
Abstract
Introduction
As populations age, the need for home and community-based long-term care services tends to increase as well. Determining the appropriate mix between unpaid care provided by family, friends, neighbors, and others with a social relationship to the supported person (informal care) and paid care services by a health care institution or individual for a person in need (formal care) has therefore become an increasingly important policy issue, both nationally and internationally (Genet, Kroneman, & Boerma, 2013; Organisation for Economic Co-operation and Development [OECD], 2005). Knowing what factors influence access to and use of various types of care and how they do so is essential to developing and evaluating such policies (Paraponaris, Davin, & Verger, 2012). For example, it is frequently reported that health-related need is the primary factor influencing the receipt of care (e.g., Kadushin, 2004), with indicators of social location and access to social resources often seen as operating indirectly, through their influence on health-related needs for care. This, in turn, has led to conclusions that formal services are generally provided equitably, insofar as they are primarily or exclusively responsive to health-related needs for care. Conversely, it is informal care that is sometimes found to be more strongly influenced by enabling factors such as the availability of informal sources of support (e.g., van Groenou, Glaser, Tomassini, & Jacobs, 2006).
Yet, caution is needed when drawing conclusions regarding equity of access to in-home care services. Despite extensive research, whether and how predisposing, enabling, and need factors influence the receipt of in-home care remains unresolved. Findings tend to be inconsistent, perhaps reflecting the diverse and continually changing societal and policy contexts within which care arrangements are situated and shaped (Kadushin, 2004). The role of social support in influencing the receipt of care appears particularly unclear. To date, considerable research has been conducted on relationships between informal and formal care, focusing primarily on the issue of whether they tend to substitute for or complement one another (e.g., Bonsang, 2009; Geerts & van den Bosch, 2012; Pezzin, Kemper, & Reschovsky, 1996). Yet, social support, as generally conceptualized, encompasses more than the provision of tangible forms of informal care or assistance (e.g., affection, information, and companionship). However, we know little about the significance of overall support or of these specific domains for the receipt of care.
Given the limitations of currently available studies, the main objective of the current study is to empirically assess to what extent individual-level indicators of social location, access to social and economic resources, and health-related needs for care are associated with the receipt of informal care, formal care, or a mix of both informal and formal care among middle-aged and older adults with functional health limitations. We address these questions using data from the 2008-2009 Canadian Community Health Survey (CCHS).
The Behavioral Model and the Determinants of In-Home Care
Numerous studies have addressed the determinants of informal as well as formal in-home care in Canada, the United States, and European countries (see Kadushin, 2004 for a review). To frame their studies theoretically, many have drawn on the behavioral model proposed and subsequently modified by Andersen and his colleagues (e.g., Andersen, 1995; Andersen & Newman, 1973). The model identifies various societal-, health system-, and individual-level determinants that are said to influence the receipt of care. Individual level determinants include predisposing, enabling, and need factors. Predisposing factors influence the propensity that people will use services and include background characteristics such as age and gender as well as individual preferences and expectations about health and health care. Enabling factors refer to the resources that facilitate or inhibit access to care services. These could be either personal or community resources including social support, financial capacity, or health insurance coverage. Finally, need factors represent the need for the care based on functional limitations as well as other indicators of physical and mental health status.
Empirical assessments of the utility of the behavioral model for an understanding of health service use generally confirm the importance of various predisposing, enabling, and need factors to in-home and other health services use (e.g., see Bruni & Ugolini, 2016; Forbes & Janzen, 2004; Grabbe et al., 1995; Pinquart & Sörensen, 2002; Wallace, Levy-Storms, Kington, & Andersen, 1998). However, results are frequently contradictory and difficult to interpret, in part, due to differences in the groups being compared. Some studies compare those receiving informal care with those receiving no informal care (with the latter potentially including those receiving no care as well as formal care—for example, see Larsson & Silverstein, 2004; Vlachantoni, Shaw, Evandrou, & Falkingham, 2015) whereas others compare those receiving informal care only with those receiving no care (Paraponaris et al., 2012; Suanet, van Groneau, & van Tilburg, 2012) or both informal and formal (i.e., mixed) care (Carrière, Martel, Légaré, & Morin, 2006). Similar differences characterize their focus on the factors that influence formal care and/or mixed care.
Differences also emerge with respect to how both informal care and formal care are defined as well as the samples studied. Whereas some focus on determinants of the receipt of care among middle-aged and/or older adults in general (e.g., Chappell & Blandford, 1991; Suanet et al., 2012), others restrict their focus to those with selected types or levels of functional limitations (Carrière et al., 2006; Paraponaris et al., 2012; Vlachantoni et al., 2015). Finally, there is also some evidence to suggest cross-national differences and temporal changes in the factors that influence the receipt of care, in part reflecting the different and changing policy contexts within which the provision of care is situated (e.g., see Bolin, Lindgren, & Lundborg, 2008; Geerts & van den Bosch, 2012; Suanet et al., 2012; van Groenou & De Boer, 2016; van Groenou et al., 2006; Wilkins, 2006).
