
Abstract
Introduction
The disablement process model describes a conceptual pathway showing the progression from underlying subclinical pathology to the onset of disability (Verbrugge & Jette, 1994). According to this model, pathology increases the risk for impairment, functional limitations, and subsequent disability. Disability describes difficulty or dependency in carrying out activities essential to independent living (Campbell & Buchner, 1997). Demographic factors and intra- and extraindividual factors may modify the disablement process by either accelerating or decelerating progression to disability (Schure & Goins, 2016). Intraindividual factors include person-level psychological attributes and health behaviors, while extraindividual factors describe environmental conditions and support systems. Similar to disability, frailty describes increased vulnerability to stressors due in part to decreased physiological reserves (Fried et al., 2001). Both frailty and disability are suboptimal functional states common in aged populations (Lowry, Vallejo, & Studenski, 2012).
Recent estimates indicate that 15% of U.S. community-dwelling older adults are frail (Bandeen-Roche et al., 2015) and 25% have a disability (Hung, Ross, Boockvar, & Siu, 2011). Among African American and Hispanic/Latino elders, estimates of frailty prevalence are 65% to 85% higher than those for White elders (Bandeen-Roche et al., 2015). Prior work focused on racial disparities in functional health reports that differences in socioeconomic status play a key role. Low socioeconomic positioning is associated with limited access to preventative health care (Shenson et al., 2012; Wright & Perry, 2010) and increased exposure to maladaptive psychosocial and environmental stressors. Preventative care interventions focused on addressing the unmet health care needs of this segment of the population may mitigate further functional decline and globally reduce health care costs.
Decreased physical function, declining bone density (Lowry et al., 2012; Pluijm et al., 2006), and depressed mood (Richardson et al., 2012) are shared risk factors for disability and frailty. Poor physical function, a marker of functional limitations, is linked to adverse health outcomes including increased risk for falls and fractures (Ward et al., 2015), hospitalizations (Wolinsky et al., 2007), and mortality (Cesari et al., 2008). Impaired mobility, a common indicator of decreased physical function in older adults, is also associated with lower health-related quality of life (HRQL; Davis et al., 2015). Decreased bone density, an index of underlying pathophysiology, increases risk for physical impairments, functional limitations, and disability. Low bone mineral density (BMD) is also a surrogate index of osteoporosis, a key risk factor for fragility fractures (Dawson & Dennison, 2016). Use of Vitamin D and calcium supplements (Weaver et al., 2016) and behavioral health interventions, such as exercise (Courteix et al., 2015), have been shown to attenuate losses in bone density and improve physical function. Finally, depressed mood has been shown to co-occur in individuals with reduced functional difficulties (Dunne, Wrosch, & Miller, 2011; Gitlin, Winter, & Stanley, 2012) and is linked to Vitamin D activity. Neurobiology studies of depression show age-related decreases in 25-hydroxyvitamin D [25(OH)D] levels likely affect central nervous system Vitamin D activity (Eyles, Smith, Kinobe, Hewison, & McGrath, 2005) as Vitamin D receptors are densely located in limbic structures, the hippocampus, and the prefrontal cortex—key brain structures that govern mood (Langub, Herman, Malluche, & Koszewski, 2001; Okereke & Singh, 2016).
Early identification of key risk factors for frailty and disability may provide an opportunity to modify risk factors and provide services to help older adults maintain their independence. Intervention studies aimed at preventing functional decline in aged populations have generally focused on a single risk factor (Bauer et al., 2015; Cesari et al., 2015; Lyons & Hall, 2016). Existing multidimensional interventions have centered primarily on physical activity regimens and have shown promise in reducing risk factors for disability and frailty in high-risk community-dwelling older adults (Fairhall et al., 2014). We extend this work by implementing a tailored, multidimensional health intervention targeting pathology (low bone density), functional limitations (physical function), and psychological attributes (depressed mood) associated with disability and frailty in community-dwelling older adults. Our approach is based on previous studies demonstrating the utility of multidimensional interventions in addressing risk factors for frailty and disability in community settings (Gates, Fisher, Cooke, Carter, & Lamb, 2008; Gitlin et al., 2012; Guo, Tsai, Liao, Tu, & Huang, 2014). Our use of a transdisciplinary team of health professionals and students to implement our program is based on research demonstrating the effectiveness of teams in reducing frailty and disability in clinical practice (Dulin et al., 2012) and research settings (Fairhall et al., 2014). Thus, we describe a program that leverages interprofessional expertise in geriatric health and multiple evidence-based strategies to deliver a multidimensional, community-based intervention program targeting risk factors for frailty and disability in a diverse sample of older adults at risk for poor functional health. As previous studies have described racial disparities in functional health outcomes, we also examine whether African American and White elders differed in response to the interventions.
