
Abstract
Keywords
Studies in China have consistently reported that rural older adults have higher levels of depressive symptoms than their urban counterparts (Chen, Hu, Qin, Xu, & Copeland, 2004; Chen et al., 2005; Dong & Simon, 2010; Li et al., 2011; Ma et al., 2008). A recent meta-analysis shows that the mean pooled prevalence rate of depression in rural older Chinese was 29.2%, significantly higher than it was in urban older Chinese (20.5%; Zhang, Xu, Nie, Zhang, & Wu, 2012). Most prior studies have not controlled for other factors when examining the association between rural–urban strata and late-life depression. An exception was Ma et al. (2008) who, drawing on a regional sample of older persons in Beijing, found that rural older adults were 3 times more likely to have depression than urban older adults, adjusting for age, sex, marital status, education, household income, and major medical conditions.
The pattern of rural–urban differences in depression observed among older adults in China is very different from that found in other countries (e.g., Britain, Canada, Japan, Korea, Taiwan, and the United States) where either no significant difference (Abe, Fujise, Fukunage, Nakagawa, & Ikeda, 2012; Kim, Shin, Yoon, & Stewart, 2002; St. John, Blandford, & Strain, 2006) or a rural advantage (Chiu, Chen, Huang, & Mau, 2005; Evans, 2009; Friedman, Conwell, & Delavan, 2007; Kim, Stewart, Shin, Yoon, & Lee, 2004; Walters et al., 2004) has been reported. Why is the prevalence of depression higher in rural than urban older adults in China? The current study aims to assess the extent to which a series of social and health characteristics at the individual, household, and community levels account for rural–urban differences in depressive symptoms among older Chinese. These characteristics include (a) socioeconomic status (SES), (b) health care access, (c) health status, and (d) social support and participation.
Possible Explanations for Rural–Urban Differences in Depression Among Older Chinese
First, sharp social and economic disparities exist between the rural and urban populations. Since the 1950s, China has implemented a household registration system (hukou), which requires every citizen, on birth, to register as belonging to agricultural (rural) or non-agricultural (urban) groups. The identity given by hukok is practically for life, as change of hukou, especially from rural to urban, is very difficult (Wang, 2005). While urban residents have access to a broad range of state-sponsored public goods—including jobs, subsidized housing, education, medical care, and pensions—rural residents have limited access to such community resources and opportunities as quality schools and formal employment with pension benefits. Thus, rural residents have fewer prospects for moving up the social ladder and accumulating wealth, and they are at a greater risk of poverty in old age (Cai, Giles, O’Keefe, & Wang, 2012). In addition, despite accumulation of national wealth in recent decades, development of public facilities and amenities that help to improve quality of life has been slow in rural areas (Park, 2008), which may increase sense of relative deprivation and abandonment among rural residents (Hill & Maimon, 2013). Research in the West as well as in China has demonstrated that people with low SES are vulnerable to develop depressive symptoms (Lorant et al., 2003; Ma et al., 2008). Beyond individual-level SES, studies have shown that neighborhood socioeconomic disadvantages could undermine mental health (Julien, Richard, Gauvin, & Kestens, 2012).
Second, health systems and policies for China’s urban and rural populations vary widely (Yip, 2010). Many studies have shown that rural residents were at a disadvantage regarding health care access (Liu & Griffiths, 2011; Yip, 2010). In recent years, the Chinese government has invested substantial resources to expand health insurance coverage and reduce health care disparity (Yip et al., 2012). Some recent studies report that rural residents had equal or better health care access than urban residents (Fang, Chen, & Rizzo, 2009; M. Liu, Zhang, Lu, Kwon, & Quan, 2007), others suggest that the rural–urban gap remained, as evidenced by rural residents’ greater likelihood of early self-discharge from the hospital due to financial reasons (Jian, Chan, Reidpath, & Xu, 2010). Health care disadvantages may be particularly detrimental to the mental health of older adults as their need for health care is greater than that of younger people.
Third, some studies have suggested that rural elders in China had worse health status, faster decline in physical function, and higher rates of mortality than urban elders (Yu et al., 2012; Zimmer, Kaneda, & Spess, 2007; Zimmer, Wen, & Kaneda, 2010), although others report that older adults in rural China had better physical functioning and overall health than their urban counterparts (Feng et al., 2013; Wen & Gu, 2011; Zeng, Vaupel, Zhenyu, Chunyuan, & Yuzhi, 2002). Physical illness and disability have been known to increase risks of depression in older persons (Blazer, 2003).