Social Support as an Enabling Factor
Andersen’s behavioral model includes social support as an enabling factor for health care utilization. As a concept, social support has been variously defined and operationalized (Cohen, Gottlieb, & Underwood, 2000; Gottlieb & Bergen, 2010). However, it is perhaps most frequently used to refer to the functional resources accessible through one’s informal network (i.e., family members, friends, neighbors—see Cohen et al., 2000). Most often, these include tangible or instrumental support (e.g., help with everyday activities such as housekeeping, transportation, and financial assistance) as well as emotional support (e.g., information leading persons to believe that they are loved, cared for, esteemed and valued—see Cobb, 1976), informational support (the provision of relevant information intended to help the individual cope with current difficulties—Cohen, 2004), appraisal support (information relevant to self-evaluations) and social companionship (spending time with others in social and/recreational activities) perceived and/or enacted within the context of people’s informal relationships (Cohen et al., 2000; House & Kahn, 1985; Sherbourne & Stewart, 1991).
To date, limited attention has been focused on the impact of social support on the receipt of informal and/or formal care (see Penning, 1995). Instead, research attention has been directed almost exclusively to the role of informal care in influencing the use of formal care, with informal care frequently considered a measure of social support or as one type of support (i.e., tangible or instrumental support—for example, see Pinquart & Sörensen, 2002). At a theoretical level, however, whether informal care should be considered synonymous with social support remains unresolved. As concepts, care and support often appear to be used interchangeably: “(c)are and support from family members, as well as from friends and neighbors, are typically referred to as informal social support” (Williams & Dilworth-Anderson, 2002, p. 225). However, other researchers consider them to be distinct, with the difference lying not in what is being provided but rather, the circumstances in which it is being provided: “when support is provided because of a senior’s long-term health problems or functional limitations, it should be designated as care . . .” (Keating, Otfinowski, Wenger, Fast, & Derksen, 2003, p. 120).
To the extent that social support and informal care can be differentiated based on health limitations and/or the need for assistance, the issue becomes whether one can receive both social support and informal care at the same time. In other words, if and when support/care is being provided in response to specific functional limitations (e.g., limitations on one’s ability to do heavy housework), does this mean that all forms of support being provided within the context of the informal relationship should now be considered forms of care rather than of support? Conversely, can they even be separated? Calasanti and Bowen (2006) suggest not: researchers often use a definition of caregiving that includes only instrumental and personal care tasks. However, feminists have long argued that much invisible labor is involved in care work. A more inclusive definition takes into account the caregiver’s mental and emotional responsibility for the care receiver, in addition to their responsibility for their physical well-being . . . (p. 261)
On the contrary, redefining all forms of “support” as forms of care appears equally problematic.
Research Questions
The current study builds on the theoretical background and research findings reviewed above. Specifically, it draws on Andersen’s behavioral model to identify the predictors of home care use—including informal, formal, and mixed home care—among middle-aged and older adults in the contemporary Canadian context who experience some level of functional impairment. In Canada, as in many other countries, publicly funded formal in-home care is increasingly becoming a residual form of care to that being provided or funded privately by families (Forbes et al., 2003; Martin-Matthews, Sims-Gould, & Tong, 2013; Penning, Brackley, & Allan, 2006). Formal in-home care also has become increasingly restricted in the type of services provided (often providing personal care, nursing, and therapeutic services rather than supportive care—Keefe, Légaré, Charbonneau, & Décarie, 2012) as well as to whom such services are provided (through means testing, restricting access to those who are at the end of life or at risk of hospitalization). These changes, which have been linked to reductions in the utilization of governmentally subsidized home care services (Brackley & Penning, 2009; Wilkins, 2006), may well influence the importance of various factors (e.g., income—see Mery, 2013) in influencing the receipt of care, whether it be formal or informal. These changes, gradually implemented since the 1990s (Penning et al., 2006), point to a need for studies to be conducted using data collected following the implementation of such measures. For example, Carrière et al. (2006), in the most recent Canadian study to address such issues, drew on data collected in the mid-1990s and found that factors such as gender and income did not predict the receipt of informal, formal, or mixed in-home care among older adults who received assistance because of a long-term health problem. Is this still the case?
The role of social support in influencing the receipt of informal and/or formal care also warrants investigation. If social support and informal care are synonymous, there seems little basis for addressing the role of social support as an enabling factor influencing informal care. Instead, studies should continue to focus primarily on associations between informal and formal care. However, to the extent that they are distinct from one another, there is a clear gap in our understanding of the role of social support in influencing informal care. Here, we address this issue as an empirical question, focusing on associations between multiple dimensions of social support and the receipt of various forms of informal care as reported by care recipients.
The following research questions are addressed:
Method
Data and Sample
We used the public use microdata file (PUMF) from the 2008-2009 CCHS—Healthy Aging (Statistics Canada, 2010). The survey was designed to collect information about the factors and processes that contribute to healthy aging, including health, social, and economic determinants.
The CCHS was a cross-sectional survey of persons aged 45 and older living in private dwellings in the 10 Canadian provinces. Residents of the three territories, persons living on reserves or in institutions, as well as full-time members of the Canadian Forces and residents of some remote regions were excluded from the sampling frame. Together, these exclusions represent less than 3% of the target population (Statistics Canada, 2010). A total of 30,865 valid interviews were conducted using computer-assisted personal interviewing (CAPI) with a response rate of 74.4%. Additional information on methodology and sampling strategies of the CCHS is available elsewhere (Statistics Canada, 2010). For the current study, we selected all respondents who provided information on in-home care services (13 cases were excluded due to missing data) and who indicated experiencing at least some level of functional impairment in their activities of daily living (N = 5,898). Missing data from the independent variables were handled using the listwise deletion. All statistical estimates were conducted using data weighted to be representative of the target population.
