
Abstract
Advance care planning (ACP) is a process through which competent adults can discuss their health care goals and communicate their preferences about life-sustaining treatment in the event they are ever unable to make medical decisions for themselves (Brinkman-Stoppelenburg, Rietjens, & van der Heide, 2014). Advance directives, a key component of ACP, are legal forms used to document instructions regarding how future health care decisions should be made (Schmidt, 2015). The living will portion of an advance directive allows individuals to state what medical treatment they would or would not wish to receive. It is also possible to nominate one or more surrogates to make medical decisions on one’s behalf in the event of incapacity. This nomination may be part of an advance directive or in an accompanying document called a durable power of attorney for health care (Institute of Medicine [IOM], 2015).
Although advance directives have their limitations (Ditto & Hawkins, 2005; Emanuel, 1995; Fagerlin & Schneider, 2004; Lo & Steinbrook, 2004; Perkins, 2007; Sudore & Fried, 2010), considerable effort has been made in the United States over the past quarter century to encourage their use. Since 1991, all hospitals, long-term care facilities, hospices, home health agencies, and health maintenance organizations that receive Medicare or Medicaid funding are mandated by the Patient Self Determination Act (PSDA) to provide patients with written information about advance directives at the time of admission or enrollment (U.S. Government Accountability Office [GAO], 2015). National private sector efforts to promote ACP include educational campaigns carried out by the American Bar Association Commission on Law and Aging, the Center for Practical Bioethics, and National Healthcare Decisions Day, to name just a few (IOM, 2015).
The development and promotion of advance directives emerged in response to two fundamental changes in health care over the past half century (U.S. Department of Health and Human Services [HHS], 2008). First, advances in life-sustaining medical care and technology profoundly changed death and dying. Many patients are now able to survive traumatic injuries or serious illnesses that were once fatal. As a result, modern end-of-life decision making increasingly occurs in the hospital and often involves quality-of-life considerations. Second, bioethics moved away from professional benevolent paternalism toward patient autonomy. Advance directives arose in response to the growing need to make difficult end-of-life choices in the context of an emerging recognition of patients’ rights to make these decisions for themselves.
There are disparate data on what extent advance directives influence medical treatment, outcomes, or costs (Brinkman-Stoppelenburg et al., 2014; Detering, Hancock, Reade, & Silvester, 2010; Garrido, Balboni, Maciejewski, Bao, & Prigerson, 2015), but advance directives have been found to be associated with at least some important end-of-life care quality indicators. Having an advance directive increases the odds of dying at home, receiving hospice services for more than 3 days prior to death, not dying on a respirator or feeding tube, and receiving end-of-life treatment consistent with one’s expressed wishes (Bischoff, Sudore, Miao, Boscardin, & Smith, 2013; Kessler & McClellan, 2004; Silveira, Kim, & Langa, 2010; Teno, Gruneir, Schwartz, Nanda, & Wetle, 2007; Tschirhart, Du, & Kelley, 2014). Psychological benefits for family decision makers have also been documented (Tilden, Tolle, Nelson, & Fields, 2001).
Rates of Advance Directive Completion
Advance directive completion among the general public is fairly low in the United States. A 2009 survey found that 29% of adults reported having a living will (defined as written medical treatment wishes; Pew Research Center, 2009). However, rates among older U.S. adults are much higher. The same Pew study found that 54% of respondents aged 65 and older reported having completed a living will. Similar rates were reported by Rao, Anderson, Lin, and Laux (2014), who found that 51% of adults age 65 and older had advance directives (defined in the HealthStyles survey question as a document such as a living will or durable health care power of attorney designed to help others make medical decisions on behalf of the respondent if ever unable). Moreover, a recent report based on exit survey data from the Health and Retirement Study (HRS) suggests that advance directive completion rates among older adults have substantially increased over the past decade. Silveira, Wiitala, and Piette (2014) observed the proportion of decedents aged 60 and older who were reported to have had advance directives (defined as having a living will and/or durable power of attorney for health care) at the time of death increased from 47% in 2000 to 72% in 2010.