Fourth, compared with their urban peers, older adults in rural China may have lower levels of social support and social participation. As mentioned above, mortality rates are higher in rural than urban older adults; thus, rural elders are more likely to be widowed and lack spousal support (Zimmer et al., 2007). In addition, older persons in rural villages may be less likely than those in the city to have children living close by to provide instrumental and emotional support, due to out-migration of rural youths (National Bureau of Statistics of China [NBS], 2012). Rural older adults also may not have as many opportunities as their urban peers to participate in social and community activities—in part because fewer organizations and amenities exist in rural villages to facilitate social interaction of older adults. Social support and participation have been suggested to have mental health consequences for older adults (Chiao, Weng, & Botticello, 2011; George, 2011).
Late-life depression is a serious public health issue in China (Zhang et al., 2012). Identifying the factors that are responsible for rural–urban differences in depressive symptoms among older adults can inform interventions to improve mental health of older Chinese and reduce mental health disparities, ultimately lowering health and related costs (Hu, He, Zhang, & Chen, 2007).
Method
Data and Sample
Data for this analysis were taken from the 2011 baseline survey of the China Health and Retirement Longitudinal Study (CHARLS), which was based on the Health and Retirement Study (HRS) in the United States and related aging surveys around the world (charls.ccer.edu.cn/en). The sample was obtained through multistage probability sampling. It began with randomly selecting 150 county-level units from a sampling frame containing all county-level units, which had been stratified by region, and within region, urban district or rural county and gross domestic product (GDP) per capita. Then three primary sampling units (PSUs; administrative villages in rural areas and neighborhoods in urban areas) were selected from each county-level unit. Within each PSU, dwellings were randomly selected. If a household had one or more members aged 45 and older, only one was randomly selected as the main respondent. If the main respondent’s spouse was available, he or she was also interviewed. The survey had a response rate of 80.5% (Zhao et al., 2013).
In addition to collecting individual-level data, CHARLS collected information related to the social, economic, and policy environments of the community in which respondents resided by interviewing community leaders (persons in charge of village/neighborhood committees). Community leaders were asked to look up certain statistics of the village/neighborhood when completing the community survey. Respondents who comprised the analyzed sample resided in 447 communities.
This study focused on older adults, so we included in our sample only CHARLS respondents who were 60 years old or older. If a household had two age eligible respondents (i.e., both the main respondent and his or her spouse), we included the main respondent only so to avoid interdependency of sampling units within the same household. The final sample was composed of 5,103 older Chinese adults.
Variables and Measures
Depressive symptoms
Our dependent variable was depressive symptoms, measured by the 10-item Center for Epidemiologic Studies Depression Scale 1 (CESD-10), which has been widely used in prior studies (Andresen, Malmgren, Carter, & Patrick, 1994), validated in older Chinese in Hong Kong (Boey, 1999; Cheng & Chan, 2005), and has demonstrated factorial validity in the CHARLS sample (Chen & Mui, 2014). It asked respondents to rate depressive symptoms in the past week on a 4-point scale (from rarely or none of the time to most or all of the time). With two items reverse coded, the sum of the CESD-10 scores ranged from 0 to 30 (Cronbach’s α = .81).
Rural–urban
The official household registration (hukou) system has been the legal division of rural and urban populations since the establishment of the People’s Republic of China (Chan, 2009). We used respondents’ report of current hukou status to classify them as rural (agricultural) or urban (non-agricultural) residents. More recently, some areas have abolished the hukou differentiation and included both agricultural and non-agricultural hukou as unified residency hukou. For respondents who reported to have unified residency hukou (n = 28), their prior hukou status was used.
Socioeconomic status
We used indicators of SES at the individual (education, pension benefit), household (asset), and community (infrastructure) levels to capture socioeconomic resources available to respondents. Education was coded in four categories—illiterate, less than primary but can read and write, primary school, and junior high or more. Pension benefit refers to income from public and private pension programs, and was classified into four categories—no pensions, and low, medium, and high benefits. Low, medium, and high benefits were based on dividing the amount of benefits, among respondents receiving pensions, into tertiles.
At the household level, asset indicates a household’s wealth or long-term standard of living (Filmer & Pritchett, 2001). Compared with household income and expenditure—two commonly used indicators of household economic resources—composite asset index is less subject to measurement errors, particularly in the context of developing countries (Bollen, Glanville, & Stecklov, 2002). Following the approach of Filmer and Pritchett (2001), we constructed an index derived from principal components analysis of 35 asset variables. 2
Infrastructure deficiency was used to indicate SES at the community level. Adequate infrastructure supports proper community function and economic growth (Aschauer, 1989). The community survey of CHARLS collected data about the basic infrastructure of respondents’ communities. Using these data, we constructed an infrastructure-deficiency index using principal components analysis that included nine indicators in four areas: connectedness, sewer, waste management, and electricity. 3 Based on index scores, communities were divided into four quartiles, from least to most infrastructure-deficient.