Method
Program Description
The Collaborative Assessements to Revitalize Elderly (CARE) program was a by-product of a partnership among the Division of Geriatrics at Washington University in St. Louis, the George Warren Brown School of Social Work, the Barnes-Jewish College Goldfarb School of Nursing, the St. Louis School of Medicine, and the St. Louis College of Pharmacy. The CARE program served 1,593 older adults, and 337 of them participated in the 6-month intervention program. Of the 337 participants, 98.7% of them completed the postintervention and 74.5% of them completed the 12-month assessment. The program was implemented in senior living facilities and community centers in St. Louis, Missouri. The Washington University Institutional Review Board reviewed and approved the implementation of this program.
Participants and Transdisciplinary Care Team
Participants were recruited from senior apartments and community centers. Inclusion criteria for this program specified that participants be aged 55 years and older, community-dwelling, able to give informed consent, fluent in English, and able to complete all assessments. Participants were identified as high-risk if they had more than one frailty risk factor (osteoporosis, impaired mobility, and/or low mood) identified during the preintervention assessment. Prospective participants were excluded if (a) unable to ambulate alone or with assistive device, (b) current substance abuse or alcohol abuse, and (c) major depressive disorder current or within the last 6 months.
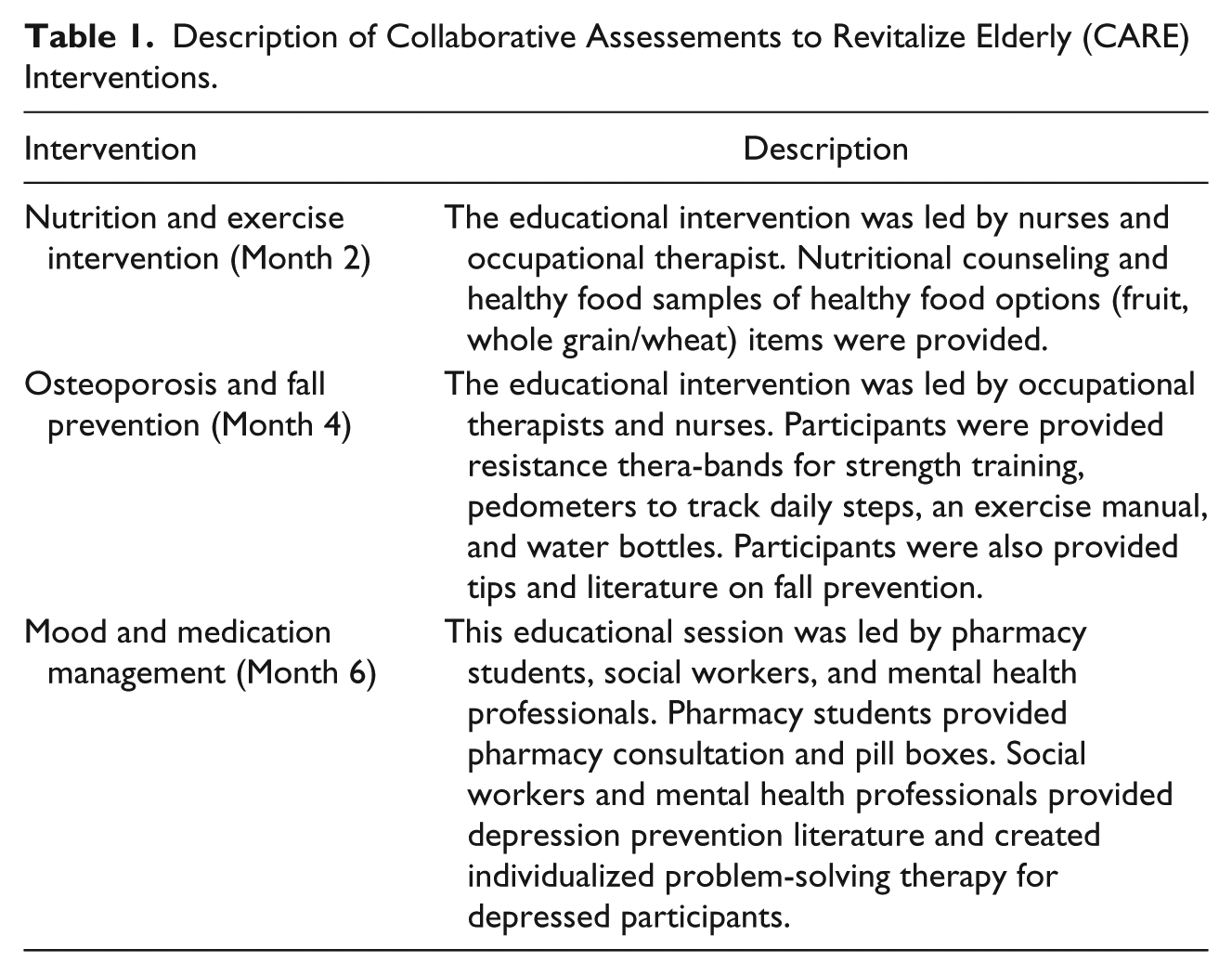
The transdisciplinary team included physicians, nurses, pharmacists, social workers, occupational therapists, and students from the participating colleges and universities. Social workers and mental health professionals provided expertise in depression and facilitated the intervention on mood. Physicians and nurses provided expertise in bone density, frailty, and nutrition. Physicians created and reviewed personalized CARE plans, completed osteoporosis assessments, and dispensed Vitamin D and calcium supplementation based on bone density screening results. Nurses participated in pre- and postintervention assessments and completed fall and fracture risk assessments. Pharmacy students provided medication safety review and facilitated the educational intervention on medication management. Occupational therapists provided expertise in physical function and facilitated the intervention on fall prevention and exercise. A detailed description of the interventions is provided in Table 1.
Description of Collaborative Assessements to Revitalize Elderly (CARE) Interventions.
Intervention
