
Abstract
In many developing countries, intensified rural–urban migration coupled with globalization has brought about profound changes in rural family life. These changes have contributed to changes in the psychological well-being of the older adults (Abas et al., 2009; Adhikari, Jampaklay, & Chamratrithirong, 2011; Antman, 2010, 2012; Chang, Dong, & MacPhail, 2011). This is especially true where filial expectations of adult children remain strong, and intergenerational familial care is still a social safety net for the rural older adults (Benjamin, Brandt, & Fan, 2003). Extant studies usually consider the migration of adult children as causes for changes in family structure and living arrangements (e.g., causing more single-generation or skipped-generation households), which in turn impact the psychological health of older adults. Indeed, living arrangements have been found to be linked to the mental well-being of the older adults in a number of settings, including China (F. Chen & Short, 2008; Hughes & Waite, 2002; Qian & Knoester, 2015; Zunzunegui, Beland, & Otero, 2001). However, fewer studies have considered the fact that in addition to a family process, migration in itself is also a unique social process. Instead of an “absence” from the household, migration patterns of adult children such as short-distanced or long-distanced migration can directly expose the left-behind to a series of differentiated psychosocial processes that affect their psychological well-being. Moreover, there is little understanding of how extra-familial support in the communities may play a role in cushioning such familial impact.
This study investigates the association between patterns of migration and the depressive symptoms of left-behind elderly in rural China, and how community contexts moderate such relationships within the context of massive internal migration. In particular, I ask the following questions:
Given that children’s migration status also partly determines living arrangements, the analysis integrates adult children’s migration status and living arrangements of older adults, and creates a multi-category variable to examine the differences between the parents of migrants and non-migrants in the same living arrangements.
In the context of rural China, this study is also among the first to use village to represent community, and to identify the role of community poverty in the depressive symptoms of older adults.
Background
Study Context
China is now witnessing the largest migration in human history. In 2000, the floating population 1 comprised 6% (79 million) of the total Chinese population; by 2010, this share had increased to 17% (221 million; China Statistics Press, 2012; Liang, Li, & Ma, 2014; Liang & Ma, 2004). At the same time, China is rapidly aging: With a total population of more than 1.3 billion, more than 202 million people were above 60 years in 2013. This number is set to reach around 288 million by 2025, and 370 million by 2050 (National Statistics Bureau, 2014; United Nations, 2002). Currently, two thirds of the older Chinese reside in rural areas (China Statistics Press,2011). These rural older adults usually have worse health status, faster decline in physical functions, and are more depressed than their urban counterparts (L. Li, Liu, Xu, & Zhang, 2016; Zimmer, Kaneda, & Spess, 2007; Zimmer, Kaneda, Tang, & Fang, 2010; Zimmer, Wen, & Kaneda, 2010). 2 It is estimated that by 2011, at least half of the rural older adults had been impacted by migration. 3
Moreover, these migrants do not travel equal distances. As important dimensions of migration, the patterns of migration distance are usually proxied by inter-provincial migration and intra-provincial migration, with the former indicating longer migration distance and higher migration costs (Poncet, 2006). Due to the regional economic disparity that drives inter-provincial migration, inter-provincial migration usually reflects the inter-regional movement of migrants, with migrants traveling from the Central or Western regions to the Coastal region (Chunyu, Liang, & Wu, 2013; Ding, Liu, Cheng, Liu, & Zou, 2005; Fan, 2005a, 2005b; Liang & White, 1997). These inter-provincial migrants consistently constitute approximately 50% of the total migrant population (Liang et al., 2014; Poston & Mao, 1998). Nevertheless, while studying familial migration outcomes, the differences created by these patterns of migration distance are usually left out of the discussion.
Family Disruption and the Role of Community Poverty
Does migration matter?
According to the family disruption framework, changes in family structure that remove close family members from the household—such as marital disruption or death of a spouse or child—bring negative consequences for individuals’ well-being (Gilman, Kawachi, Fitzmaurice, & Buka, 2003; McLanahan & Bumpass, 1988; Sampson, 1987). This perspective has most often been invoked to understand parental divorce and children’s well-being (Gilman et al., 2003; Ross & Mirowsky, 1999). In the context of rural China, the migration of a spouse or adult child similarly removes close family members from the household. This may diminish social support and lead to more depressive symptoms among older adults (Lu, 2012; McKenzie, 2005; Taylor et al., 1996). In particular, in the context that coresidence with adult children is beneficial to the mental health of older adults (F. Chen & Short, 2008; X. Chen & Silverstein, 2000; Chi & Chou, 2001; Leung, Chen, Lue, & Hsu, 2007), it has been widely implied that adult outmigration influences elderly psychological health by reducing coresidence with adult children (i.e., changing family structure). However, it is less acknowledged that adult migration may directly create psychological stress for their older parents by reducing accessibility and face-to-face exposure to migrant kin. It may also cause anxiety toward migrant children. Living a certain distance away from the migrant child, the older adults might also develop a differentiated emotional cohesion with the migrant and non-migrant children. This could contribute to their depressive symptoms (Silverstein, Cong, & Li, 2006). Moreover, residing far away from the elderly parents is usually perceived as being defiant to traditional filial expectations and obligations, which can be detrimental to their mental health (He, 2002; Mjelde-Mossey, Chi, & Lou, 2006; Silverstein et al., 2006; L. C. Yu, Zhang, & Draper, 1997). Therefore, even for the coresident older adults, having a migrant child may still be associated with an increased probability of developing depressive symptoms.
However, it is also possible that the migration of children may not take a significant toll on the mental health of older adults. Migration enriches rural households (Rozelle, Taylor, & DeBrauw, 1999; Taylor, Rozelle, & DeBrauw, 2003), and higher socioeconomic status (SES) is associated with less depressive symptoms (L. Li et al., 2016). Migration may not significantly disrupt family life for older adults, as they may enjoy other types of support in the household, such as a present spouse, or the presence of other adult children or children-in-law in the household. 4 Nevertheless, the left-behind elderly may still experience diminished mental health compared with normatively mandated traditional living arrangements in which older adults coreside with adult children and do not have migrant children. Therefore, I expect the following:
Do patterns of migration distance matter?
