
Abstract
Introduction
During the last few decades, a significant increase in worldwide prevalence of chronic non-communicable diseases such as hypertension has occurred (Centers for Disease Control and Prevention [CDC], 2013; World Health Organization [WHO], 2013). The demographic transition has resulted in rapid aging of the population worldwide. This explains, in part, the increased prevalence of such conditions. In addition, the adoption of unhealthy lifestyles resulting in less balanced diets and decreased physical activity also adds to this raising prevalence (Arredondo & Zuniga, 2006; He et al., 1991). Furthermore, developing countries in Latin America are experiencing an abnormally rapid demographic transition, where hypertension is strongly associated with premature deaths caused by stroke and coronary heart disease, (Yusuf et al., 2004) resulting in poor overall health and higher health care expenses (Kearney et al., 2005). This highlights the importance of prevention and early detection of hypertension (Mancia et al., 2007).
The 10/66 Group reported the prevalence of hypertension in those aged 65 and older in some Latin American populations between 42% and 80% (Prince et al., 2012). This study, however, did not include Colombia. Another study reported hypertension prevalence rates in Bogotá of 13.4% for a cohort of adults between 25 and 64 years of age (Hernandez-Hernandez et al., 2010). Other studies have reported prevalence rates between 12.0% and 33.9% in other cities in Colombia, and only 28.3% of respondents reported adequately controlled blood pressure. (Bautista et al., 2002; Intersalt, 1988; Naranjo, 1994; Newman & Herrera, 1993) These studies however are limited to selected cohorts in a small city in Colombia and include younger age groups. In addition, these reports vary by year, some in the late 1990, some in the early 2000, and some in the last 5 years; definitions of hypertension and guidelines have significantly changed in this time period.
Colombia, like most Latin American countries is rapidly aging. Unfortunately, there are limited data available to inform policy makers on the magnitude of the problem and the likely consequences of ignoring the fast increase in chronic diseases like hypertension. The association between age and hypertension has been widely described in many epidemiological studies (Bautista et al., 2002; Drizd, Dannenberg, & Engel, 1986), however, lack of data in Colombia focused on older adults has prevented researchers from providing more detailed information, limiting public health efforts to prevent, better diagnose, and treat hypertension among older adults in Colombia. In addition, researchers have shown that when hypertension is present in older adults with other non-communicable diseases such as diabetes mellitus, depression, and joint diseases, the risk of complications, disability, and use of health services are significantly increased (Fultz, Ofstedal, Herzog, & Wallace, 2003). This highlights the importance of understanding hypertension to better manage older adults suffering from it.
With this in mind, we wanted to estimate the prevalence of hypertension in a cohort of 2,000 adults aged 60 years and older who were interviewed in 2012 for the SABE Bogotá study. In addition to determining the prevalence of hypertension, we also wanted to identify the sociodemographic and health factors associated to hypertension as a first step toward informing health policy on factors where interventions can be designed to prevent and manage high blood pressure. The current manuscript summarizes these findings and discusses the implications for future interventions that can improve older adult health in Colombia.
Method
Sample and Design
Data were taken from the SABE Bogotá Study, a cross-sectional study conducted in 2012, in urban and rural areas of the city of Bogotá, Colombia. The sample was collected by multistage clusters (sectors, sub-sections of neighborhoods, blocks, and sets of 10 houses). A correction factor was used to obtain a statistical confidence of 95%. Of all individuals invited to participate, 81.9% agreed for a total of 2,000 participants. This population was statistically representative of 779,534 aged 60 years and older and living in the city of Bogotá in 2012.
The survey included 11 main topics: (a) identification of the house and the older adults to be interviewed, (b) house and home characteristics, (c) personal and family data, (d) violence experiences, (e) cognitive status, (f) health status, (g) characterization and causes of disabilities, (h) functional evaluation, (i) medication usage and health care access, (j) anthropometric measures and execution measures, and (k) health, disease, and a social history framework (biographical component). All respondents signed an informed consent to participate in the study. The informed consent, the survey questionnaire, and all study materials were approved by the ethics committee at Pontificia Universidad Javeriana.
Variables
Dependent variable
Hypertension is the dependent variable. There are two indicators for hypertension: self-reported and measured blood pressure. For the self-reported hypertension, respondents were asked, “Has a doctor or a nurse told you that you have high blood pressure?” Respondents answered either yes or no. Those with an affirmative response were then asked, “How do you control your hypertension?” Respondents could select from the following four choices: medications, diet, exercise, or nothing.
