
Abstract
Mattering to others is a fundamental human motivation. As such, feelings that “others depend upon us, are interested in us, are concerned with our fate, or experience us as an ego-extension” (Rosenberg & McCullough, 1981, p. 165; Turner, Taylor, & Van Gundy, 2004) have been strongly linked to health and well-being (Pearlin & LeBlanc, 2001). Although an abundance of research shows how mattering is associated with mental health (Dixon Rayle, 2005; Marshall, 2001; Piliavin & Siegle, 2007; Raque-Bogdan, Ericson, Jackson, Martin, & Bryan, 2011; Rosenberg & McCullough, 1981; Taylor & Turner, 2001; Thoits, 2012; Turner et al., 2004), especially depressive symptoms (Taylor & Turner, 2001), suicide ideation (Elliot, Colangelo, & Gelles, 2005; Milner, Page, & Lamontagne, 2016) as well as more global assessments like happiness (Demier, Özen, Doğan, Bilyk, & Tyrell, 2011; Taniguchi, 2015) and psychological well-being (Dixon Rayle, 2005; Marshall, 2001), it is unclear whether these protective effects extend to physical health. Initial findings suggest a positive association (Fazio & Nguyen, 2014; Raque-Bogdan et al., 2011; Thoits, 2011). These findings center primarily on younger people, making it unclear whether the effects of mattering vary by age. This said, there are reasons to believe that these processes may vary by age, which is a key focus of the present research.
Aging, Relationships, and Health Processes
It is now well documented that the quality and quantity of personal ties change with increased age. Relative to younger adults, older people are more selective about their interpersonal relationships. They tend to be more concerned about emotionally meaningful experiences than on novel or future-oriented tasks, a process explained by the tenets of socioemotional selectivity theory (SST; Cartensen, Isaacowitz, & Charles, 1999). Age is associated with greater selectivity, focusing on and bolstering relationships that are more meaningful and fulfilling (positive), and abandoning or avoiding those that are extraneous (negative; Cartensen et al., 1999). Although the shrinking of social ties is an “adaptive” process (Charles & Cartensen, 2010), those who prune too much or never cultivate meaningful social relationships are at higher risk for a range of physical health consequences. For example, the risk for mortality among the socially isolated is about the same as for those who smoke (House, Landis, & Umberson, 1988). Therefore, maintaining robust social relationships throughout life, and in later periods of adulthood in particular, is positively associated with health and well-being (Berkman, Glass, Brissette, & Seeman, 2000; Holt-Lunstad, Smith, & Layton, 2010).
One useful measure for assessing biological pathways between relationships and health is allostatic load (AL), which is an index of the physiological wear and tear induced by the stress that is positively associated with morbidity and mortality (McEwen & Stellar, 1993). Although there is minimal research specifically examining the relationship between AL and social ties, there is evidence that suggests that appraisals of the quality of these relationships are important, particularly at older ages. Specifically, being more socially integrated and having higher emotional support from others is related to lower AL (Seeman, Singer, Ryff, Dienberg Love, & Levy-Storms, 2002) and helps to sustain allostasis (i.e., equilibrium in physiological function).
Adults become better at regulating their emotions and social lives as they age, and therefore, have more positive appraisals of life and people (Charles & Piazza, 2007). The unique skills and abilities that are obtained with age (e.g., managing interpersonal conflict) translate to older people being, on average, better at maintaining lower levels of distress than younger people (Newsom, Rook, Nishishiba, Sorkin, & Mahan, 2005). On the contrary, biological systems also become less flexible with age, and consequently, when faced with high levels of distress over an extended period of time, the age advantage associated with responding to stressors reverses. Older adults become less capable of regulating biological systems in the face of long-term high stress environments, leading to physiological dysregulation over an extended period of time (Levenson, 2000; Sapolsky, Krey, & McEwen, 1986). This may be one reason that research has shown that AL increases with age. To summarize, if older individuals are faced with brief periods of interpersonal conflict, they tend to maintain a balanced physiological system (i.e., allostasis) better than younger people, but when faced with sustained stressful or negative situations, older people are at higher risk of experiencing negative physiological responses, emerging in systemic ways such as through increased risk of high blood pressure (Hawkley & Cacioppo, 2007; Uchino, Uno, Holt-Lunstad, & Flinders, 1999).
