
Abstract
Introduction
Our population is getting older at an unprecedented rate (Lyketsos, Sheppard, & Rabins, 2000). From 1980 to 2010, the number of people aged 90 and above had tripled to 1.9 million (Vincent & Velkoff, 2010). This group, referred to as oldest-old, is projected to quadruple by 2050, while individuals aged 60 to 90, here referred to as young-old, are only expected to double during the same time period (Vincent et al., 2010). The oldest-old population is the fastest growing age group in the United States (Guay, Dubois, Corrada, Lapointe-Garant, & Kawas, 2014). As the population continues to age in the coming decades, the disease as well as financial burden associated with an aging population will likely continue to increase, affecting our country’s health care system tremendously (Guay et al., 2014). According to the Alzheimer’s Disease Facts and Figures (2011), Medicare spending has already increased ninefold in the past two decades: from 37 billion in 1980 to 336 billion in 2005. Yet, there is little preparation for this impending “Silver tsunami.”
The rate of growth of this population has left us with an information vacuum regarding certain diseases associated with the oldest-old and their care in hospital settings. One disease that is of greatest concern in this population and one that is believed to have an extremely high prevalence is dementia (Brumback-Peltz, Balasubramanian, Corrada, & Kawas, 2011). Today, there is paucity of information regarding dementia prevalence in the oldest-old and its care in the hospital setting or beyond (Brumback-Peltz et al., 2011).
Several studies have reported reduced rates of dementia incidence after the age of 90 (Holland, Desikan, Dale, & McEvoy, 2012; Miech et al., 2002; Ruitenberg, Ott, Van Swieten, Hofman, & Breteler, 2001). However, recent data have demonstrated that the rate of dementia incidence may continue to increase beyond 90 years of age, even double with every 5.5 years past age 100 (Brumback-Peltz et al., 2011; Corrada, Brookmeyer, Paganini-Hill, Berlau, & Kawas, 2010). Rates of dementia and Alzheimer’s disease in the oldest-old have been published in numerous epidemiological studies, but the number of cases was modest, with wide confidence intervals and rates varying more than eightfold (Brumback-Peltz et al., 2011). Therefore, it has been extremely difficult to demonstrate if the risk of dementia increases, decreases, or levels off after the age 85 (Brumback-Peltz et al., 2011). There are insufficient data regarding gender, race, or other health care characteristics among the oldest-old population, and almost none describing those suffering from dementia in the hospital setting.
In this study, our goal is to identify patients with dementia in the oldest-old age group using the Nationwide Inpatient Sample (NIS), explore the mortality and comorbidity rates, examine racial/ethnic and gender variations, as well as develop a better understanding of care of oldest-old patients in the hospital setting.
Method
A retrospective analysis was performed using the NIS data for the years 1999 to 2008. The NIS is a database maintained as a part of the Healthcare Cost and Utilization Project (HCUP) sponsored by the Agency for Healthcare Research and Quality (AHRQ). It represents 20% of the U.S. community hospitals, comprising 5 to 8 million inpatient records per year. It captures discharge-level information on primary and secondary diagnoses, including procedures, discharge vital status, and demographics. The sampling strategy selects hospitals from State Inpatient Database according to defined strata, based on ownership, bed size, teaching status, urban/rural location, and region. All discharges from sampled hospitals for the calendar year are then selected for inclusion into NIS. To allow extrapolation for national estimates, both hospital and discharge weights are provided. Detailed information on the design of the NIS is available at http://www.hcup-us.ahrq.gov.
The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) was utilized to analyze primary or secondary diagnosis of dementia as demonstrated in Table 1 (290.X, X including 290.0, 290.10, 290.11, 290.12, 290.13, 290.20, 290.21, 290.3, 290.40, 290.41, 290.42, 290.43; 294.1, and 331.X, X including 331.0, 331.11, 331.19, 331.82).
Characteristics of Dementia and Non-Dementia Hospitalizations Among the Oldest-Old in the United States, 1999-2008.