Blood pressure was measured with an automatic blood pressure monitor (OMRON, model HEM 7113) following guidelines previously published for blood pressure measurement in community-based studies (Vera-Cala, Orostegui, Valencia-Angel, Lopez, & Bautista, 2011). Uncontrolled hypertension was defined as having a blood pressure ≥150/90 mmHg among participants who self-reported hypertension, based on the recommendations of the 8th Report of the Joint National Committee (James et al., 2014). Undiagnosed hypertension was defined as having a blood pressure ≥150/90 mmHg among participants who self-reported no hypertension. Untreated hypertension was defined as having a blood pressure ≥150/90 mmHg and reporting no use of antihypertensive medication (only among those with self-reported hypertension who were then asked how they control hypertension; Prince et al., 2012; Wright, Hughes, Ostchega, Yoon, & Nwankwo, 2011). Life-style changes such as diet and exercise as treatment options for hypertension control were not thoroughly evaluated in the study so they are not included as part of the definition of the dependent variable.
Independent variables
Sociodemographic variables included were age (years), gender, education (years), and health insurance. In Colombia, health coverage is universal. All employees and their families belong to the contributive system where employers and employees contribute to health care coverage with different percentages. Unemployed individuals, self-employed individuals, and those working part-time get a subsidy from the government and belong to the subsidized system. There are still some individuals who have no insurance and some others who belong to special insurance regimes. Therefore, in the SABE Bogotá study, four insurance categories were included: contributive, subsidized, none, or other. For the current study, “none” and “other” were combined into a single category. Education was categorized according to the Colombian education system as: none (0 years), primary (1-5 years), secondary (high school, 6-11 years), and higher education (more than 12 years).
Four medical conditions were included in the analyses: diabetes, coronary heart disease, congestive heart failure, and stroke. Respondents were asked, “Has a doctor or a nurse told you that you have . . .?” for each of the conditions previously listed.
Physical activity was evaluated with the following question: “During the past 7 days, how often did you . . .?” The following options were provided: walk, do light exercise, do moderate exercise, or vigorous exercise. Responses were grouped into three categories: 1-2 days a week, 3-4 days a week, or 5-7 days. Scores for every activity were added and a total physical activity variable was created. Then, tertiles were estimated for all informants and categorized as having low, medium, or high levels of physical activity.
Self-rated health was evaluated by the following question: “Would you describe your health as: 1= excellent, 2 = very good, 3 = good, 4 = fair, or 5 = bad?” This variable was dichotomized as good health (Categories 1, 2, & 3; code = 0) versus poor health (Categories 4 & 5; code = 1).
Smoking was divided into three categories: 1 = never smoked; 2 = smoked before, but is not currently a smoker; and 3 = currently a smoker. It was then dichotomized as not currently smoking (Categories 1 & 2; code = 0) versus current smoker (Category 3; code = 1). Alcohol consumption was evaluated with the following question: “How often do you drink alcoholic beverages?” 1 = never, 2 = less than once per week, 3 = two or more days per week. It was then dichotomized as never (Categories 1 & 2; code = 0) versus any consumption (Category 3; code = 1).
Anthropometric measures included were weight (kg), height (m), waist circumference (cm), and body mass index (BMI; calculated by dividing the weight by the height2). The instruments for anthropometric measurement were electronic calibrated scales (brand Seca ref. 813), stadiometers (brand Seca ref. 206), and meter tapes (fiberglass made with rewind button, measuring capacity between 0-150 mm and 0-60 inches). BMI was categorized as <30 kg/m2, ≥30 kg/m2 (obesity), and missing. Waist circumference was categorized as lower (<102 cm in men and <88 cm in women), higher (abdominal obesity, ≥102 cm in men and ≥88 cm in women), and missing (Grundy et al., 2006).
Statistical Analysis
To adjust for sampling survey design, data were weighted by using complex survey analyses. Weighted percentages were used to present the prevalence of self-reported hypertension, uncontrolled hypertension, and untreated hypertension by age, in the overall population and by gender, and differences were tested by Wald chi-square (using the SURVEYFREQ procedure in SAS software).