Health care access
Five variables were used to measure health care access. The first was distance to health care facility. It was a community-level variable, measured by the distance from the village/neighborhood office to the closest health care facility. The distance was classified as within 1 km or more than 1 km. The other four variables were based on respondents’ report of whether they had (a) health insurance, (b) not visited a physician when ill in the month prior, (c) not been hospitalized when suggested by a doctor as needed in the year prior, and (d) discharged themselves from the hospital before recovery in the year prior. Each was coded as a dichotomous variable.
Health status
Respondents’ health status was indicated by chronic conditions and disability in activities of daily living (ADL) and instrumental activities of daily living (IADL). Respondents were asked whether they had been diagnosed with any of 14 chronic conditions (e.g., heart disease, diabetes, chronic lung disease). We used this information to classify respondents into one of four categories—no, one, two, and three or more chronic conditions. Items on the ADL included dressing, bathing/showering, eating, getting in and out of bed, using the toilet, and bladder and bowel control. Items on the IADL included doing household chores, preparing meals, shopping for groceries, managing money, and taking medications. For each ADL and IADL item, respondents reported levels of difficulty in performing the activity. Two dichotomous variables were used to indicate whether respondents had ADL and IADL disability, respectively. No disability was defined as having no difficulty in all corresponding items.
Social support and participation
Four dichotomous variables—partnered status, children nearby, social participation, and elder activity center in community—were used to indicate social support and participation. Partnered status was measured as currently married/cohabiting (=1) and not (=0). Children nearby was coded yes (=1) if respondents lived with children or had children living in the same community; otherwise, it was coded no (=0). Social participation was coded yes (=1) if respondents had engaged in any of the following seven activities in the month prior: spent time with friends, played cards, chess, or ma-jong with others, provided help to non-co-residing family members, friends, or neighbors, visited a park or a social center to dance/exercise, participated in activities organized by community organizations, participated in volunteer work, and attended a class or training workshop. Otherwise, it was coded no (=0). A community-level variable—whether respondents’ community had an elder activity center—was used to indicate opportunities for social interaction and participation.
Age and sex
We included respondents’ age (measured in years) and sex (1 = male; 0 = female) as control variables.
Data Analysis
We first tested differences between rural and urban older adults in depressive symptoms and the four sets of factors (SES, health care access, health status, and social support and participation) thought to account for their depression gap. Then we conducted multilevel linear regression, because the data we analyzed involved individuals nested in communities and the dependent variable is a continuous variable. To assess the extent to which rural–urban differences in depressive symptoms were explained by a particular set of social and health characteristics, we estimated a series of models with different sets of covariates. Model 1 was a base model and simply included rural–urban, age, and sex as covariates. Models 2 to 5 each added SES, health care access, health status, and social support and participation, respectively, to the base model. Changes in the coefficient for rural–urban from the base model as different sets of covariates were added would indicate the extent to which the set of covariates accounts for differences in depressive symptoms between rural and urban older adults in China.
The independent variables had a modest amount of missing values (<1%), but the dependent variable, depressive symptoms, had 13.5% missing. We conducted multiple imputation. Results reported here were based on analyses of five imputed datasets. We found similar results when repeating the analysis excluding cases missing depressive symptoms. All analyses were conducted using Stata 13.0 (StataCorp, 2013). Below, we first present the descriptive results that have been weighted. We then present the results from multilevel linear regression in which robust standard errors (SE) were used (unweighted). The CHARLS provided only individual-level but not community-level weighting variables. As a form of sensitivity test, we had included a scaled individual-level weight in the multilevel regression models in an extra analysis. The weighted results (available on request) are similar to the ones reported below.
Results
Characteristics of the Sample
Table 1 presents characteristics of the sample (weighted and not weighted). About 23% belonged to urban and 77% belonged to rural hukou. Based on the weighted sample, they averaged 69.6 years old and 48% were male. Most had low education, and 41% were illiterate. A majority (64%) did not have pensions. We classified the respondents into quartiles based on scores of the household asset index. Respondents’ communities were also divided into quarters based on community infrastructure deficiency scores.
Sample Characteristics: Total, by Urban and Rural.