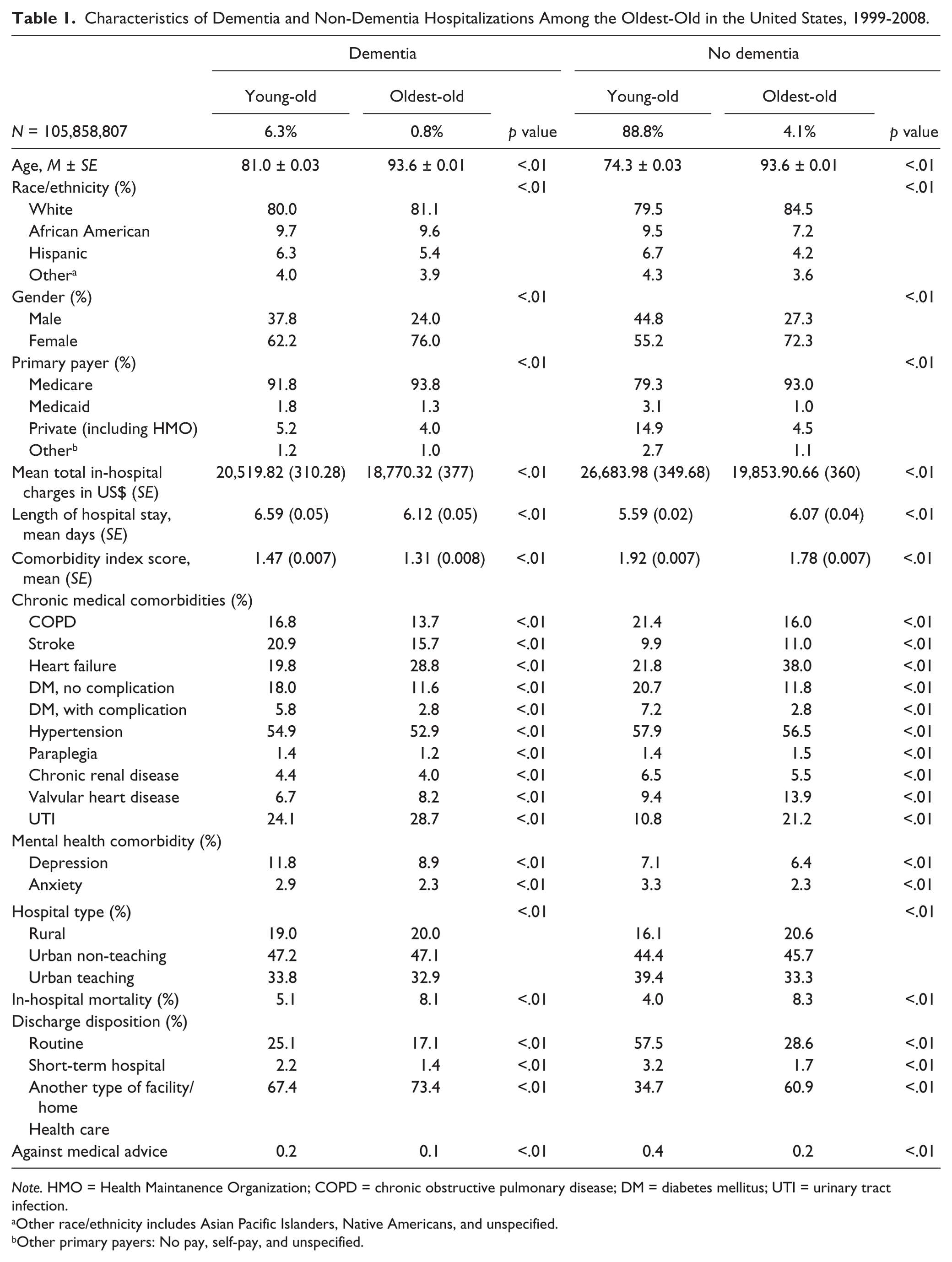
Note. HMO = Health Maintanence Organization; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus; UTI = urinary tract infection.