The family disruption perspective tends to focus on whether or not a disruption has occurred. However, in the case of migration, family disruption may be temporary and communication and support may still flow between family members. Importantly, adult children’s migration may be less associated with negative outcomes such as depressive symptoms, if that migration does not take adult children too far to continue to provide some support to the elderly family members left-behind (e.g., intra-provincial migration). Indeed, migration is a social process where patterns of travel distance can be transformed into perceived meanings to both migrants and their older parents. These perceived meanings include factors such as the affordability of a return trip, in terms of both costs and time (Logan, 2012; Lu, 2012). For the older adults, a manageable travel time could mean this migrant child is able to return within a single day, if instrumental and/or emotional support is needed. A travel time beyond these boundaries may create additional emotional stress, or even cause further loss of anticipated support, which will contribute to depressive symptoms for older adults (Krause, 1997). In reality, due to busy work schedules in the coastal region and large financial and time costs in visiting their elderly parents, most inter-provincial migrants can only afford to return home several times a year. Therefore, regardless of their living arrangements, I expect the following:
Does community poverty matter?
Just as the patterns of migration distance may be associated with more or less of a loss of social support, so too might the ability of the origin community contexts to differentially buffer the loss of migrant children’s support. The older population is especially sensitive to the communities where they reside because they tend to be less mobile and more reliant on locally accessible services and amenities, as well as social support (Kubzansky et al., 2005). Community poverty and deprivation have been used to proxy community resources and social support; their associations with poor mental health have been widely documented in both developed and developing settings (Galea et al., 2007; L. Li et al., 2016; Ross, 2000). Compared with impoverished communities, non-impoverished communities may offer more resources for the left-behind elderly to substitute for children’s presence. Such resources may include recreational projects and village programs (e.g., recreational centers, nursing homes, organizations for helping the older adults). These provisions can further create physical and social space for left-behind elderly to obtain access to high-quality social interaction, and to help foster better community cohesion. Alternatively, for impoverished communities, in addition to lack of resources, community poverty is also associated with a lack of supportive social relationships, higher levels of perceived social disorder, and inability to prevent the occurrence of negative experiences (e.g., crime). Each of these factors contributes to high stress and depressive symptoms among the older population (Kubzansky et al., 2005; Ross, 2000; Yen, Michael, & Perdue, 2009).
In the context of China, Wen and Gu (2011) have also found that older adults living in low-income counties are more likely to be depressed. There are, however, usually a greater amount of heterogeneities within a county than a community. The current study uses a much smaller and more accurate scale to proxy rural community—the rural village. I expect that when facing a possible stressful event (i.e., children’s migration), the left-behind elderly living in non-impoverished communities have better access to extra-familial support for protection, and share more supportive social relationships than those in impoverished villages. Thus, I derive my third hypothesis:
Data and Method
Data
The data used for this analysis come from the baseline survey of the China Health and Retirement Longitudinal Study (CHARLS), conducted in 2011. 5 It is a high-quality nationally representative sample of Chinese residents age 45 and older. The data quality of the survey has been evaluated, and research results derived from them have been published widely (Han & Shibusawa, 2015; L. Li et al., 2016; Zhao, Hu, Smith, Strauss, & Yang, 2014; Zhao, Smith, & Strauss, 2014). Adopting multi-stage stratified Probability Proportional to Size (PPS) sampling, the baseline national included approximately 10,000 households and 17,500 individuals in 150 counties/districts and 450 villages/resident committees in 28 provinces. Importantly, CHARLS 2011 contains a detailed household roster, a family roster, a section on a broad range of health questions, and a community questionnaire. Household members are defined in the survey as those who live in the same residence, or who have migrated to other places but live in dormitories. Living in a dormitory is usually only temporary. This is also different from the traditional form of a “split household” in which adult children move out of the parental households and establish their own families. The household roster collects information about each household member with regard to his or her demographic characteristics, whether he or she had been away from the residence for more than a month over the past year and where they had gone. The family roster asks about each non-resident member’s current residence, the amount of financial transfers from each of the non-resident household members over the past year and so on. In the community questionnaire, local cadres provide information on a series of topics about the resident communities. In particular, income per capita for the village is polled, which is utilized in this study as a proxy for community wealth. To date, CHARLS 2011 is the only national representative survey on elderly Chinese that contains these data. 6
The analysis is restricted to older adults 60 and above who resided in rural areas. Older adults who did not have a living child at the time of survey (approximately 2% of the rural older adults) are excluded from the sample. Approximately 92% of these older adults have information on their depressive symptoms. Other control variables are missing at 0% to 1% levels. The final sample consists of 4,888 rural older adults living in 3,335 households and 296 rural communities.
Method
Dependent variables
A short version of the Center for Epidemiologic Studies–Depression Scale (CES-D 10) is provided in CHARLS. CES-D is a widely used measure across many societies (L. Li et al., 2016; Radloff, 1977; Weissman, Sholomskas, Pottenger, Prusoff, & Locke, 1977). Different types of shorter forms were also tested and found to be reliable (Kohout, Berkman, Evans, & Cornoni-Huntley, 1993). In this short form, 10 questions were asked (those CES-D items and Chinese translations are listed in Appendix A). Each inventory was ranked on a 4-point Likert-type scale, ranging from 0 to 3, with higher scores demonstrating more depression. I created a dichotomous measure by summing all the scores and using a cutoff of 12, as was determined by Cheng and Chan (2005) to be the optimal threshold for predicting depression in an older Chinese population. This threshold indicates the clinically concerning depressive problems for the older adults. 7
Independent variables
Migrants are defined broadly as those who have left their rural parents’ households and have resided in a different county for more than 1 month. They include both the migrant children in and outside of the elderly households. Left-behind elderly are defined as those who had at least one adult child who had migrated. Because households usually make simultaneous decisions on adult migration and living arrangements for older adults, I combine children’s migration status and older adults’ living arrangements into a set of dummy variables. An examination of the arrangement “living nearby” shows that this living arrangement is not significantly associated with the mental health of older adults. Therefore, this variable is dropped from the key predictors. This yields four basic groups: coresident older adults with no migrant children (reference), coresident older adults with migrant children, non-coresident older adults with migrant children, and non-coresident older adults with no migrant children. 8 Demographic characteristics include the older adult’s age, gender, educational attainment, total number of children, and whether or not she or he has a son. Functional impairments are calculated as the mean of 15 items reflecting difficulties in performing activities of daily living such as difficulties in getting dressed, bathing/showering, eating, and getting in and out of bed, as well as instrumental activities of daily living such as doing household chores, preparing meals, shopping for groceries, managing money, and taking medication. A mean score is taken for each individual where 0 = no difficulty in every indicator and 4 = cannot do any of these at all.