Numerous studies have found that older African Americans are significantly less likely to complete advance directives compared with their White counterparts (Carr, 2012a; Degenholtz, Arnold, Meisel, & Lave, 2002; Frahm, Brown, & Hyer, 2012; Gerst & Burr, 2008; Hopp & Duffy, 2000; Kahana, Dan, Kahana, & Kercher, 2004; Kiely, Mitchell, Marlow, Murphy, & Morris, 2001; Kwak & Haley, 2005; Rao et al., 2014; Rich, Gruber-Baldini, Quinn, & Zimmerman, 2009; Welch, Teno, & Mor, 2005). This relatively low rate of written ACP among African Americans is cause for concern given the increased frequency of difficult end-of-life decisions and the likely relationship between advance directives and the quality of care received before death.
Multiple explanations have been proposed for low rates of ACP among African Americans. Some of the most common include mistrust of doctors and the health care system, religiosity and a belief that God determines time of death, lack of knowledge and lower levels of health literacy, reluctance to acknowledge terminal prognosis, fear of receiving too little or lower quality care, implicit racial biases of health care providers, doubt about the efficacy of ACP, and preference for family-centered rather than individual-centered decision making (Blackhall et al., 1999; Bullock, 2006; Hlubocky, 2014; Johnson, Kuchibhatla, & Tulsky, 2008; Ladd, 2014; Murphy et al., 1996; Perkins, Geppert, Gonzales, Cortez, & Hazuda, 2002; Smith, Davis, & Krakauer, 2007; Smith et al., 2008; Waters, 2001).
Prior studies of race disparities in advance directive completion have either considered rates at one point in time or have aggregated data across time. To contribute to our understanding of trends in advance directive completion among older adults, this study examined changes in the rates of advance directive completion among White and African American older adults over a 12-year period using weighted nationally representative data.
Method
Sample and Data
Research was conducted using exit survey data from the HRS (Health and Retirement Study [HRS], 2002-2012), a longitudinal survey of older adults sponsored by the National Institute on Aging (Grant NIA U01AG009740) and conducted by the University of Michigan. When sampling weights are applied, as was done for this analysis, the HRS data are representative of the U.S. population above the age of 50 (Sonnega et al., 2014). The present sample is made up of non-Hispanic African American and non-Hispanic White individuals who died between 2001 and 2012 and for whom exit interviews with surviving proxies were completed between 2002 and 2012. Although the HRS includes Hispanics, this study looks only at African Americans and Whites because the number of Hispanics in the HRS exit survey data was relatively small and because many of the historical and cultural factors that influence ACP among African Americans and Hispanics are different.
Individuals were excluded if they were not age eligible (at least 51 years old) when originally enrolled in the study, were reported to reside outside of the 50 United States at the time of death, were less than 65 or more than 99 years old at death, or for whom no respondent-level sampling weight had been assigned between 1992 and 2012. A minimum age at death of 65 was selected to maximize the uniformity of insurance coverage (94% were on Medicare). The upper age limit of 99 was imposed after preliminary analysis revealed problems with nonlinearity caused by 83 outlier cases (73 White and 10 African American) who were 100 years old or older. Of the 6,114 subjects who met the inclusion criteria, 4.6% were missing data for at least one variable (1.8% advance directive status, 2.6% death expected, and 0.4% marital status). Listwise deletion was used to handle this relatively small amount of missing data.
Measures
During exit interviews, proxies were asked two yes/no questions regarding the deceased subjects’ written end-of-life instructions: “Did [FIRST NAME] provide written instructions about the treatment or care [she or he] wanted to receive during the final days of [her or his] life?” and “Did [FIRST NAME] (also) make any legal arrangements for a specific person or persons to make decisions about [her or his] care or medical treatment if [she or he] could not make those decisions [herself or himself]? This is sometimes called a Durable Power of Attorney for Health Care.”
Consistent with similar studies (Campbell, Edwards, Ward, & Weatherby, 2007; Silveira et al., 2014), those reported to have had written end-of-life instructions, a durable power of attorney for health care, or both were considered to have died with an advance directive.
Changes in rates of advance directive completion over time were compared by race (non-Hispanic White, non-Hispanic African American). Covariates included sex, age at death, education (<high school, high school/general education development (GED), >high school), marital status (married, widowed, separated/divorced, never married), geographic region (Midwest, Northeast, South, West), whether the decedent lived in a nursing home or other health care facility at the time of death (yes, no), and whether death was expected (expected, unexpected).