Measures
In-home care services
Four categories of in-home care services were differentiated: (a) no care, (b) formal care only, (c) informal care only, and (d) both (mixed) formal and informal care. These were constructed based on respondents’ answers to questions regarding their receipt of six specific services (i.e., personal care; medical/nursing care; care management; help with housework, home maintenance, or yardwork; transportation; and assistance with meal preparation or delivery) provided by professionals (=formal care) and/or by family members, friends, or neighbors (=informal care) during the past 12 months because of physical, mental, or cognitive health problems or limitations or because of aging. Professional assistance included help from paid workers or volunteer organizations and thus included both publicly funded and privately paid services.
Predisposing factors
Predisposing factors included gender, age, education, and race. Each was a categorical variable. Gender was a dichotomous measure (male, female). Age was measured using the four categories available within the PUMF data files: (a) 45 to 54 years, (b) 55 to 64 years, (c) 65 to 74 years, and (d) 75 and older. Level of education was categorized as: (a) less than secondary school completion, (b) secondary school completion but no postsecondary education, and (c) some postsecondary education (with or without a postsecondary degree or diploma). Finally, race was assessed based on the respondents’ self-identified cultural and racial backgrounds as White or non-White.
Enabling factors
Three enabling factors were included in the analyses: income, living arrangements, and social support. Income was assessed based on respondents’ estimates of their total household income (received by all household members, from all sources, before taxes and deductions, in the past 12 months) with responses categorized into five groups: (a) less than Can$20,000, (b) Can$20,000 to Can$39,999, (c) Can$40,000 to Can$59,999, (d) Can$60,000 to Can$79,999, and (e) Can$80,000 and over. To assess living arrangements, those living alone were compared with those living with someone else (e.g., a spouse and/or others).
Finally, we drew on the Medical Outcomes Study (MOS) Social Support Survey (Sherbourne & Stewart, 1991) to measure social support. The MOS is a 19-item self-administered scale that assesses the perceived availability of functional social support in four domains: affectionate support, emotional/informational support, positive social interaction, and tangible support. For each item, respondents were asked to indicate how often support was available (1 = none of the time; 2 = a little of the time; 3 = some of the time; 4 = most of the time, or 5 = all of the time). Affectionate support items measured the level of affection the respondent received and included questions about whether or not the respondent had someone that showed him or her love, someone to hug or love, and make him or her feel wanted (0-12). In the CCHS, emotional and informational support items were scored together and assessed whether the respondent had someone to listen and to advise them in a crisis, someone to give information and confide in or talk to, or someone who understands his or her problems (0-32). Positive social interaction measured whether the respondent had someone to have a good time with, get together with for relaxation, do things with to get his or her mind off things, or someone to do something enjoyable with (0-16). Finally, tangible support covered the provision of material aid or behavioral assistance, and included help if confined to bed, having someone to take you to the doctor, and having someone to prepare meals or do daily chores (0-16).
Correlations among the four social support domains were fairly strong (.66-.82), providing some initial support for using the combined measure (0-76). In contrast, correlations between each of the support domains and informal care were weak (.04-.10). Given these findings, our analyses drew on both the overall measure of social support (0-76) as well as on the four domain-specific measures. All scores were standardized with higher scores indicating more support within or across the four social support subscales.
Need factors
Several health-related need factors were included in the analyses. Self-rated physical and mental health were measured as dichotomous variables based on whether respondents reported their health as being (0) fair or poor or (1) excellent, very good, or good. A measure of functional limitations was created based on respondents’ ratings on a modified module of the Activities of Daily Living questions (i.e., eating, dressing, walking, getting in and out of bed, bathing, etc.) of the Older Americans Resources and Services (OARS) Multidimensional Assessment Questionnaire (Fillenbaum, 1988). Functional limitations, were coded in the PUMF using a 5-point scale with higher values indicating greater functional impairment. Because we excluded respondents who reported no functional impairment from the study sample, our measure had four categories (1 = mild; 2 = moderate; 3 = severe; 4 = total impairment). Finally, cognitive impairment was assessed using a module containing four timed memory tests, an executive functioning test, the Mental Alternation Test (MAT, Salib & McCarthy, 2002), and a words recall test. Responses from all four tasks were integrated to create a measure of six cognition levels (1 = able to remember most things, think clearly and solve day to day problems; 2 = able to remember most things, but have a little difficulty when trying to do the above tasks; 3 = somewhat forgetful, but able to do the above tasks; 4 = somewhat forgetful, and have a little difficulty when trying to do the above tasks; 5 = very forgetful, and have great difficulty when trying to do the above tasks; 6 = unable to remember anything at all, and unable to do the above tasks).
Data Analysis Procedures
A series of multinomial logistic regression analyses were conducted to assess the impact of predisposing, enabling and need factors on in-home care use. The first set of analyses contrasted those who received each of three different home care services (formal care only; informal care only; or a mix of both formal and informal care) to those who received no care (reference category). The second set of analyses contrasted those receiving formal care only or a mix of formal and informal care to those receiving informal care only (reference category). Both sets of analyses were conducted using both: (a) the summary measure of social support (see Models 1 to 5); and (b) the four domain-specific measures of support (see Models 6 to 10). Predictor variables were entered sequentially, with predisposing factors entered first (as a block), followed by enabling factors, and finally, need factors. Here, we report the results of the final models only (the results of the sequential analyses are available upon request). Collinearity among the variables was minimal and variance inflation factors (VIFs) were less than 2 in all models.
