
Abstract
As the baby boom cohort ages, there is an increasing need to address the growing number of individuals who are likely to develop cognitive impairment, functional decline, and dementia. Alzheimer’s disease (AD), the most common form of dementia in older adults, is one of the primary causes of accelerated cognitive decline, and is the sixth leading cause of death in the United States (Carlson & Varma, 2015). With worldwide prevalence of AD expected to quadruple by 2050, effective means of reducing the incidence of AD and precursors of AD are needed. Preclinical interventions may be important in altering progression of cognitive impairment and dementia as current treatment interventions post-diagnosis are relatively ineffective (Engelhart et al., 2002; Petersen et al., 2005). As such, there is great interest in identifying modifiable risk factors to formulate effective interventions and policies to delay and prevent cognitive impairment in later life.
Physical activity is a promising target for preventive intervention, as numerous observational and trial-based studies have demonstrated cross-sectional associations between remaining physically active and cognitively healthy in older adults (Carlson et al., 2012; Colcombe & Kramer, 2003; Hamer & Chida, 2009; Kramer et al., 1999; Larson et al., 2006; Ngandu et al., 2015; Studenski et al., 2006). In addition, physical activity may prevent or delay the onset of age-related cognitive impairment later in life, even among the oldest-old (Middleton et al., 2011; Sumic, Michael, Carlson, Howieson, & Kaye, 2007). For instance, Sumic and colleagues (2007) showed that women (Mage = 88.5 years) who exercised more than 4 hr per week reduced their risk of cognitive impairment by 88% compared with less active women. Similarly, the bulk of evidence to date suggests a dose–response relationship between physical activity and the preservation of cognitive functions, with greater hours and intensity of fitness-related activity being associated with better cognition (Colcombe & Kramer, 2003; Weuve et al., 2004).
Studies have also examined the impact of physical activity on AD and dementia and suggest that regular exercise, defined as exercising 3 times a week, can delay the onset of these diseases (Larson et al., 2006; Laurin, Verreault, Lindsay, MacPherson, & Rockwood, 2001). Moreover, Larson and colleagues (2006) found that the effects of exercise on dementia risk reduction were greatest in individuals with the lowest baseline physical functioning levels. However, these findings are mixed. For instance, Wang, Karp, Winblad, and Fratiglioni (2002) were unable to find a significant beneficial association between physical activity and dementia incidence after accounting for participation in other social and cognitive activities. This analysis may have had limited power to detect such an association as very few people reported engagement in physical activity, partially confirmed by a later study in this cohort showing positive associations between objectively measured physical activity and dementia risk (Buchman et al., 2012). Other studies have also failed to find a significant association between self-reported physical activity and risk of cognitive impairment or dementia (Verghese et al., 2003).
Inconsistencies in findings may be due to differences in methodological approaches, cognitive domains investigated, or measurement of physical activity. The majority of studies have used global measures of cognition, such as the Mini-Mental State Exam (MMSE). However, investigating distinct cognitive domains may be more informative, as other studies and exercise trials have demonstrated beneficial effects of physical activity on executive processes (Carlson et al., 2012; Colcombe & Kramer, 2003). Gaining a better understanding of how physical activity affects distinct cognitive domains would help identify potential targets for slowing the progression of cognitive impairment.
Studies have also used various physical activity assessments making it difficult to compare findings across studies. Inconsistencies in how to best define the frequency, duration, and intensity of activity have led to several definitions of physical activity (Hamer & Chida, 2009). These alternative measures of physical activity include questionnaires of self-reported frequency of exercise in days or hours per week (Laurin et al., 2001) or physiologic measures such as maximum oxygen volume during exercise tasks (Colcombe & Kramer, 2003). Furthermore, some self-report studies have used only athletic activities or segregate low intensity exercise from high intensity exercise (Lindwall, Rennemark, & Berggren, 2008). The majority of studies, however, ask about the number or frequency of physical activities, without accounting for varying levels of intensity across activities or specific caloric expenditures as a result of these activities.
The Minnesota Leisure Time Physical Activity Questionnaire (MLTPAQ; Taylor et al., 1978), captures intensity levels of physical activity in terms of kilocalories per week (i.e., estimate of caloric expenditure). This estimate provides a more specific and quantifiable measure of self-reported physical activity. Using this measure, it has been shown that greater caloric expenditure is associated with a lowered risk of cognitive impairment (Middleton et al., 2011). Podewils and colleagues showed quantity of physical activities was inversely associated with risk of dementia among individuals without genetic risk of dementia (Podewils et al., 2005).