To describe modalities for treatment of self-reported hypertension, weighted percentages were used. To see differences on prevalence for self-reported hypertension, uncontrolled hypertension, undiagnosed hypertension, and untreated hypertension, categorical independent variables are presented with unweighted frequencies and weighted percentages, similarly to other SABE studies (Reyes-Ortiz, Velez, Camacho, Ottenbacher, & Markides, 2008), and differences were tested by the Wald chi-square. Selection of independent variables for the multivariate analysis was performed based on the associations in the bivariate analysis, clinical relevance, and previous studies (AlGhatrif et al., 2011; Munaretti, Barbosa, Marucci Mde, & Lebrao, 2011; Rodrigues Barbosa, Balduino Munaretti, Da Silva Coqueiro, & Ferreti Borgatto, 2011; Rodrigues Barbosa & Ferreti Borgatto, 2010). For the multivariate analyses, weighted logistic regression models (SURVEYLOGISTIC procedure in SAS software) were used to test the association with hypertension (yes = 1, no = 0), uncontrolled hypertension (yes = 1, no = 0), and untreated hypertension (yes = 1, no = 0), and obtaining odds ratios (ORs) with 95% confidence intervals (CI). Because of missing values for both BMI and waist circumference, the results for other variables might be affected, we therefore only provide complete multivariate models without those two variables. We made additional separate multivariate models including either BMI or waist circumference as continuous variables because a multicollinearity problem was detected between those two variables. Data were analyzed using SAS version 9.3 for windows (SAS Institute, Cary, North Carolina, USA), statistical level of significance was set at p < .05. Figure preparation was made using SigmaPlot version 12 for windows (Systat Software Inc., San Jose, California, USA).
Results
From the original 2,000 study participants, a total of 1,999 adults were included in our study for the main analyses on self-reported hypertension, and only 1,793 adults were included for the analyses on uncontrolled hypertension, undiagnosed hypertension, and untreated hypertension because of missing values for blood pressure levels. Compared with the participants who remained in the analyses based on blood pressure measures, participants excluded due to missing data (n = 206) were more educated, had a higher frequency of contributive health insurance, better self-rated health, and higher alcohol consumption (p < .05).
Table 1 shows the prevalence of self-reported hypertension, uncontrolled hypertension, undiagnosed hypertension, and untreated hypertension by age categories and gender. The overall prevalence of self-reported hypertension was 56.9%. The overall prevalence was slightly higher for women compared with men but this difference was not statistically significant (57.8% vs. 55.4%, p = .44). An increased prevalence of hypertension was observed as age increases for both men and women (p = .002 and p < .001, respectively). The overall prevalence of uncontrolled hypertension was 28.4%, it increased with age in the total sample (p < .001) and also for women (p < .001), but no difference was observed in the overall prevalence by gender (p = .42). The overall prevalence of undiagnosed hypertension was 13.5%. The overall prevalence of untreated hypertension was 15.7% (283 out of 1,793 participants). No differences between age groups were observed in the prevalence of untreated hypertension, however, a significant gender difference was observed (18.7% vs. 13.8%, p = .036).
Prevalence of self-reported hypertension, controlled hypertension, undiagnosed hypertension and untreated hypertension by age, individuals aged 60 and older in the SABE Bogotá Study (n=1,999).