Results
Over a third (38.7%) of the respondents included in our sample of middle-aged and older adults who had functional limitations received no care from family members, friends, neighbors, or home care professionals (see the appendix). Most of those who received care relied exclusively on care from family members, friends, or neighbors (51.3% of those who received care; 31.4% of total sample). The remainder either received assistance both from family members, friends, or neighbors and formal services (33.9% of those who received care; 20.8% of total sample) or received care from formal services only (14.8% of those who received care; 9.1% of total sample).
Table 1 (Models 1 to 3) reports the results of analyses conducted to estimate the odds of receiving each type of in-home care service in comparison to the odds of receiving no care. Model 1 reveals that those who were White and who reported fair or poor physical health were significantly more likely than those in the reference categories to rely on formal care rather than no care. In contrast, those who were in middle-aged and young-old age groups, had less than a postsecondary education, were living with someone, had moderate rather than high incomes, and had comparatively high levels of cognitive functioning were significantly less likely than those in the reference categories to rely on formal rather than no care. In addition, those reporting higher levels of social support were less likely than those reporting lower levels of support to be receiving formal rather than no care. With these factors taken into account, neither gender nor functional impairment or self-reported mental health status emerged as significantly related.
Multinomial Logistic Regression Models of Types of In-home Care on Predisposing, Enabling and Need Factors.
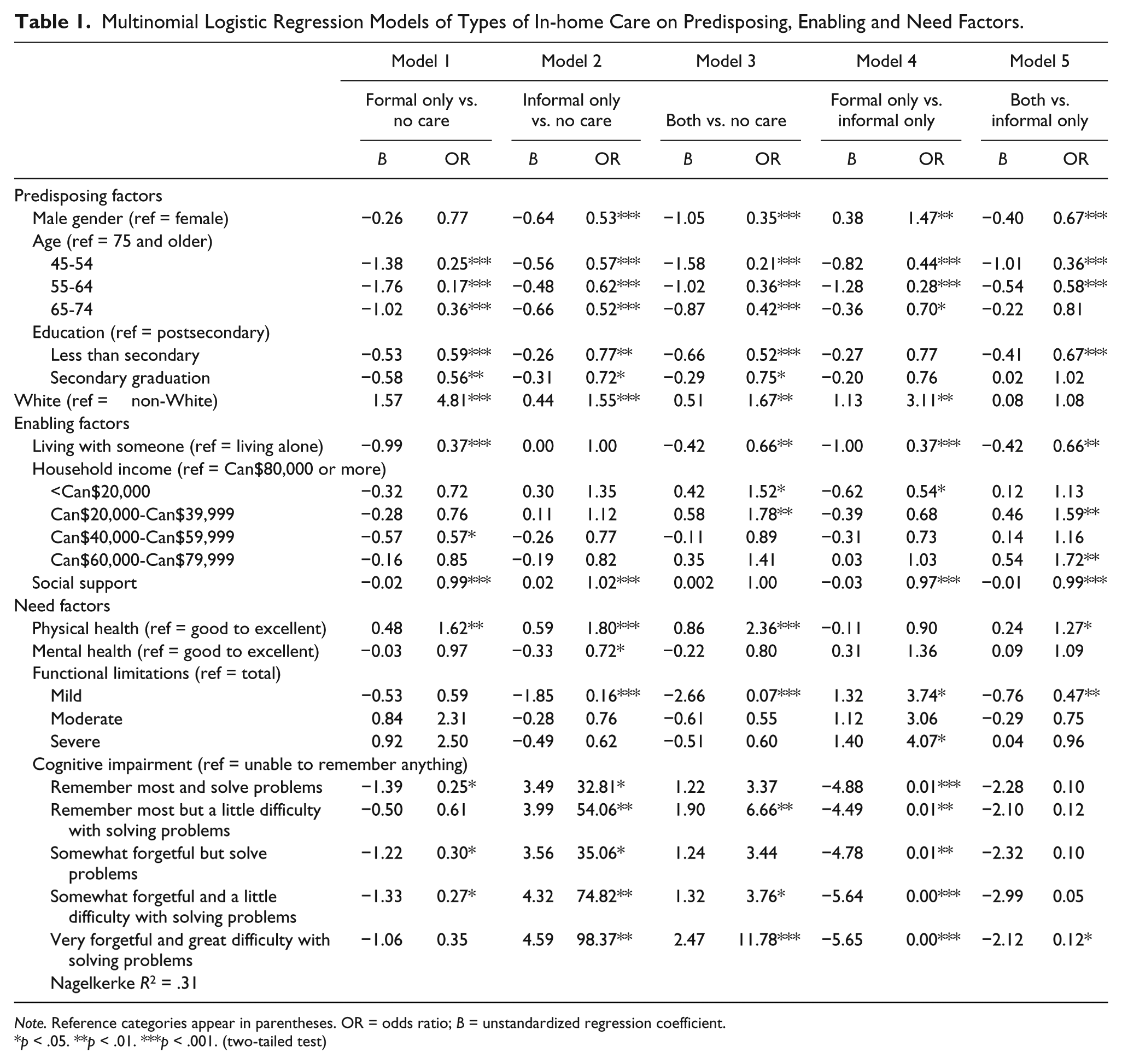
Note. Reference categories appear in parentheses. OR = odds ratio; B = unstandardized regression coefficient.
p < .05. **p < .01. ***p < .001. (two-tailed test)
Model 2 indicates that in contrast with the model for formal care, those reporting higher levels of social support were more likely to be receiving informal rather than no care. In contrast, the results were similar to those obtained when looking at the determinants of formal care with regard to the impact of age, education, race, and self-reported physical health status. However, gender was also influential, with men being significantly less likely than women to be receiving informal care than no care. In this model, health factors also emerged as significant. Those reporting only mild functional limitations were less likely than those with very high levels of functional impairment to report receiving informal care rather than no care. Mental health and cognitive impairment were also relevant: Those reporting fair to poor mental health were less likely than those reporting good to excellent mental health to report receiving informal rather than no care while those at all but the most impaired levels of cognitive functioning were more likely than the latter to report receiving informal care rather than no care. Finally, whether respondents lived alone or not did not differentiate those receiving informal care from those receiving no care. Nor was household income a significant factor.