AL and Mattering
One potential reason scholars have neglected the links between mattering, age, and health is that mattering is theorized to impact health through physiological stress pathways that necessarily involves a long latency period between stress exposure and disease onset (Kuh, Ben-Shlomo, Lynch, Hallqvist, & Power, 2003). The long and variable latency period between stress exposure and illness makes it easy to underestimate the negative effects of stress due to the misclassification of those in predisease states and stress-linked selective mortality (Turner, 2013). The social and biological processes connecting mattering to health occur over years or decades throughout the life course, but chronic disease does not generally manifest until older adulthood. Conventional health indicators, therefore, such as the number chronic conditions someone has been diagnosed with, represent instruments that are too blunt to gauge the physiological consequences of mattering for younger or middle-aged adults or accurately identify age gradations in the link between mattering and health. What is needed is an indicator that reflects the physiological residue of stress exposure that predates disease and is predictive of health. AL represents an indicator that meets these criteria.
In this study, we are interested in AL as our primary health outcome. We also present a parallel set of analyses with the number of chronic conditions as the dependent variable. We present these contrasts to illustrate the advantages of incorporating physiological dysregulation (i.e., AL) in assessing linkages between personal ties and physical health. We predict that mattering-based variations in the association between age and AL will only be detectable when AL is utilized as our health outcome of interest. Although the number of chronic conditions will likely share an inverse association with sense of mattering, this association will only reflect those old enough to experience chronic diseases linked with aging.
The present article attempts to build on current theoretical and empirical research examining age variations in the biological pathways associated with relationships, and mattering in particular, by addressing these research gaps. We employ data from a community-based study conducted in Davidson County, Tennessee (N = 1,026), to examine the relationship between mattering and AL, and whether these effects vary by chronological age. Based on our review of the literature, the analyses that follow will test the hypotheses that mattering will buffer, or condition, the positive relationship between age and AL. This hypothesis is based on the assumption that the positive relationship between age and AL will be greatest among those who possess lower levels of mattering. From this perspective, we anticipate that age-based increases in physiological dysregulation will be most harmful to those who lack meaningful personal ties.
Method
Data Source
The data for this investigation come from the Nashville Stress and Health Study (NSAHS). The NSAHS is based on a probability sample of non-Hispanic Black and White women and men (N = 1,026) aged 22 to 69 years living in Davidson County, Tennessee (http://vanderbilt.edu/stressandhealthstudy/). Survey Sampling International generated a random sample of 199 block groups in Davidson County. To adequately sample Black households, block groups were stratified by the percentage of Black residents (2010 Census). The study design included a random sample of 1,252 adults living in the sampled and stratified block groups. The sampling frame included 2,400 randomly sampled households. Only 2,065 of the 2,400 randomly sampled households were eventually contacted. Approximately 61% of contacted households agreed to participate in the study. Only one member of each household was selected to participate in the study.
The average computer-assisted interview lasted approximately 3 hr. All interviews were conducted by trained interviewers of the same race in the respondent’s home or on Vanderbilt University’s campus. All respondents received US$50 to participate in the interview phase of the study. The primary purpose of the NSAHS was to examine racial and socioeconomic disparities in health. Toward this end, the interviews collected detailed information concerning general sociodemographic characteristics, exposure to social stress, discrimination experiences, neighborhood environments, psychosocial resources, religious involvement, physical health, health care, mental health, and substance use.
During the interview phase, respondents were also given instructions and materials for biomarker collection. The morning after the in-person interview (before breakfast), a trained clinician visited the respondent to collect a 12-hr urine sample, a blood sample, three blood pressure readings (spaced 2 min apart), and anthropometric measurements of hip, waist, height, and weight. All respondents were offered an additional US$50 to participate in the biomarker phase of the study. As a result, nearly all respondents agreed to participate in the biomarker collection (less than 2% refused). Due to the complexity of the NSAHS study design, data collection lasted nearly 3 years (April 2011 to January 2014).
Measurement
AL
AL has been defined by Crimmins, Johnston, Hayward, and Seeman (2003) as an index “of the physiological challenge currently experienced by an organism with multiple complex systems which interact to produce health outcome” (p. 731). AL is measured using 10 indicators that reflect the system-wide toll taken on the body due to repeated activations of the bodies’ stress response system. Consistent with the recommendations of the MacArthur Aging Study Allostatic Load Working Group, we measure AL as consisting of primary and secondary mediators where the former represent potential hypothalamus–pituitary–adrenal axis (HPA) and sympathetic-adrenomedullary (SAM) dysregulation and the latter represent dysregulation of the cardiovascular and metabolic systems (http://www.macses.ucsf.edu/research/allostatic/allostatic.php). The 12-hr urine samples were collected and assayed to give four indicators of primary mediators (cortisol, epinephrine, norepinephrine, and dehydroepiandrosterone). Blood pressure, anthropomorphic indicators, and venipuncture blood samples were taken and utilized to give six indicators of secondary mediators: systolic and diastolic blood pressures, total cholesterol, high-density lipids (HDL), glycated hemoglobin, and waist-to-hip ratio. The participant’s blood pressure was the average blood pressure taken 3 times in 2 min intervals. AL is estimated by a count of the number of dimensions with scores falling above the 75th percentile in our sample, except for HDL and Dehydroepiandrosterone (DHEA-S), where the lowest quartile corresponds to highest risk. The means and standard deviations of each measure that comprises this scale are presented in Appendix A.