Other race/ethnicity includes Asian Pacific Islanders, Native Americans, and unspecified.
Other primary payers: No pay, self-pay, and unspecified.
The study population was stratified into two age groups: 60 to 90 years of age and greater than 90 years of age. In the NIS database, the patient’s race is categorized as White, African American, Hispanic, Asian or Pacific Islander, Native American, and Other. In this study, we chose to include Whites, African Americans, and Hispanics only because of very low numbers of individuals in the Pacific Islander and Native American populations. Primary payers included Medicare, Medicaid, private insurance, self-pay, no charge, and other. The Charlson comorbidity index score was used as a measure of medical comorbidity, for each admission, based on ICD-9 codes. Comorbidities included chronic obstructive pulmonary disease (COPD), stroke, heart failure, diabetes mellitus (DM) with no complications, DM with chronic complications, hypertension, paraplegia, chronic renal disease, valvular heart disease, HIV/AIDS, urinary tract infection (UTI), depression, and anxiety. Using Charlson’s comorbidity index, we were able to highlight differences in the distribution of medical comorbidities in the different groups.
Statistical Analysis
Descriptive statistics and normalization of the skewed continuous variables were performed, and the data were presented as mean and standard error. The primary outcome (mortality) and categorical independent variables were presented as number and percentage. Among the group with dementia, we conducted a χ2 test to test the statistically significant difference between the age groups (young-old and oldest-old) in the mortality and the other independent variables. Among the group with no dementia, we conducted another χ2 test to test the statistical significance between the age groups (young-old and oldest-old) in the mortality and the other independent variables. We considered p < .05 to be statistically significant. We examined trends in the distribution of these variables from 1999 to 2008. Thereafter, crude in-hospital mortality in the gender groups and the racial/ethnic groups by age group (young-old and oldest-old) were examined in cases of dementia. We also explored the relationship between the gender and race/ethnicity and in-hospital mortality of dementia hospitalizations stratified by age group (young-old and oldest-old) using univariate and multivariable Cox proportional Hazards Regression analysis estimating the hazard ratio (HR). Adjustments in the multivariable models were made for insurance, socio-demographic factors (race/ethnicity and gender), clinical comorbidity (COPD, stroke, heart failure, DM, hypertension, paraplegia, chronic renal disease, valvular heart disease, UTI, depression, and anxiety), and hospital characteristics (length of stay and hospital type). Appropriate NIS sampling and design parameters were applied during this analysis. All data analyses were conducted using SPSS, version 20.0 (IBM corporation, Armonk, NY) with the complex samples module and SAS, version 9.3 (SAS Institute, Cary, NC). This study was deemed exempt by the Loma Linda University Institutional Review Board.
Results
Table 1 demonstrates the baseline demographics of the participants with and without dementia in the young-old and the oldest-old population. The mean age of dementia cases in the young-old cases was 81.0 ± 0.03 and 93.6 ± 0.01 for the oldest-old group (p < .01). For both groups, young-old and oldest-old, the population of dementia and no dementia hospitalizations comprised of mostly White race, with percentages higher among the oldest-old population. More women had dementia in both age groups, with higher percentages again in the oldest-old group (76.0%). The dementia and no dementia population mostly had Medicare insurance in both groups. Total hospital charges were higher for the young-old (US$20, 519.82) when compared with the oldest-old (US$18,770.32, p < .01).
Despite the cost, differences were revealed in the length of hospital stay for the dementia cases in the young-old (6.59 ± 0.05 days) and the oldest-old (6.12 ± 0.05 days), and it was statistically significant. The medical burden was slightly higher for non-dementia cases in both age groups: young-old (1.92 ± 0.007) and oldest-old (1.78 ± 0.007). Certain comorbidities were higher in the dementia cases such as stroke, UTI, and/or depression for both age groups. However, mortality was higher in the oldest-old dementia group (8.1%). In addition, higher percentage of oldest-old dementia cases were discharged to other facilities and received home health care (73.4%), compared with the young-old population (67.4).
