
Abstract
Introduction
In general, racial and ethnic minorities experience more functional limitation and disability, compared with their White peers (Haas & Rohlfsen, 2010; Haas, Krueger, & Rohlfsen, 2012; Thorpe et al., 2011; Warner & Brown, 2011). Even after controlling for socioeconomic status, most research demonstrates functional health disparities among minority older adults (Haas et al., 2012; Thorpe et al., 2011). However, research investigating recovery from functional limitation, more specifically mobility limitation, has documented increased odds of recovery following onset of limitation among racial and ethnic minorities, net of socioeconomic status (Latham & Clarke, 2013; Latham, Clarke, & Pavela, 2015; Latham & Williams, 2015).
Using nationally representative datasets, current research suggests that racial and ethnic minorities experience increased onset of mobility limitation and recovery from mobility limitation. Yet, it is unclear whether this finding reflects differences in patterns of recovery. In other words, racial and ethnic minorities may experience more transitions in and out of impairment, but still experience worsening functional health as this episodic recovery is not related to improved health. Alternatively, these increased rates of recovery may be indicative of physical resilience in mid- and later-life. One way to test this hypothesis is to examine recovery maintenance among a group of older adults who have experienced at least one episode of recovery.
Recovery from mobility limitation may serve as a turning point in an older adults’ functional health trajectory. Prior research has observed lower odds of death and disability following recovery from mobility limitation (Latham, 2018). Yet, few studies have explored various patterns of recovery. This research examines whether racial and ethnic minorities experience less recovery maintenance (i.e., maintaining their recovery status 2 years later), compared with their White peers. This research uniquely contributes to our current understanding of recovery by examining what happens after older adults experience recovery. Instead of looking at one recovery episode in isolation, this research follows a group of older adults for an additional 2 years to see who is still recovered from their previous mobility limitation. Using the concept of recovery maintenance, this research will expand our knowledge about the processes related to onset and recovery and potentially speak to clinical and community interventions.
Minority Aging and Mobility Limitation
The extant literature demonstrates clear disparities in functional health among older racial and ethnic minorities (i.e., non-Hispanic Black and Hispanic/Latinx adults; Thorpe et al., 2011; Warner & Brown, 2011). These disparities reflect the realities of minority aging within the United States, where racial and ethnic minorities often have fewer social and economic resources and experience chronic discrimination (Williams, 2005). Moreover, racial and ethnic minorities are exposed to more health-detracting risk factors across the life course, which increases their risk of chronic conditions and subsequent disability (Bowen, 2009; Brown & Turner, 2010). For example, due to segregation, racial and ethnic minorities are more likely to live in divested neighborhoods, which exposes them to hazardous home and work environments (Williams & Sternthal, 2010). Not only are racial and ethnic minorities more at risk of poor health in the United States, access to health care, particularly high quality health care, varies by race and ethnicity (Penner, Blair, Albrecht, & Dovidio, 2014; Purnell et al., 2016). Racial and ethnic minorities face unique barriers to health care that contributes to their (in)ability to manage chronic conditions (Bowen & González, 2008). These structural inequalities contribute to worse functional health among older racial and ethnic minorities at various stages of the disablement process including mobility limitation.
Mobility limitation, defined as difficulty walking and/or climbing stairs, is the most common type of functional limitation among older adults (Okoro, Hollis, Cyrus, & Griffin-Blake, 2018). Mobility limitation is related to lower body functioning and is a robust predictor of more serious health outcomes such as activities of daily living (ADL) disability (i.e., self-care disability), mortality, or restricted social engagement (Alexander et al., 2000; Rosso, Taylor, Tabb, & Michael, 2013). According Verbrugge and Jette (1994), mobility limitation can be conceptualized as specific type of functional limitation, which represents an earlier stage of the disablement process. Functional limitations are “restrictions in basic physical and mental actions” and are often the building blocks for disability or “difficulty doing activities of daily life” (Verbrugge & Jette, 1994, p. 4). To illustrate, difficulty walking may restrict activities (particularly in demanding environments) related to self-care or participation in social life. Because mobility limitation represents an earlier stage of the disablement process among older adults, it is quite possible that interventions aimed at addressing mobility limitation may prevent subsequent disability onset.