A 6-month community-based, multidimensional health intervention program was implemented to target risk factors for frailty and disability in community-dwelling older adults, at high risk for poor functional health. The conceptual framework of the disablement process model and the previously established efficacy of multidimensional interventions informed our selection of outcome measures and program design. Our multidimensional intervention included Vitamin D and calcium supplementation and sessions on medication management, exercise, nutrition, depression prevention and management, and fall prevention. Vitamin D and calcium supplementation and exercise have shown promise in fall prevention (Annweiler et al., 2010) and increasing bone density (Courteix et al., 2015; Weaver et al., 2016). To target depression, we used problem-solving therapy strategies as they have been shown to improve depression (Apostolo, Bobrowicz-Campos, Rodrigues, Castro, & Cardoso, 2016). Finally, medication management (LeBlanc & Choi, 2015) and nutritional counseling were employed (Hamirudin, Charlton, & Walton, 2016) to improve overall health in this population.
Using a computerized algorithm, an individualized and automated CARE plan was created based on the participant’s baseline scores on bone density test, physical performance test, and depression screening results. This plan was used to communicate recommended behavioral health interventions to the participant. Each participant met with a CARE health provider to review the care plan. During each intervention visit, CARE providers dispensed Vitamin D as Vitamin D3, and cholecalciferol and calcium supplements based on pDEXA results and body weight. Doses of Vitamin D3 ranged from 1,000 to 4,000 IU. Participants engaged in CARE sessions every 2 months for 6 months. The sessions covered nutrition and exercise (Month 2), osteoporosis and fall prevention (Month 4), and mood and medication management (Month 6). Reassessment of frailty and disability risk factors occurred at 6 months and 12 months.
For the nutrition and exercise session, participants engaged in an interactive program facilitated by occupational therapists. During this session, participants received dietary resources including literature on healthy foods, healthy recipes, and dietary recommendations. Participants used exercise resistance bands to learn how to implement an exercise program in their home. Participants also received resistance bands, water bottles, pedometers, and an exercise manual to facilitate independent exercise activity. Physicians and nurses facilitated the osteoporosis and fall prevention session. Facilitators provided education on fall prevention and bone health and distributed fall prevention resources (i.e., tips on environment modification to reduce fall risk, footwear, walking outdoors, how to improve mobility). Social workers, mental health professionals, and pharmacy students facilitated the mood and medication management session. Participants engaged in individualized problem-solving therapy and received depression prevention literature. Pharmacy students distributed pill boxes and provided education on medication management. Each behavioral health session lasted approximately 1 hr and took place in a community setting (senior residential site or community center).