As demonstrated in Table 2, crude in-hospital mortality for dementia hospitalizations was highest among Whites, followed by Hispanics and African Americans in the young-old group (5.4%, 4.9%, and 4.6%, respectively). However, in the oldest-old population, Hispanics had the highest mortality, followed by Whites and African Americans (9.4%, 8.3%, and 7.4%, respectively; p < .01). The crude in-hospital dementia mortality was higher in men than in women in both age groups (young-old: 5.9% male vs. 4.6% female; oldest-old: 9.9% vs. 7.5%; p < .01).
In-Hospital Dementia Mortality for the Racial/Ethnic and Gender Groups by Age.

Statistically significant at p < .01.
Table 3 demonstrates univariate and multivariate analyses for in-hospital mortality in dementia hospitalized patients for gender stratified by age groups (young-old and old est-old). In univariate analysis, overall, in-hospital mortality was higher for men compared with women in both the young-old (HR = 2.72, 95% confidence interval [CI] = [2.67, 2.77], p < .01) and the oldest-old age groups (HR = 1.26, 95% CI = [1.21, 1.31], p < .01) with cases of dementia. In the adjusted model, although the mortality was attenuated in the young-old, but the pattern did not change, with mortality still higher in young-old males (HR = 1.21, 95% CI = [1.18, 1.23], p < .01) and the oldest-old age groups (HR = 1.22, 95% CI = [1.17, 1.28], p < .01).
Unadjusted and Adjusted Cox Regression Analysis Models for In-Hospital Dementia Mortality for Gender, Odds Ratio (95% CI).

Note. Adjusted for insurance, socio-demographic factors (race/ethnicity), clinical comorbidity and hospital characteristics. CI = confidence interval.
In the unadjusted model, young-old African Americans and Hispanics had lower mortality rates (African Americans: HR = 0.75, 95% CI = [0.72, 0.79]; Hispanics: HR = 0.85, 95% CI = [0.80, 0.91]) with Whites as reference (Table 4). In the unadjusted model for the oldest-old, mortality rates remained low for African Americans (HR = 0.78, CI = [0.72, 0.85]), but increased for the Hispanics, but did not reach statistical significance (HR = 1.03, 95% CI = [0.92, 1.14]; Table 4). Similarly, in the adjusted model, young-old African Americans and Hispanics had lower mortality rates compared with Whites (African Americans: HR = 0.76, 95% CI = [0.72, 0.79]; Hispanics: HR = 0.87, 95% CI = [0.81, 0.92]; Table 4). The mortality rates in the oldest-old African Americans remained low (HR = 0.80, CI 0.74 - 0.87), but increased in Hispanic without achieving statistical significance when compared with Whites (HR = 1.04, 95% CI = [0.93, 1.15]; Table 4).
Unadjusted and Adjusted Cox Regression Analysis Models for In-Hospital Dementia Mortality for Race, Odds Ratio (95% CI).