Model 3 reports the results obtained when comparing those receiving both informal and formal care to those receiving neither. In these analyses, social support did not emerge as being significantly related to the receipt of both informal and formal rather than no care. However, the results were once again similar with regard to the impact of age, education, race, and self-reported physical health status. Like the results obtained with regard to the receipt of informal care only (Model 2), gender once again emerged as significantly related, with men being less likely than women to be receiving both informal and formal care than no care. Functional and cognitive limitations also emerged as related. Those reporting mild rather than extreme functional limitations were less likely to report receiving both informal and formal care. In contrast, those reporting some cognitive impairment were more likely than those with the highest levels of cognitive impairment (the reference category) to report receiving both informal and formal rather than no care. However, similar to Model 1 (formal care only), those living with others were less likely than those living with others to be receiving both informal and formal care compared with no care. As in Model 1 as well, mental health did not emerge as a significant factor in Model 3. Finally, with all of these factors taken into account, those with lower levels of household income were more likely than those with high incomes to be receiving both informal and formal care than no care.
Models 4 and 5 examined the probability of receiving formal care only (Model 4) or a mix of both forms of care (Model 5), using informal care only (rather than no care) as the reference. Model 4 revealed that reporting higher levels of social support was associated with a lower likelihood of receiving formal care only rather than informal care only. In addition, men, those who were White, and those who reported mild to severe rather than total functional impairment were significantly more likely than the reference categories to rely on formal care rather than informal care only. In contrast, those in each of the younger age categories, those who lived with someone else, who had the lowest incomes and who reported less than the most severe levels of cognitive impairment were less likely than those in the reference categories to rely only on formal care rather than only on informal care. With these factors taken into account, neither education nor self-reported physical and mental health status emerged as significantly related.
In Model 5, higher levels of social support once again were associated with a reduced likelihood of receiving both formal and informal care rather than informal care only. In addition, those with moderate rather than high incomes and who reported poorer physical health were significantly more likely to rely on both formal and informal care than informal care only. Men, those who were comparatively younger (45-54 years and 55-64 years), who had less than a secondary level of education, who lived with someone, who had mild functional limitations, and fairly high but not extreme levels of cognitive impairment were significantly less likely than those in their reference categories to rely on both formal and informal care than informal care only. With these factors taken into account, race and self-reported mental health status did not emerge as significantly related.
So far, our results suggest that higher levels of social support significantly reduce the likelihood of receiving formal care compared with either no care (Model 1) or to informal care only (Model 4). They also reduce the likelihood of reporting receiving both informal and formal care compared with informal care only (Model 5). In contrast, they increase the odds of receiving informal care only rather than no care (Model 2) and are unrelated to the odds of receiving both informal and formal care compared with no care (Model 3). To further address the impact of social support on the receipt of care, ancillary analyses were conducted in which the impact of each dimension of support was examined separately (see Table 2).
Multinomial Logistic Regression Models of Types of In-home Care on Social Support.
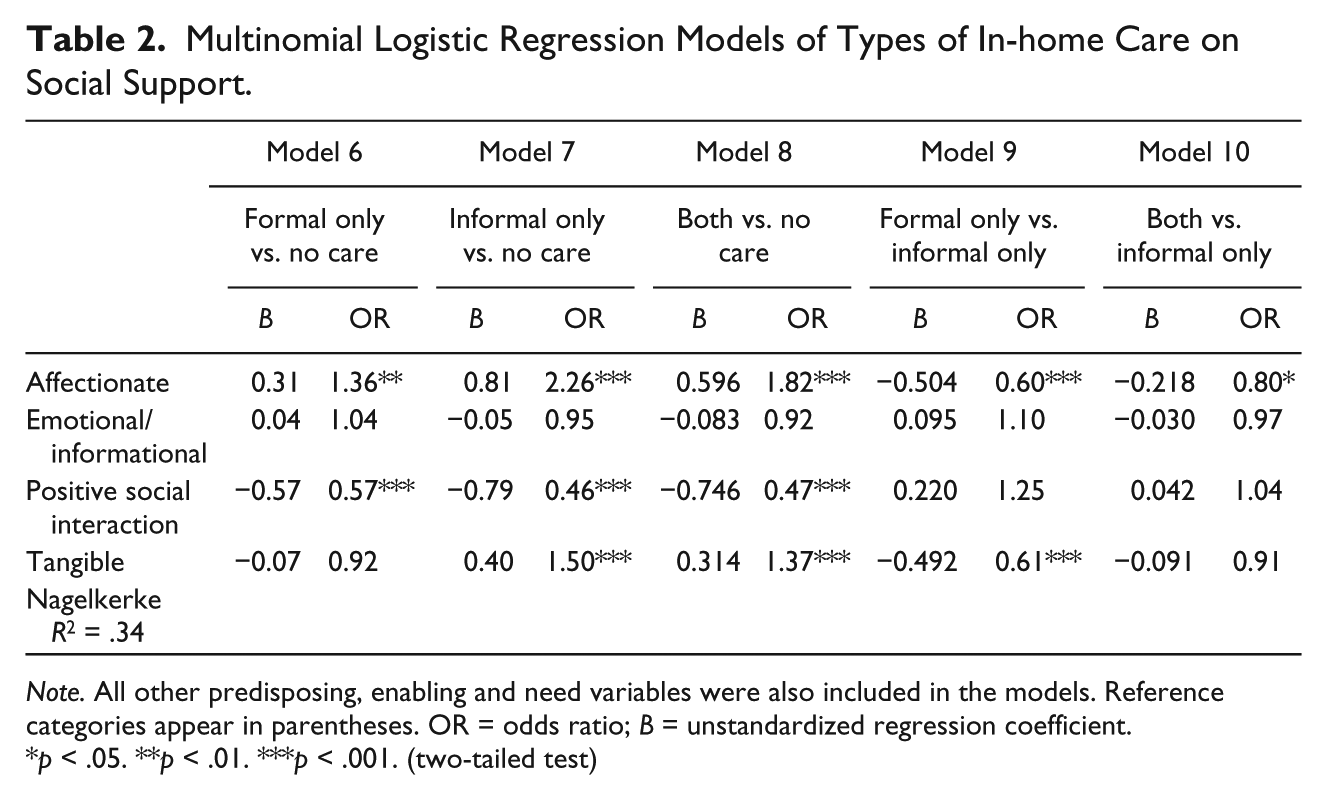
Note. All other predisposing, enabling and need variables were also included in the models. Reference categories appear in parentheses. OR = odds ratio; B = unstandardized regression coefficient.
p < .05. **p < .01. ***p < .001. (two-tailed test)