Racial and ethnic minorities report more mobility limitation over their life course, compared with their White peers (Okoro et al., 2018). In addition, racial and ethnic minorities have a higher prevalence of ADL disability (i.e., self-care disability) in mid- and late-life (Courtney-Long et al., 2015; Okoro et al., 2018). Although the extant literature characterizes racial and ethnic minorities as having worse functional health across multiple measures of physical functioning, longitudinal data highlight some important differences in the onset and progression of mobility limitation and disability among older minorities. For example, Vásquez and colleagues (2018) found that older Hispanic adults had lower odds of mobility limitation after controlling for sociodemographic characteristics, whereas non-Hispanic Blacks did not significantly differ from Whites after controlling for sociodemographic characteristics and comorbidities. Yet, both Hispanic and non-Hispanic Blacks had higher odds of ADL disability, net of sociodemographic characteristics and comorbidities (Vásquez et al., 2018). Likewise, Shumway-Cook, Ciol, Yorkston, Hoffman, and Chan (2005) found no significant differences in the progression of mobility limitation by race.
Although previous research clearly demonstrates important racial and ethnic disparities in functional health, there are important differences between mobility limitation and ADL disability. It appears that racial and ethnic minorities may be less likely to have mobility limitation after controlling for key socioeconomic and health factors, whereas most research consistently shows ADL disability disparities among older minorities, net of socioeconomic factors. This implies that mobility limitation, relative to ADL disability, may be more sensitive to interventions among older minorities.
Recovery and Physical Resilience Among Older Adults
Prior research has documented variation in recovery patterns among older racial and ethnic minorities. For example, Latham-Mintus and Aman (2017) explicitly investigated recovery from mobility limitation, and documented higher odds of recovery among racial and ethnic minorities, net of socioeconomic status. Within the context of the disablement process, it is important to probe whether these differences in mobility onset and recovery signal meaningful improvement in functional health among older racial and ethnic minorities.
According to Resnick, Galik, Dorsey, Scheve, and Gutkin (2011), “[p]hysical resilience is the ability to recover or optimize function in the face of age-related losses or disease” (p. 644). Although multiple definitions and measures of resilience have been used in the literature, physical resilience is thought to stem from adaptations to physiological challenges such as chronic disease or impairment. Resilience has been linked to increased optimism, mastery/self-efficacy, perseverance, determination, tenacity, fewer negative emotions, and more active engagement in disease management (Becker & Newsom, 2005; Felten, 2000; Resnick et al., 2011), which are all vital for recovery. Among racial and ethnic minorities experiencing serious illness or disability, qualitative research has outlined how prior hardships due to racism and discrimination enable older racial and ethnic minorities to be resilient in the face of health concerns (Becker & Newsom, 2005; Felten, 2000). To illustrate, Felten (2000) states “As a result of facing hardship earlier in their lives, [minority women] grew stronger and were able to cope better with devastation in later life” (p. 118).
Given the systemic racism and discrimination experienced by racial and ethnic minorities in the United States (Williams, 2005), recovery from mobility limitation may be a form of physical resilience. However, it is possible that the increased rates of recovery from mobility limitation among racial and ethnic minorities may represent variation in reporting patterns (Melzer, Lan, Tom, Deeg, & Guralnik, 2004). Racial and ethnic minorities may have episodic recovery, where they move in and out of mobility limitation more often than their White peers. The objective of this research is to examine whether the increased rates of recovery from mobility limitation among racial and ethnic minorities have a lasting influence on their functional health. To accomplish this objective, I use the concept of recovery maintenance, which I define as continued improvement in functional health following onset. If racial and ethnic minorities experience more episodic recovery, then one would expect to see variation in recovery maintenance by race and ethnicity. Otherwise, a lack of significant variation in recovery maintenance would suggest that recovery indicates meaningful changes in functional health trajectories among racial and ethnic minorities. To further investigate this claim, a secondary set of analyses were completed to examine whether recovery maintenance predicts ADL disability onset, and whether the effect of recovery maintenance on ADL disability onset varies by race and ethnicity.
This research contributes to the literature by taking a closer look at mobility limitation onset and recovery among racial and ethnic minorities within the context of the disablement process. Moreover, this research aims to expand our knowledge of minority aging as it relates to physical resilience and recovery. In doing so, this research may speak to important individual- and community-level interventions that may slow or reverse the disablement process.
Method
Data
Data come from the Health and Retirement Study (HRS), which is an ongoing panel study of Americans (and their spouses) older than the age of 50 years. Data are collected every 2 years. The HRS has an oversampling of racial and ethnic minorities and detailed health information making it well suited for this analysis (Health and Retirement Study, 2016). To aid in data management, the most recent version of the RAND HRS datafile (Version P) was employed. The RAND HRS datafile is a harmonized, user-friendly version of the most commonly used HRS variables (RAND, 2018). The HRS started data collection in 1992, but did not become representative of all noninstitutionalized Americans older than the age of 50 years until 1998. Therefore, I used Wave 4 (1998) through Wave 12 (2014) for these analyses.
