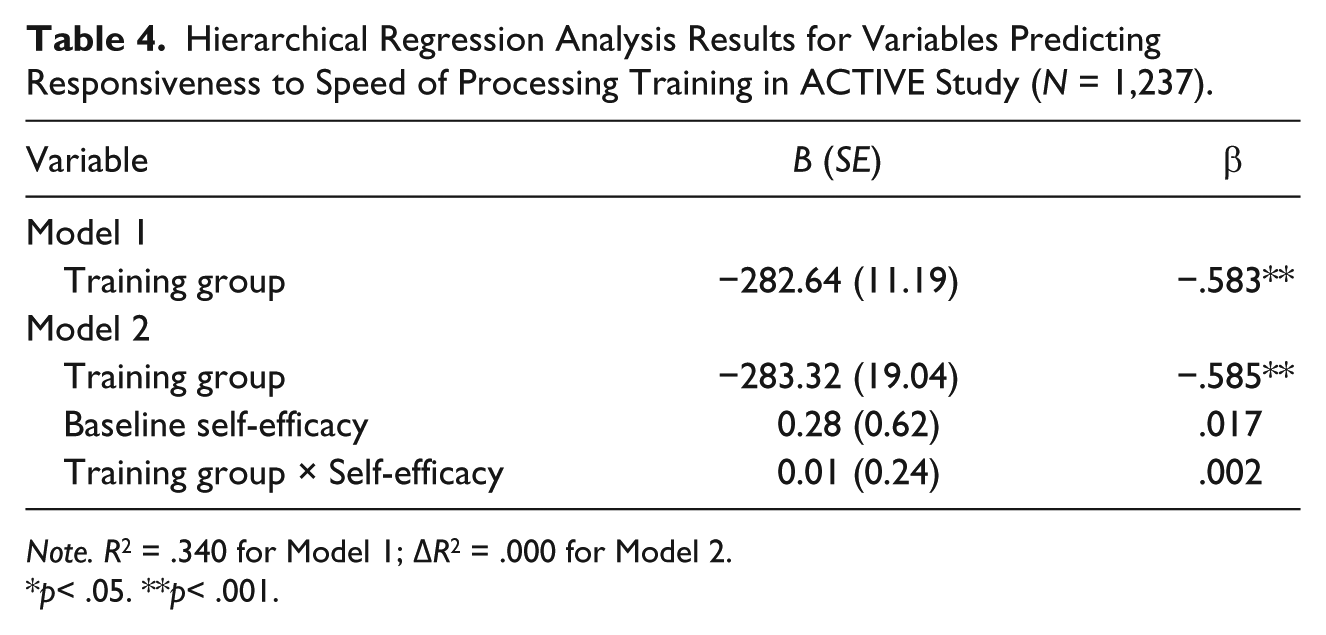
Note. R2 = .340 for Model 1; ΔR2 = .000 for Model 2.
p< .05. **p< .001.
As shown in Figure 1, results of the mediation demonstrated that the total effect (path c) of SOPT on UFOV gain was significant, c = −283.63, t(2, 1211) = −25.04, p< .05. In addition, the model’s a path (the direct effect of training on self-efficacy) was significant, t(2, 1211) = 2.44 and p = .02. However, the b path indicating the direct relationship between self-efficacy and UFOV scores was not significant, p = .58. The direct effect of training on UFOV performance as shown by c’ was significant, t(2, 1211) = −24.93 and p< .05. The indirect effect of self-efficacy on change in UFOV performance from pre- to post-test was calculated by multiplying the point estimate a path × point estimate b path, which is denoted by ab (Preacher & Hayes, 2004). The indirect effect of the change in self-efficacy from pre- to post-test did not significantly mediate change in UFOV scores, with point estimates (ab) of −.46 and 95% confidence intervals (CIs) of [−2.27, 1.07].
Discussion
The present study examined whether responsiveness to SOPT is moderated by general or cognitive specific self-efficacy among older adults, and whether cognitive specific self-efficacy mediates SOPT gains. The findings in this study indicate that responsiveness (moderator) to or effectiveness (mediator) of SOPT is not related to self-efficacy. Similarly, Edwards, Hauser, et al. (2013) found that SOPT did not improve cognitive self-perceptions, as measured by perceptions of cognitive and everyday functioning. However, with regard to memory training, higher specific self-efficacy scores are associated with greater memory training gains (West et al., 2008). Similarly, S. McDougall and House (2012) showed that cognitive self-perceptions were related to training gains (Nintendo DS Brain Training) in short-term/working memory, but were not associated with training gains in other cognitive abilities.
Self-efficacy may not affect response to SOPT because it is a process-specific cognitive intervention. Process-specific cognitive interventions target basic fluid abilities and involve perceptual practice that is procedural in nature (Lustig, Shah, Seidler, & Reuter-Lorenz, 2009; Wolinsky, Mahncke, et al., 2010). Strategy-based cognitive training programs, however, are declarative in nature and teach specific strategies to improve cognitive performance on a particular task (such as the use of a mnemonic to enhance memory). In comparing SOPT with other strategy-based approaches, Wolinsky, Mahncke, et al. (2010) point out that SOPT differs in that it involves “sensory-motor elaboration and repetition” as opposed to the explicit strategy application employed in other cognitive training techniques. Although self-efficacy affects responsiveness to memory and reasoning training, self-efficacy may not moderate or mediate responsiveness to SOPT, which is a fundamentally different cognitive training approach.