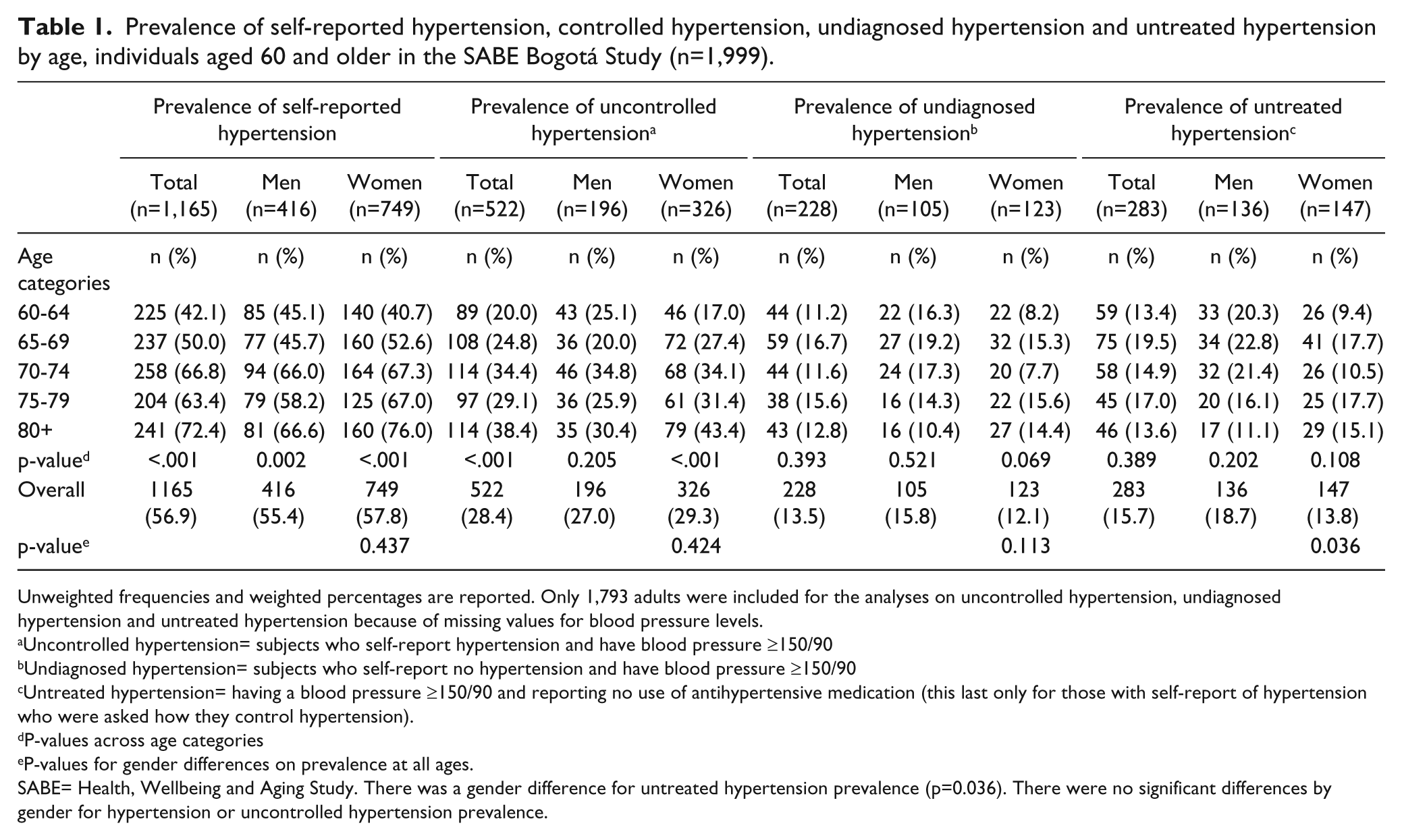
Unweighted frequencies and weighted percentages are reported. Only 1,793 adults were included for the analyses on uncontrolled hypertension, undiagnosed hypertension and untreated hypertension because of missing values for blood pressure levels.
Uncontrolled hypertension= subjects who self-report hypertension and have blood pressure ≥150/90
Undiagnosed hypertension= subjects who self-report no hypertension and have blood pressure ≥150/90
Untreated hypertension= having a blood pressure ≥150/90 and reporting no use of antihypertensive medication (this last only for those with self-report of hypertension who were asked how they control hypertension).
P-values across age categories
P-values for gender differences on prevalence at all ages.
SABE= Health, Wellbeing and Aging Study. There was a gender difference for untreated hypertension prevalence (p=0.036). There were no significant differences by gender for hypertension or uncontrolled hypertension prevalence.
In Figure 1, the treatment modalities for data for self-reported hypertension are shown. Unweighted frequencies and weighted percentages are presented. Among those with self-reported hypertension (1,165 out of 1,999 participants), 93.5% (1,065 out of 1,165) were receiving antihypertensive medication, 61.0% (720 out of 1,165) reported adherence to a healthy diet, and 41.7% (440 out of 1,165) exercised. Percentages of combined treatment modalities are significantly lower.