Main Sample
Because I am interested in recovery maintenance, I first identified our risk group of older adults who have experienced recovery. To complete this objective, I used two waves to establish recovery from mobility limitation. To illustrate using the first two waves, I identified all respondents with at least one mobility limitation (i.e., difficulty walking or climbing stairs) in 1998. Next, I assessed whether these respondents experienced recovery (i.e., no mobility limitation) in the subsequent wave (2000). This group of respondents who had mobility limitation and then experienced recovery in two adjoining waves comprises the risk group. Following establishing the risk group of respondents with recovery, I then assessed their recovery status in the ensuing wave (2002) (see Figure 1). The proportion of the full sample that matches the risk group criteria is relatively small for any given wave; therefore, I created multiple risk groups using all the available waves and pooled the analysis, while controlling for the baseline entry wave. This approach increased statistical power by enabling older adults with newly acquired mobility limitation (or newly added HRS respondents) to be included in the analyses. The final analytic sample of age-eligible respondent with valid data was 9,378 person-intervals.
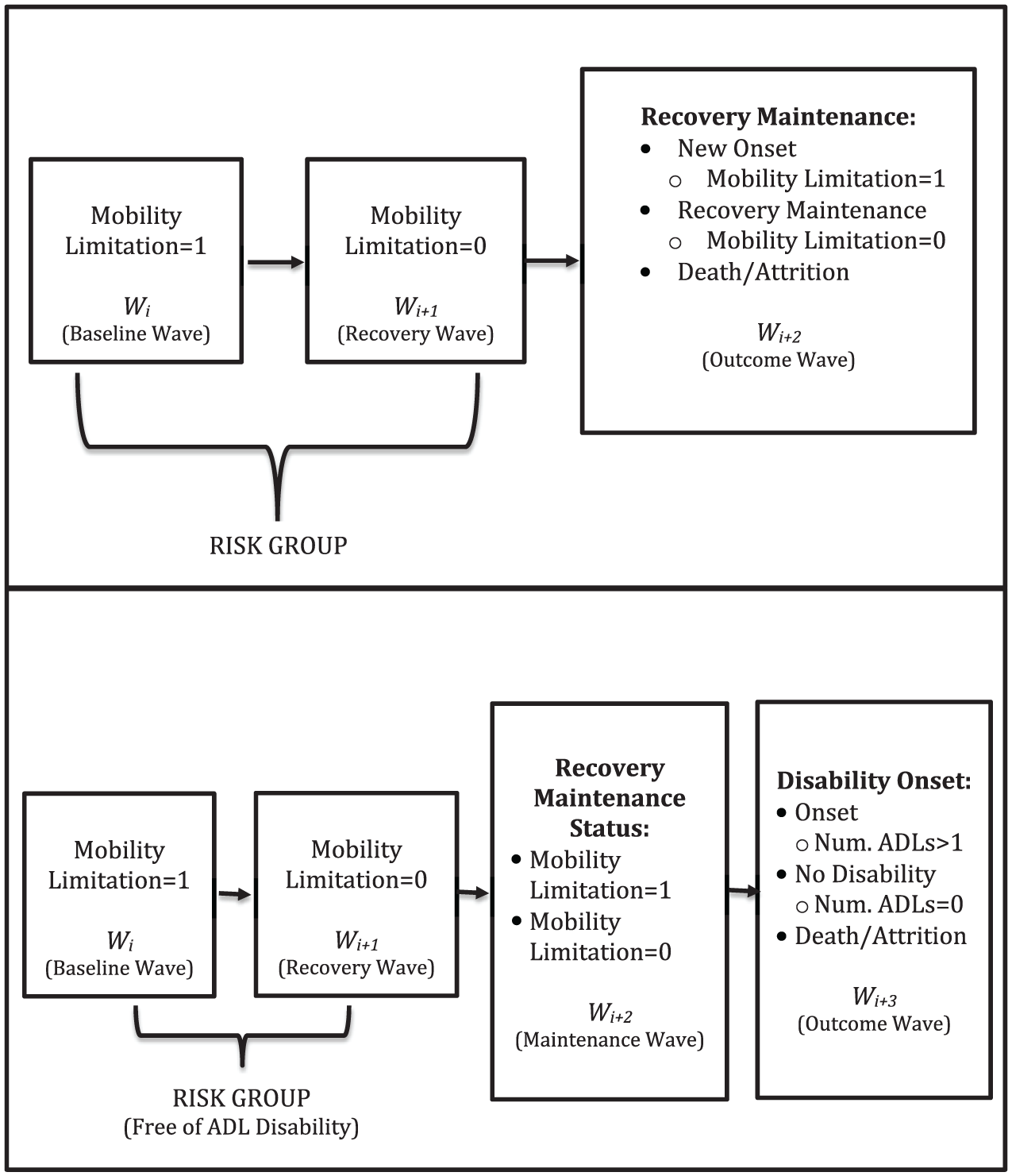
Illustration of risk group and outcomes for recovery maintenance analytic samples.