The present study focuses on the relationship between baseline physical activity as defined by caloric expenditure using the MLTPAQ and risk of cognitive impairments in later life in a cohort of initially high-functioning older women over a 9-year interval. The cognitive domains measured included executive function, verbal memory, and psychomotor speed. Comparison across multiple domains allows us to more specifically identify those cognitive components most strongly linked to physical activity. Based on prior work, we will examine whether the associations may be especially pronounced for executive functioning, a domain that is particularly vulnerable to aging and affected by exercise (Carlson, Xue, Zhou, & Fried, 2009; Colcombe & Kramer, 2003; Kramer et al., 1999; West, 1996).
Method
Sample
The Women’s Health and Aging Study II (WHAS II) is a prospective study evaluating the least disabled two thirds of 70- to 80-year-old women in eastern Baltimore, MD (Carlson et al., 2009). WHAS II was designed to evaluate the epidemiology of disability onset within 436 high-functioning community-dwelling women. This study complemented the WHAS I, a study of the one-third most disabled older women (Guralnik, Fried, Simonsick, Kasper, & Lafferty, 1995). The sampling frame for WHAS II was based on the same survey population as WHAS I, female Medicare beneficiaries on Health Care Financing Administration Medicare eligibility lists. Study aims, sampling designs, and recruitment methods can be found in detail elsewhere (Carlson et al., 1999).
Briefly, following baseline interviews, 5 follow-up exams were administered in 1.5-year intervals, with the exception of a 3-year interval between Exams 3 and 4, spanning a 9-year period. To be eligible for participation, individuals had to be (a) aged 70 to 79 years; (b) proficient in English and sufficient hearing to comprehend questions; (c) able to be contacted by telephone; (d) free of substantial cognitive impairment as indicated by an MMSE (Folstein, Folstein, & McHugh, 1975) score >23; and (e) display no difficulty in more than one of the following functional domains: mobility and exercise tolerance, upper extremity, higher functioning, and basic self-care (Fried, Bandeen-Roche, Kasper, & Guralnik, 1999). The Johns Hopkins Institutional Review Board reviewed and approved the study. Written, informed consent was obtained from all participants before each interview.
A total of 436 women comprised the WHAS II sample. Of 436 participants, 60 were excluded from this study because they were missing baseline caloric expenditure data, died during follow-up, or did not have complete follow-up data for at least one cognitive test. This resulted in 376 individuals eligible for this study. The 60 individuals excluded had lower education (p < .001), lower MMSE scores (p < .003), lower caloric expenditure (p < .02), and were more often non-White (p < .02) than the remaining sample. This group was comparable in age and comorbidities to those with all available data.
Measures
Cognition
Cognitive measures included a measure of global cognitive status (MMSE; Folstein et al., 1975) and several distinct cognitive abilities, including psychomotor speed, executive function, and verbal memory. The two-part Trail Making Test (TMT; Reitan, 1958) was used to evaluate psychomotor speed (Part A) and executive function (Part B). Participants were timed to completion, with a maximum allotted time of 240 s on Part A and 360 s on Part B. Times on the TMT were transformed to speed, in minutes (1/completion time in minutes), such that higher scores indicated better performance.
The Hopkins Verbal Learning Test (HVLT-R; Benedict, Schretlen, Groninger, & Brandt, 1998) was used to assess verbal immediate and delayed recall memory. Participants were scored based on the total number of words correctly recalled from a 12-word list over three learning trials (immediate recall) and following a 20-min filled interval (delayed recall). Higher HVLT scores indicated better performance.
Time to impairment for each test was defined as the initial onset of impairment and treated as a terminal event. Impairment cutoffs were defined as performance below 10th percentile values, using age- and education-matched norms (Carlson et al., 2009). Specifically, cutoff scores are as follows: (a) TMT Part A ≥81 s, (b) TMT Part B ≥225 s, (c) HVLT immediate recall ≤16, and HVLT delayed recall ≤4. For each test, participants with prevalent impairment at baseline, either on that test or globally based on MMSE scores, were removed from analysis. This resulted in the exclusion of 18 participants for the TMT A (n = 358), 32 participants for the TMT B (n = 344), 34 participants for the HVLT immediate recall (n = 342), 28 participants for the HVLT delayed recall (n = 348), and 3 participants for the MMSE analysis (n = 373).