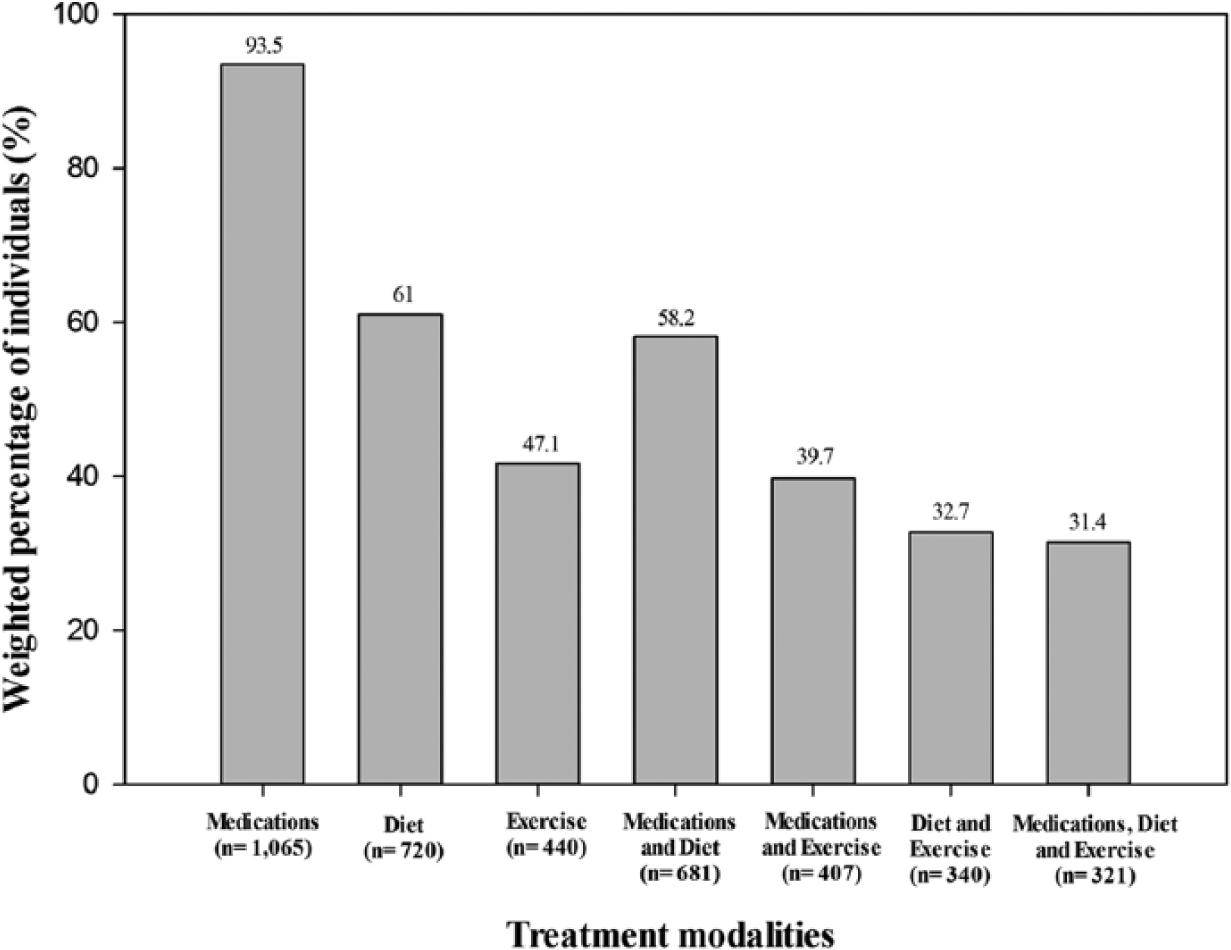
Treatment modalities for self-reported hypertension in individuals aged 60 years and older: SABE Bogotá Study (n = 1,165).
In Table 2, sociodemographic characteristics, anthropometric measures, and comorbidities are shown by hypertension status. Unweighted frequencies and weighted percentages are presented. Higher prevalence of self-reported hypertension was observed in older age, among those with lower education, and having health coverage. In addition, significantly higher prevalence of self-reported hypertension was observed for those with comorbidities such as diabetes, coronary heart disease, stroke, and congestive heart failure, as well as those reporting poor self-rated health (67.2%), not being a current smoker (58.3%), or no alcohol consumption (60.9%). Prevalence of hypertension among those in the highest tertile of physical activity was significantly lower (48.5%) compared with 56.9% in the middle tertile and 65.2% in lower tertile (p < .001). Finally, higher blood pressure was observed for those with higher BMI and waist circumference (p < .001).
Anthropometric Measures and Comorbidities by Hypertension Status, Individuals Aged 60 and Older in the SABE Bogotá Study.