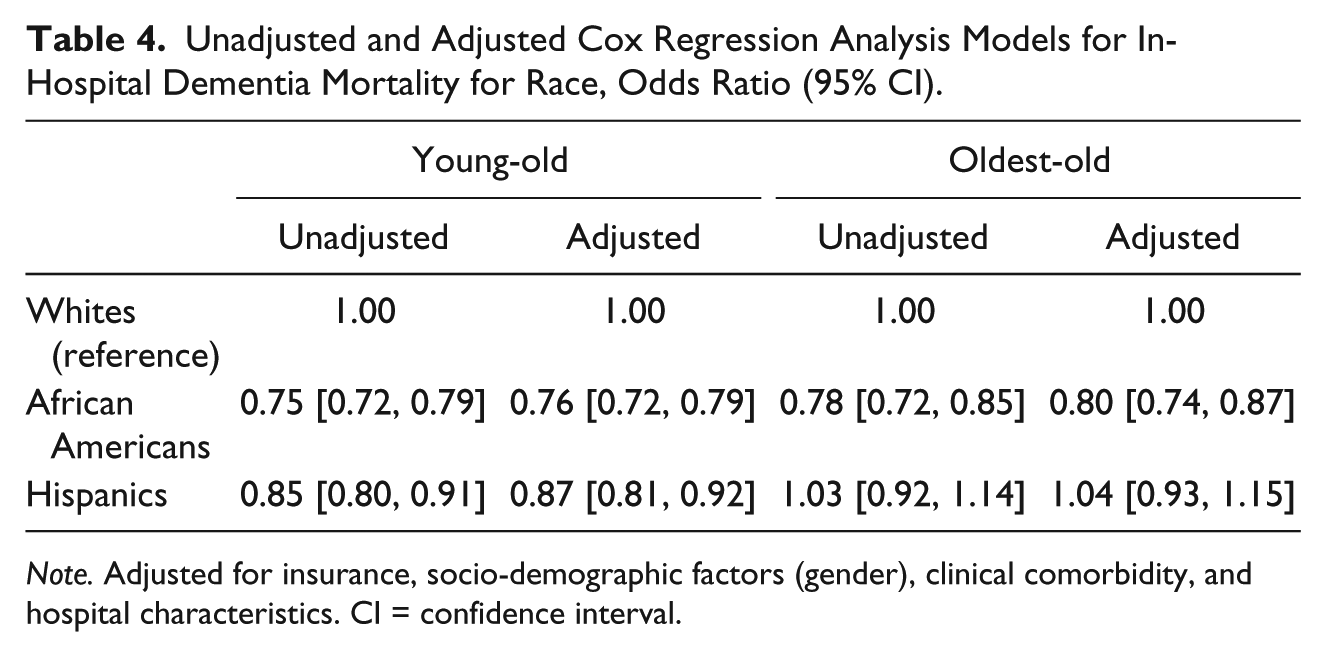
Note. Adjusted for insurance, socio-demographic factors (gender), clinical comorbidity, and hospital characteristics. CI = confidence interval.
Discussion
Given that the oldest-old population is the fastest growing segment of our society, our analyses reveal some intriguing findings. The most interesting revelation was the association between mortality and total in-hospital charges, length of stay, and comorbidity burden among cases of dementia in the oldest-old population when compared with the young-old with dementia. In contrast with previous studies, we found the oldest-old population to have higher in-hospital mortality rates, despite a low comorbidity index score, length of stay, and total in-hospital charges, when compared with the young-old group (Gutterman, Markowitz, Lewis, & Fillit, 1999; Sloan & Taylor, 2002). Although much of these paradoxical findings may be due to patients’ Do Not Resuscitate (DNR) or Do Not Intubate (DNI) status, some of the disparity in the oldest-old population might be due to certain biases, where usual in-patient care may be considered unnecessary, futile, and in many cases harmful toward the oldest-old with dementia (Fried & Gillick, 1994). These biases may be further compounded by cultural nuances, and biases given the disparate odds of mortality that were found among the different races (Heok, 2012).
There were 6,660,483 dementia cases among the young-old and 814,339 among oldest-old (Table 1). The most common comorbidities contributing to admission were stroke, UTIs, and depression when compared with the no dementia population. Despite the high mortality rate among men, consistent with previous findings, majority of the dementia hospital admissions in both age groups were women (Brookmeyer, Gray, & Kawas, 1998). Previous studies have explored factors such as hormonal and genetic influences to explain this greater preponderance for dementia in women (Barron & Pike, 2012; Carroll & Rosario, 2012; Pan & Chang, 2012), but, to date, there have been no conclusive results. Given that, by the middle of this century, the oldest-old is expected to grow exponentially to nearly 9 million and be predominantly female, it is imperative that we further investigate these findings.
Upon controlling for socio-demographic factors, clinical comorbidities and hospital characteristics, mortality for cases of dementia among African Americans in both age groups and Hispanics in the young-old population revealed to be lower when compared with Whites. Given that recent data have shown higher prevalence of dementia in African Americans and Hispanics (Demirovic et al., 2003; Tang et al., 2001), lower hospital admission and mortality may be reflective of underdiagnosis of dementia in the minority population, rather than the true diminished risk of disease. In addition, another possible explanation for our findings might be the low likelihood of hospital usage among minority groups.