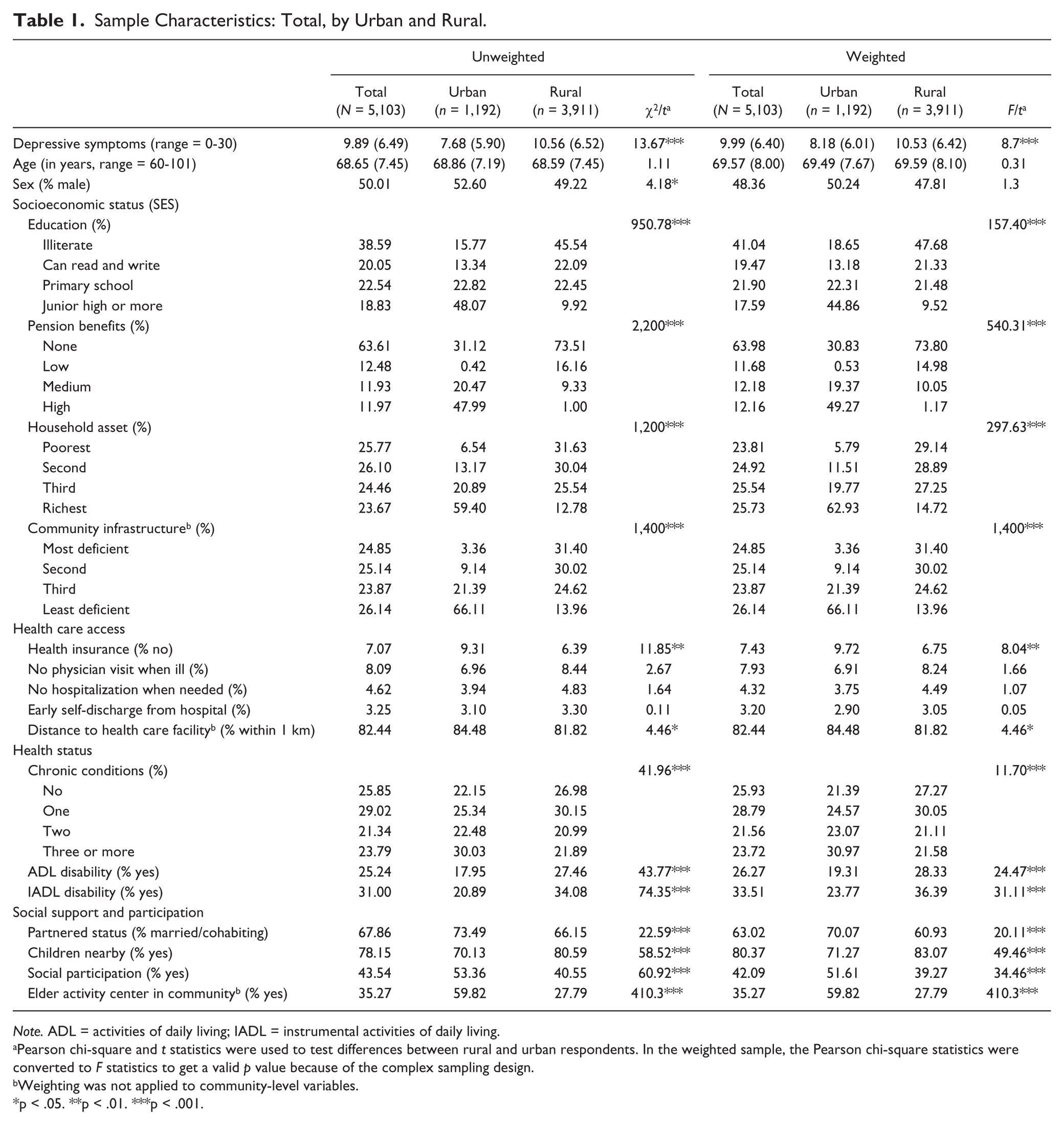
Note. ADL = activities of daily living; IADL = instrumental activities of daily living.
Pearson chi-square and t statistics were used to test differences between rural and urban respondents. In the weighted sample, the Pearson chi-square statistics were converted to F statistics to get a valid p value because of the complex sampling design.
Weighting was not applied to community-level variables.
p < .05. **p < .01. ***p < .001.
Only a minority of respondents indicated barriers in health care access—7% had no health insurance; 8% did not visit a physician when ill; 4% did not get hospitalized when needed; 3% discharged themselves from hospital before recovery; and 82% lived in communities that had a health care facility nearby. Slightly more than a quarter (26%) of the sample had no chronic conditions; 29%, 22%, and 24%, respectively, reported to have 1, 2, and 3 or more conditions. A majority had no ADL (77%) and IADL (71%) disability. About 63% of the respondents were married/cohabiting. Most (80%) had children living close by. About 42% of the sample had some level of social participation, and 35% lived in communities that had an activity center for older people.
Rural–Urban Differences in Study Variables
Table 1 also shows differences in all study variables between rural and urban older adults. As expected, the former had significantly higher levels of depressive symptoms. All indicators of SES show that rural older adults were more disadvantaged than their urban counterparts: Rural elders had significantly lower education, and they were more likely to have no or low pension benefits, be in the lower household asset strata, and live in communities with deficient infrastructure. However, rural–urban differences in health care access were almost negligible. They only differed in health insurance and distance to health care facility—rural older adults demonstrated a slight advantage over urban older adults in the former and a slight disadvantage in the latter.