Note. Physical activity variable corresponds to tertiles of the distribution. Unweighted frequencies and weighted percentages are reported. HTN = hypertension; SABE = Health, Well-being, and Aging Study.
This sample applies to uncontrolled, undiagnosed, and untreated hypertension calculations.
When analyzing the hypertension subgroups, significantly higher prevalence of uncontrolled hypertension was observed in older age, among those with lower education, having health insurance and those reporting poor self-rated health. Significantly higher prevalence of undiagnosed hypertension was observed among those without coronary heart disease or stroke (p < .001), and those reporting poor self-rated health (p = .001). Significantly higher prevalence of untreated hypertension was observed among men compared with women, among those without health insurance, those without coronary heart disease or stroke, and those reporting good self-rated health. A higher prevalence of untreated hypertension was observed for current smokers, compared with non-smokers (p < .001).
In Table 3, multivariate logistic regression analyses predicting hypertension are presented. Factors independently associated with higher odds of self-reported hypertension were older age, having health coverage (compared with none/other), reporting diabetes, heart disease, stroke, heart failure, and poor self-rated health. Two additional separated multivariate models (adjusted for all other variables in Table 3—data not shown) showed that BMI (used as continuous variable, OR = 1.07, 95% CI = [1.02, 1.10]; model with n = 1,572) and waist circumference (used as continuous variable, OR = 1.03, 95% CI = [1.01, 1.04]; model with n = 1,698) were associated with higher odds of self-reported hypertension. In comparison, more education was associated with lower odds of uncontrolled hypertension; however, this relationship was only significant for those participants with 6 to 11 years of education (high school). In addition, any type of health insurance was associated with significantly higher odds of uncontrolled hypertension, compared with those with no health insurance. For the group with undiagnosed hypertension, lower odds were found associated with having health insurance; however, this association was only significant for those with contributive health insurance. In addition, history of coronary artery disease, stroke, and those reporting poor self-rated health had significantly lower odds of undiagnosed hypertension. Finally, for the group with untreated hypertension, having health insurance was associated with lower odds of untreated hypertension, as well as those having history of stroke or those reporting poor self-rated health. Smoking significantly increased the odds of untreated hypertension.