This study also controls for a wide range of variables to capture familial social support for the older adults who may serve as mediators. Time taking care of grandchildren is controlled, as it can be influenced by adult children’s migration and also has an effect on older adult’s mental health (F. Chen & Liu, 2012; Chu, Xie, & Yu, 2011; Ku et al., 2013; Silverstein et al., 2006; Zeng & Xie, 2014). It is measured by hours per year. Household income and financial transfers from non-resident adult children are included to jointly account for the economic status of the older households. The frequency of older adults’ social activity is measured by self-reported activity in the last month, and is treated as a set of dummy variables (have daily interactions with people, have weekly interactions with people, and rarely interact with people [reference]). Poverty status of villages is used to approximate community poverty. A dummy variable is generated based on the income per capita for each surveyed village in 2010. Villages whose income per capita was above the poverty line in 2010 are considered as the reference category. The 2010 national poverty line of 1,274 yuan 9 is used as the cutoff point.
Analytical strategy
The analytical sample is older adults (60+) who lived in rural areas at the time of the survey. Logit models are first performed at the individual level. The first step controls for children’s migration status and living arrangements, demographic characteristics, and provinces of residence. To further evaluate possible mediating factors, the second step uses random effects Hierarchical Linear Modeling (HLM; Luke, 2004), and further controls for the following factors: financial transfers from children, time spent caring for grandchildren, time spent on farmwork, and the poverty status of rural communities. After controlling for these factors, if we still observe significant associations between the key predictors (i.e., children’s migration status and living arrangements) and the mental health of older adults, these associations may be due to the factors directly associated with children’s migration and changes in living arrangements. These include reduced face-to-face interactions with, and/or perceived support from, migrant children; anxieties toward out-migrated children; greater disparity of emotional cohesion with their children and other psychosocial pathways. Tests of differences in coefficients among the key predictors are also performed to evaluate how migration itself makes a difference among older adults of the same living arrangements. The third step adds cross-level interactions between the poverty status of villages and adult children’s migration status and living arrangements. The equation for the third step is as follows:

where Depressionij is the logged odds of having depressive symptoms; γ0,0 is the adjusted mean health outcome (intercept); γ1,0, γ2,0, and γ3,0 are the coefficients for the three types of combined characteristics of children’s migration and living arrangements for individual i at village j; Povertyj is the feature poverty of village j; γ1,0, γ2,0, and γ3,0 are the coefficients for the cross-level interaction terms between the two characteristics. There are also 16 covariates and 34 provinces controlled at Level 1 of the regression, and β and α are vectors of coefficients for these controls. Finally, u0j is the random effect for the jth village, and rij is the random effect for the ith individual in the jth village. All analyses were conducted in STATA 12 (StataCorp, 2011). To adjust the covariance between older adults from the same household, Huber–White sandwich estimators (robust option in Stata) are used for estimating the standard errors.
To capture the overall role of migration and that of patterns of migration distance, respectively, I adopt a two-stage analysis strategy: In the first stage (Models 1-3), the combination of children’s migration status and older adults’ living arrangements are used as the key predictors. The second stage (Models 4-6) aims to evaluate the role of the patterns of migration distance. Adult children’s patterns of migration distance are combined with living arrangements as the key predictors: coresident older adults with no migrant children (reference), coresident older adults with intra-provincial migrant children, non-coresident older adults with intra-provincial migrant children, coresident older adults with inter-provincial migrant children only, non-coresident older adults with inter-provincial migrant children only, and non-coresident older adults with no migrant children.