Analyses
Descriptive statistics were tabulated for the entire sample and by race. Year of death was modeled as a linear spline with four nodes: 2001-2003, 2004-2006, 2007-2009, and 2010-2012. Three-year intervals were chosen to maintain sufficient detail while smoothing trend lines to minimize the noise of year-to-year variations. Pearson chi-square (χ2) tests were used to examine changes in the proportion of written ACP overall and for each racial group. Two logistic regression models were run to predict and compare the odds of having an advance directive at death for African Americans and Whites during each 3-year period. The first model included the independent variables race and time period as well as the Race × Time interaction. In the second model, all control variables were added simultaneously.
The complex sampling design of the HRS was accounted for by using subjects’ most recent (community-dwelling) sampling weights from the 2012 Tracker File. There were no significant issues with multicollinearity, outliers, or nonlinearity. Leverage values greater than expected were observed for 354 cases indicating these may be exerting disproportional influence, although all Cook’s distance values were less than one (Field, 2013; Menard, 2002). All analysis was conducted using SPSS Version 22.
Ethical Considerations
This study was exempted from institutional review board review by the University of Kansas.
Results
Descriptive Statistics
Non-Hispanic African Americans made up 10% of the sample. Seventy-four percent of White decedents were reported to have had an advance directive compared with only 38% of African Americans. A majority (55%) of both the White and African American decedents were female, with no significant gender difference between the two groups. The White and African American sub-samples differed significantly on all the other variables at p < .001. The mean age at death for Whites was just over 82 years, while for African Americans, the mean age was just under 80. The White decedents tended to have more education, with 31% having less than a high school diploma and 32% having at least some college. In contrast, 62% of the African Americans had less than a high school education and 14% had post–high school education. An approximately equal proportion of Whites and