In terms of health status, rural older adults were more likely to have ADL and IADL disability compared with urban older adults, but the former reported fewer chronic conditions. Regarding social support, rural elders were less likely to be married/cohabiting and more likely to have children living close by than their urban peers. A smaller proportion of rural older adults than urban older adults had some level of social participation and lived in communities that had activity centers for older people.
Accounting for Rural Disadvantages in Depressive Symptoms
Results of the multilevel linear regression analysis to examine the factors that account for rural–urban differences in depressive symptoms are presented in Table 2. The base model (Model 1) shows that rural older adults were 2.549 points (SE = .234, p < .001) higher than their urban peers on the measure of depressive symptoms (i.e., CESD-10), adjusted for age and sex. Age had a significantly positive relationship with depressive symptoms, and men had fewer symptoms than women. We had estimated an unconditional model (i.e., without any covariates, not shown in Table 2), which suggests that the total variance in depressive symptoms was 42.139, of which 12.2% were between communities (community-level variance = 5.122, SE = 0.543), and 87.8% were between individuals (individual-level variance = 37.017, SE = 0.811). The variance component of Model 1 shows that rural–urban, age, and sex explained about 6.9% ([42.139 − {4.028 + 35.205}] / 42.139 × 100%) of the total variance in depressive symptoms.
Multilevel Linear Regression of Rural–Urban Differences in Depressive Symptoms Among Older Adults in China (N = 5,103).
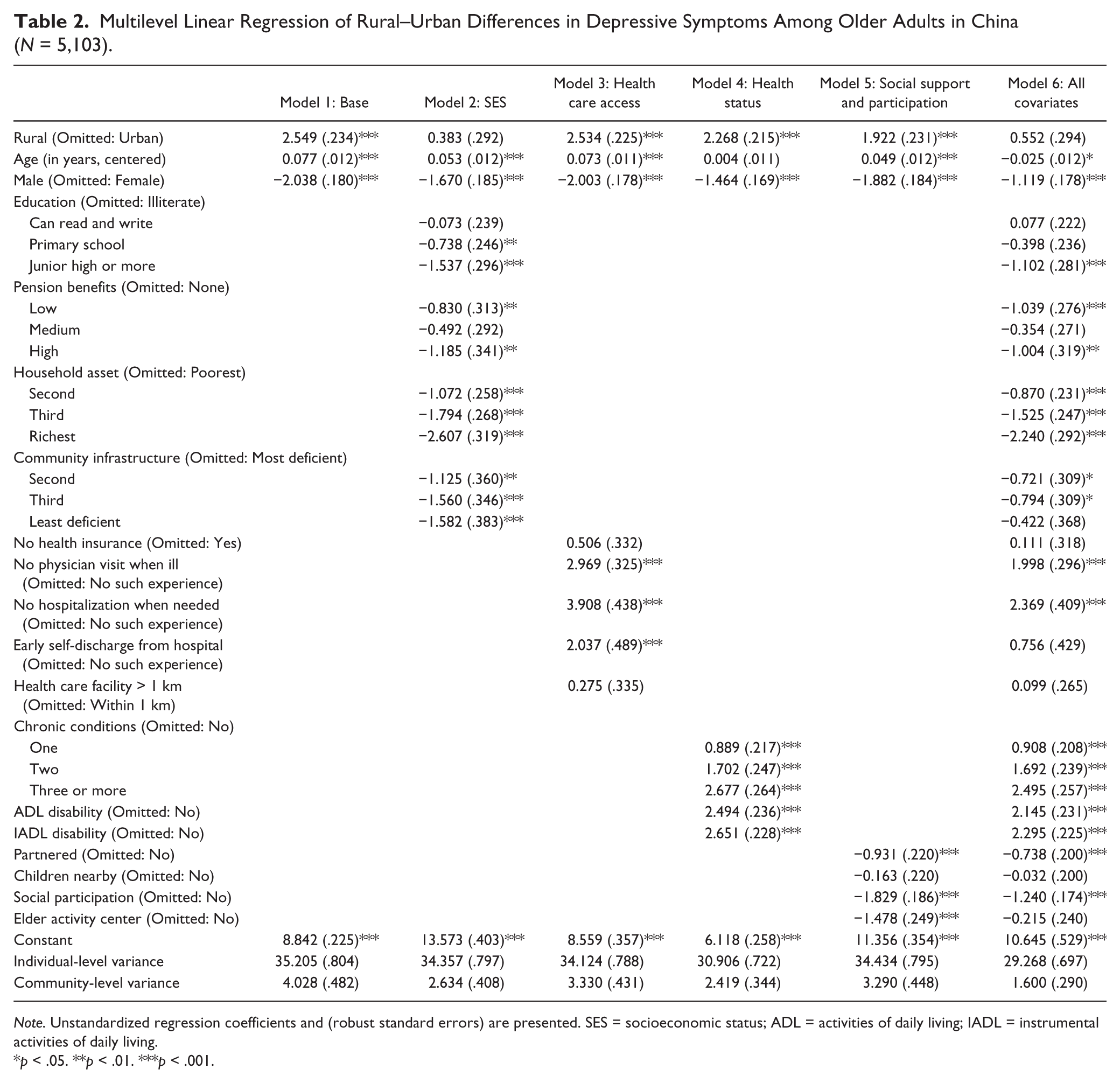
Note. Unstandardized regression coefficients and (robust standard errors) are presented. SES = socioeconomic status; ADL = activities of daily living; IADL = instrumental activities of daily living.