Measures
Participant demographics and health survey
Participant demographic information was collected at baseline. Self-report of overall health status was measured using the Medical Outcomes Survey 36-item short form (Ware & Sherbourne, 1992).
Bone health
Bone density was measured using peripheral dual energy x-ray absorptiometry (pDEXA) of the forearm and wrist. Peripheral DEXA is a portable screening tool for osteoporosis and osteoporotic fracture risk. Key outcomes were bone mineral content and bone density T-scores of the proximal forearm (cortical bone) and the distal forearm (trabecular bone). Osteoporosis was defined using World Health Organization (WHO) criteria (WHO, 2003).
Physical function
The mini-Physical Performance Test (mini-PPT; Wilkins, Roe, & Morris, 2010) was used to measure balance, strength, and mobility. This validated measure includes four items: picking up a penny from the floor, a timed 50-foot walk, chair rises (5 times), and a progressive Romberg test. The first three items were assessed on a 5-point scale based on time to complete and the final item was coded one or zero. Table 2 describes the coding of the mini-PPT. Higher scores indicated better overall physical function, with a maximum score of 16.
Description of Mini-PPT and PHQ-9.
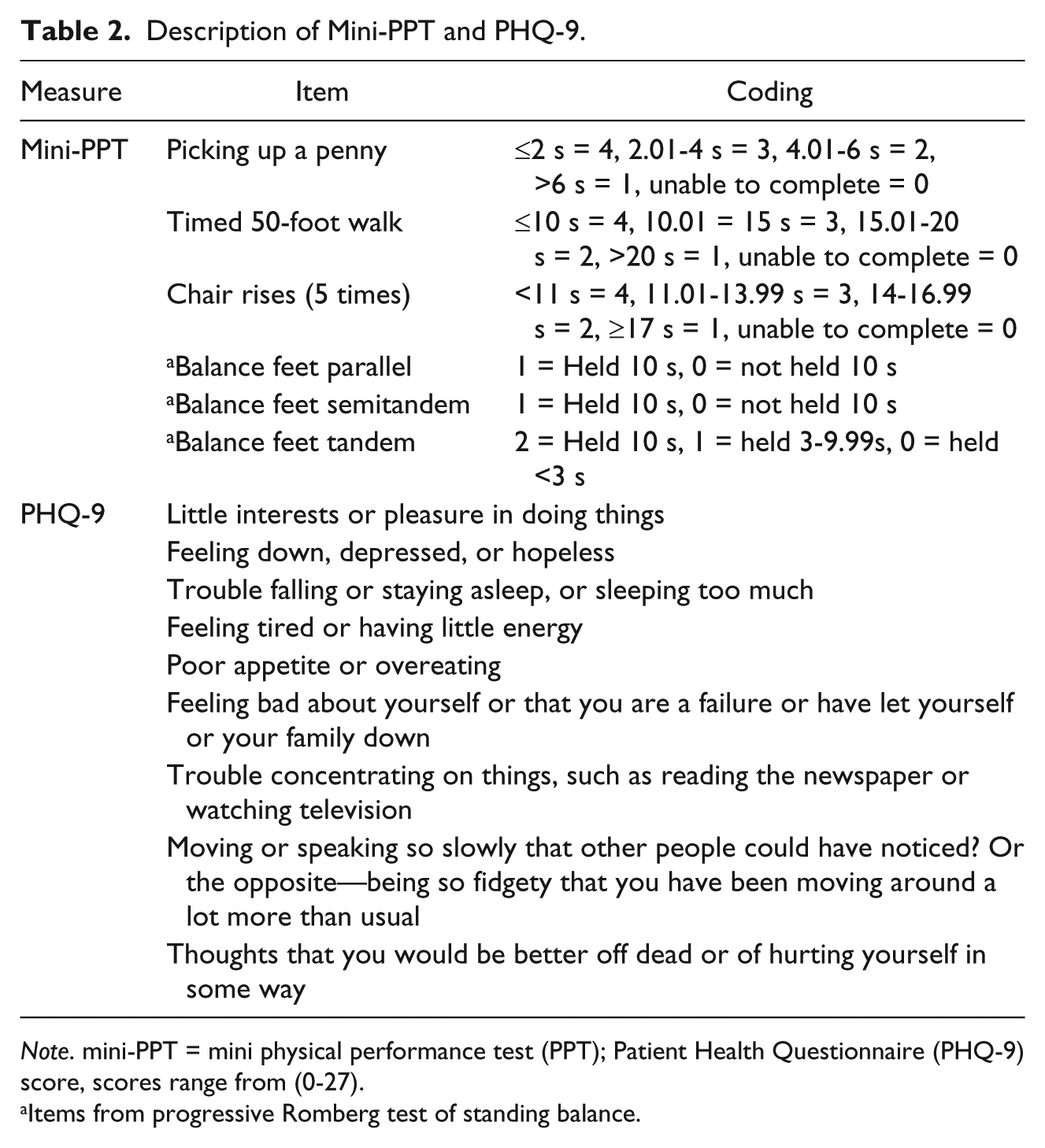
Note. mini-PPT = mini physical performance test (PPT); Patient Health Questionnaire (PHQ-9) score, scores range from (0-27).
Items from progressive Romberg test of standing balance.
Mood
The nine-item Patient Health Questionnaire (PHQ-9; Kroenke, Spitzer, & Williams, 2001) was used to determine severity of depression symptoms over the last 2 weeks; item scores ranged from zero (not at all) to 3 (nearly every day). Higher scores on the PHQ-9 indicated more severe depressive symptoms, with a maximum score of 27. Survey items are noted in Table 2.
Analytical Plan