African Americans were widowed (48% and 46%, respectively), but a higher percentage of Whites were married (39% vs. 31%) and the proportion of African Americans who were separated or divorced was almost twice that of Whites (16% vs. 9%). There were also geographic differences, with more than half (58%) of African Americans living in the South at the time of death compared with 35% of Whites, who made up higher proportions in the other regions. Death was reported to have been expected for 63% of Whites compared with 53% of African Americans. A lower percentage of African Americans (33%) lived in nursing homes or other health care facilities at the time of death compared with Whites (41%). Weighted statistics and additional descriptive demographic characteristics are presented in Table 1.
Descriptive Characteristics of Sample (Weighted).
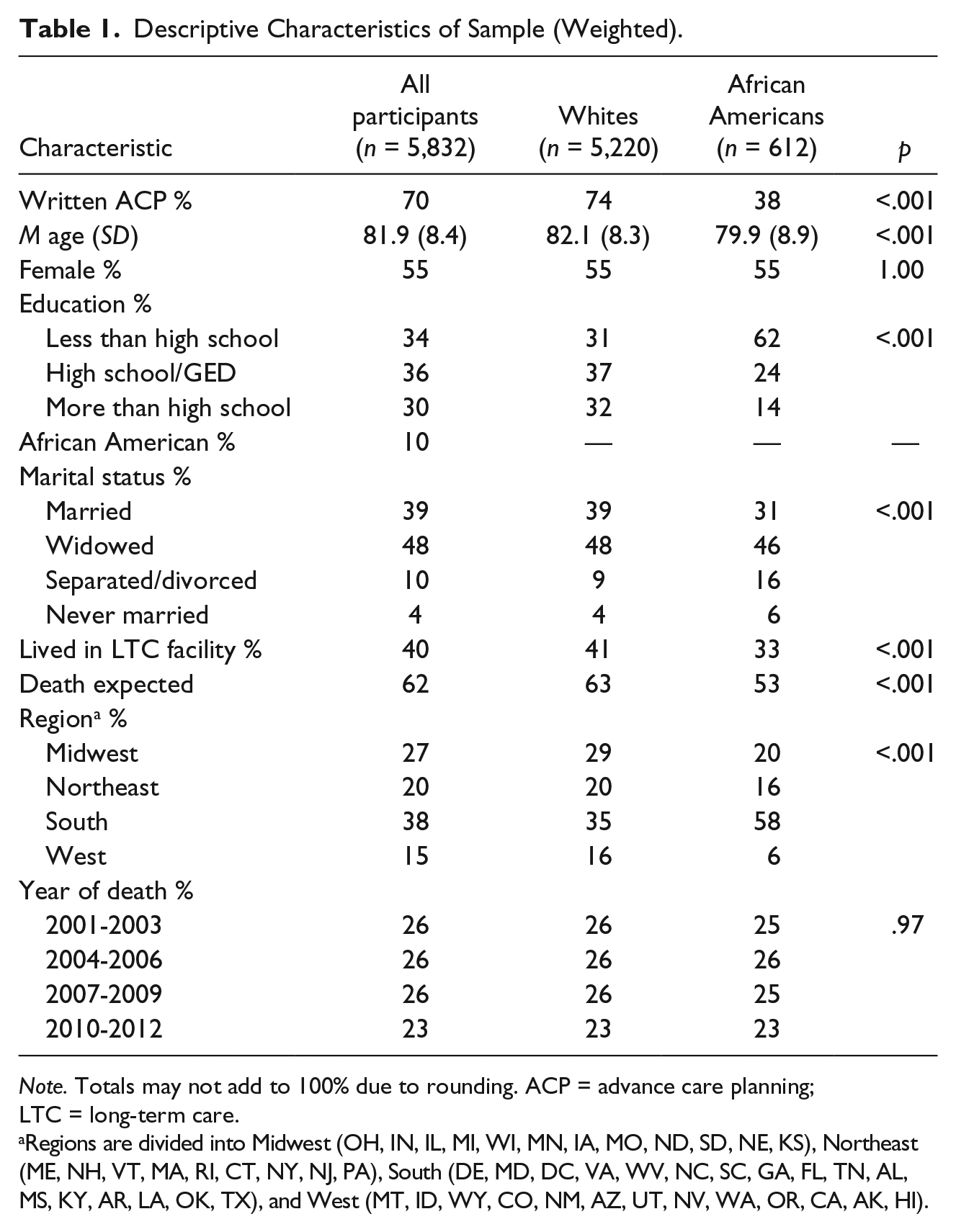
Note. Totals may not add to 100% due to rounding. ACP = advance care planning; LTC = long-term care.
Regions are divided into Midwest (OH, IN, IL, MI, WI, MN, IA, MO, ND, SD, NE, KS), Northeast (ME, NH, VT, MA, RI, CT, NY, NJ, PA), South (DE, MD, DC, VA, WV, NC, SC, GA, FL, TN, AL, MS, KY, AR, LA, OK, TX), and West (MT, ID, WY, CO, NM, AZ, UT, NV, WA, OR, CA, AK, HI).
T tests and chi-square (χ2) analyses were used to compare the 282 subjects who had one or more missing variables with the 5,832 cases included in the final sample. The deleted subjects were more likely to be never married, χ2(3, N = 6,114) = 13.20, p = .004, less likely to have died between 2001 and 2003, χ2(1, N = 6,114) = 12.36, p < .001, and more likely to have died between 2010 and 2012, χ2(1, N = 6,114) = 34.52, p < .001. There were no other statistically significant differences between those who were deleted due to missing data and the remaining sample.
Trends in Advance Directive Disparities
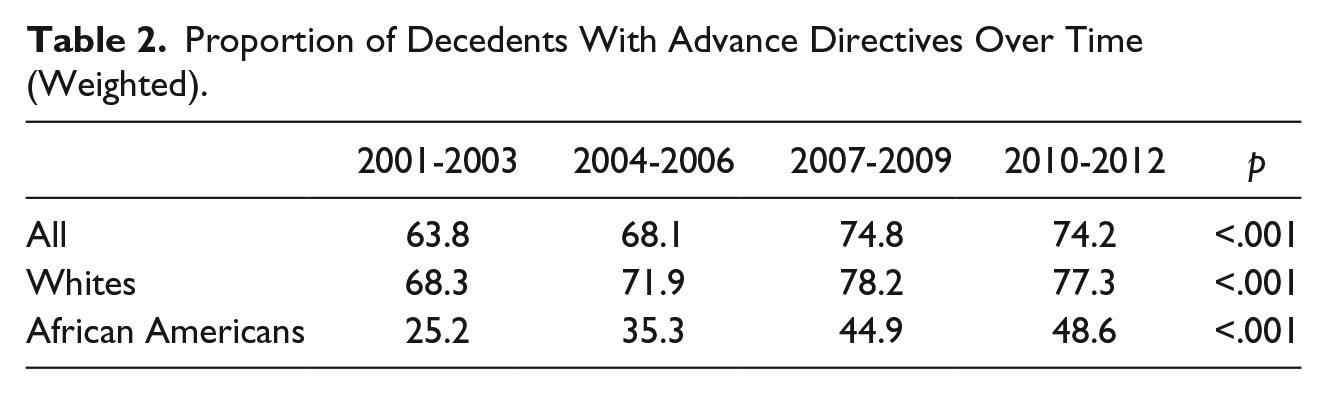
Rates of advance directive completion significantly increased among both White and African American decedents (Figure 1). For Whites, the percentage who had completed advance directives rose from 68.3% in 2001-2003 to a high of 78.2% in 2007-2009 before leveling off in 2010-2012 (77.3%). For African Americans, the percentages almost doubled from 25.2% in 2001-2003 to a high of 48.6% in 2010-2012 (Table 2).
