
Abstract
Introduction
Back pain is the most frequent type of pain and among the most common complaints leading to a clinic visit (Deyo, Mirza, & Martin, 2006). We previously reported that back pain severe enough to restrict activities, hereafter referred to as restricting back pain, is common in older adults, with more than 77% reporting an episode over 10+ years; episodes were often short-lived, lasting an average of 1 month (Makris, Fraenkel, Han, Leo-Summers, & Gill, 2011), and typically recurrent (Thielke et al., 2012). Based on 2005 dollars, the United States spends more than US$100 billion for direct and indirect costs related to back pain (Katz, 2006), and these costs are expected to rise as the prevalence of back pain increases (Freburger et al., 2009). Over the last decade, both diagnostic and therapeutic costs for back pain have escalated, but outcomes have not improved (Martin et al., 2008; Weiner, 2015).
While back pain is highly prevalent and costly, longitudinal data evaluating its functional consequences in older adults are limited. Understanding the various ways that back pain affects older adults is important as it can help guide appropriate outcome assessments as well as management approaches (Deyo et al., 2014; Makris et al., 2016; Weiner, 2015). In 2014, experts and leaders in the field of chronic back pain published the “Report of the NIH Task Force on Research Standards for Low Back Pain” (Deyo et al., 2014). This report emphasized the importance of evaluating physical function as it relates to back pain (Deyo et al., 2014).
Activities of daily living (ADL), both essential and instrumental, are fundamental to maintaining independence in older adults. Disability is commonly assessed in the literature by inability to perform ADL. It has been reported that 9% of the U.S. population over 65 years of age has one or more disabilities in ADL (Cigolle, Langa, Kabeto, Tian, & Blaum, 2007). Those who lose the ability to perform ADL are more likely to become institutionalized, have higher rates of morbidity and mortality, and experience poorer quality of life (Andrews, Cenzer, Yelin, & Covinsky, 2013; Docking et al., 2015; Fried & Guralnik, 1997). Several cross-sectional studies have demonstrated a strong relationship between pain, functional limitations, and disability in ADL (Covinsky, Lindquist, Dunlop, & Yelin, 2009; Leveille et al., 1999; Reid, Guo, Towle, Kerns, & Concato, 2002). Given the dynamic nature of pain and disability, longitudinal data are needed that will appropriately capture changes in these clinical phenomena (Gill, Guo, & Allore, 2008).
Few longitudinal studies have evaluated back pain and subsequent ADL disability in both older men and women. We have shown a significant association between restricting back pain and subsequent mobility disability in community-living older adults using longitudinal data (Makris, Fraenkel, Han, Leo-Summers, & Gill, 2014). To gain a more comprehensive understanding of the deleterious effects of restricting back pain in older adults, we sought to evaluate the associations between restricting back pain and both essential (e) and instrumental (i) ADL disability. We used data from a unique longitudinal study that includes monthly assessments of both restricting back pain and disability for more than 13 years in a large cohort of older community-living men and women. A better understanding of the impact of restricting back pain on eADL and iADL disability would provide additional evidence to support the need and targets for interventions to improve clinical outcomes in this population.
Method
Study Population
Participants were drawn from the Precipitating Events Project (PEP), a longitudinal study of 754 community-living adults, aged 70 and older, who were initially nondisabled in their eADL: bathing, dressing, walking inside the house, and transferring from a chair (Gill, Desai, Gahbauer, Holford, & Williams, 2001). Exclusion criteria were inability to speak English, significant cognitive impairment with no available proxy (Gill et al., 2008), life expectancy less than 12 months, and plans to move out of the area. Based on initial sample size calculations, physically frail adults were oversampled in PEP. Of 2,753 potential participants, only 4.6% of persons refused screening, and 75.2% of those eligible agreed to participate and were enrolled from March 1998 to October 1999. Those who refused to participate did not differ significantly from those who were enrolled in terms of age or sex (Gill et al., 2001). The study protocol was approved by the Yale Human Investigation Committee.
Data Collection
Comprehensive home-based assessments were completed at baseline and every 18 months for up to 144 months, while telephone interviews were completed monthly through June 2011, with a completion rate of 99%. For participants with significant cognitive impairment or who were not available, a proxy was interviewed using a standardized protocol (Gill et al., 2008). Deaths were ascertained from the local obituaries and/or an informant during a subsequent interview. Four hundred ninety-three (65%) participants died after a median follow-up of 82 months, and 38 (5.0%) dropped out of the study after a median follow-up of 26 months. Data were otherwise available for 98.4% of the 4,175 comprehensive assessments and 98.5% of the 75,340 monthly interviews.