Analyses were conducted using SPSS, version 23 (SPSS, Inc., Chicago, IL). Descriptive statistics were provided for sociodemographic and outcome variables. Performance on the PHQ-9 was log transformed, and performance on the PPT at 12 months was square root transformed to correct for positive skewness and kurtosis. A 2 × 2 mixed design analysis of covariance (ANCOVA) was completed to determine repeated measure effects (baseline, 12-months) and between-group effects (race: African American and White) for bone health. A 2 × 3 mixed design (ANCOVA) was used to determine between-group effects (race) and repeated-measure effects (baseline, 6-months, 12-months) for physical function and mood measures. Covariates were selected based on their influence on outcomes variables and typical inclusion in the relevant literature. Covariates included body mass index (BMI) and current smoking status (yes/no). Due to the small representation of other racial/ethnic minorities (n = 20), these participants were not included in analyses. Bonferroni post-hoc analyses were conducted if a significant main effect for time (baseline, 6 month, 12 months) was observed.
Results
The baseline demographic data was collected for 1,362 participants. Participants who completed the intervention study were significantly older than those who did not complete the intervention (p = .002). The completer group also had significantly lower male representation than the noncompleter group (p = .003). The completer group differed more significantly in racial makeup than the noncompleter group (p < .001). Participants who were lost to follow-up at the 12-month assessment had a higher BMI and were more likely to be African American (ps = .02). Descriptive statistics and baseline clinical characteristics for completers are provided in Table 3. The average age of the 337 community-dwelling adults was 76 years old, and 83% lived in HUD-subsidized housing. The sample was predominately African Americans (60%) and women (91%).
Demographic and Clinical Characteristics of Study Participants.