p < .05. **p < .01. ***p < .001.
All the added SES variables in Model 2 were significantly correlated with depressive symptoms in the expected direction: Those with more education, higher pension benefits, more household assets, and who lived in neighborhoods with better infrastructure had fewer depressive symptoms. More importantly, the coefficient for rural–urban was reduced by almost 85% compared with that in Model 1, and it was no longer statistically significant (β = .383, SE = .292, p > .05). This suggests that rural–urban differences in depressive symptoms were largely accounted for by SES.
Model 3 shows that health care disadvantages, indicated by not visiting a physician when ill, not being hospitalized when needed, and early self-discharge from hospitalization, were significantly correlated with higher levels of depressive symptoms. However, the rural–urban coefficient (β = 2.534, SE = .225, p < .001) remained almost unchanged compared with that in Model 1. The results thus suggest that health care access contributes little to rural–urban disparities in depressive symptoms.
Model 4 indicates that having more chronic conditions and disabilities in ADL and IADL was correlated with more depressive symptoms. After controlling for health status, rural–urban differences were reduced by 11% but remained statistically significant (Model 4, β = 2.268, SE = .215, p < .001). These results suggest that health status is not a primary factor responsible for the rural–urban depression gap.
In Model 5, living with a spouse/partner, having some level of social participation, and living in communities that had an elder activity center were significantly correlated with lower levels of depressive symptoms. The coefficient indicating rural–urban differences (β = 1.922, SE = .231, p < .001) in depressive symptoms was reduced by about 25% after controlling for the social support and participation variables, compared with the one estimated in the base model. However, it remained statistically significant, suggesting that social support and participation accounted for some but not all variation between rural and urban older adults in depressive symptoms.
Finally, we estimated a full model including all covariates to take into account correlations among them (Model 6). Although the magnitude of the coefficients for most covariates in the full model changed somewhat from those in previous models, the pattern remained and the rural–urban coefficient was not statistically significant (.552, SE = .294, p > .05). The full model explained about 26.7% ([42.139 −{29.268 + 1.6}] / 42.139 × 100%) of the total variance in depressive symptoms. Overall, results support that socioeconomic differentials between rural and urban older adults in China largely account for rural disadvantages in depressive symptoms.
To understand the contribution of each component of SES to the rural–urban gap in depressive symptoms, we conducted additional analyses in which each SES component was added to separate models (Table 3). The results show that, among the four SES components, household assets had the largest relative effect in explaining the rural–urban gap. However, no SES component by itself, or in combination with one or two components, could reduce the rural–urban coefficient to statistically not significant. Only when all four SES components were controlled did the rural–urban coefficient become statistically not significant (Model 6, Table 2). This suggests that rural–urban differences in depressive symptoms among older Chinese are linked to socioeconomic disparities at the individual, household, and community levels.
Depressive Symptoms, Rural–Urban Hukou, and SES Components (N = 5,103).