Restricting Back Pain
Back pain leading to restricted activity (restricting back pain), the independent variable, was assessed during monthly interviews with the following series of questions. Each month, participants were asked, “Since we last talked [1 month ago], have you stayed in bed at least half the day due to an illness, injury, or other problem?” and, “Have you cut down on your usual activities due to an illness, injury, or other problem?” Participants who answered yes to either question were considered to have restricted activity and were subsequently asked whether their restricted activity was due to back pain. Test–retest reliability for restricting back pain was high, with kappa = 0.84 (Reid, Williams, Concato, Tinetti, & Gill, 2003). The referent group included participants who did not have restricted activity, regardless of whether they had back pain, as this was not assessed in the absence of restricted activity.
Disability in ADL
Disability, the dependent variable, was defined for eADL as dependence in bathing, dressing, walking inside the house, and transferring from a chair; and for iADL as dependence in doing housework, preparing meals, and shopping. Each month, participants were asked, “At the present time, do you need help from another person to [complete the task]?” for each of the eADL and iADL. Participants who reported “Yes” or “Unable to complete the task” were considered to have disability. For both eADL and iADL, an episode of disability was defined as disability in any of the relevant tasks that had to be preceded by a month with no disability. Among a subgroup of participants interviewed twice within a 2-day period by different interviewers (n = 91), the test–retest reliability was substantial for eADL with a kappa of 0.75 and moderate for iADL disability with a kappa of 0.46 (Gill et al., 2008; Kramer, 1981).
Covariates
Data were collected on several covariates during the comprehensive assessments and dichotomized to assist in clinical interpretation (Gill, Murphy, Barry, & Allore, 2009). Covariates were selected based on known associations with adverse functional outcomes (Gill et al., 2001; Gill, Hardy, & Williams, 2002; Gill et al., 2009; Makris et al., 2014). Demographic characteristics included age, sex, race/ethnicity, living situation, and education. Cognitive status was assessed by the Folstein Mini-Mental State Examination (MMSE; Folstein, Folstein, & McHugh, 1975). Depressive symptoms were assessed by the Center for Epidemiologic Studies Depression (CES-D) Scale (Kohout, Berkman, Evans, & Cornoni-Huntley, 1993). Nine self-reported, physician-diagnosed chronic conditions were assessed: arthritis, hypertension, diabetes mellitus, myocardial infarction, chronic lung disease, cancer, stroke, congestive heart failure, and hip fracture. Body mass index (BMI) was calculated using participants’ self-reported height and weight, according to the World Health Organization definition. Physical frailty was defined by slow gait speed, as previously described (Gill et al., 2008). Lower extremity (hip) weakness, an independent risk factor for restricting back pain, was assessed with a hand-held Chatillon MSE 100 dynamometer (AMATEK Measurement and Calibration, Largo, Florida; Makris et al., 2014). The cut points demarcated the worst sex-specific quartile for the nondominant limb, on the basis of the first 356 enrolled participants randomly selected from the source population (Gill et al., 2009). Table 1 provides additional operational details of the covariates.
Baseline Characteristics of Study Participants in Two Analytic Samples.

Note. eADL = essential activities of daily living; iADL = instrumental activities of daily living; MMSE = Mini-Mental State Examination; CES-D = Center for Epidemiologic Studies Depression Scale; BMI = body mass index.
Cut-point was defined on the basis of the frequency distributions in the analytic sample.
Statistical Analysis
Of the 754 participants, all were included in the eADL analysis as all participants were free of eADL disability at baseline. For the iADL analysis, 51 (6.7%) participants reported iADL disability at baseline and throughout the follow-up period and were never at risk for developing a new episode of iADL disability. Therefore, the primary analytic sample for the iADL analysis included the remaining 703 participants, who were at risk for developing iADL disability over the follow-up period.
The baseline characteristics were summarized using means and standard deviations for continuous variables, and frequencies and proportions for categorical variables. The amount of missing data for the covariates ranged from 0 for physical frailty to 3.5% for depressive symptoms, with the exception of hip weakness, for which 10% of the observations were missing. This small amount of missing data was accounted for using multiple imputation with 50 random draws per missing observation. The incidence of disability in eADL and iADL was estimated using a generalized estimation equation binomial model. The 95% confidence intervals (CI) were based on empirical standard errors that accounted for the correlation of recurrent events in the same participants.