Chronic health conditions
The number of chronic conditions in this study is utilized as an alternative health outcome. Its inclusion allows us to test to what extent it is associated with mattering and to highlight the utility in incorporating AL as our primary outcome. Study participants reported lifetime and past-year occurrences of 27 potential diseases and disorders. Consideration of these conditions was limited to those disorders that included a yes response to, “Was this health problem diagnosed by a physician?” In the analyses to be presented, “doctor-diagnosed health” was a lifetime count of the number of reported disorders. Study participants reported a mean of 2.76 chronic conditions. This measure ranged from zero to 13.
Mattering
Mattering is assessed by a five-item index designed by Morris Rosenberg that was first validated in a community study in Toronto, Canada (Taylor & Turner, 2001). This measure (α = .75) is a standardized count of the following items: (a) “How important do you feel you are to other people?” (b) “How much do you feel other people pay attention to you?” (c) “How much do you feel others would miss you if you went away?” (d) “How interested are people generally in what you say?” and (e) “How much do other people depend on you?” Responses range from “not at all” to “a lot,” and are coded so that higher values reflect a greater sense of mattering. Mattering is thought to be conceptually and empirically distinct from other socially based resources, such as social support. Taylor and Turner (2001) conducted factor analyses to test the empirical distinctiveness mattering had from social support and found that while there was some empirical overlap between measures of mattering and social support from friends and spouse, this empirical redundancy was largely limited to male study respondents. Additional analyses showed that mattering was distinct from social support from family and coworkers. Lewis and Taylor (2009) conducted a similar analysis with data from a sample of South Floridians and found no evidence of empirical confounding between mattering and social support.
Age
Age is a continuous variable ranging from 22 to 69 years.
Control variables
Given the well-established variation among African Americans and Whites with respect to parental status, marital status, and employment status, coupled with evidence that these statuses are positively associated with perceptions of mattering (Schieman & Taylor, 2001), we control for these social statuses. We also control for gender (female = 1). Race is comprised of three dummy coded variables for White (n = 521), African American (n = 491), and members of other racial/ethnic groups (n = 14). Educational attainment was measured with two dichotomous indicators that reflect whether the respondent completed some college (1 = some college, 0 = no college) or a college degree (1 = college degree; 0 = no college degree) based off an item that asked about the highest grade of school the respondent completed successfully. Household income was obtained across 15 categories ranging from less than US$5,000 to more than US$135,000 per year. Parental status is a count of the number of children reared. Marital status is a three-category dummy variable consisting of currently married, currently cohabitating, and single. Current employment status is a three-category variable consisting of full-time employment (62%), part-time employment (32%), and retired (5%). Frequency of religious attendance is an ordinal variable that reflects how often the respondent reported attending religious services with responses ranging from 0 (never) to 6 (every week or more).
Additional variables
Physical activity was using a shortened version of the International Physical Activity Questionnaire (Craig et al., 2003) that asked about moderate and vigorous physical activity. It was expressed as overall energy expenditure in metabolic equivalent total minutes per week. Former smokers = 1. Frequency of drinking alcohol measured past-year behaviors ranging from 0 = never to 4 = almost every day. Separate eight-item scales measured family and friends social support. Measurement included the following items: “You feel close to your family”; and “You have family who would always take the time to talk over your problems should you want to.” The alphas for family and friend social support are .91 and .95. Chronic strains are measured by a six-item inventory developed using the logic and items of Wheaton’s (1994) previously developed measure.
Analytical Strategy
We began by examining the associations between sense of mattering and both AL and number of chronic conditions using one-way ANOVA tests. Next, we investigated how sense of mattering is associated AL and number of chronic conditions using multivariate modeling. The first set of models establishes the association between mattering and both outcome measures after adjusting for basic demographic controls. The second adds the full set of controls into the model. The third tests whether the association between mattering and our outcomes varies by age by including an interaction term to assess whether mattering moderates the relationship between age and AL. We estimated all models with Poisson regression. Incident rate ratios (IRR) are presented throughout. The IRR coefficients can be interpreted as a unit increase in the independent variable produces a percentage change in the expected count. For example, for all variables, coefficients above 1 produce a (β – 1) × 100 percentage increase in the expected count, whereas coefficients below 1 produce a (1 – β) × 100 percentage decrease in the expected count.