Subsample
An additional objective of this research is to understand the relationship between recovery maintenance and ADL disability among racial and ethnic minorities. To accomplish this objective, a subsample was created to examine whether recovery maintenance was associated with lower odds of ADL disability, and whether this association varied by race and ethnicity. The subsample comprised respondents who had experienced recovery maintenance. The initial risk group included respondents with mobility limitation, but free of ADL disability at baseline. I used two adjoining waves to establish recovery maintenance. Respondents needed to be alive and have valid information for three adjoining waves to be included in the subsample (see Figure 1). Respondents who had mobility limitation at baseline, but were free of mobility limitation the following two waves were classified as having recovery maintenance = 1. The dependent variable for this set of analyses was onset of ADL disability. The final analytic sample size for this subsample was 6,359 person-intervals.
Measures
The main dependent variable was recovery maintenance (or remaining free of mobility limitation). Mobility limitation was measured using an index from the RAND HRS datafile. Five mobility indicators were used: (a) difficulty walking several blocks, (b) difficulty walking one block, (c) difficulty walking across the room, (d) difficulty climbing several flights of stairs, and (e) difficulty climbing one flight of stairs. Respondents reporting any difficulty were categorized as having “mobility limitation” = 1. Respondents who had mobility limitation at baseline (i.e., Wi) and reported no mobility limitation in the subsequent wave (Wi + 1) were classified as having experienced recovery and entered into the risk group. Recovery maintenance was then assessed in the following wave (Wi + 2) using a respondent’s current mobility limitation status (i.e., free of mobility limitation or newly acquired mobility limitation). A categorical variable was created, where (a) recovery maintenance, (b) new onset of mobility limitation (reference), and (c) death/attrition were the categories.
A secondary dependent variable was used to assess the relationship between recovery maintenance and ADL disability onset. Respondents were asked about five common ADL disability tasks: (a) difficulty walking across the room, (b) difficulty eating, (c) difficulty bathing, (d) difficulty getting in/out of bed, and (e) difficulty dressing. Respondents reporting difficulty with at least one ADL task in the outcome wave (Wi + 3) were classified as having disability onset. A three-category variable was created where (a) free of disability (reference), disability onset, and died/attrited were the categories. The mobility limitation index and ADL index from the RAND HRS datafiles both use difficulty walking across the room as an item; however, one of the criteria for the subsample risk group was to be free of ADL disability—meaning that none of the respondents in the subsample risk group reported difficulty walking across the room.
The independent variable of interest was race and ethnicity. A four-category variable was created using the race and ethnicity variables, where non-Hispanic White (reference), non-Hispanic Black, Hispanic/Latinx, and other race were the categories.
Sociodemographic characteristics (age, sex, and marital/partner status), socioeconomic status (education, work status, and logged income), and health risk factors (self-rated health, number of chronic conditions, obesity, and smoking status) were included in the analysis as controls. All control variables were measured at baseline or the initial wave of mobility limitation (see Figure 1). Age was measured in years. A dichotomous variable was created for sex, where female = 1. Similarly, a dichotomous indicator was created for marital/partner status, where married or partnered = 1. Socioeconomic status was captured using three measures. A categorical measure of education was created based on degree with “no high school degree,” high school degree or equivalent, some college, and college degree as the categories. High school degree served as the reference category. Regardless of the hours worked, respondents who reported working for pay were classified as “working for pay” = 1. The total household income variable was transformed to address skewness. Households reporting zero income were defined as “0,” and all other incomes were logged.
Because health care access contributes to racial and ethnic health disparities including progression of disability (Bowen & González, 2008), a measure of health insurance status was included in the analyses. A three-category variable was created with private health insurance (from either respondent or spouse), public health insurance (e.g., Medicare), and no health insurance as the categories. The public health insurance category included respondents with only public health insurance. Respondents who reported a combination of private and public health insurance were classified as having “private insurance.” Health insurance coverage was measured at baseline, and private insurance was used as the reference category.