Results
Descriptive Statistics
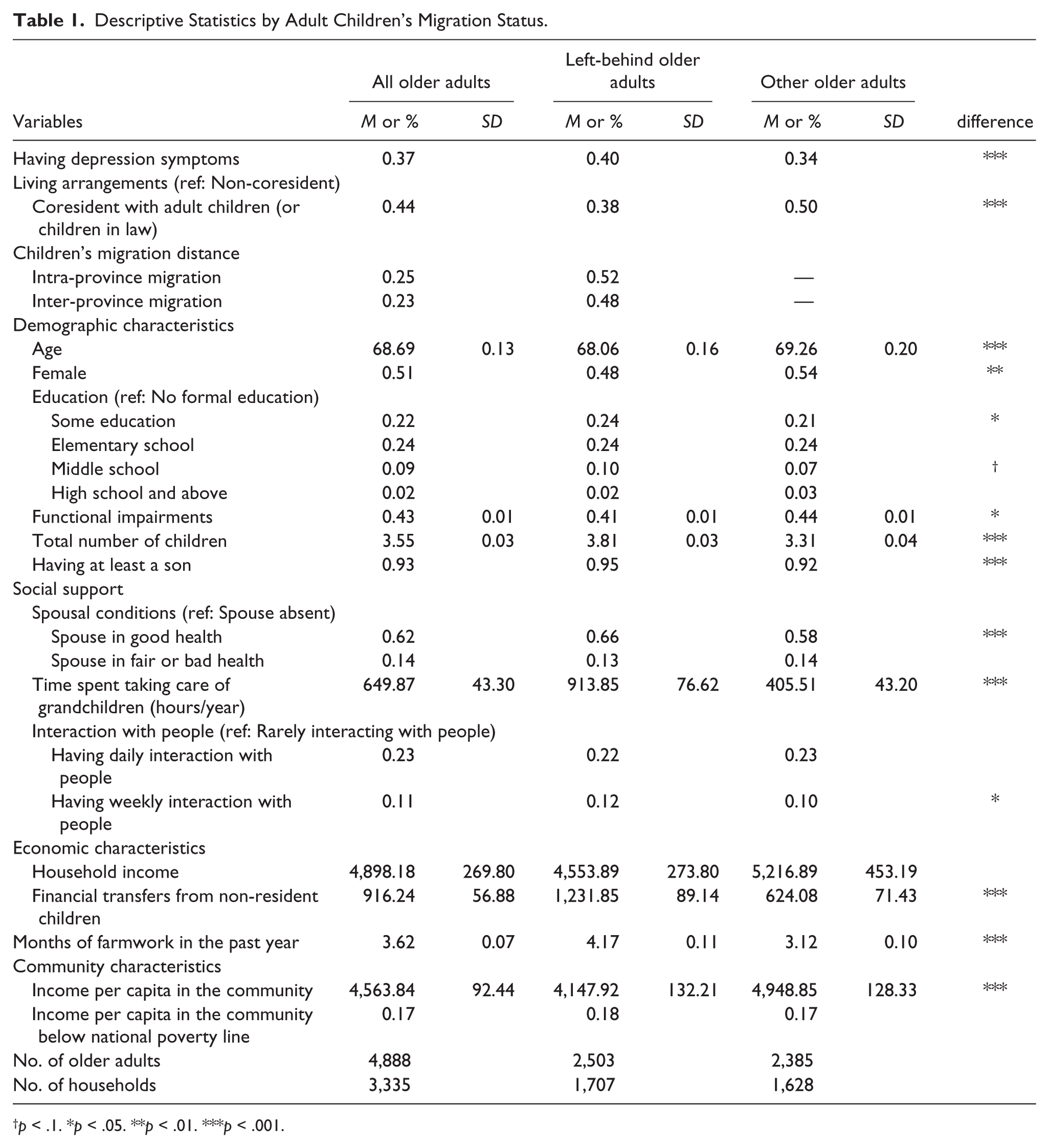
The first column of Table 1 shows the characteristics of all rural older adults in the sample. Sample weights are used in descriptive statistics and tests of differences. Overall, approximately 37% of the older adults have depressive symptoms, which is a high percentage compared with their counterparts in Europe and the United States. Reduced social support from families and high levels of physical adversities among rural older Chinese might contribute to this high percentage (Gao et al., 2009; J. Yu, Li, Cuijpers, Wu, & Wu, 2012). Whereas 50% of the older adults with no migrant children coreside with adult children or children-in-law in the sample, only 38% of the parents of migrants do so. In terms of children’s patterns of migration distance, 25% of the older adults have at least one of their migrant children residing in the same province, and another 23% have all their migrant children residing outside the province. This means 48% of the older adults constitute the left-behind elderly. This is in line with the general pattern of internal migration obtained in the census. In general, the older adults in the sample have an average of 3.55 living children. Consistent with previous findings (Giles, Wang, & Zhao, 2010), the financial transfers from non-resident children to the older household are moderate—the mean was 916 yuan in 2010. Overall, income per capita in the community was 4,564 yuan in 2010, with 17% of respondents living in communities below the poverty line. Comparisons between the left-behind older adults and other older adults show that the former group is significantly more likely to have depressive symptoms (40% vs. 34%). They are also slightly younger, tend to be male, have more children, are more likely to have a son, and to be from low-income communities. The left-behind older adults also tend to have less functional impairments, which suggests that functional impairments can be part of migration decisions (i.e., adult children are more likely to become migrants if their elderly parents have fewer barriers to physical activities). A distribution of the sample by individual provinces (not shown) demonstrates that the left-behind elderly are more likely to come from the Western region of China, the poorest region among Coastal, Central, and Western regions.
Descriptive Statistics by Adult Children’s Migration Status.
p < .1. *p < .05. **p < .01. ***p < .001.
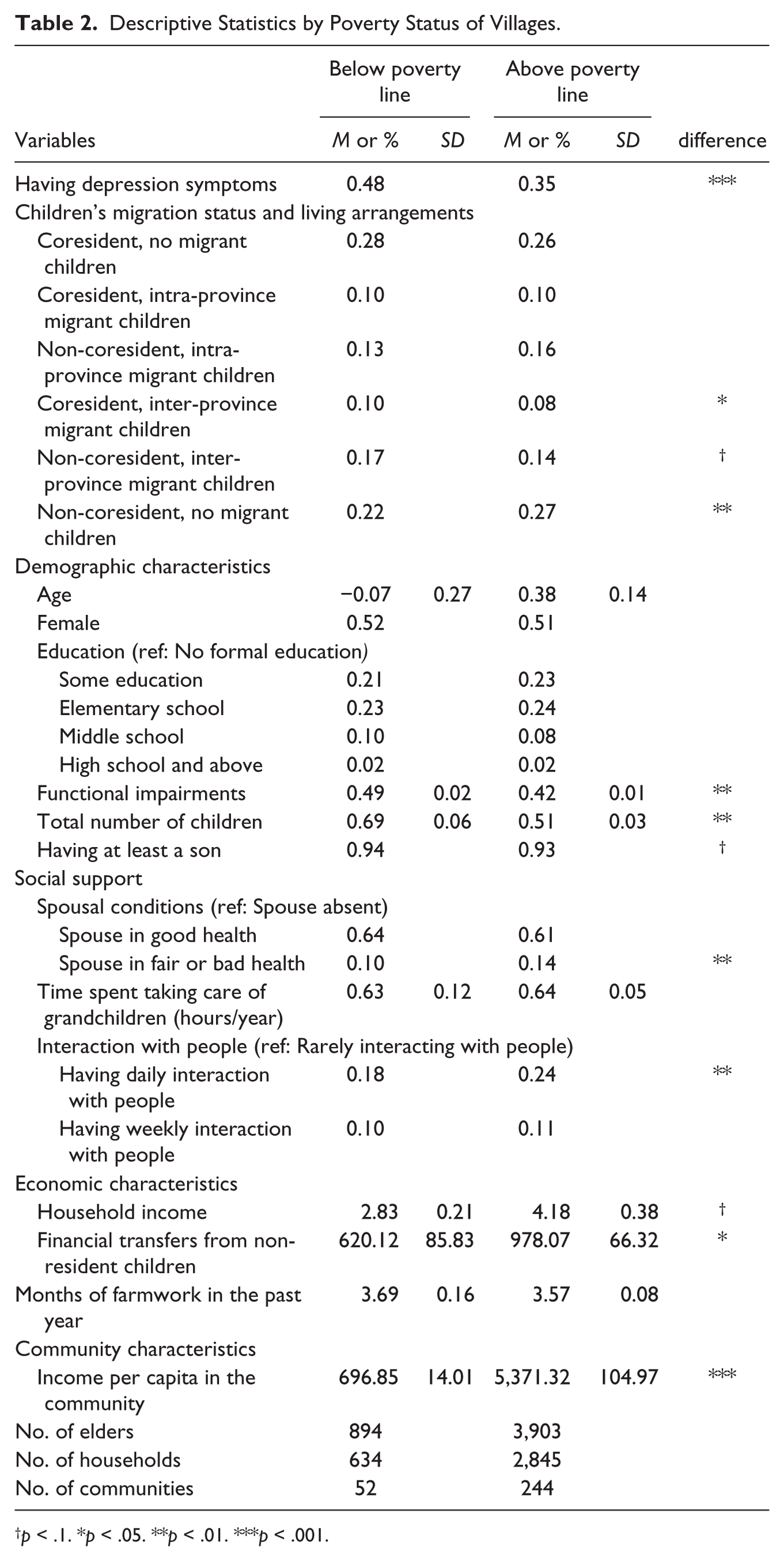