We performed several ancillary analyses using different model specifications and different modeling techniques. First, we replicated all findings using a negative binomial regression that produced the same substantive findings as presented here. Moreover, we conducted log likelihood ratio tests comparing the Poisson and negative binomial models that showed that the latter models did not fit the data better than the former. Second, we replicated all findings pertaining to the AL analysis by counting those who reported taking medications for cholesterol as having high total cholesterol, and those taking blood pressure medication as having high systolic blood pressure. This analysis yielded results similar to those presented below. Third, we reanalyzed the data by including all individuals with at least five valid AL indicators, which increased the valid sample size to 1,157. This set of analyses indicated that our reported results were not sensitive to our choice to only include individuals who had valid indicators for all AL items. Finally, we tested whether mattering makes an independent contribution in the prediction of AL after adjusting the model for social support.
We also tested the robustness of our results regarding the interaction effect between sense of mattering and age in three ways. This is important because interpreting interaction effects is not straightforward with Poisson regression as the nature of the interaction, as well as statistical significance, can vary by the levels of the other covariates in the model (Buis, 2010). First, we tested for interaction effects with the Poisson model when other covariates were not included in the model. Second, we tested for interaction effects using ordinary least squares regression, which is not subject to this issue. Finally, we re-ran our tests for interaction effects numerous times for different values of the other covariates in the full model and interpreted each. These ancillary analyses all yielded results that mirror the pattern of findings as presented below.
Results
Table 1 presents mean AL scores across age categories by the variables mattering, gender, race, and educational attainment. The values presented at the top of the table provide some evidence that perceptions of mattering may moderate the positive relationship between age and AL. AL scores are shown to increase with age, but these increases vary by level of mattering. For example, for those study participants who are one standard deviation below the mean for mattering, the value of AL is twice as large in the oldest age category compared with those aged 22 to 35 years (3.54 compared with 1.70). Increases in AL for those in the medium and high categories of mattering are much less dramatic. Scores increase from 1.93 to 2.80 for those in the medium category and from 2.12 to 2.76 for those at one standard deviation above the mean. Part of the reason for this variation in the magnitude of increases of AL is because of the anomalous pattern of findings presented among 22- to 35-year-olds. In contrast with those in the older age categories, AL is positively related to mattering. For those aged 36 and older, AL is inversely related to mattering. The pattern of AL scores presented in the remainder of the table conforms to those reported in previous studies. AL increases with age and is higher for men compared with women, Blacks compared with Whites, and is inversely associated with educational attainment.
Social Status Variation Mean Allostatic Load Scores by Age Category (Standard Deviations) (N = 1,026).

Note. Level of allostatic load varies by gender, race, and education based on one-way ANOVAs within each age category.
Only 14 respondents identified as being non-Black or non-White. These age ranges were chosen so that there would be a sufficient number of cases within each category.
p = .029 based on one-way ANOVAs within age category.
In Table 2, AL (Models 1-3) and number of chronic health conditions (Models 4-6) are regressed on the variables of interest. The IRR presented in Model 1 of Table 2 are consistent with descriptive analyses presented above. Mattering shares a modest negative association with AL as a one-unit increase in mattering is associated with approximately an 8% drop in the expected AL count. AL is also shown to vary by age, gender, race, and education. Model 2 shows that the IRR for mattering is no longer statistically significant after including additional covariates in the model.
Multivariate Models From Poisson Regressions (N = 1,026).