Health risk factors included two indicators of morbidity: (a) poor/fair health and (b) number of chronic conditions. Respondents were asked to rate their health from excellent to poor. In line with previous research, the response categories for self-rated health were collapsed into poor/fair health versus good/very good/excellent. Prior research notes that collapsing response categories may reduce concerns related to variation in reporting by race and ethnicity (Dowd & Todd, 2011). The HRS asks about eight physician-diagnosed chronic conditions comprising heart disease, cancer, lung disease, diabetes, high blood pressure, psychiatric disorders, arthritis, and stroke. An index was created by summing the number of chronic conditions (range = 0-7). An indicator of obesity was created using a measure of body mass index (BMI) based on self-reported height and weight. A higher cut-point was used for defining obesity (i.e., BMI >35) because overweight and obesity in older ages is not as predictive of adverse health outcomes compared with midlife (Lang, Llewellyn, Alexander, & Melzer, 2008). Finally, a dichotomous measure of current smoking status was created, where “current smoker” = 1.
Analytic Strategy
Analyses used multinomial logistic regression to estimate the odds of recovery maintenance 2 years later among a group of previously “recovered” older adults. The risk group comprised multiple baseline waves; therefore, a categorical measure of baseline wave was included in the analyses with Wave 4 (1998) as the reference category. This strategy controlled for any potential wave/year-specific effects. The dependent variable was recovery state (i.e., recovery maintenance, new onset of mobility limitation [reference]), and death/attrition. Only the recovery maintenance versus new onset models is presented; however, the results for death/attrition are available from the author upon request. Given the unique risk group and large set of control variables, analyses were left unweighted; however, robust standard errors (PROC CLUSTER in SAS 9.4) were used to adjust for clustering at the household level. Three sets of models are presented with Model 1 adjusting for sociodemographic characteristics (i.e., age, race/ethnicity, sex, and marital status). Model 2 further adjusting for socioeconomic status and health insurance coverage, and Model 3 introduced health risk factors. This modeling choice allowed for a closer examination of the effect of race and ethnicity on recovery maintenance, net socioeconomic status, and health risk factors.
Because racial and ethnic minorities experience higher levels of disability, this research also sets out to investigate the role of recovery maintenance on ADL disability onset. Given that racial and ethnic minorities experience more recovery, it is important to understand how recovery may influence subsequent disability outcomes. A second set of analyses were performed on the subsample of respondents. Respondents who were free of ADL disability and experienced recovery maintenance were then followed for an additional wave (Wi + 3). Multinomial logistic regression was used to generate odds ratio estimates of disability onset with death/attrition as an additional outcome category (not shown). Similar to the main analyses, these models were left unweighted, but robust standard errors were employed to adjust for clustering at the household level.
Results
Table 1 presents the analytic sample for both the main sample and subsample. Among the main sample of previously recovered respondents (N = 9,378), approximately, 48% of the sample reacquired mobility limitation in the subsequent wave, while 43% experienced recovery maintenance. About 9% of the sample died or attrited between waves during the observation period. The average age of the sample was 67 years (range = 50-104 years), and a majority (i.e., 60%) of respondents were female. Approximately 16% of the sample identified as non-Hispanic Black, while 11% identified as Hispanic or Latinx. Less than 3% of the sample identified as another race or ethnicity. About 68% of the sample was married or partnered. In the recovery maintenance subsample (N = 6,359), 48% of the sample had experienced recovery maintenance, whereas 11% of the sample experienced disability.
Sample Characteristics.