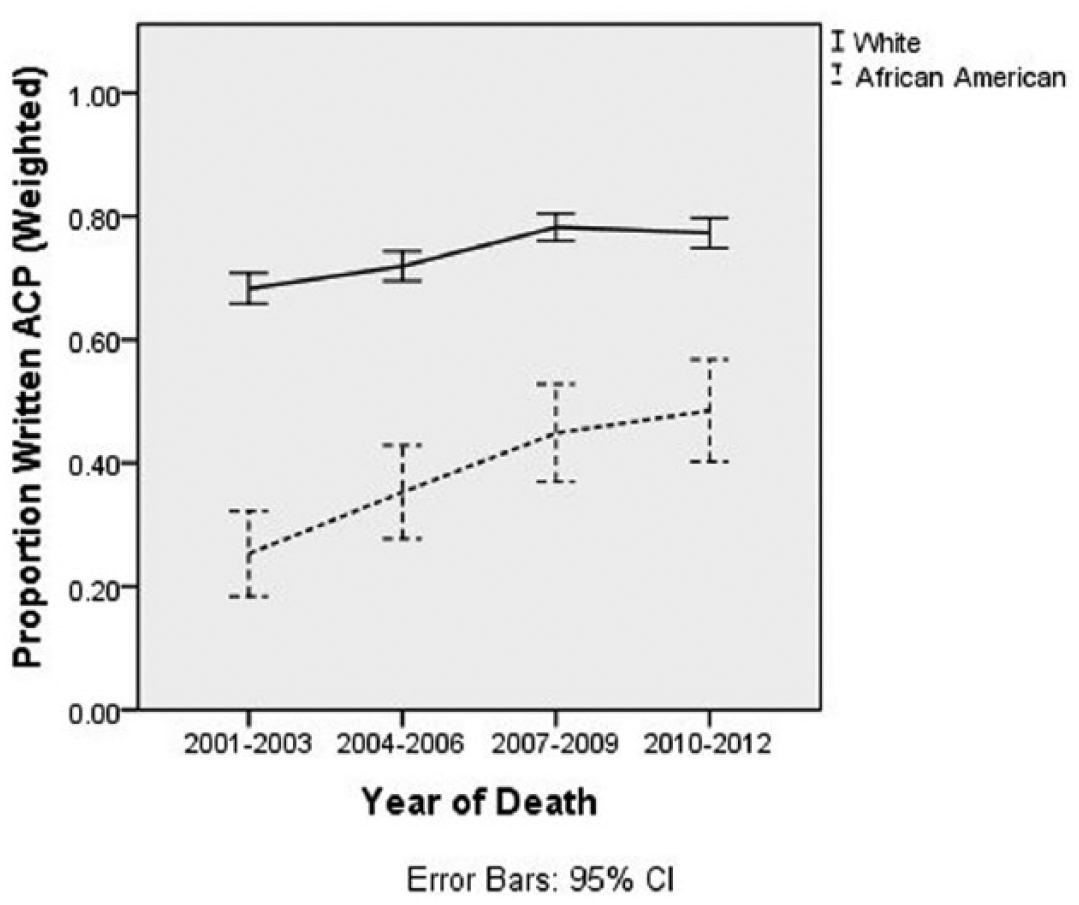
Weighted proportions of decedents aged 65 to 99 with advance directives by year of death (2001-2012).