The results show that higher levels of Affectionate social support significantly increased the use of all types of care (formal only, informal only, both formal and informal) compared with no care (see Table 2, Models 6-8) and reduced the likelihood of relying on formal care only or on a mix of formal and informal care rather than informal care only (see Models 9 and 10). The receipt of Emotional and Informational support had no significant impact on the receipt of any type of care. In contrast and unlike Affectionate social support, Positive Social Interaction reduced the probability of receiving all types of care compared with no care. However, it had no significant impact on the likelihood of relying on formal care or a mix of formal and informal care rather than informal care only (Models 9 and 10). Finally, the receipt of Tangible support did not differentiate those who relied on formal care only from those receiving no care (Model 6). However, those receiving higher levels of Tangible support were more likely report receiving informal care only or a mix of informal and formal care rather than no care. Conversely, they were less likely to rely on formal than informal care only. No evidence was found to indicate that the receipt of Tangible support differentiated those relying on a mix of informal and formal care from those relying on informal care only.
Discussion
This study was conducted to empirically assess the impact of predisposing, enabling, and need factors on the receipt of in-home care—including informal, formal care, or a mix of both types of care—among middle-aged and older adults with functional health limitations who lived in the community. The role of social support was of particular interest given its theoretical significance together with indications that it is distinct from informal care and yet, research evidence regarding its significance is lacking. Several theoretically and empirically significant results emerged.
First, our results indicated that the largest proportion (38.7%) of middle-aged and older adults with functional health limitations reported receiving no care, whereas 31.4% received only informal care, 9.1% received only formal care, and 20.8% received both informal and formal care. Thus, among those who reported receiving some form of care only, over one half (51.3%) received informal care only whereas 14.8% received formal care only, and 33.9% received a mix of informal and formal care. To some degree, these results approximate those reported in other countries, albeit perhaps with greater variations evident in levels of formal and mixed care than informal care (e.g., see Hellström & Hallberg, 2004; Paraponaris et al., 2012). Interestingly, the proportion relying on formal services alone appears somewhat lower whereas the proportion relying on informal care only or on a mix of informal and formal care appears somewhat higher than that reported in previous Canadian research (Carrière, Martel, Légaré, & Morin, 2006). These differences may reflect differences in the age ranges and/or disability levels of the samples studied as well as the measures of informal and formal care used. However, they may also stem from changes in policies governing access to formal in-home care services and implemented in the Canadian context as of the 1990s and which focus on restricting the use of public services while increasing private responsibilities for care (i.e., both privately paid and unpaid family care—see Martin-Matthews et al., 2013; Penning et al., 2006).
Predisposing, enabling and need factors were significantly related to the receipt of care. Although we reported the results of the final models only, our hierarchical regression analyses nevertheless provide evidence revealing both the main effects of each set of factors as well as the mediating effects of enabling and need factors in influencing the receipt of care. With regard to predisposing factors, for example, while men were less likely than women to receive formal care rather than no care, gender was no longer a significant determinant of formal (vs. no care) once enabling factors were included in the model. However, age and race retained their significance despite the introduction of enabling and need factors into the model, suggesting that both factors influence the receipt of formal care independently of such factors, at least in part. Education on the contrary, was not significantly related to the receipt of formal care when only predisposing factors were considered; however, it became significant (with higher education associated with the use of formal rather than no care) once enabling factors were included. Overall, our findings provide limited support for the view that predisposing and enabling factors have only indirect effects (i.e., by influencing access to resources and/or health-related needs) and the corresponding conclusion that need factors are the most important determinants of the receipt of care. Instead, our findings support the broader utility of the behavioral model—one that includes the direct as well as indirect effects of predisposing, enabling and need factors—as a framework for addressing the determinants of both formal and informal in-home care arrangements.