A multivariate Cox model for recurrent events was used to evaluate the association between restricting back pain and incidence of subsequent eADL and iADL disability. Temporal precedence, as depicted in Figure 1, was established, using monthly interviews, by assessing ADL disability “at the present time,” while assessing restricting back pain over the preceding month, “Since we last talked [one month ago] . . .” In this model, participants were at risk for developing recurrent episodes of eADL and iADL disability over the 13+ years of follow-up. All covariates, other than sex and race, were updated every 18 months, and entered into the models as time-dependent variables. The crude and adjusted hazard ratios (HRs; and 95% CIs) for developing eADL and iADL disability were estimated for restricting back pain, with robust sandwich variance estimators to account for the correlation within individuals (Therneau & Grambsch, 2000; Wei, Lin, & Weissfeld, 1989).
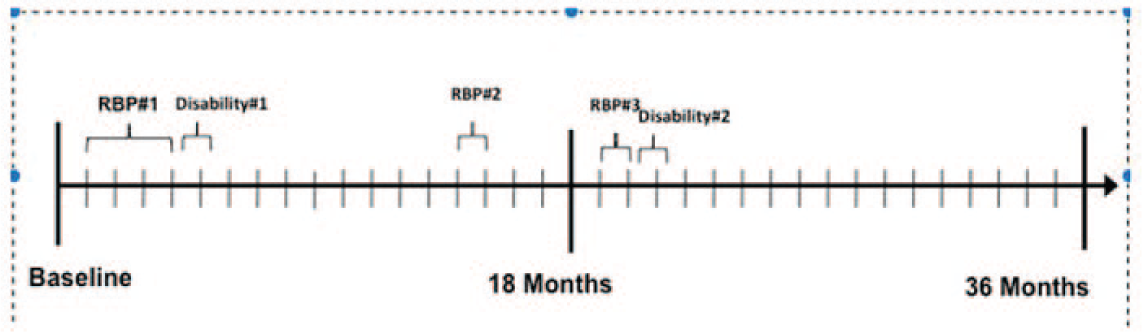
Assessing association between restricting back pain (RBP) and subsequent disability over time.
As prior research shows that women report back pain more frequently than men (Makris et al., 2011), we tested for potential statistical interaction between restricting back pain and sex. We also conducted two sets of secondary analyses. First, based on prior work demonstrating that episodes of disability are often short-lasting (i.e., 1 month or less), we evaluated the association between restricting back pain and eADL and iADL disability that persisted for at least 2 months (persistent disability) (Gill et al., 2008). Second, to further strengthen a temporal and potentially causal association, we repeated the primary iADL analysis after excluding participants who had iADL disability at baseline (n = 532); all participants were nondisabled in eADL at baseline, as described above.
All statistical tests were two-tailed, and p < .05 was considered to indicate statistical significance. All analyses were performed using SAS version 9.1 (SAS Institute, Inc., Cary, NC).
Results
As shown in Table 1, the baseline characteristics of participants in the two analytic samples were comparable. On average, participants were nearly 80 years old; the majority were female, White, and had completed high school. A minority of participants were cognitively impaired or reported depressive symptoms. The majority of participants were overweight. More than half of the participants reported two or more chronic conditions, with the most common being hypertension, arthritis, coronary artery disease, or diabetes.
Over a median follow-up of 111 months, the rate (95% CI) of eADL and iADL disability was 3.6 [3.4, 3.9] and 8.5 [8.1, 9.0] per 100 person months, respectively. Of the 2,269 episodes of eADL disability and 6,103 episodes of iADL disability, the median duration was 2 months for each (interquartile range [IQR], 1-4 and 1-5, respectively). The frequency of disability in each of the eADL and iADL tasks is provided in Table 2.
Frequency of Disability in eADL and iADL.