Table 2 displays descriptive statistics for the older adults by the poverty status of their village. T tests with assumption of unequal variances as well as chi-square tests were used in the analysis. It is worth noting that although both kinds of communities are the same in terms of their propensity to send migrants in general, the poorer communities tend to send more inter-provincial migrants (27% vs. 22%) than the others. This further demonstrates that inter-provincial migration, to a large extent, reflects inter-regional migration, in which individuals migrate from poorer to wealthier regions. Moreover, older adults in the non-impoverished communities tend to have more frequent communication with other people in the community. This suggests a higher level of social support than their counterparts in impoverished villages.
Descriptive Statistics by Poverty Status of Villages.
p < .1. *p < .05. **p < .01. ***p < .001.
Regression Results
Models in Table 3 use adult children’s migration status and the living arrangements of older adults to predict the probability of having depressive symptoms. First, according to Model 2, for the non-coresident older adults with migrant children, their odds of having depressive symptoms are 1.7 (exp(0.54)) times that of the reference group. It seems that the coresident left-behind elderly are not exempted from this “migration penalty” of adult children: Compared with the coresident older adults with no migrant children, their counterparts with migrant children have 40% (exp(0.36) −100%) higher odds of having depressive symptoms. These results support Hypothesis 1. Compared with Model 1, the associations observed in Model 2 are stronger in these key predictors. This suggests that all the additional variables controlled in Model 2, including social support, functional impairments, economic characteristics, and community poverty, help to suppress the association between children’s migration and depressive symptoms among the older adults. Interestingly, for the older adults with no migrant children, their coresident status with adult children does not appear to make a significant difference: The non-coresident older adults are only marginally more likely to have depressive symptoms than their coresident counterparts. Time spent taking care of grandchildren and time spent on farmwork are also associated with increased depressive symptoms. While the left-behind elderly spent more time on household and farmwork than others (Chang et al., 2011), my results show that they are also more prone to depressive symptoms because of this. Importantly, the coefficient of remittances (in thousands) is small (−0.03). This means that adult children might have to send back at least 12,000 yuan during the last year to compensate for the detriments caused to coresident older adults. This figure is 18,000 yuan in cases with a non-coresident older adult. However, in reality, the average remittance during the last year is moderate (1,177 yuan).
Logit and Multilevel Logit Models Predicting Depressive Symptoms Among Rural Older Adults in China (Using Migration Status of Adult Children) 2011.

Note. These models also control for provincial fixed effects.
p < .1. *p < .05. **p < .01. ***p < .001.