Focusing on the final models, our results revealed that various indicators of social location were associated with in-home care use. For example, men were more likely to receive formal care only (vs. informal care only) but less likely to receive informal care only (vs. no care) or a mix of both forms of care (vs. either no care or informal care only). A significant age gradient was also evident, with those aged 75 years and older significantly more likely to receive in-home care, regardless of type, in comparison to younger respondents. Similarly, an education gradient was evident such that individuals with postsecondary education had higher odds of receiving most forms of care (with the likelihood of receiving formal care only versus informal care being the only exception). Yet, the largest disparities in in-home care utilization involved race, with Whites being approximately 1.5 to 4.8 times more likely than non-Whites to receive formal, informal, or a mix of both in-home care (vs. no care). A similar trend was evident when comparing the receipt of formal care only to informal care only. It was only when comparing the likelihood of receiving both informal and formal care to the receipt of informal care only that race was not significant.
Enabling factors were also important to the receipt of care. For example, living with others reduced the likelihood of receiving formal care only and a mix of both forms of care compared with no care as well as to informal care only. However, living alone did not differentiate those receiving informal care only from those receiving no care. The importance of living arrangements is generally consistent with previous research (Carrière et al., 2006; Forbes & Janzen, 2004; Forbes et al., 2003; Wilkins & Park, 1998). However, in contrast with some (Carrière et al., 2006) but not all previously reported Canadian research (Forbes & Janzan, 2004; Wilkins & Park, 1998), income also had an impact, particularly on the receipt of formal care. Specifically, whereas moderate (rather than high) incomes were associated with a reduced likelihood of formal in-home care (vs. no care), lower (and/or moderate) incomes were associated with an increased likelihood of receiving both informal and formal care (vs. both no care and informal care only) but a reduced likelihood of receiving formal (vs. informal) care only. Differences between these and previous findings may reflect differences in sampling and measurement procedures (e.g., whether formal care included privately paid as well as publicly subsidized services). However, they may also reflect the changing policy context—one that sees access to public services increasingly restricted to those with low incomes. To the extent that this is the case, our findings suggest that those with moderate incomes may be becoming increasingly likely to do without in-home care (since our measure includes both publicly funded and privately paid services) whereas those with lower incomes (who may be eligible for public services) are increasingly required to rely on both informal and formal care services. With regard to social support in particular, our findings are also instructive. Those reporting higher levels of social support from their social networks report being less likely to be receiving formal care alone (rather than either no care or informal care only). They are also less likely to be receiving both informal and formal care than informal care alone. Thus, the overall support that one receives from one’s social network appears to be an important determinant of the type of care received. Moreover, the impact of support is not accounted for solely by the provision of tangible support. Affectionate support and positive social interaction also contributed to the receipt of in-home care. Moreover, they appeared to do so in different ways. Affectionate support emerged as particularly important, with higher levels being associated with an increased likelihood of formal care rather than no care. They also contributed to the receipt of informal and mixed care (vs. no care) as well as informal (vs. formal or mixed care). Positive social interaction, in contrast, was linked to a reduced likelihood of care regardless of its source, rather than no care. Finally, tangible support was not strongly associated with the receipt of informal care at the bivariate level but, in our multivariate analyses, was positively associated with the receipt of informal and mixed care rather than no care and negatively associated with the receipt of formal rather than informal care only. Thus, not only do tangible support and informal care appear to be distinct, but social support appears to be implicated in the receipt of care beyond its importance as a source of instrumental aid. The nature or quality of the relationships involved—whether they involve high levels of affection, social interaction, and/or tangible forms of support—also matters. Thus, our findings suggest a need to broaden our focus on the importance of the support network beyond its direct involvement in the provision of care itself.
Finally, our findings once again point to the importance of health-related need factors for the receipt of care. For example, the odds of receiving any type of in-home care versus no care were considerably higher for individuals with poorer physical health. Findings indicating that the odds of receiving informal care (vs. no care) or mixed care (vs. no care or informal care) were significantly lower among those reporting mild rather than extremely high levels of functional limitations suggests that informal and formal care networks are both responsive to levels of functional need. Cognitive impairment also had an impact. Low to moderate rather than extremely high levels of impairment reduced the likelihood of reporting formal care (vs. no care or informal care only) but increased the likelihood of informal or mixed care (vs. no care). Thus, formal in-home care services appear most involved when cognitive impairment is fairly high with informal care more likely to be involved in care for those with mild to moderate levels of impairment.
Several limitations should be noted when interpreting our results. First, although they were the most recent data available to us, the data employed within our analyses are now almost a decade old. Yet, the policy environment within which care arrangements are situated is constantly changing. Additional research conducted using more recent data will be needed to confirm the findings reported here as well as to help determine whether some of the differences evident between our findings and those reported in previous Canadian studies (e.g., regarding the prevalence of informal and formal care or the impact of income on the receipt of care) are consistent with changes evident in the policy context. In addition, our data were cross-sectional and limited to a focus on individual-level determinants of care. Thus, reverse causation (e.g., between social support and informal care), might result in problems of endogeneity. Also, like many other studies, we did not examine the impact of macro-contextual factors (e.g., societal determinants, policy factors) which more recent versions of the behavioral model suggest are also important to consider. For example, given that health care is a provincial responsibility and public home care policies and services differ somewhat across provinces in Canada, it is possible that differences in access to these services might influence the results. Furthermore, our study sample included those aged 45 years and older living in the community who reported some level of functional impairment, thereby restricting generalizability to this subpopulation and comparability to other studies employing similar sampling restrictions. With regard to measurement, we were unable to distinguish between publicly and privately paid formal care. Yet, in view of the shifts in health care policies evident in Canada and elsewhere in recent decades, this has become an increasingly significant distinction and one that requires in-depth study. It may be that several of the factors we found to be significant were relevant to one or the other of these sources of care. As well, we focused only on the receipt versus nonreceipt of care and did not address the levels of care received.