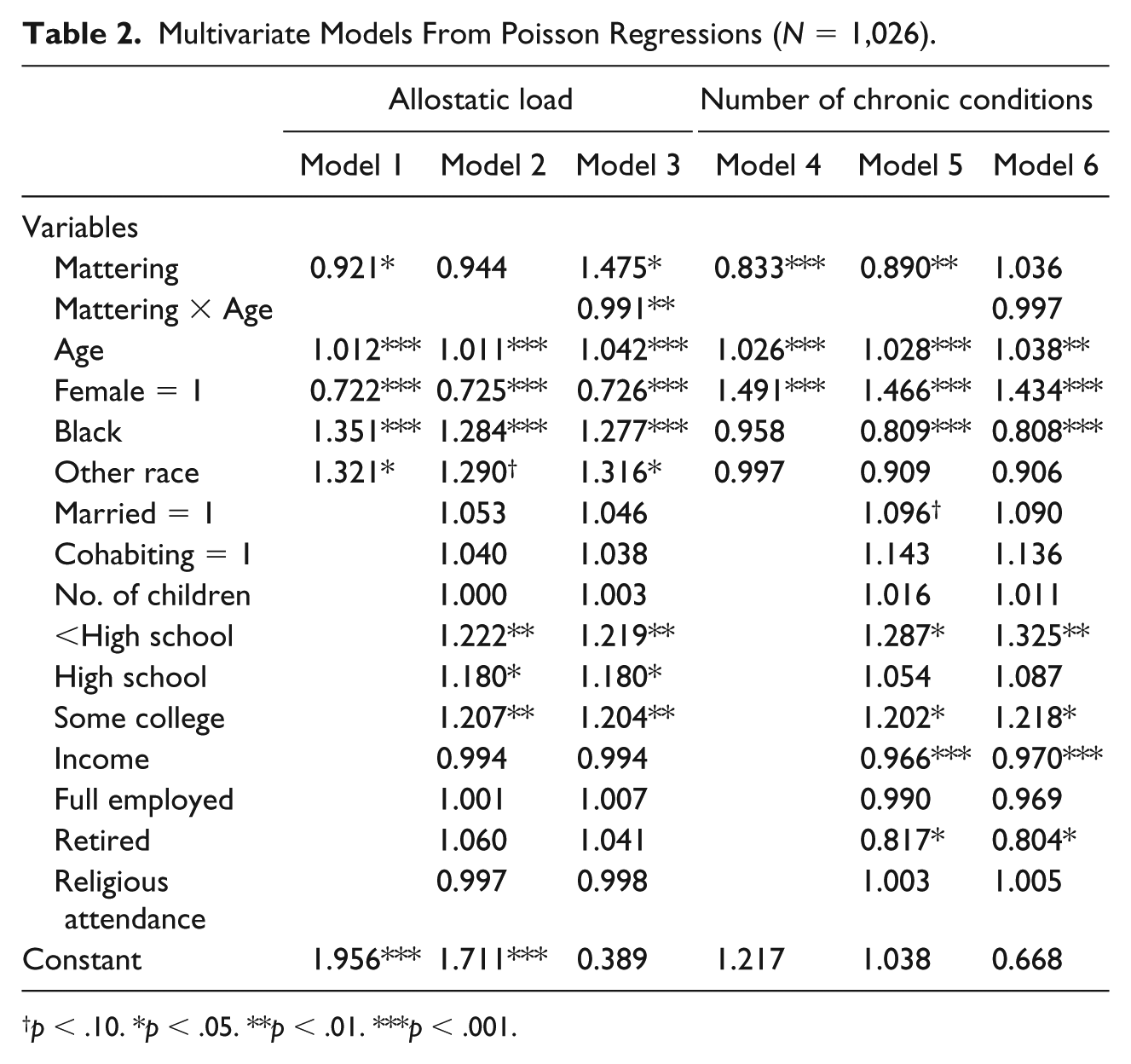
p < .10. *p < .05. **p < .01. ***p < .001.
A mattering by age interaction term is presented in Model 3. Product term interaction models were computed to assess whether regression slopes for age varies by level of mattering. The interaction term supports the hypothesis that mattering conditions the relationship between age and AL. AL increases with age, but these increases are largely limited to those study participants who report lower levels of mattering. Mattering by age regression slopes are displayed in Figure 1. They indicate that AL increases with age, but this increase is limited to study participants with mean or below mean levels of mattering. In contrast, the regression slope for respondents with mattering scores at one standard deviation above the mean is relatively flat. It is also noteworthy that a crossover is observed at about age 40. This is consistent with the information presented in Table 1 where higher levels of AL were observed at lower levels of mattering.

Mattering by Age Regression Slopes.
As a check of the robustness of the relationships reported here, we added an additional equation to the Model 3 analysis that included covariates for health behaviors, two forms of social support, and chronic stressors (Model 4 of Appendix B). The addition of these variables did not alter the relationships reported in Model 3.