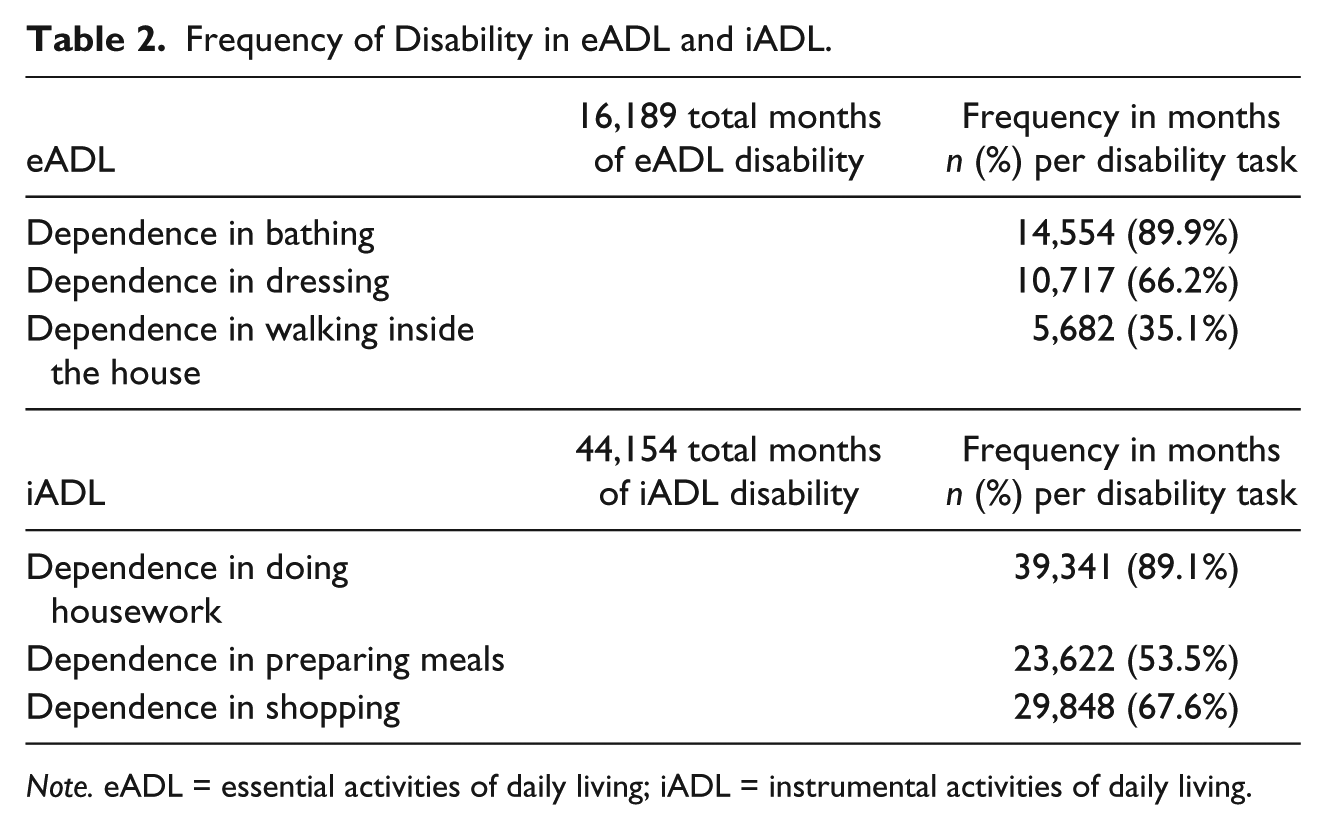
Note. eADL = essential activities of daily living; iADL = instrumental activities of daily living.
Table 3 provides HRs for the association between restricting back pain and eADL and iADL disability in the primary and secondary analyses. In the primary analysis, there was a strong independent association between restricting back pain and eADL and iADL disability, with adjusted HR (95% CI) = 3.47 [3.01, 3.90] and 2.33 [2.08, 2.61], respectively. There was no significant interaction between restricting back pain and sex for either outcome (p = .57 for eADL and .24 for iADL). In the secondary analysis, the results were comparable for persistent disability. When participants with baseline iADL disability were excluded (analytic sample, n = 532), there was also a strong independent association between restricting back pain and iADL disability, with adjusted HR (95% CI) = 2.56 [2.26, 2.91].
Associations of Restricting Back Pain and Subsequent Disability.