These and other limitations point to the need for further research to be conducted. Nevertheless, with these caveats in mind, our findings point to the importance of social location and social resources for influencing the receipt of in-home care over and above health-related needs. In particular, they suggest the need for researchers to direct greater attention to the role of social support in influencing the receipt of care, both informal and formal. Furthermore, they suggest the need for policy attention to be directed toward addressing the inequities in access to in-home care that appear to be associated with race and other markers of social location and access to social resources.
Footnotes
Appendix
Descriptive Statistics for Independent Variables by Type of In-home Care Use (N = 5,898).

| No care (n = 2,285, 38.7%) | Formal care only (n = 535, 9.1%) | Informal care only (1,853, 31.4%) | Both (n = 1,225, 20.8%) | |
|---|---|---|---|---|
| Predisposing factors | ||||
| Female, n (%) | 1,400 (61.3) | 348 (65.2) | 1,274 (68.8) | 920 (75.1) |
| Age | ||||
| 45-54 | 448 (19.6) | 90 (16.8) | 340 (18.3) | 70 (5.7) |
| 55-64 | 506 (22.1) | 38 (7.1) | 313 (16.9) | 188 (15.4) |
| 65-74 | 562 (24.6) | 85 (15.9) | 348 (18.8) | 229 (18.7) |
| 75 and older | 769 (33.7) | 322 (60.2) | 852 (46.0) | 737 (60.2) |
| Education | ||||
| Less than secondary | 893 (39.6) | 214 (43.1) | 896 (49.1) | 523 (43.3) |
| Secondary graduation | 405 (18.0) | 76 (15.3) | 265 (14.5) | 201 (16.6) |
| Postsecondary | 955 (42.4) | 206 (41.5) | 662 (36.3) | 485 (40.1) |
| White | 1,868 (82.3) | 452 (85.8) | 1,558 (85.1) | 1,080 (89.9) |
| Enabling factors | ||||
| Lives alone | 554 (24.3) | 269 (50.4) | 455 (24.6) | 489 (39.9) |
| Social support (SD) | ||||
| Total | 61.2 (18.1) | 55.4 (20.1) | 62.8 (15.0) | 59.3 (15.9) |
| Affectionate | 10.0 (3.0) | 9.1 (3.5) | 10.5 (2.5) | 9.93 (2.8) |
| Emotional/informational | 25.5 (8.2) | 23.6 (8.9) | 26.2 (7.0) | 24.8 (7.5) |
| Positive social interaction | 13.0 (4.0) | 11.0 (4.7) | 12.8 (3.8) | 12.0 (4.0) |
| Tangible | 12.6 (4.2) | 11.4 (4.9) | 13.2 (3.5) | 12.6 (3.7) |
| Household income | ||||
| <Can$20,000 | 340 (19.0) | 140 (35.4) | 331 (22.6) | 256 (26.1) |
| Can$20,000-Can$39,999 | 505 (28.3) | 125 (31.6) | 488 (33.3) | 370 (37.8) |
| Can$40,000-Can$59,999 | 372 (20.8) | 48 (12.2) | 287 (19.6) | 153 (15.6) |
| Can$60,000-Can$79,999 | 215 (12.0) | 26 (6.6) | 132 (9.0) | 100 (10.2) |
| Can$80,000 or more | 354 (19.8) | 56 (14.2) | 227 (15.5) | 101 (10.3) |
| Need factors | ||||
| Physical health: fair and poor | 897 (39.3) | 285 (53.3) | 1,054 (56.9) | 734 (60.2) |
| Mental health: fair and poor | 294 (13.5) | 102 (20.1) | 319 (19.6) | 181 (16.9) |
| Functional limitations | ||||
| Mild impairment | 2,024 (88.6) | 394 (73.6) | 1,220 (65.8) | 614 (50.1) |
| Moderate impairment | 207 (9.1) | 92 (17.2) | 452 (24.4) | 355 (29.0) |
| Severe impairment | 28 (1.2) | 26 (4.9) | 108 (5.8) | 129 (10.5) |
| Total impairment | 26 (1.1) | 23 (4.3) | 73 (3.9) | 128 (10.4) |
| Cognitive impairment | ||||
| Remember most and solve problems | 1,357 (59.4) | 245 (45.9) | 849 (46.0) | 580 (47.7) |
| Remember most but a little difficulty with solving problems | 64 (2.8) | 64 (12.0) | 78 (4.2) | 70 (5.8) |
| Somewhat forgetful but solve problems | 503 (22.0) | 125 (23.4) | 320 (17.3) | 212 (17.4) |
| Somewhat forgetful and a little difficulty with solving problems | 258 (11.3) | 59 (11.0) | 450 (24.4) | 184 (15.1) |
| Very forgetful and great difficulty with solving problems | 81 (3.5) | 18 (3.4) | 135 (7.3) | 124 (10.2) |
| Unable to remember and solve problems | 20 (0.9) | 23 (4.3) | 14 (0.8) | 46 (3.8) |
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education of the Republic of Korea