Multivariate Logistic Regression Analyses Predicting Self-Reported Hypertension, Uncontrolled Hypertension, Undiagnosed Hypertension, or Untreated Hypertension, Individuals Aged 60 and Older in the SABE Bogotá Study.
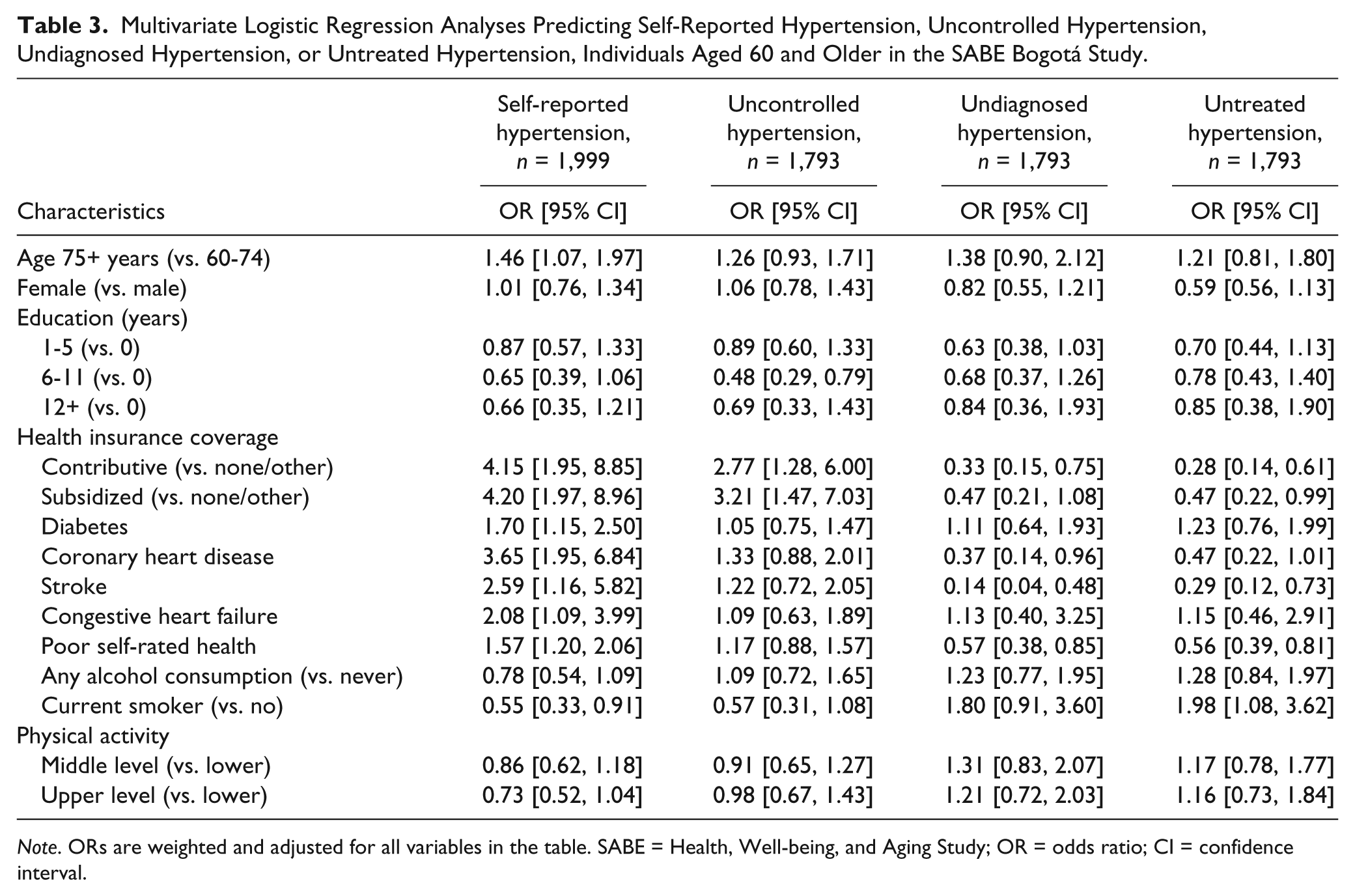
Note. ORs are weighted and adjusted for all variables in the table. SABE = Health, Well-being, and Aging Study; OR = odds ratio; CI = confidence interval.
Discussion
Although there have been previous studies describing prevalence of hypertension in other populations in Colombia (Bautista et al., 2002; Intersalt, 1988; Naranjo, 1994; Newman & Herrera, 1993), this is the first study that focuses on adults more than 60 years of age in the capital city of the country, Bogotá. Our group collected data from a representative sample of individuals of 60 years and older in the city of Bogotá. Manuscripts using data from SABE studies in other countries have successfully described epidemiological characteristics of older adults in several Latin American cities and have significantly impacted public health (Palloni & McEniry, 2007).
The current study reports a high prevalence of hypertension (56.9%), as well as a high prevalence of uncontrolled hypertension (28.4%), which corresponds, respectively, to 443,555 and 221,388 older adults in the city. Although this prevalence agrees with prevalence reports from other Latin American countries (Hernandez-Hernandez et al., 2010; Prince et al., 2012), the very high prevalence of uncontrolled hypertension and the significant prevalence of participants with untreated hypertension is alarming and a potential indicator of poor health care services that need to be addressed by policy makers to improve standards of medical treatment of highly prevalent and potentially deadly conditions such as hypertension. In addition, there is an important percentage of older adults with undiagnosed hypertension implying that despite universal health care coverage, improvements are required in primary care for prevention and early diagnosis. We also show significantly higher rates of hypertension and uncontrolled hypertension in older ages compared with younger ages as well as among women compared with men. These data agree with data reported by others on hypertension occurring mainly due to high systolic blood pressure and being more prevalent among older women compared with older men (Bautista et al., 2002; Franklin et al., 1997). Given the extant literature on adverse events related to hypertension among older adults and given that women have significantly higher life expectancy compared with men, both clinicians and policy makers need to design programs targeting risk factors and providing treatments that will improve quality of life in the long run (Acelajado & Oparil, 2009; August, 2013; Denker & Cohen, 2013; Virdis et al., 2011).