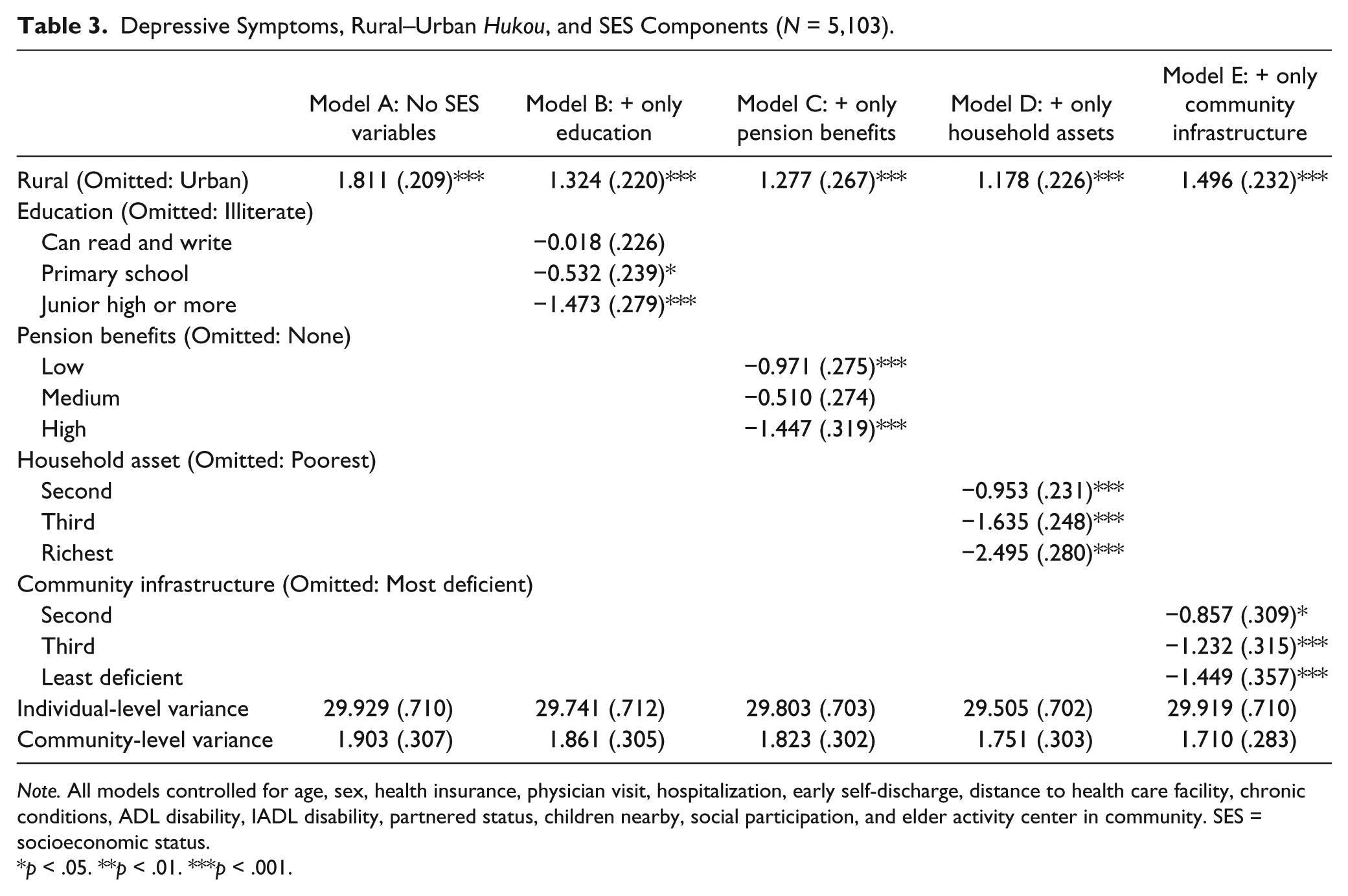
Note. All models controlled for age, sex, health insurance, physician visit, hospitalization, early self-discharge, distance to health care facility, chronic conditions, ADL disability, IADL disability, partnered status, children nearby, social participation, and elder activity center in community. SES = socioeconomic status.
p < .05. **p < .01. ***p < .001.
Discussion
Consistent with several studies using regional survey data (Dong & Simon, 2010; Li et al., 2011; Ma et al., 2008), we found that on average, adjusting for age and sex, depression levels were significantly higher among rural older persons than their urban peers. We proposed four sets of factors that may explain such rural–urban differences and tested them in a systematic fashion by estimating a series of multilevel linear regression models. Overall, SES was shown to be the predominant factor that accounted for rural disadvantages in depressive symptoms among older persons in China. Not only was each of the four SES components (education, pension benefits, household assets, community infrastructure) related to depressive symptoms in the expected direction, but together, they attenuated the rural–urban gap by nearly 85% and more importantly, to be statistically not significant.
We have defined rural and urban populations based on the hukou system. The NBS defined rural and urban areas based largely on population density (Chan, 2007). In our sample, there was high concordance (79%) between the hukou and NBS classification of rural and urban. To test the robustness of our findings, we had repeated the analysis with rural and urban coded according to the NBS definition and found a similar pattern of results (available on request) as reported in the “Results” section of this article.
The specific mechanisms that link each SES component to late-life depression may differ by component. Better-educated people tend to attain a greater sense of control, which in turn facilitates their adaptive strategies for coping with adversity (Williams, 1990). Pensions enable older adults to be financially independent and have a sense of security. Household assets represent economic resources available to the household—and by extension to individual members of the household—to mitigate poverty-related stress and to exchange for such health-generating resources as better housing conditions and health care (Elo, 2009). Ongoing exposure to a community with deficient infrastructure may increase the likelihood of experiencing allostatic load, which refers to the wear and tear that the body experiences in responding to repeated hardship and demand (McEwen & Gianaros, 2010). The four components of SES should be correlated. In our data, the highest correlation was between household asset and community infrastructure (r = −.54). However, our analysis suggests that each was associated with depressive symptoms independent of the others (Model 2, Table 2). Yet, none of the SES components alone can fully explain the rural–urban difference (Table 3). The direction of the relationship between SES and depression is debatable, but increasing evidence supports that individuals with low SES are vulnerable to develop depressive symptoms (Lorant et al., 2003). Our analysis cannot examine causal relationships as cross-sectional data were used. More studies are needed to understand how SES at the individual, household, and community levels, separately and as a whole, is related to mental health of older persons in the context of China’s hukou system.