The influence of self-efficacy on cognitive training gains may vary for different cognitive abilities as well as for strategy versus process-based cognitive training approaches. Verhaeghen (2011) demonstrated that cognitive speed of processing accounted for the majority of variance in complex cognition (including episodic memory, reasoning, and spatial ability), executive function, and short-term/working memory among older adults. Thus, cognitive speed of processing could be considered a very basic/core cognitive ability that is not affected by self-efficacy. Process-based training techniques attempt to improve participants’ component abilities such that transfer of training may occur (Lustig et al., 2009). Such component abilities may be less likely to be affected by psychological beliefs than complex cognition.
Interestingly, other analyses from ACTIVE examined whether SOPT has the ability to improve participants’ cognitive specific self-efficacy (Wolinsky, Vander Weg, et al., 2010) as indicated by locus of control (Bandura, 1989). Results demonstrated that SOPT resulted in improved internal locus of control (i.e., ability to direct one’s own life). Furthermore, SOPT served as a protective factor against substantial decline in chance locus of control (i.e., outside forces controlling one’s life; Wolinsky, Vander Weg, et al., 2010). In the current study, we additionally examined each subscale of self-efficacy, as potential moderators and mediators, but analyses yielded the same results as when examining self-efficacy as a composite measure. Thus, SOPT may enhance general or specific self-efficacy, but self-efficacy is unrelated to benefits from SOPT.
Limitations of the present study should be considered. The self-efficacy measures available for these secondary data analyses were limited, and were not specific to cognitive speed of processing. In Study 1, we had only a general self-efficacy measure. As previously noted, the test–retest reliability of the self-efficacy measure used in Study 1 was low (i.e., .50-.64). We only measured self-efficacy at baseline, so the low test–retest reliability is unlikely to have affected Study 1 results. However, replication of findings with more reliable measures of self-efficacy is warranted. In Study 2, self-efficacy was specific to cognitive abilities, but not cognitive speed of processing in particular. Similarly, the PIC, which was used in Study 2, measures self-efficacy in relation to individual attributions and capabilities (Lachman et al., 1982). In the future, use of multiple self-efficacy scales to provide a clear differentiation between perceived cognitive abilities and individual attributions, as well as use of self-efficacy measures more specific to cognitive speed of processing, is needed to better understand the relationship between self-efficacy and responsiveness to SOPT. To our knowledge, there are no existing speed-of-processing-specific measures of self-efficacy. It is possible that different results would be found with such a measure. The results of these analyses are most generalizable to community-dwelling older adults residing in the eastern regions of the United States rather than other geographic regions or facility-based settings. Future research with larger sample size and more varied measures of self-efficacy is needed to confirm these findings.
While it has been demonstrated elsewhere that self-efficacy predicts participants’ ability to perform certain tasks (e.g., physical exercise, memory training; McAuley et al., 2011; West et al., 2008), there does not appear to be any predictive value when analyzing cognitive gains from SOPT. Ball et al. (2007) examined other predictors of SOPT gains from six different studies. The results showed weak but significant (rs < .17) relationships between training gain and education, mental status, and age. Thus, these factors account for very little variance in SOPT responsiveness. Overall, it remains unclear what moderates gains from SOPT. Only one prior study has examined mediators of SOPT. This study indicated that improvements in divided attention significantly mediated the effect of SOPT on Timed Instrumental Activities of Daily Living (TIADLs) performance (Edwards, Ruva, O’Brien, Haley, & Lister, 2013).
Given the value of increased speed of processing in older adults and the transfer potential of SOPT to IADL, including driving, health-related quality of life, and depressive symptoms (Ball et al., 2010; Edwards, Delahunt, & Mahncke, 2009; Edwards, Wadley, et al., 2005; Wolinsky et al., 2006; Wolinsky et al., 2009), future studies analyzing predictors of SOPT responsiveness are worthwhile endeavors to potentially improve the everyday lives of older adults.
Footnotes
Acknowledgements
The authors also wish to acknowledge Dr. Karlene K. Ball, who was awarded the MERIT grant to conduct the Staying Keen in Later Life (SKILL) study, and the investigators of SKILL, Drs. Daniel Roenker, Lesley Ross, David Roth, Virginia Wadley, and David Vance. We also thank the staff and students of the University of Alabama at Birmingham Center for Translational Research on Aging and Mobility. The authors would also like to acknowledge the Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) principal investigators, including Hebrew Senior Life (U01 NR04507)—John N. Morris, PhD; Indiana University School of Medicine (U01 NR04508)—Frederick W. Unverzagt, PhD; Johns Hopkins University (U01 AG14260)—George W. Rebok, PhD; New England Research Institutes (Data Coordinating Center; U01 AG14282)—Sharon L. Tennstedt, PhD; Pennsylvania State University (U01 AG14263)—Sherry L. Willis, PhD; University of Alabama at Birmingham (U01 AG14289)—Karlene K. Ball, PhD; University of Florida/Wayne State University (U01 AG014276)—Michael Marsiske, PhD; National Institutes of Health—Kathy Mann Koepke, PhD; and National Institute on Aging—Jonathan King, PhD.
Authors’ Note
Dr. Rebok is an investigator with Compact Disc Incorporated for the development of an electronic version of the ACTIVE memory intervention. Dr. Marsiske has received support from Posit Science for another research project using Insight program licensure. Dr. Ball owns stock in the Visual Awareness Research Group and Posit Science, Inc., the companies that market the Useful Field of View Test (UFOV) test and speed of processing training software (now called Insight). Posit Science acquired visual awareness, and Dr. Ball continues to collaborate on the design and testing of these assessments and training programs as a member of the Posit Scientific Advisory Board. Dr. Edwards worked as a limited consultant to Posit Science from June to August 2008.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the National Institutes of Health/National Institute on Aging Grant 5 R37 AG05739-16, Improvement of Visual Processing in Older Adults, Karlene K. Ball, principal investigator.