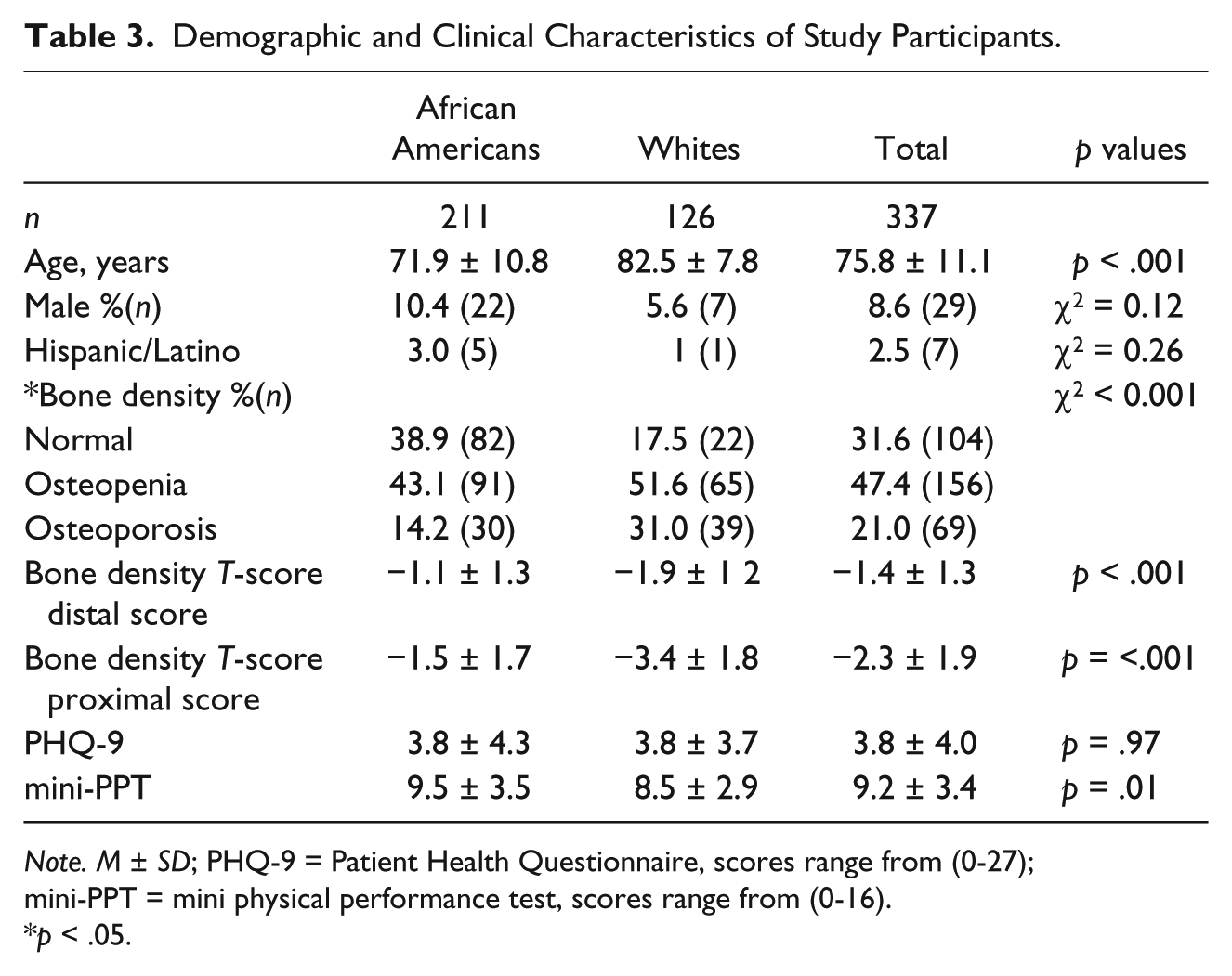
Note. M ± SD; PHQ-9 = Patient Health Questionnaire, scores range from (0-27); mini-PPT = mini physical performance test, scores range from (0-16).
p < .05.
Bone Density
After controlling for BMI and smoking status, there was no main effect for bone density distal (p = .71) or proximal (p = .51) scores. These findings indicate that bone density scores did not significantly differ from baseline and 12 months. African Americans had higher bone density scores than Whites (ps < .05). There was no significant interaction between race and rate of change in distal T-scores (p = .72) or race and proximal T-scores (p = .83), see Figure 1.

Bone density (distal T-scores) at baseline and 12-month postintervention by race.
Physical Function
There was a main effect for physical function, F(2, 172) = 3.02, p = .45, η2 = .06, thus indicating physical function differed over time. Post-hoc comparisons showed at maintenance of physical function from baseline (M = 9.60, SE = 0.35) to 6 months (M = 9.50, SE = 0.38, p > .05). At 12 months, physical function abilities had declined (M = 2.94, SE = 0.07, p < .001) relative to baseline and 6-month scores. There was no main effect for race (p = .19), nor was there a significant Race × Physical function interaction, F(2, 172) = 2.59, p = .08, indicating the trajectory of decline in physical function which over time did not differ between African Americans and White elders (Figure 2).