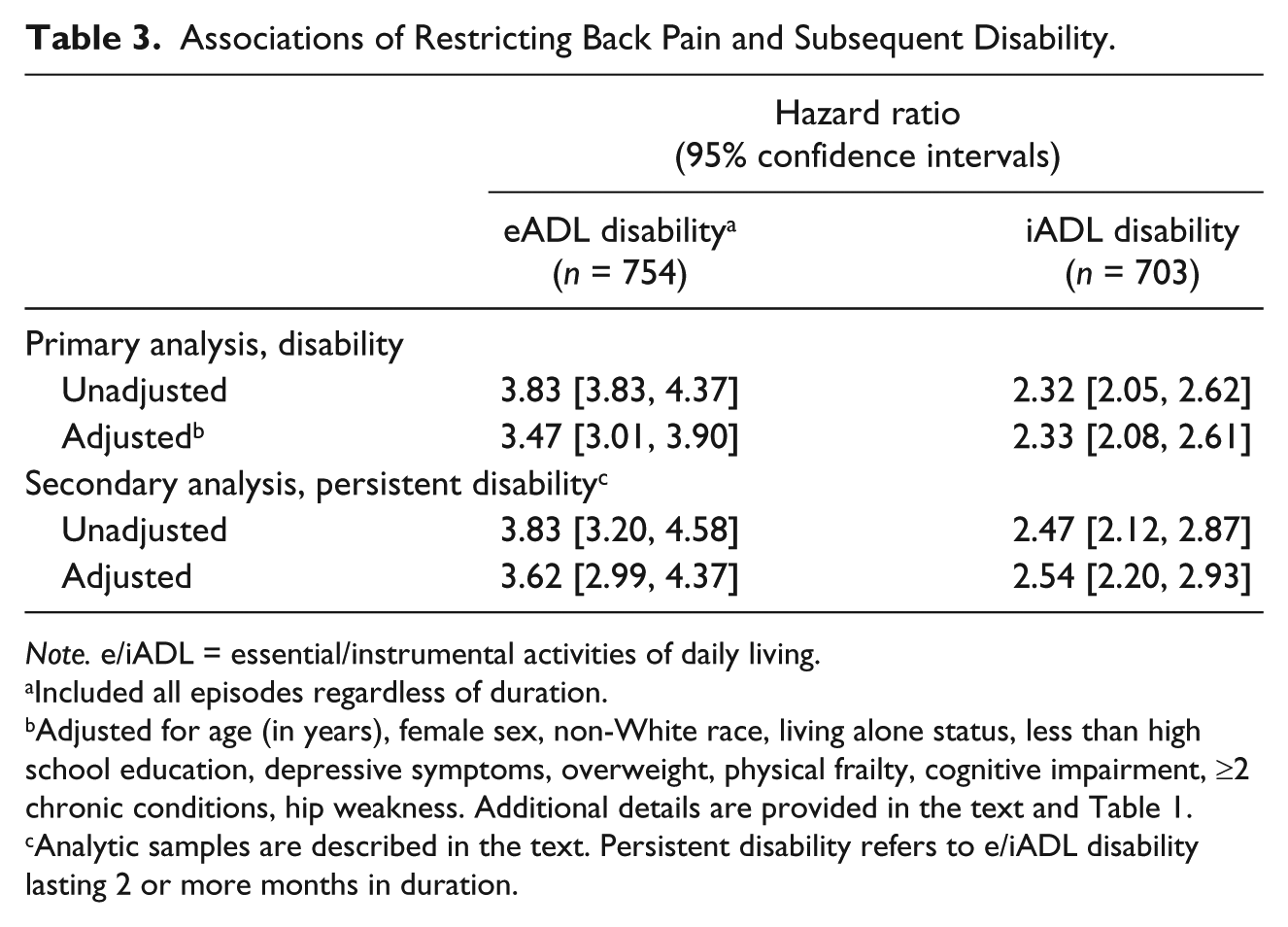
Note. e/iADL = essential/instrumental activities of daily living.
Included all episodes regardless of duration.
Adjusted for age (in years), female sex, non-White race, living alone status, less than high school education, depressive symptoms, overweight, physical frailty, cognitive impairment, ≥2 chronic conditions, hip weakness. Additional details are provided in the text and Table 1.
Analytic samples are described in the text. Persistent disability refers to e/iADL disability lasting 2 or more months in duration.
Discussion
We found that restricting back pain, commonly reported in older adults (Makris et al., 2011), is independently associated with subsequent (within 1 month) disability in both eADL and iADL. These relationships did not differ between men and women. It has become increasingly important to understand back pain in the context of physical function, and our study contributes to this literature.