Although the other three sets of covariates (health care access, health status, and social support and participation) were also significantly correlated with depressive symptoms, their explanatory power for the rural–urban difference was somewhat limited. Controlling for health care access barely affected the estimated rural–urban gap, which was unsurprising given the negligible difference in our measures of health care access between rural and urban older adults. Some studies show that the Chinese government’s recent investment in health care reforms has greatly increased health care utilization and reduced rural–urban gap in health care access (Meng et al., 2012; Yip et al., 2012). However, the quality of health care that rural and urban elders receive may differ. The CHARLS does not provide measures of health care quality.
The role health status played in the rural–urban gap in depressive symptoms was more complex than we had expected. Rural older adults reported fewer chronic conditions and more physical disabilities than urban elders. In the regression analysis, rural–urban differences increased after controlling for chronic conditions, countering the reduction in the rural–urban gap by controlling for ADL and IADL disability. Thus, health status as a whole only accounted for a small portion of rural–urban differences in depressive symptoms. Although it was not our focus, the findings that rural elders had higher levels of physical disability than urban elders were contrary to some (Feng et al., 2011; Wen & Gu, 2011; Zeng et al., 2002) but consistent with other prior studies (He, Sengupta, Zhang, & Guo, 2009; Zimmer, Kaneda, Tang, & Fang, 2010; Zimmer, Wen, et al., 2010). Many reasons, including variation in samples and measurement, may contribute to the mixed findings.
Social support and participation attenuated but did not eliminate the rural disadvantage in depressive symptoms. In the full model, only two indicators in this category—partnered status and social participation—were significantly associated with depressive symptoms. Rural older Chinese were less likely to be married/cohabiting than their urban counterparts, and less likely to have some level of social participation. Prior studies have shown that being unmarried and low levels of social participation increase risks of depression (Adams, Sanders, & Auth, 2004; Chiao et al., 2011).
As mentioned in the introduction, relevant research in other countries tends to report either no significant differences (Abe et al., 2012; Kim et al., 2002; St. John et al., 2006) between rural and urban older adults or an urban disadvantage (Friedman et al., 2007; Kim et al., 2004; Walters et al., 2004) in depressive symptoms. One reason for their findings may be that most of these studies were conducted in developed nations where urban life, relative to rural living, may be more stressful, due to faster pace, higher crime rates, more crowded environment, and higher levels of pollution (McKenzie, Murray, & Booth, 2013). Social isolation may also be more prevalent in urban residents as community relationships may be weaker in the city than in the countryside. Most urban cities in China may not have yet developed to the stage where urban hazards offset or outweigh the advantages associated with urban living. In addition, few countries have institutionalized SES inequalities between the rural and urban population like the hukou system in China.
Limitations of this study should be noted. First, our findings should be interpreted as correlations only. The factors that we hypothesized to influence depressive symptoms, for example, health care access, social participation, and physical disability, could be influenced by depressive symptoms. We cannot establish the direction of effects as cross-sectional data were used. Caution should be taken when interpreting the findings. Second, we have taken a static view on depressive symptoms, which by nature are dynamic. Further studies need to investigate how rural and urban older adults differ in the way they experience the onset and trajectory of depressive symptoms. Third, although we have used multiple indicators to measure the four sets of factors (SES, health care access, health status, and social support and participation) that may account for the rural–urban difference in depressive symptoms, the constructs may not have been captured fully or precisely, which may have contributed to the modest power of some in explaining the rural–urban depression gap. Even with these limitations in mind, this study contributes to growing efforts to understand the rural–urban inequality in mental health among older adults in China and other developing countries where populations are aging and depression is emerging as a public health issue.
Given the cross-sectional nature of our analysis, it may be immature to discuss implications of the findings for practice. Nevertheless, we think that policies and programs that aim to reduce SES inequalities between rural and urban residents, such as expanding pension coverage among the rural population, improving village infrastructure, and enabling rural households to accumulate wealth, should do many goods including preventing depression among older adults in rural China.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Li was supported by a grant from the National Institute of Health (R01MH100298). Dr. Liu was supported by a post-doc fellowship at the Curtis Center, School of Social Work, University of Michigan.