Physical activity
Physical activity was measured by a modified version of the MLTPAQ (Taylor et al., 1978) asking six questions regarding activities most applicable to older individuals, including strenuous household chores, strenuous outdoor chores, dancing, bowling, walking, and participation in a regular exercise program, such as stretching or swimming. Individuals were asked to self-report the frequency and duration of participation in these six physical activities over the past 2 weeks. Caloric expenditure was calculated by assigning intensity weights to different activities and estimating the total caloric expenditure of the activity by multiplying the intensity by the duration.
Data Analyses
Discrete-time Cox proportional hazard regression models were used to examine the relationships between physical activity and domain-specific cognitive impairments over a 9-year period (Singer & Willett, 1991). Models were adjusted for age (years), education (years), race (White vs. non-White), number of chronic diseases, and depressive symptoms measured by the Geriatric Depression Scale (Yesavage et al., 1983) at baseline. The model for the TMT B also adjusted for TMT A scores at baseline. Baseline caloric expenditure was modeled as a categorical predictor in quintiles. Hazard ratios were generated for comparisons against the reference group (bottom quintile of individuals).
Results
Baseline demographic and health characteristics of the sample (N = 376) are summarized in Table 1. At baseline, participants were, on average, 74 years old, 17% African American, and most had a high school education (M = 12.7 years; SD = 3.2). The participants were in relatively good cognitive (MMSE: M = 28.2; SD = 1.8) and physical health (chronic health conditions: M = 1.5; SD = 1.0). In terms of physical activity, the majority of our study population was active, with 59.3% of individuals reporting more than 150 min/week of moderate intensity physical activity, at baseline. Only a small percentage of individuals could be classified as sedentary. Specifically, 23 individuals (6.12%) were inactive at baseline with 0 min/week of moderate intensity physical activity and 34.6% of individuals were performing insufficient physical activity, more than 0 min/week but less than the recommended 150 min/week.
Baseline Demographic and Health Characteristics of 376 Cognitively Healthy Participants in the Women’s Health and Aging Study II.

Number of chronic diseases is the sum of 14 chronic diseases.
In addition, individuals expended, on average, 1,409.0 kcal per week (SD = 1,598.0), at baseline. For analyses, participants were stratified into quintiles based on baseline caloric expenditure, with the least active quintile expending less than 336 kcal per week whereas the most active quintile expended greater than 2,213 kcal per week.
Table 2 shows the findings from models adjusted for age, race, years of education, number of chronic diseases, and depressive symptoms at baseline. Furthermore, individuals in the highest quintile of caloric expenditure had better TMT B speed, as compared with individuals in the lowest quintile of activity (p < .03). There were trends toward reduced risk of cognitive impairment in TMT A (p = .06) and delayed recall in participants reporting moderate levels of physical activity (p = .09), although conventional levels of significance were not reached (p’s < .05).
Cox Proportional Hazard Models Examining the Associations Across Quintiles Between Physical Activity and Incident Cognitive Impairments (N = 376).