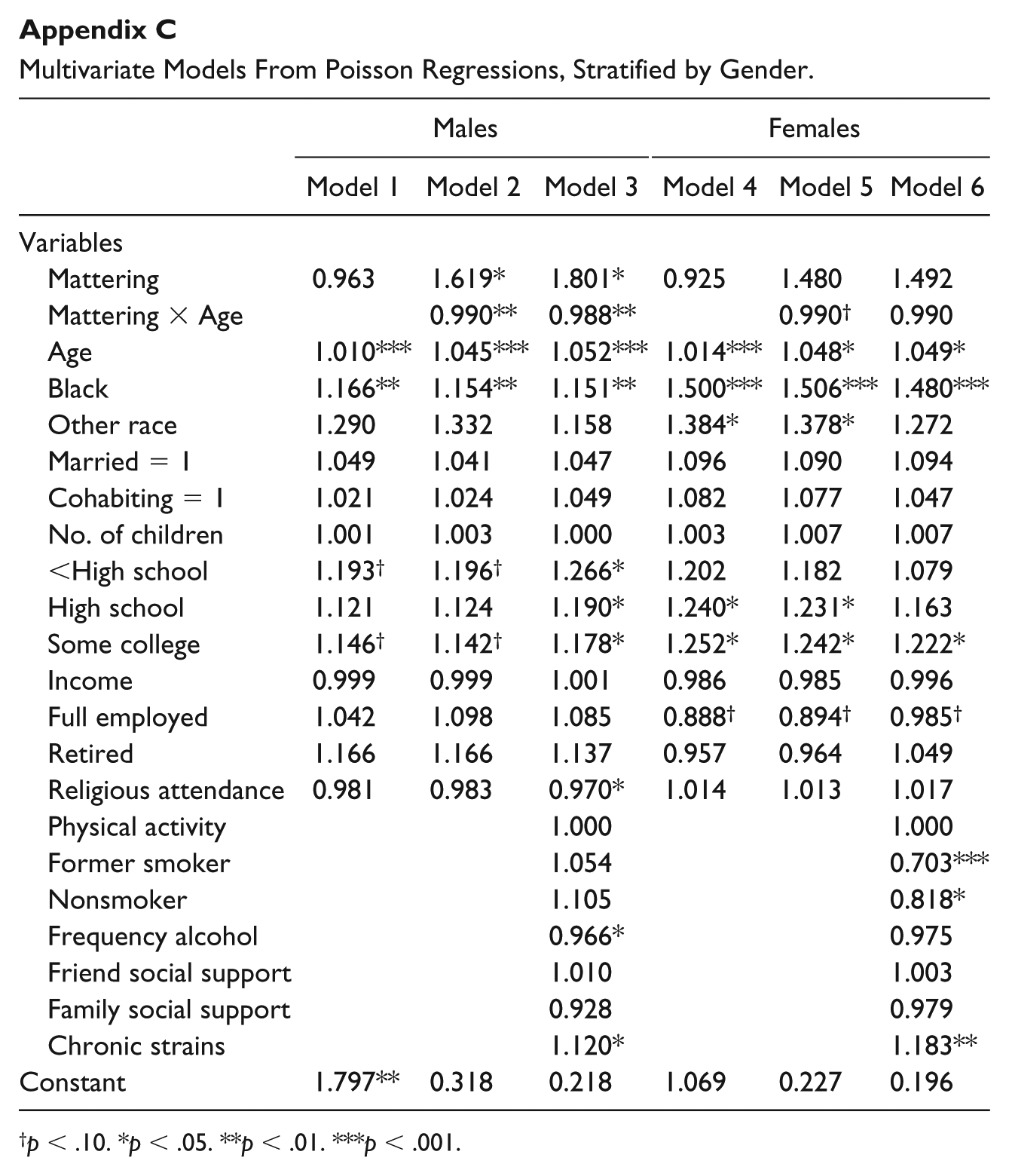
Because past studies have shown that mattering and AL vary by gender, we replicated regression Models 1 to 3 separately for men and women (Appendix C). Significant mattering by age coefficients were again observed for men (Models 2 and 3), but not for women. The interaction term presented in Model 5 was marginally significant, but this was no longer the case when additional covariates were added in Model 6. These contrasts were unexpected, given that women tend to report higher levels of mattering compared with men and that the health benefits of mattering tend to be greater for women compared with men.
In Models 4 through 6, number of chronic health conditions was regressed on the variables of interest in a parallel analysis to those presented in Equations 1 to 3. These analyses were conducted to see whether we could replicate the buffering relationship illustrated in Figure 1. We could not. As expected, mattering is protective for physical health (Models 4 and 5), but it does not moderate the positive relationship between age and health conditions (Model 6).