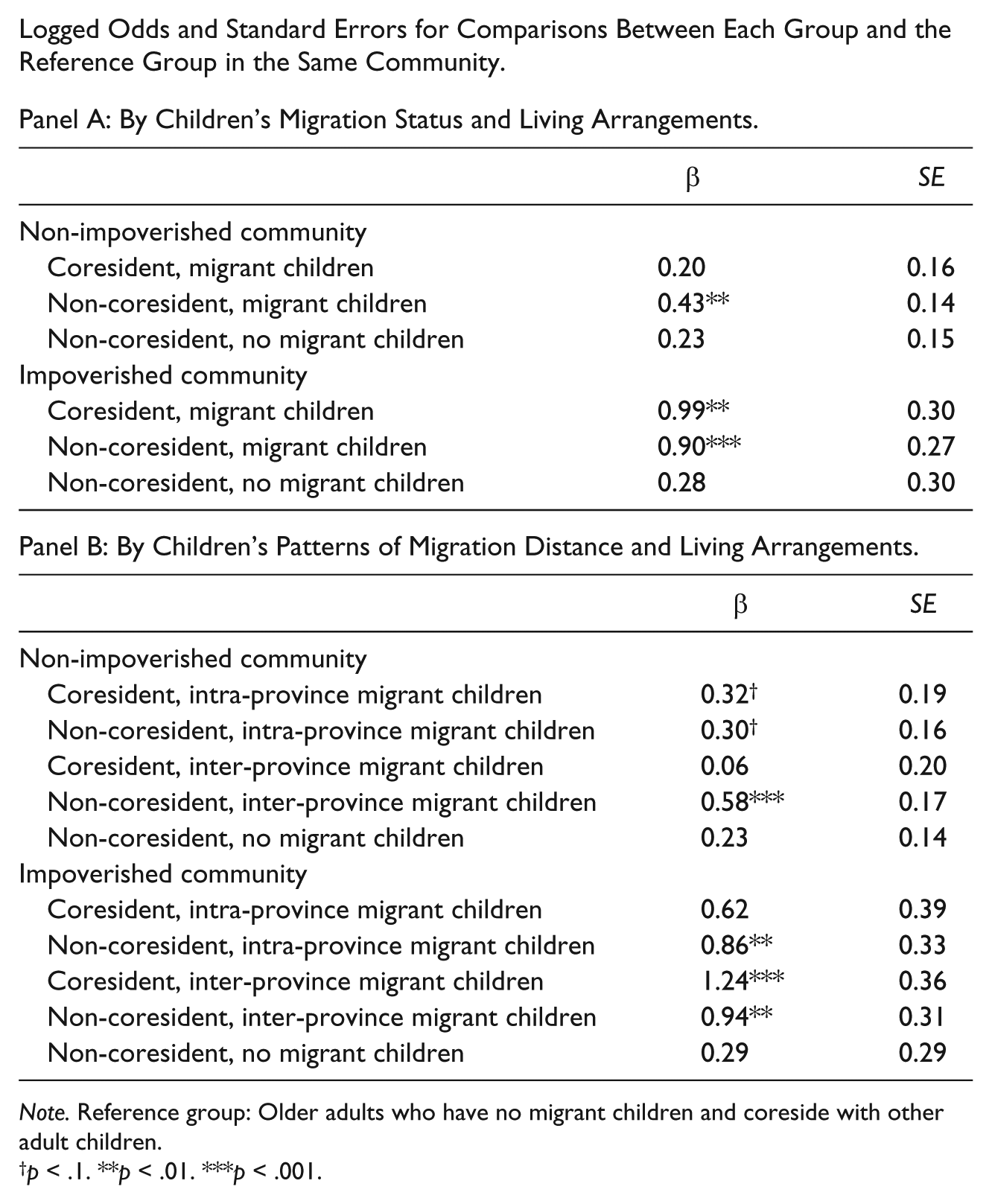
Residing in a community below the poverty line is associated with 70% higher odds of having depressive symptoms. Model 3 demonstrates that the disadvantages observed among the coresident older adults with migrant children are mostly found in this group of older adults residing in impoverished villages. Based on this model, Panel A in Appendix B shows the logged odds and standard errors for comparisons between each group and the reference group in the same community. It is evident that all the left-behind elderly face an aggregated disadvantage by residing in impoverished villages. It appears as if the migration of adult children is a more powerful determinant of older adults’ mental well-being in impoverished villages than in non-impoverished villages. In other words, the left-behind elderly experience “double jeopardy” by simultaneously having migrant children and living in impoverished villages.
Models in Table 4 further disaggregate migration patterns into inter-provincial and intra-provincial migration. Model 4 demonstrates a revealing difference between the two types of children’s migration, especially among the non-coresident left-behind elderly. For the non-coresident left-behind elderly, if their migrant children are all in a different province, they are predicted to have higher odds of having depressive symptoms than their counterparts who have at least one intra-provincial migrant child (the difference in the βs, p < .05, tables not shown). When other mediating variables are controlled, in Model 5, this distinction becomes marginally significant (the difference in the βs, p < .1). This suggests that the additional factors controlled in Model 5, such as familial social support and remittances help to mitigate the mental health disparities created by this additional distance penalty. For the coresident left-behind elderly, this difference in migrant children’s distance patterns is not visible. Therefore, Hypothesis 2 is moderately supported with the condition of non-coresidence with adult children. It is also worth noting that for the parents of inter-provincial migrants only, living with adult children significantly decreases the odds of having depression symptoms (the difference in the βs, p < .05). This suggests that when migrant children are engaging in a long-distance migration, coresidence with adult children is particularly crucial for the mental health of the older adults. Model 6 demonstrates the moderating role of community poverty. The disadvantages of coresident older adults with inter-provincial migrant children are mostly found among those residing in impoverished villages. According to Panel B in Appendix B, it is apparent that such a “double jeopardy,” observed among the left-behind elderly in impoverished villages, is more prominent among parents of inter-provincial migrants.
Logit and Multilevel Logit Models Predicting Depressive Symptoms Among Rural Older Adults in China (Using Adult Children’s Patterns of Migration Distance) 2011.