The ranks of oldest-old are growing, and concurrently the prevalence of dementia in this age group is increasing exponentially. This will certainly overwhelm the hospitals with elderly dementia patients (Corrada, Brookmeyer, Berlau, Paganini-Hill, & Kawas, 2008). It is thus vital for health care providers to be cognizant of dementia and its hospital-based management for the elderly to improve and enhance their care. However, providing appropriate treatment for the oldest-old with dementia is challenging and also different than providing care for other age groups (Donnelly, McElhaney, & Carr, 2011). An effective approach to care utilized in some emergency departments is the use of the 48/5; meaning within 48 hr of emergency or hospital admission there are five areas in which care plans are developed to address the needs of older patients (Donnelly et al., 2011). These five key areas include delirium/cognition, medications, functional mobility, nutrition/hydration, and bladder/bowel symptoms (Donnelly et al., 2011; Peterson & Bogue, 2011). In acute care settings, specifically focusing on these areas will ensure high-quality care for seniors (Donnelly et al., 2011). Additional education in geriatric care would also be essential in improving treatment plans for the oldest-old (Donnelly et al., 2011). Importantly, as a culture we need to realize that our biases regarding the care of the oldest-old may be false and may need to be revisited in the context of an ever-aging society with evolving beliefs regarding their own end of life care (Heok, 2012).
Given that end-of-life issues are central to the elderly concerns, these data should prompt further research regarding congruence of the wishes of the oldest-old and their treatment in the hospital setting. Hospitals’ inability to effectively recognize the oldest-old population’s health needs is the largest contributing factor as to why systematic treatment and care frameworks are essential components to improving the care for this group (Donnelly et al., 2011). Our study has important strengths, including data on a large oldest-old cohort, among whom the diagnosis of in-hospital dementia has been less frequently studied. In addition, our sample also consists of the largest number of cases of in-hospital dementia comparing the two age groups: young-old (60-90 years of age) and the oldest-old (>90 years of age).
Limitations
Our study has several limitations as well, including the use of administrative data that extrapolate dementia occurrence using ICD-9 codes. Coding errors may be over- or underreported. Medical comorbidity patterns described in this study are also dependent on appropriate coding. Although rare, discharge disposition and mortality estimates may not account for transfer between hospitals or facilities for the selected population.
Diagnosis of dementia in the oldest-old is arduous and prone to significant mistakes due to difficulty in use of daily functional capacity as a part of the diagnosis (McKhann, Drachman, Folstein, Katzman, Price, & Stadlan, 1984). In this group, daily functional capacity is often influenced by physical rather than cognitive decline. In the minority population, diagnosis of dementia has proven to be more challenging, as language and cultural nuances add layers of complexity to the process of diagnosis. An additional limitation is the nature of cross-sectional studies and their intrinsic limitation toward drawing cause-and-effect relationships.
Conclusion and Future Study
In conclusion, we found that in patients with a diagnosis of dementia, the length of hospital stay was shorter for the oldest-old and the cost of care was less. Men had a greater risk of dying from dementia in the hospital settings, while the oldest-old women had significantly greater prevalence of dementia. Ostensibly, it appears that minorities have lower prevalence of dementia and lower dementia mortality in the hospital setting. Further work is needed to clarify whether this is a diagnostic bias or related to true underlying risk and physiological differences, and whether the lower spending on the older dementia patients represents patient and family-driven decisions related to care in late stages of a chronic disease, or partial indifference on the part of the health care community. It is critical to understand that to treat dementia in the oldest-old, health care professionals need to be aware of the appropriate interventions for this age group. Given the rapidly growing numbers of elderly being hospitalized with a diagnosis of dementia and the paucity of any data on this population, we believe this information will serve as a foundation for further research.
Footnotes
Acknowledgements
The authors thank the National Health and Nutrition Examination Survey (NHANES) for providing data and instructions on usage.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by Hasso account for Neuroscience Research.