While disability in eADL and iADL is associated with increased morbidity (Gill et al., 2008; Leveille et al., 1999), the relationship with restricting back pain is uncertain. In a prior study that used data from the Women’s Health and Aging Study, older women with severe back pain had a higher likelihood of having difficulty with eADL (Leveille et al., 1999). However, because this study was cross-sectional and focused on women who were disabled, the directionality of the pain–disability relationship could not be established. Recent longitudinal data found that older individuals with chronic noncancer pain, including spine pain, were not at higher risk of subsequent ADL disability; however, this study was limited by the biannual frequency of assessments and limited characterization of pain (Andrews, Cenzer, Yelin, & Covinsky, 2013). Prior studies that did not show a significant association between (back) pain and subsequent disability were not designed to satisfactorily establish a temporal relationship (Andrews, Cenzer, Yelin, & Covinsky, 2013; Leveille et al., 1999). Our study, evaluating both men and women, showed a strong association between restricting back pain and subsequent disability in eADL and iADL. These results complement our previous work that showed a strong relationship between restricting back pain and mobility disability as well as our qualitative findings highlighting not only the physical but also the psychological and social impacts of restricting back pain (Makris et al., 2014; Makris et al., 2016). We now have a more thorough understanding of the various ways restricting back pain affects older adults, and therefore can attempt to target these areas of importance for older adults.
Our study has several strengths. PEP data include monthly assessments of restricting back pain and disability in both eADL and iADL with more than 13+ years of follow-up. There was a very low rate of attrition for reasons other than death. In contrast to other observational studies that assessed exposure and outcome at limited/infrequent intervals, our study, with monthly assessments, increases the likelihood of a temporal relationship. To help show temporal precedence, during monthly interviews, restricting back pain was ascertained over the preceding month, whereas eADL and iADL disability were assessed “at the present time,” creating a time lag between exposure and outcomes. While monthly data are more granular than available in many observational studies, the data do not specify which days during the preceding month the restricting back pain resulted in eADL or iADL disability.
Our study also has several limitations. The severity, etiology, and the treatments used for restricting back pain were not evaluated. Self-reported restricted activities due to back pain may be secondary to other factors including a number of psychosocial factors, such as fear avoidance (Camacho-Soto, Sowa, Perera, & Weiner, 2012). While the focus of the current study was on restricting back pain, participants could have provided reasons other than back pain for their restricted activity (Gill et al., 2001). Although test reliability was substantial for eADL, it was only moderate for iADL disability. Measurement error, however, should have reduced the associations between restricting back pain and these disability outcomes. The generalizability of our results may be limited because participants were members of a single health care plan in the greater New Haven region. The demographics of our cohort, however, mirror those of the U.S. population except for race and ethnicity (American FactFinder, 2013). Finally, this was an observational study, and therefore, the associations reported cannot be interpreted as causal.
Conclusion
In conclusion, restricting back pain is strongly associated with subsequent disability in both eADL and iADL. This study provides further evidence for the functional impact of restricting back pain. In the evaluation and treatment of back pain, the impact on function of these everyday activities should be strongly considered.
Footnotes
Acknowledgements
We thank Heather G. Allore, PhD, director of the Biostatistics Core at the Yale Program on Aging, for her statistical expertise and guidance. We also thank Denise Shepard, BSN, MBA; Andrea Benjamin, BSN; Barbara Foster; and Amy Shelton, MPH, for assistance with data collection; Wanda Carr and Geraldine Hawthorne, BS, for assistance with data entry and management; Peter Charpentier, MPH, for design and development of the study database and participant tracking system; and Joanne McGloin, MDiv, MBA, for leadership and advice as the project director.
Author Contributions
Study concept and design: Makris, Fraenkel, Han, Leo-Summers, Gill; acquisition of data: Gill; analysis and interpretation of data: Makris, Weinreich, Fraenkel, Han, Leo-Summers, Gill; preparation of manuscript: Makris, Weinreich, Fraenkel, Han, Leo-Summers, Gill
Authors’ Note
Una E. Makris had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The views expressed in this article are those of the author(s) and do not necessarily represent the views of the Department of Veterans Affairs or UT Southwestern Medical Center and its affiliated academic and health care centers, the National Center for Advancing Translational Sciences, or the National Institutes of Health. The sponsor had no role in the design or conduct of the study; in the collection, management, analysis, or interpretation of the data; or in the preparation, review, or approval of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work for this report was funded by a grant from the National Institute on Aging (R01AG17560). The study was conducted at the Yale Claude D. Pepper Older Americans Independence Center (P30AG21342). Una E. Makris was supported by an NIA GEMSSTAR (R03AG040653), the Center for Translational Medicine, NIH/NCATS Grants (KL2TR001103 and UL1TR001105), and the Yale Training Program in Geriatric Clinical Epidemiology and Aging Related Research (T32AG19134). Dr. Makris is currently supported by a Career Development Award IK2HX001916 from the U.S. Department of Veterans Affairs Health Services Research and Development. Liana Fraenkel is supported by K24AR060231. Thomas M. Gill is currently supported by K07AG043587.