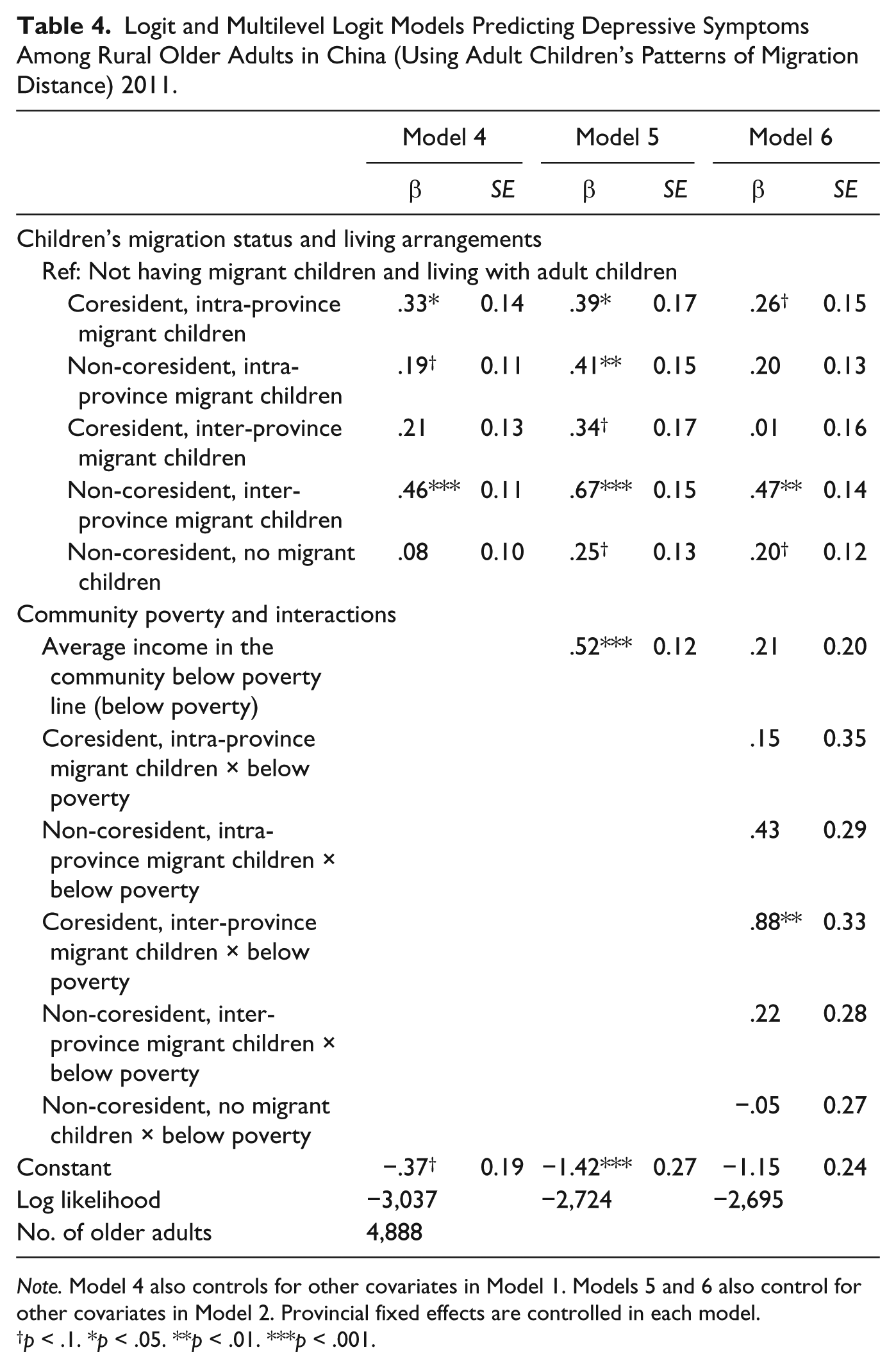
Note. Model 4 also controls for other covariates in Model 1. Models 5 and 6 also control for other covariates in Model 2. Provincial fixed effects are controlled in each model.
p < .1. *p < .05. **p < .01. ***p < .001.
Table 5 reports predicted probabilities of having depressive symptoms for all rural older adults. According to Panel A, older adults who have migrant children and reside in impoverished communities have the highest probability of having depressive symptoms (.51 and .49, depending on their living arrangements). Panel B further demonstrates that among the left-behind elderly, the parents of all inter-provincial migrants are penalized even heavier (.56 and .50) than parents who have intra-provincial migrant children (.44 and .48). Another finding is that for older adults without migrant children, there is only a modest difference (.33 vs. .38) in the probability of having depressive symptoms between different living arrangements (coresidence vs. non-coresidence). This finding suggests that previous studies that considered only the association between living arrangements and the well-being of the older adults may be biased in that they neglect the important heterogeneities that lie in children’s migration status, as well as the poverty status of the residing village.
Predicted Probabilities of Having Depressive Symptoms for Rural Older Adults, 2011.
Panel A: By Children’s Migration Status and Living Arrangements.

Conclusion
Traditional family values in China emphasize filial support from adult children, and coresiding with adult children is a culturally expected living arrangement as individuals age (X. Chen & Silverstein, 2000). Although the process of economic development and modernization has weakened these traditional norms, by 2000 the majority of the elderly population (65+) still coresided with their children (Zeng & Wang, 2003). However, as internal migration from rural areas continued to intensify over the past decade, an increasing number of rural older adults have been forced to experience changes in such traditional family structure. This analysis shows that whereas still 50% of rural older adults without a migrant child lived with an adult child by 2011, only 38% of parents of migrants did so.
Extant studies have consistently found that coresidence with adult children is associated with better subjective well-being and the emotional health of the older adults in rural China (F. Chen & Short, 2008; X. Chen & Silverstein, 2000; Qian & Knoester, 2015). The results of this study reveal important heterogeneities in the associations between living arrangements and the psychological well-being of rural older adults in China. When traditional family arrangements for the older adults—older adults with no migrant children and who coreside with adult children is used as a reference, the analysis finds that coresident older adults with migrant children still experience an increased probability of having depressive symptoms. In particular, when the left-behind elderly also reside in impoverished villages, where support from the community is lacking, they even face aggregated probability of having depressive symptoms—in effect “double jeopardy.” Older adults are the worst off in terms of mental health when they have all their migrant children in a different province, do not coreside with any other children, and reside in an impoverished village. In contrast, for the older adults without migrant children, those who do not coreside with adult children are, at most, marginally more likely to develop depressive symptoms than their counterparts who do coreside with children. And, this association is on a much smaller scale than those in the previous cases.
Living in proximity to adult children is another living arrangement that has been increasing over the past decades. Some argue that this living arrangement may benefit the older adults by obtaining flexible support from adult children while maintaining a level of self-independence. However, this analysis did not find a significant association in terms of depressive symptoms in the rural older adults. This may be because the preference for coresidence with adult children in rural China remains strong, as opposed to in urban China where the older adults usually have better SES and better health care, leading to a preference for independent living (Sereny, 2011). An additional possibility is that the mental health of older adults in turn influences the decisions of children’s migration and living arrangements. This scenario is discussed in detail below.