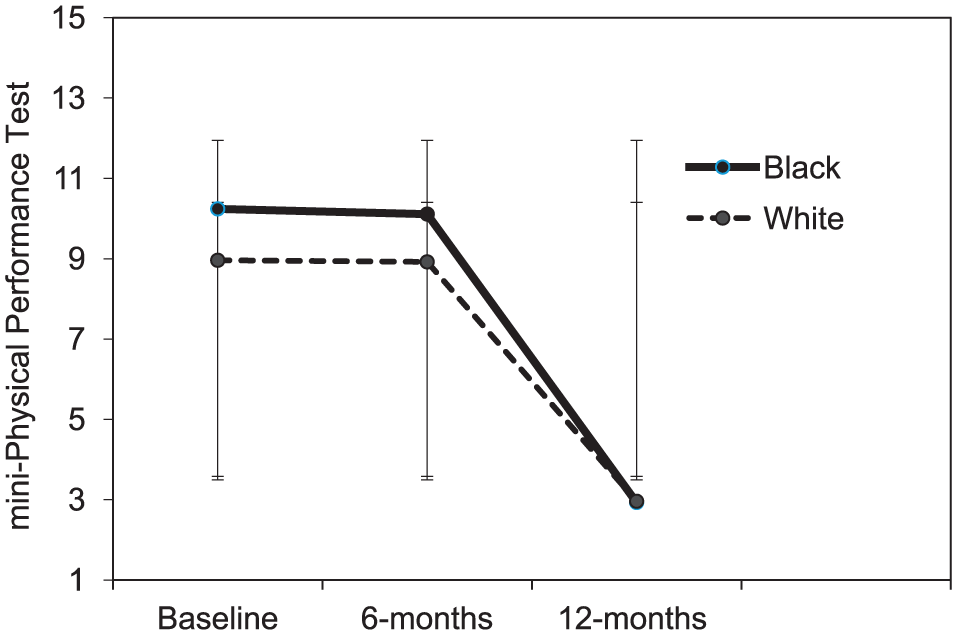
mini-Physical Performance Test (mini-PPT) performance at baseline, 6-month postintervention, and 12-month postintervention by race.
Mood
Depression symptoms changed over time, F(2, 40) = 25.70, p < .001), η2 = .55. Post-hoc tests showed that depressive symptoms decreased from baseline (M = 0.65 ± 0.07) to 6 months (M = 0.15 ± 0.04, p < .001) and increased from 6 months to 12 months (M = 0.68 ± 0.07, p < .001). There was no main effect for race (p = .17), nor was there a significant Race × Depression score interaction (p = .52), see Figure 3.

Log-transformed scores on Patient Health Questionnaire-9 (PHQ-9) performance at baseline, 6-month postintervention, and 12-month postintervention by race.
Discussion
This program combined evidence-based interventions and transdisciplinary expertise to implement a multidimensional intervention targeting key risk factors for disability and frailty. Our program resulted in short-term maintenance of physical function and a decrease in depressive symptoms among community-dwelling older adults at risk for frailty and disability. Bone density scores were maintained from baseline to 12 months. These results suggest a community-based, multidimensional intervention may be useful in attenuating decline in risk factors for disability and frailty in this population.
Few multidimensional intervention studies have examined racial differences in functional outcomes in older adults. In our study, physical function was maintained during the 6-month intervention for both White and African American elders; however, at the 1-month assessment, physical function had declined. Our findings are similar to that of Gitlin and colleagues (Gitlin, Winter, Dennis, & Hauck, 2008) who reported similar functional outcomes between White and African American elders who participated in a 6-month, multidomain, in-home intervention. In that study, African Americans reported more functional difficulty in instrumental activities of daily living than Whites 12-months postintervention.
One reason for a reduction in effect in our study may be due to the relatively low intensity of our physical activity intervention. We provided participants with resistance bands, pedometers, and exercise manual, along with a single interactive physical activity session; this may not be adequate for sustainable effects on physical function. Relatedly, we did not include measures of adherence to the program recommendations; therefore, we cannot determine if participants followed recommended guidelines. A separate community-based study that implemented a multidimensional intervention to address heath behaviors in older adults found improvement in functional mobility and walking behavior after 12 weeks (Turk, Elci, Resick, & Kalarchian, 2016). This study did not complete a follow-up assessment; however, the findings do highlight the efficacy of a relatively low-intensity intervention to improve physical function in community-dwelling older adults.