Proportion of Decedents With Advance Directives Over Time (Weighted).
Model 1 shows the overall odds of having an advance directive compared with 2001-2003 rose in 2004-2006, odds ratio (OR) = 1.19, p = .04, 95% confidence interval (CI) = [1.01, 1.40], continued to increase in 2007-2009, OR = 1.67, p < .001. 95% CI = [1.40, 1.98], but then leveled off in 2010-2012, OR = 1.58, p < .001, 95% CI = [1.32, 1.89]. The odds of having an advance directive for African Americans between 2001 and 2012 were 16% of the odds for Whites, p < .001, 95% CI = [0.11, 0.23]. There were no significant interactions between race and year of death before 2010. During 2010-2012, the increase in the odds for African Americans was greater than for Whites, as indicated by the significant interaction term, OR = 1.76, p = .03, 95% CI = [1.05, 2.95] (Table 3).
Logistic Regression Models Predicting the Odds of Advance Directive Completion (N = 5,832).

The addition of the control variables in Model 2 strengthened the interaction effects. There were still no significant interactions until the 2010-2012 period, although the interaction approached significance in 2007-2009, OR = 1.65, p = .07, 95% CI = [0.97, 2.81]. As in Model 1, the significant interaction term indicated the rate of increase in the odds of having an advance directive was steeper for African Americans than for Whites during the 2010-2012 period, OR = 1.95, p = .02, 95% CI = [1.14, 3.35]. The odds of having an advance directive in 2010-2012 increased almost twice as much over 2001-2003 odds for African Americans compared with Whites.
All control variables except sex were statistically significant. The addition of covariates increased the Nagelkerke pseudo-R2 from .09 to .19. However, classification for both models was rather poor (72.6% and 73.8%). Almost all errors resulted from overinclusion, misclassifying those who did not have advance directives.
Discussion
There is a compendium of extant data highlighting the benefits of ACP. Despite the potential advantages, there are significant racial disparities in ACP. Social determinants of health (SDoH), defined by five key domains (economic stability, education, health and health care, neighborhood and built environment, social and community context), provide an explanation for differences that may exist within and between groups on a myriad of social, mental, and physical health issues (Centers for Disease Control [CDC], 2015; Solar & Irwin, 2010). The World Health Organization (WHO) further cites social determinants as being multifaceted, integrated, and overlapping social structures and economic systems that include upstream and downstream factors that may impact decision making on a number of critical health, social, and policy issues (Solar & Irwin, 2010).
In an attempt to define the underlying mechanisms of health disparities, the theory of fundamental causes (Phelan, Link, & Tehranifar, 2010) suggests that as the overall rates of a beneficial health behavior such as written ACP increase, disparities are likely to persist or even grow as a result of differential access to enabling resources. Individuals at a financial, physical, temporal, informational, psychological, or social advantage are better positioned to profit from innovations that improve health and health outcomes. Particularly when health interventions require knowledge, funds, time, or personal initiative, successful efforts to improve public health overall may exacerbate disparities by disproportionately benefiting those who can most easily obtain and act on new information or opportunities (Mechanic, 2002).
However, when underlying barriers are addressed to make health innovations more easily accessed, disparities may decrease. For example, Medicare has helped to reduce, but not eliminate, health disparities among older adults by making almost all individuals eligible for insurance coverage once they reach age 65. From the start, Medicare made a significant impact by requiring hospitals to desegregate as a condition of receiving reimbursement (Eichner & Vladeck, 2005). In the context of near-universal Medicare coverage among older adults, the federal requirement that all Medicare-funded health care institutions provide information about advance directives could potentially equalize access to information, advice, or other resources that enable patients to engage in ACP.
Using weighted HRS exit survey data for individuals who died between 2001 and 2012, this study examined trends in advance directive completion among White and African American decedents aged 65 to 99 in the United States. Nearly 70% of the total sample were reported to have engaged in written ACP in the form of a living will and/or durable power of attorney for health care prior to death. This is slightly higher than the 63% rate found by Silveira et al. (2014) who analyzed HRS data for decedents of all races and ethnicities 60 and older who died between 2000 and 2010. Consistent with prior research, there were substantial race disparities, with 74% of White decedents reported to have an advance directive compared with 38% of African Americans.