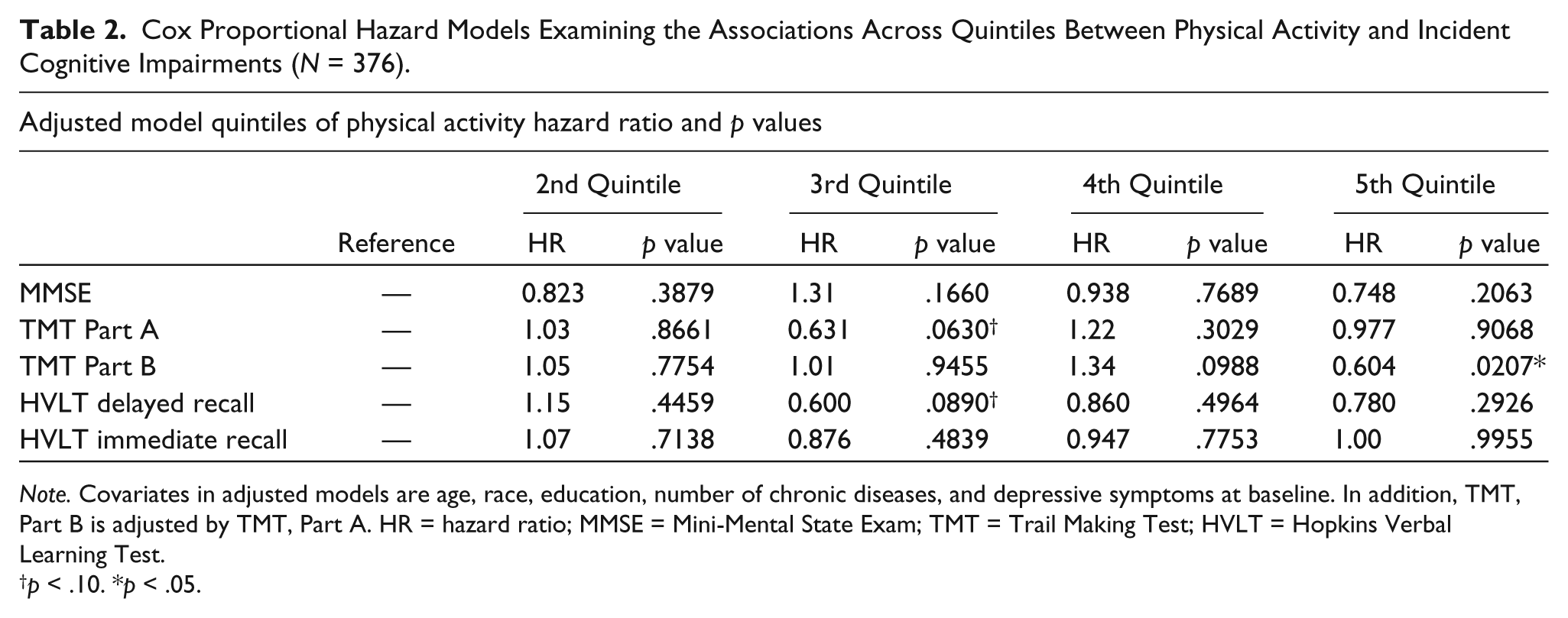
Note. Covariates in adjusted models are age, race, education, number of chronic diseases, and depressive symptoms at baseline. In addition, TMT, Part B is adjusted by TMT, Part A. HR = hazard ratio; MMSE = Mini-Mental State Exam; TMT = Trail Making Test; HVLT = Hopkins Verbal Learning Test.
p < .10. *p < .05.
Discussion
This study examined the associations between physical activity and risk of incident impairment in psychomotor speed, executive function, and verbal memory over a 9-year interval in older women free of cognitive impairment at baseline. Consistent with previous investigations, we found an association between caloric expenditure and improved executive function between women in the most active versus least active quintiles (Carlson et al., 2012; Colcombe & Kramer, 2003; West, 1996). Previous studies have also suggested beneficial effects of physical activity for psychomotor speed (Spirduso, 1980) and delayed recall (Weuve et al., 2004); however, we failed to find similar associations between caloric expenditure and these domains of cognition. Our findings do suggest that moderate levels of physical activity may exert some benefit in reducing incident impairment in psychomotor speed and delayed recall, although these trends did not reach statistical significance. This may indicate that different cognitive abilities are differentially affected according to levels of physical activity, highlighting the importance of measuring moderate, and even lower intensity levels of physical activity for their potential benefits on multiple cognitive domains.
Given the benefits to cognitive health that regular physical activity may confer, it is important to consider how to increase physical activity in older populations that are sedentary and at elevated risk of dementia. Physical activity is already recommended for adults to enhance cardiovascular health and has proven beneficial to prevent several other chronic diseases associated with increased risk of cognitive impairment, such as hypertension, obesity, and type II diabetes (Launer et al., 2000). A recent study found older men who completed 150 min of vigorous physical activity per week were more likely to remain free of mood, cognitive, or functional impairments after 10 to 13 years compared with those who did not complete as much physical activity (Almeida et al., 2014).