Depressive symptoms decreased during the intervention but increased at 12-months postintervention for both African American and White elders. Prior work has shown depressed mood in older adults is responsive to nonpharmacological interventions (Fuentes & Aranda, 2012; Lee et al., 2012). Research reporting longer-term, positive effects on mood were randomized controlled trials that utilized complimentary therapies (Ciechanowski et al., 2004) including individualized cognitive-behavioral therapy (Serfaty et al., 2009). Prior research focused on effective strategies to improve depressed mood among racial and ethnic minority elders stressed the importance of collaborative and integrated care models (Fuentes & Aranda, 2012). In our program, we utilized a collaborative care model to implement our mood intervention. Acute benefits for mood among our participants were observed possibly because the mood intervention occurred at the 6-month time point concurrent with our scheduled reassessment. Given these short-term positive effects on mood, our findings may imply that longer-term mood interventions that incorporate complementary therapies may be necessary for prolonged improvement of depressive symptoms in this population.
The use of Vitamin D and calcium supplementation for the prevention of fractures is controversial. The 2013 U.S. Preventative Services Task Force reports there is insufficient evidence to assess the benefit and harms of combined Vitamin D and calcium supplementation for the primary prevention of fractures in postmenopausal women (Moyer, 2013). Despite this evidence, Vitamin D and calcium supplementation is often recommended to postmenopausal women for the prevention of fractures (Abrahamsen, 2017). Randomized controlled trials have reported a modest reduction in fracture risk in this population. Modest improvements in BMD have also been reported; however, these results have been most consistently reported for lumbar spine, total hip, femoral neck, and total body skeletal sites (Tai, Leung, Grey, Reid, & Bolland, 2015). We assessed the proximal and distal forearm, common sites for osteoporosis screening (Marshall, Johnell, & Wedel, 1996; Wilkins & Birge, 2005). Our null findings may suggest this is an adequate skeletal site for assessing changes in BMD. It is also plausible that our relatively short intervention impeded our ability to measure modest increases in BMD, as other studies reporting positive effects were at least a year in duration (Tai et al., 2015). Twelve-month focus groups indicated that compliance with the Vitamin D supplements was poor (50%) consistent with other Vitamin D intervention trials (Brunner et al., 2008; Brunner et al., 2011). The inclusion of supplemental, nonpharmacological therapies (i.e., weight-bearing exercises) that improve bone and muscle strength may be necessary as complementary therapies to preserve bone health in this population (Dawson & Dennison, 2016).
The CARE program has several strengths. First, we designed and implemented a multidimensional intervention program targeting risk factors for frailty and disability in a community setting. Our use of a transdisciplinary team of health professionals to design and implement this program helped to ensure a breadth of geriatric health expertise while providing an applied learning experience for future health professionals. Second, our longitudinal design allowed us to examine both acute and longer-term effects of targeted evidence-based interventions on major risk factors for frailty and disability. Third, the recruitment and retention of a substantial proportion of African American elders in this study is noteworthy, as this population is disproportionately affected by risk factors for disability (Latham, 2012), while being underrepresented in behavioral health interventions. Lastly, the pragmatic design of the program is easily replicable and may serve as a basis for future studies to examine how feasible it is to translate this program design in clinical practice. Despite these strengths, our program was limited by underrepresentation of males and a nonrandomized control study design. We did not include measures to determine the effectiveness of the intervention sessions or adherence to program recommendations. We did not adequately query physical activity, which may be a confounder in our findings.
Targeting risk factors for frailty and disability in vulnerable aged populations has broad implications for decelerating the disablement process prolonging years of independent living in this population. Our community-based program shows promise as a method for providing preventative care to at-risk seniors. Extended benefits of this care model likely are contingent on a continued relationship with this community. Future work should seek to address limitations of our program, namely the implementation of a longer-term multidimensional program and the inclusion of a randomized controlled study design. Extension of this work may inform a new model of preventative care for community-dwelling seniors at risk for frailty and disability.
Footnotes
Authors’ Note
Researchers will provide select research materials upon request. The funders had no role in the design or conduct of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Barnes-Jewish Hospital Foundation and the NIH-Beeson Career Development Award in Aging Research-K23AG026768.