So what are the possible psychosocial pathways that link children’s migration and their elderly parents’ depression? These pathways may include reducing face-to-face interactions with, and perceived support from, migrant children; inducing anxieties toward migrant children; and creating greater disparities of emotional cohesion with their children. Each of these pathways has been proven to be associated with decreased mental well-being among older adults. For the non-coresident older adults, adult children’s inter-regional migration, in particular, may translate into an even greater reduction in face-to-face interactions with the migrant children, as well as a further loss of anticipated support from children. According to results not reported here, female older adults are affected more in the case of their children’s migration. This is consistent with the findings derived from various contexts that indicate that females are more likely to derive stress from the realm of family than males (Aneshensel & Pearlin, 1987). Community context may play an important role in buffering these emotional strains associated with children’s outmigration. However, residing in impoverished communities could alternatively add to such strains if economically deprived communities have fewer resources, lack supportive social networks, and accordingly expose individuals to high stress environments (Yen et al., 2009).
It is also important to note that there are other ways adult migration impacts the well-being of older adults, in addition to bringing changes to living arrangements. First, spousal migration has become increasingly popular over the years, making caregiving from grandparents a necessity. Many left-behind elderly have to spend extensive hours caring for the left-behind children. More hours of caregiving is associated with worse mental status. The same can also be said for increased household chores and farmworks for older adults, after their children have migrated. It is also true that migrant children transfer more money to their elderly parents left-behind, which improves mental health. The amount of remittances, nonetheless, on average, does not fully compensate for the loss of their parents’ mental well-being. Finally, considering the fact that impoverished villages are usually located in the poorer regions, families in these villages usually send more inter-regional migrants. It is not hard to imagine that the scale of older adults facing such “double jeopardy” can be substantial.
Policy Implications
These results also carry important policy implications. First, this study identifies the group of left-behind elderly who are most in need—non-coresident parents of inter-provincial migrants who reside in impoverished villages. Given that the Western region holds the majority of high poverty rural communities, and is the major inter-provincial/inter-regional migrant point of origin, this region should enjoy more favorable development policies to draw migrants back to their home provinces. Although China’s Western Development Project has built much infrastructure in the Western region, policies and resources should be devoted to facilitating employment opportunities for migrant workers in these areas. In addition, the role of rural communities should be addressed and enhanced. This includes their role in providing resources, providing social support, and improving the psychological well-being of older migrant parents, and older adults as a whole.
Limitations of the Study and Directions of Future Research
As with many studies on familial migration outcomes, one concern of the study is reverse causation. One such scenario is the selectivity of migration on the older parents’ health conditions. Adverse condition of older parents could directly impinge on adult children’s migration decisions, and therefore, keep them around the parents. Alternatively, it could drive the migrants back home, causing return migration (Giles & Ren, 2007). A “healthy migrant effect” may also occur, in which migrants are positively selected based on their mental health status, such that parents of migrants might also share a latent genetic disposition for good mental health, such as determination or optimism (Palloni & Arias, 2004). Nevertheless, this selectivity can be considered at a moderate level. In traditional Chinese values, in stark contrast to physical impairment, depressive symptoms are not regarded as a health condition, and especially not a disease for adult children to constantly attend to. Furthermore, to date, current literature on the healthy migrant effect in China can only be found on the physical health of migrants, not psychological distress (J. Chen, 2011). Nonetheless, should this scenario happen, the negative effect of migration should be even more pronounced than what has been observed in this study.
Although caution is needed in interpreting the results, this study has also utilized and controlled the wide range of factors that are the usual suspects to cause migration selectivity and reverse causation. These variables include older adults’ social activities, amount of financial transfers from non-resident children, household income, time spent on farming and time spent caring for grandchildren, and functional impairments, which could go hand in hand with depression.
The current data also do not allow me to assess the duration of migration, which is another important dimension of the migration process. Longer duration of migration may create more loneliness or anxiety for the left-behind parents. Alternatively, it may over time make them feel more settled with the current arrangements, and thus improve their mental health. In the future, it would be fruitful to position the role of migration duration in shaping the trajectories of the mental health of the left-behind elderly.
Footnotes
Appendix A
Appendix B
Logged Odds and Standard Errors for Comparisons Between Each Group and the Reference Group in the Same Community.
Panel A: By Children’s Migration Status and Living Arrangements.
| β | SE | |
|---|---|---|
| Non-impoverished community | ||
| Coresident, migrant children | 0.20 | 0.16 |
| Non-coresident, migrant children | 0.43** | 0.14 |
| Non-coresident, no migrant children | 0.23 | 0.15 |
| Impoverished community | ||
| Coresident, migrant children | 0.99** | 0.30 |
| Non-coresident, migrant children | 0.90*** | 0.27 |
| Non-coresident, no migrant children | 0.28 | 0.30 |
| Panel B: By Children’s Patterns of Migration Distance and Living Arrangements. | ||
| β | SE | |
| Non-impoverished community | ||
| Coresident, intra-province migrant children | 0.32 † | 0.19 |
| Non-coresident, intra-province migrant children | 0.30 † | 0.16 |
| Coresident, inter-province migrant children | 0.06 | 0.20 |
| Non-coresident, inter-province migrant children | 0.58*** | 0.17 |
| Non-coresident, no migrant children | 0.23 | 0.14 |
| Impoverished community | ||
| Coresident, intra-province migrant children | 0.62 | 0.39 |
| Non-coresident, intra-province migrant children | 0.86** | 0.33 |
| Coresident, inter-province migrant children | 1.24*** | 0.36 |
| Non-coresident, inter-province migrant children | 0.94** | 0.31 |
| Non-coresident, no migrant children | 0.29 | 0.29 |
Note. Reference group: Older adults who have no migrant children and coreside with other adult children.
p < .1. **p < .01. ***p < .001.
Acknowledgements
The author thanks Jennifer Glick, Zai Liang, Kate Strully, Nancy Denton, Glenn Deane, and Zoya Gubernskaya for their insightful comments.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is partly supported by the Karen R. Hitchcock New Frontiers Fund.