The physical activity levels of participants in this study appear to be higher than levels found in other studies of older adults. For comparison, in the Baltimore Experience Corps Trial, Varma and colleagues found that only 7.0% of older men and women were considered active and met physical activity guidelines, compared with 59.3% of individuals in our WHAS II sample (Varma et al., 2013). In addition, a study by Stewart and colleagues (2001) found that 30.5% of older women and men were classified as “inactive” at baseline. Similarly, the Aerobics Center Longitudinal Study of older women found that 70% aged 60+ engaged in less than 150 min/week of moderate intensity physical activity in the past 3 months (Stofan, DiPietro, Davis, Kohl, & Blair, 1998).
Although the exact mechanisms are still unclear, and likely pleiotropic, physical activity may help enrich neural networks and promote efficient processing through cardiovascular and neurotrophic and other pathways (Carlson & Varma, 2015), increasing brain and cognitive reserves that buffer progression to cognitive impairment (Stern, 2006; Verghese et al., 2003). Functional imaging studies have shown that older individuals who engaged in physical activity showed significant increases in brain volume, suggesting a relationship between cardiovascular fitness and brain tissue (Colcombe et al., 2006). Physical activity is also associated with reduced levels of B-amyloid plaque in animal models, a hallmark feature of AD (Adlard, Perreau, Pop, & Cotman, 2005). Increased physical activity may also influence cognitive health through its effects on blood pressure, lipoprotein levels, endothelial function, and increased oxygenation in the brain, thereby increasing the brain’s vascular health (Rosendorff, Beeri, & Silverman, 2007; Taddei et al., 2000).
This study benefits from multiple visits conducted over a period of follow-up longer than many other observational studies of physical activity and cognition. Our study provides further information on a dose–outcome relationship that older adults may experience with increasing levels of physical activity. Because our study sample was selected to be high functioning at baseline, we may have observed higher levels of daily activity than in other studies, as noted above, and were thus able to examine the natural association of physical activity and components of cognition in individuals capable of participating in physical activities.
There are several limitations of this study to consider. First, this study relied on self-reported activity rather than on more objective measures (i.e., step counts), which may yield more accurate estimates of activity and therefore, dementia incidence (Buchman et al., 2012; Carlson & Varma, 2015). Furthermore, it has been shown that self-reported estimates of physical activity on the MLTPAQ may underestimate true total caloric expenditure by 37% to 62%, therefore, our findings may represent conservative estimates of total daily physical activity on cognitive health in older women (Neilson, Robson, Friedenreich, & Csizmadi, 2008). Second, our analyses excluded 60 individuals due to missing baseline caloric expenditure data, death, or incomplete follow-up data on at least one cognitive test. As participants lost to follow-up had lower education, lower MMSE scores, less caloric expenditure, and were more likely to be non-White, it is possible that our results may not generalize to populations with those characteristics. However, our exclusion of these individuals, who were likely to be declining more rapidly, may have led to a more conservative estimate of the impact of physical activity on cognitive decline. More importantly, these findings focused only on older women and may not generalize to older men. However, it is important to investigate these issues in older women who tend to live longer and have an increased risk of cognitive impairment and dementia. Third, a limitation of observational studies is the possibility that physical activity may be an indicator of an overall healthier lifestyle and better cognitive health. As such, those who engage in physical activity may also more likely to engage in a larger number of activities that are associated with improved health behaviors and outcomes (Carlson et al., 2012). For some physical activities, such as dancing, it is difficult to separate the social from the physical demands, which may also benefit cognition in adulthood. Research has also shown that individuals with larger social networks exhibit less cognitive decline than those with smaller social networks (Seeman & Crimmins, 2001). To advance our understanding of the mechanisms of benefit from physical activity and the overlap of physical activity with other types of activity, next-generation research will need to apply objective, real-time measures (Carlson & Varma, 2015).
In summary, our study findings showed that the most versus least physically active older women showed better maintenance of executive function over 9 years. This study corroborates existing evidence that physical activity in daily life plays a particularly important role in this, relative to other domains of cognition in older adults. This finding may be related to the earlier onset of declines in executive function relative to memory observed in this and other cohorts (Carlson et al., 2009). Furthermore, estimates obtained from the MLTPAQ on caloric expenditure suggest that even modestly higher levels of physical activity confer health benefits (Carlson & Varma, 2015). This study serves to provide yet another reason why older adults should be encouraged to partake in a range of daily physical activities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grants R01 AG19825-02 and R01 AG11703-10 from the National Institute on Aging, National Institutes of Health.