Discussion
This article adds to a growing body of evidence documenting the role and significance that relationships play in shaping healthy aging. The primary objective of this article was to test the hypothesis that mattering buffers the relationship between age and AL. Our test of this hypothesis was supported. The significant age by mattering interaction term confirmed that AL increases with age and this increase is significantly greater among those with moderate or low perceptions of mattering to others. Another finding of note was the age crossover, at about age 40, in the mattering by age regression slopes. Although prior research has produced inconsistent findings with respect to age distributions of AL, most show steady increases from early adulthood through late middle age (Crimmins et al., 2003; Geronimus, Hicken, Keene, & Bound, 2006). The fact that a similar pattern was observed only among those study participants at mean or below mean levels of mattering suggests two things. First, the protective effects of mattering are less evident at earlier ages. This is most likely due to the fact that population differences physiological wear and tear do usually not emerge until later in life. Second, the extent to which people perceive how much they matter to others is particularly salient as it relates to physical health processes.
The present research adds to a growing base of evidence that suggests positive intimate relationships act as mechanisms that modify biological pathways associated with disease. For instance, social support, a key factor associated with one’s perception of mattering, is associated with regulation of immune function, including inflammation, which is related to a range of chronic conditions including heart disease (Cohen, Doyle, Skoner, Rabin, & Gwaltney, 1997).
Most prior research on social relationships and health has focused on social support. In contrast, there is a relatively small body of work that has looked at the protective aspects of mattering to others. There is reason to believe that mattering may be a better predictor of health and well-being than other conceptualizations of social relationships. Because mattering and social support are both anchored in perceptions of close personal ties, they undoubtedly share some theoretical and empirical ground. However, we believe that these two constructs are conceptually and empirically distinct. We base this assessment on several considerations. First, our data show only modest associations between mattering and social support (.401 for friend support and .312 for family support). Second, there are several different domains of social support including informational, instrumental, emotional, and structural, and the effects of each are likely to differentially influence health and well-being in later life, particularly in relation to the way they shape stress processes over the life course. Moreover, individuals evaluate their social support differently based on the source of support among different network members—spouse, family, friends, and coworkers—some of which is beneficial and some of which may be harmful. For instance, using data from the Midlife in the United States (MIDUS) Study, Brooks and colleagues (2014) explored how several sources of social support were related to AL. Their analyses produced mixed results with respect to the protective effects of social support. Family support was unrelated to AL and a higher level of friend support was positively related to AL, but only among older adults. They also found that network support was associated with lower AL at younger ages and higher AL at older ages. Finally, they found that more frequent contact with friends and family was associated with higher AL. These set of findings contrast rather strongly with the analyses presented here.
Mattering captures the net effect of all domains of social support, and the net effect of all sources of support in an individuals’ life. Many individuals may report high levels of social support, but that support may not lead them to feel connected in a meaningful way, subsequently leading to lower levels of mattering. These processes may relate to the fact that some sources of support are achieved while others are ascribed. This is because individuals usually have little control in selecting coworkers or family, and relationships with these sources of social support can often be harmful as well as beneficial.
In contrast to most conceptualization of social support, mattering captures more global perceptions of one’s relationships with significant others. For example, none of the items measuring mattering are anchored to specific others. Instead, respondents are asked about their general impressions of how important they are to the people in their lives. Because of this, past research has failed to identify the negative effects of mattering. Rosenberg and McCullough (1981) emphasized this long ago when he wrote, When others depend upon us, worry about us, expect things from us, we are constrained and inhibited by these expectations. The person who infers that he is significant may consciously experience this burden as a burden and a constraint; but the unhappy person is the one who is free of the burden. (p. 179)
Alternatively, when a son or daughter is disciplined, the child may be unhappy with her punishment, but the punishment may also convey information that others are concerned and care about her. The obverse of mattering is being inconsequential or insignificant, but these circumstances are probably not the result of having negative interactions with others.
There are three limitations in this study worth noting. First, because this project employed a cross-sectional study design, it was not possible to distinguish age versus cohort effects. We also lacked the ability to establish temporal ordering between mattering and our dependent variables. It is likely that these relationships are bidirectional and play out in complex ways over the life course. For instance, declines in health that are associated with increased AL may compromise one’s ability to maintain important social roles and relationships that underlie perceptions of mattering. We also know that the quality and structures of relationships have an influence on health behaviors and psychological processes. Having relationships with people who exercise and eat well increases the likelihood of following suit (Antonucci et al., 2014). A second limitation of this research was that it was limited to study participants who resided in Davidson County, Tennessee. It is therefore possible that the findings presented here do not generalize to other geographic areas. Finally, we were unable to look at adults over age 70, as our sample was limited such that the oldest participants were in their late 60s. Future studies would benefit from exploring whether our age-related findings persist among adults in later stages of old age.