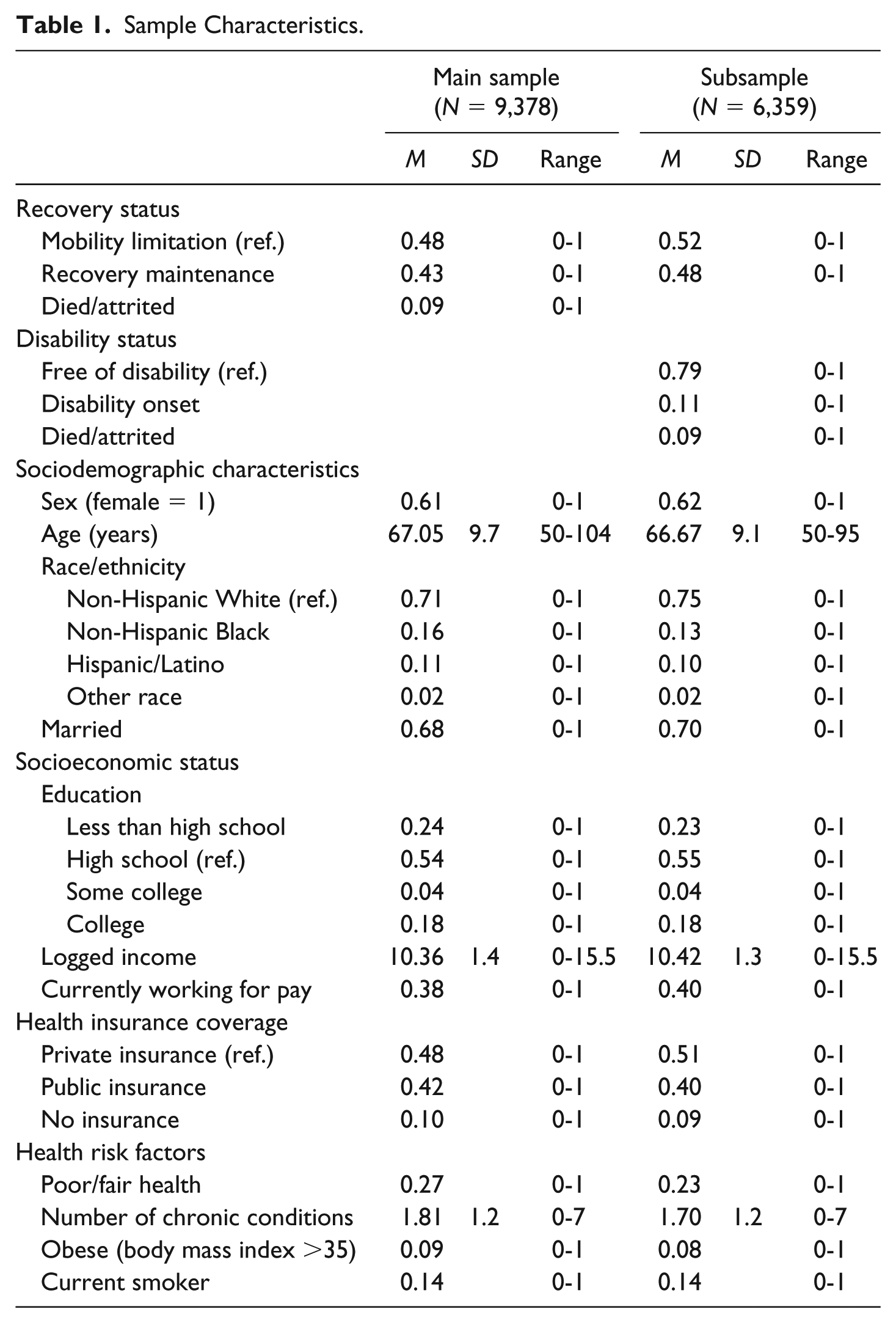
Nearly a quarter of the sample did not have a high school education. The averaged logged income was 10.4 (range = 0-15.5). Nearly 40% of the sample was currently working for pay. Having private health insurance was the modal category. About 10% of the sample reported having no health insurance. Among the health risk factors, more than a quarter of the sample reported fair or poor self-rated health. The average number of chronic conditions was 1.8. About 9% of the sample was obese (BMI >35). Approximately 14% of respondents reported being current smokers.