Between 2001 and 2012, advance directive rates rose for both White and African American decedents. Disparities between Whites and African Americans remained large but gradually narrowed. A significant interaction between race and time period during 2010-2012 indicated that the increase in the odds of having an advance directive was greater for African Americans than for Whites. The inclusion of covariates in the model strengthened the interaction effect. All control variables except sex were significant. Age, education, widowhood, living in a long-term care facility, and expected death were positively associated with advance directive completion before death. Regional differences were also observed, with higher odds of written ACP for those living in the Midwest and West compared with the South and Northeast.
Contrary to what would be predicted based on the theory of fundamental causes, overall improvements in advance directive completion rates did not lead to widening racial disparities. Public education and outreach promoting written ACP do not appear to be disproportionately benefiting Whites. Given the fact that much of these efforts are conducted by health providers, near-universal Medicare coverage for older adults may be an equalizing influence.
Although not the focus of this study, it is interesting to note regional differences in addition to racial disparities, with those residing in the Midwest and West being more likely to have an advance directive in place compared with those in the South and Northeast. In addition to regional cultural and economic characteristics, variations in state laws and regulatory schemes may partially account for different rates of advance directive completion. These results highlight the need to further consider geographic factors on SDoH among diverse populations.
Looking to the future, several recent developments may influence overall rates of ACP as well as ACP disparities. In October of 2015, the Centers for Medicare and Medicaid Services (CMS) approved new reimbursement codes permitting physicians and other qualified health care providers to bill Medicare for time spent with patients to discuss and/or complete advance directives (Sabatino, 2015). Another area to consider is the potential influence that formal and/or informal caregiving has on ACP in general, and among African Americans in particular. Questions remain as to the role that family members, clergy, and other informal support systems have in decision-making processes.
Another trend that may help reduce disparities is increasing rates of Internet usage among older adults as well as among African Americans of all ages (Pew Research Center, 2015). There is a growing body of literature citing the use of technology and information gathering among African Americans and other minority populations (McCleary-Jones et al., 2013), where the Internet may be used as a source of knowledge transfer. When health technologies and information are widely and easily available, socially determined differences in knowledge, proactivity, or other resources play a relatively minor role in perpetuating disparities (Williams & Jackson, 2005). This may contribute to a positive trajectory in the number of African Americans actively seeking information about ACP, which may lead to higher rates of advance directive completion.
Although this study, by looking at changes in advance directive completion over time, showed novel findings in ACP trends among White and African American older adults, there are a few limitations that must be acknowledged. First, data regarding advance directive completion was based on proxy reports, sometimes collected more than a year after a person had passed away. These proxies may not be aware of or may inaccurately recall decedents’ advance directive status. Second, the relatively modest R2 and misclassification rate indicate that important influences on advance directive completion are unaccounted for in the model. Finally, disparities among other race or ethnic groups are unaddressed in the present study. There are similarly a number of strengths that should likewise be recognized. Data from this study were taken from a large, nationally representative sample that reflects population prevalence and trends. The main findings were consistent even after controlling for several significant covariates, some of which also provided results worthy of further exploration.
Despite some indications that disparities in advance directive completion have begun to narrow, findings from this study are consistent with current literature recognizing significant and persistent race differences in ACP. The comparatively low rate of advance directive completion by older African Americans is cause for concern given the likely relationship between ACP and medical treatment affecting quality of life prior to death. Initiatives encouraging more African Americans to engage in ACP were the subject of a recent New York Times article highlighting racial differences in rates of hospice use and palliative care at the end of life (Varney, 2015). More attention is needed to identify what social determinants function as facilitators and/or barriers to ACP, particularly among diverse race and marginalized populations. Pervasive and ongoing differences in patterns of access to resources between minority and majority groups may be mechanisms by which certain race and economic groups are privy to the benefits of ACP. For example, Carr (2012b) found that home ownership and net worth were positively associated with ACP, suggesting a potential link between estate planning and end-of-life planning that could be contributing to ACP disparities. Although the present study provided novel data on trends in ACP among older White and African American adults, further research is needed to identify the factors that influence the likelihood of older African Americans (or other minority groups) engaging in open discussions about end-of-life preferences and/or completing advance directives as well as how these factors may be evolving.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.