Despite these limitations, this study makes several contributions that could have important implications. As noted by Holt-Lunstad and colleagues (2010), social relationships are as influential to health as other health behaviors such as smoking and exercising. Our findings suggest that mattering may provide a robust measure of the quality and nature of these relationships, and future research should consider the extent to which it is possible to cultivate a stronger sense of mattering to bolster health and well-being over the life course.
Currently, there are few interventions designed to modify social relationships, particularly among those in later life, but there is an evidence that suggests that social health interventions could play an important role (Cohen & Gottlieb, 2000). One area that may be particularly fruitful to consider is the potential role of volunteer interventions. Volunteering typically involves engaging in an activity with others that is meaningful, which often cultivates one’s sense of purpose. It is plausible that such activities could facilitate development of broader social support networks and also enhance one’s feeling of mattering to others. Alongside observational studies showing health benefits attributed to becoming a volunteer (e.g., Carr, Kail, & Rowe, 2018), the few volunteer interventions that have been completed such as the well-known Baltimore Experience Corps Trials (Fried, Carlson, Freedman, et al., 2004) suggest volunteering leads to enhancement of physical health. These findings may well be attributed, in part, to enhanced sense of mattering. In fact, a recent study by Thoits (2012) lends strong support to this claim. She found that mattering was part of a social process linking the salience of volunteering to increases in perceptions of purpose and meaning, which in turn, was linked to positive well-being. Future research linking health interventions that focus on meaningful social interactions, like volunteering, should consider the role of enhanced perceptions of mattering as a key factor.
Ideally, future research should employ prospective longitudinal study designs to assess age trajectories in the relationship between mattering and the biological risks that precede the onset of illness. Doing so is important because it could provide information about the direction of the relationship between mattering and AL as well as the stability of this self-perception across the life course. It could also help to identify the broader social forces and arrangements that foster a sense of mattering to others. Future studies should also consider gender differences in the role of mattering in health. As noted above, our findings suggest that mattering was more beneficial for men compared with women. Understanding the social dynamics that underlie this contrast is not yet understood. Such information is crucial for identifying strategies designed to improve successful aging. We therefore encourage scholars to continue work on this important topic.
Footnotes
Appendix
Multivariate Models From Poisson Regressions, Stratified by Gender.
| Males |
Females |
|||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |
| Variables | ||||||
| Mattering | 0.963 | 1.619* | 1.801* | 0.925 | 1.480 | 1.492 |
| Mattering × Age | 0.990** | 0.988** | 0.990 † | 0.990 | ||
| Age | 1.010*** | 1.045*** | 1.052*** | 1.014*** | 1.048* | 1.049* |
| Black | 1.166** | 1.154** | 1.151** | 1.500*** | 1.506*** | 1.480*** |
| Other race | 1.290 | 1.332 | 1.158 | 1.384* | 1.378* | 1.272 |
| Married = 1 | 1.049 | 1.041 | 1.047 | 1.096 | 1.090 | 1.094 |
| Cohabiting = 1 | 1.021 | 1.024 | 1.049 | 1.082 | 1.077 | 1.047 |
| No. of children | 1.001 | 1.003 | 1.000 | 1.003 | 1.007 | 1.007 |
| <High school | 1.193 † | 1.196 † | 1.266* | 1.202 | 1.182 | 1.079 |
| High school | 1.121 | 1.124 | 1.190* | 1.240* | 1.231* | 1.163 |
| Some college | 1.146 † | 1.142 † | 1.178* | 1.252* | 1.242* | 1.222* |
| Income | 0.999 | 0.999 | 1.001 | 0.986 | 0.985 | 0.996 |
| Full employed | 1.042 | 1.098 | 1.085 | 0.888 † | 0.894 † | 0.985 † |
| Retired | 1.166 | 1.166 | 1.137 | 0.957 | 0.964 | 1.049 |
| Religious attendance | 0.981 | 0.983 | 0.970* | 1.014 | 1.013 | 1.017 |
| Physical activity | 1.000 | 1.000 | ||||
| Former smoker | 1.054 | 0.703*** | ||||
| Nonsmoker | 1.105 | 0.818* | ||||
| Frequency alcohol | 0.966* | 0.975 | ||||
| Friend social support | 1.010 | 1.003 | ||||
| Family social support | 0.928 | 0.979 | ||||
| Chronic strains | 1.120* | 1.183** | ||||
| Constant | 1.797** | 0.318 | 0.218 | 1.069 | 0.227 | 0.196 |
p < .10. *p < .05. **p < .01. ***p < .001.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant (R01AG034067) from the Office of Behavioral and Social Science Research and the National Institute on Aging to R. Jay Turner.