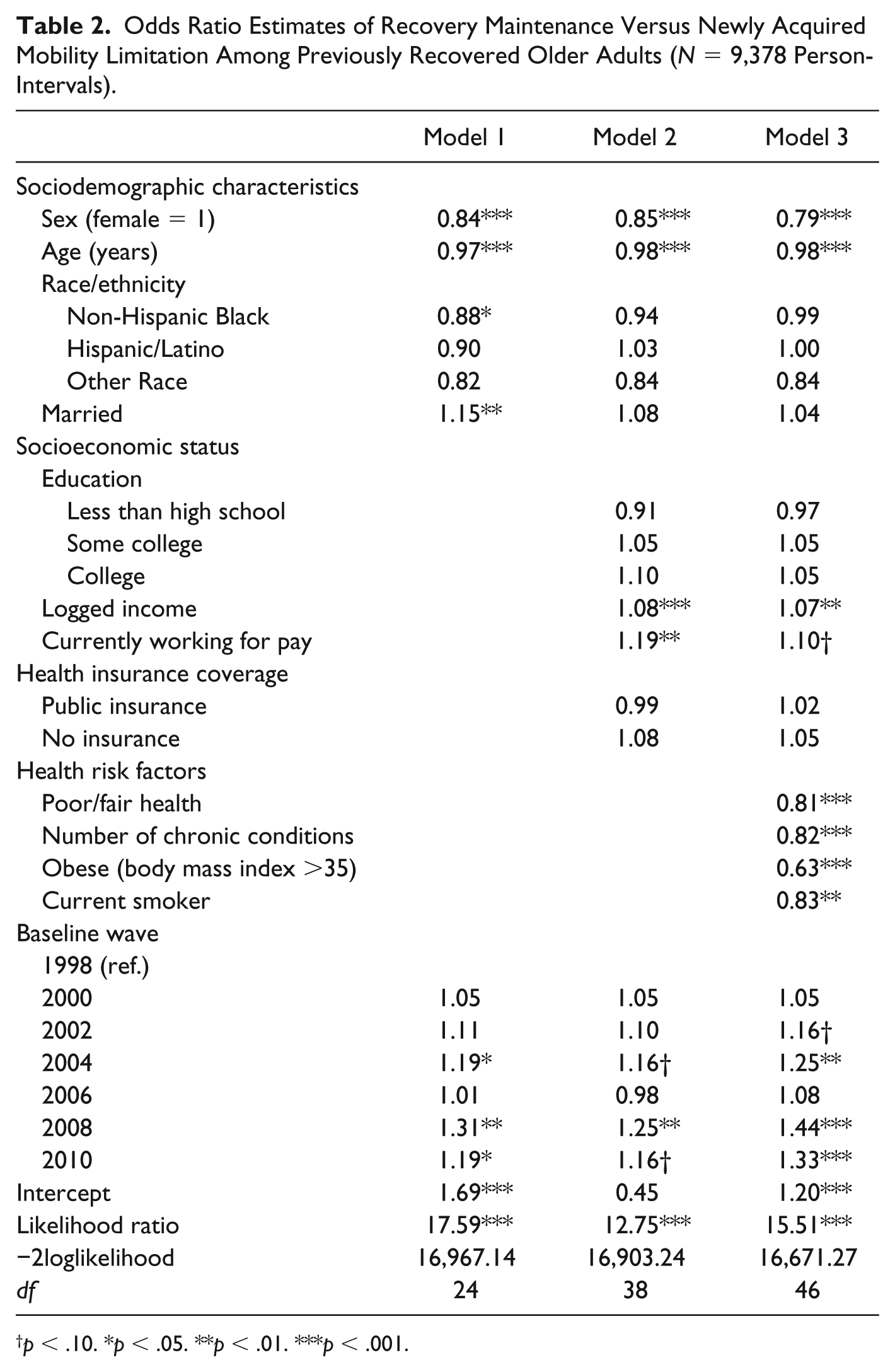
Table 2 presents the odds ratio estimates of recovery maintenance versus newly acquired mobility limitation. The first model only adjusted for sociodemographic characteristics. Women had lower odds of recovery maintenance, compared with men. Older ages were associated with reduced odds of recovery maintenance. Relative to White older adults, Black older adults had lower odds of recovery maintenance, net of age, sex, and marital status. Married and partnered respondents had higher odds of recovery maintenance. Model 2 further adjusted for socioeconomic status and health insurance coverage. After controlling for these factors, there were no longer any significant differences between recovery maintenance by race or ethnicity. Income and working status were both positively associated with recovery maintenance.
Odds Ratio Estimates of Recovery Maintenance Versus Newly Acquired Mobility Limitation Among Previously Recovered Older Adults (N = 9,378 Person-Intervals).
p < .10. *p < .05. **p < .01. ***p < .001.
Finally, Model 3 introduced health risk factors. Age and sex continued to be associated with recovery maintenance. In addition, there were no racial or ethnic differences in recovery maintenance, controlling for all covariates. Income and work status continued to be protective of recovery maintenance. All four health risk factors were negatively associated with recovery maintenance. In general, respondents reporting worse health at baseline had lower odds of recovery maintenance 2 years after they had previously recovered.