In this study, poor self-rated health was significantly related to increased odds of hypertension. Poor self-rated health has been reported as a major contributor of poor adherence to treatment and poor disease control (Idler & Benyamini, 1997). Yet many physicians forget to assess this in routine medical visits. From the policy perspective, psychological aspects of disease prevention and management are many times forgotten (Schneiderman, Antoni, Saab, & Ironson, 2001). Therefore, interventions aimed not only at disease prevention and treatment, but also at improving psychological aspects of diseases and psychological burden of diseases need to be implemented to obtain better results.
In addition, the four medical conditions included here were also related to higher odds of hypertension. A more comprehensive approach to chronic diseases in old age, both from the clinical and policy perspectives, is needed. In recent aging literature, a paradigm shift has been proposed. Given the high prevalence of older adults presenting with more than one medical condition, analysis of a single disease may not be the best approach to these individuals (Hughes, McMurdo, & Guthrie, 2013). Therefore, it has been proposed to establish a new methodical approach that allows both clinicians and researchers to analyze individuals with multiple conditions and determine the best approach for managing them (Tinetti, Fried, & Boyd, 2012). Future studies in Colombia need to explore this new approach and decide whether it provides better results for older individuals suffering from multiple conditions.
We also found a low frequency of individuals with hypertension who are current smokers. We hypothesize this could be related to the efforts made by their physicians to modify unhealthy lifestyles. However, the data presented in this study are very likely showing a health selection phenomenon in smokers, explaining the very low prevalence of smokers with hypertension, and also why the individuals that are current smokers have lower odds for hypertension. This could be due to higher mortality rates at younger ages in smokers and individuals who stopped smoking at a younger age due to health-related issues, thus showing a low prevalence of hypertension. Furthermore, this is consistent with the latter finding of higher prevalence of untreated hypertension and higher odds for untreated hypertension within smokers (Adda & Lechene, 2013; Becklake & Lalloo, 1990; Primatesta, Falaschetti, Gupta, Marmot, & Poulter, 2001). Nevertheless, alcohol drinkers may also be displaying a health selection phenomenon related to drinkers that also smoke, but also some of the cardiovascular health-related benefits of alcohol consumption, as previously reported in a large pool of studies (Ronksley, Brien, Turner, Mukamal, & Ghali, 2011). However, adults with hypertension also had higher BMI and waist circumference, which is likely associated with a greater cardiovascular disease burden. Such factors are very important and should be discussed in detail at every physician visit. Policy makers should also take these factors into account when developing interventions. Unless risk factors are targeted, the prevalence of chronic conditions such as hypertension will not significantly decrease.
Our study has some limitations. First, this is a cross-sectional study. Therefore, causality cannot be determined. Second, it is not clear if some of the comorbid conditions analyzed occurred before or after hypertension was diagnosed in the participants. Third, self-reported hypertension is used as the outcome variable. Recall bias could play an important role in our results. Fourth, our data come from a single city in the country, which could potentially introduce selection bias in our data. Fifth, we had important number of missing values (10.3%) related to the analyses using blood pressure measurements (uncontrolled hypertension and untreated hypertension) that might affect the interpretation of our results. Sixth, life-style changes such as diet and exercise that have been shown effective in hypertension treatment were not thoroughly evaluated in the study so they are not included in the definition of hypertension as treatment options. Nevertheless, our study has several strengths. We are reporting prevalence rates for self-reported hypertension in a representative sample of older adults in the capital city of Colombia, Bogotá. In addition, a good agreement between self-reported diseases and clinical diagnoses has been documented. Finally, we have used the methodology used in the original SABE study. Several published manuscripts using data from this study, which includes seven capital cities in Latin America, have contributed important data and have contributed to a better understanding of disease and disability related to aging in Latin America (Palloni & McEniry, 2007). Finally, our study provides the first data on older adults in Colombia and it will allow us to establish relationships that may inform policy makers and design useful interventions to benefit older adults.
Conclusion
The high prevalence of hypertension is an important concern among older adults in Bogotá. This group of individuals has unique social, economic, and health characteristics that differentiate them from younger age groups. Therefore, a different therapeutic approach that aims to modify socioeconomic factors and takes into account co-existence of non-communicable diseases is required. Additionally, life-style changes must be evaluated to have a better picture of hypertension treatment in Colombia. Given that the majority of adults 60 years or older suffer from hypertension, further research within this population regarding hypertension is paramount to design better health care interventions and public health policies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Administrative Department of Science, Technology, and Innovation—Colciencias, Code 120354531692 and the Pontificia Universidad Javeriana.