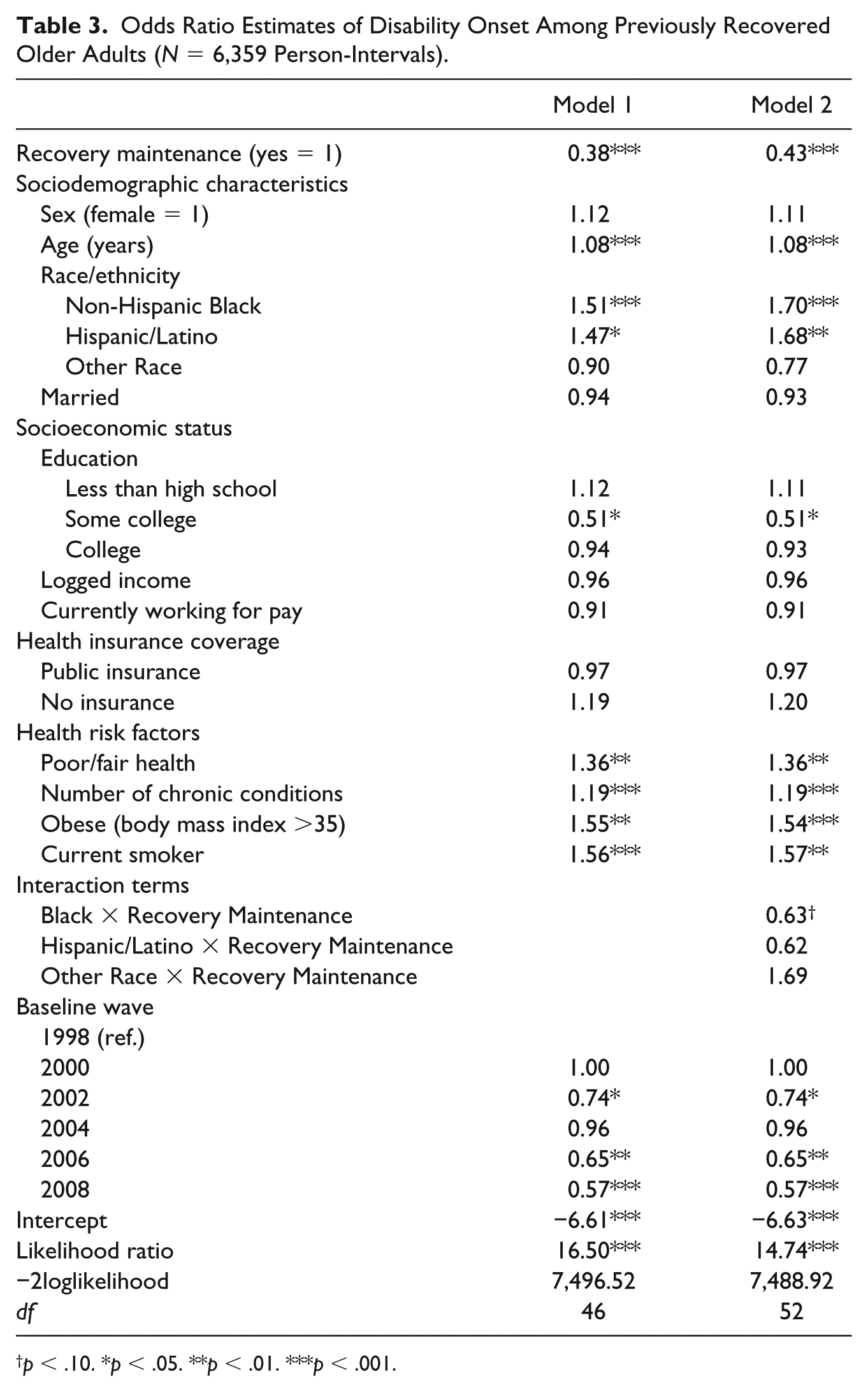
In Table 3, the odds ratio estimates of disability onset among recovery maintenance subsample are presented. In Model 1, recovery maintenance was associated with lower odds of disability onset, net of all other covariates. Respondents who experienced recovery maintenance had a 62% reduction in the odds of ADL disability onset in the subsequent wave. In line with previous research, racial and ethnic minorities had higher odds of disability onset. Both Black and Latinx respondents had higher odds of disability onset, despite having at least one episode of recovery from mobility limitation. In Model 2, an interaction term was introduced to assess whether the effect of recovery maintenance on disability onset varied by race and ethnicity. Using an alpha level of .10, there was suggestive evidence that the race moderated the relationship between recovery maintenance and disability onset. To aid in interpretation, predicted probabilities were generated for White and Black respondents by recovery maintenance status (see Figure 2).
Odds Ratio Estimates of Disability Onset Among Previously Recovered Older Adults (N = 6,359 Person-Intervals).
p < .10. *p < .05. **p < .01. ***p < .001.
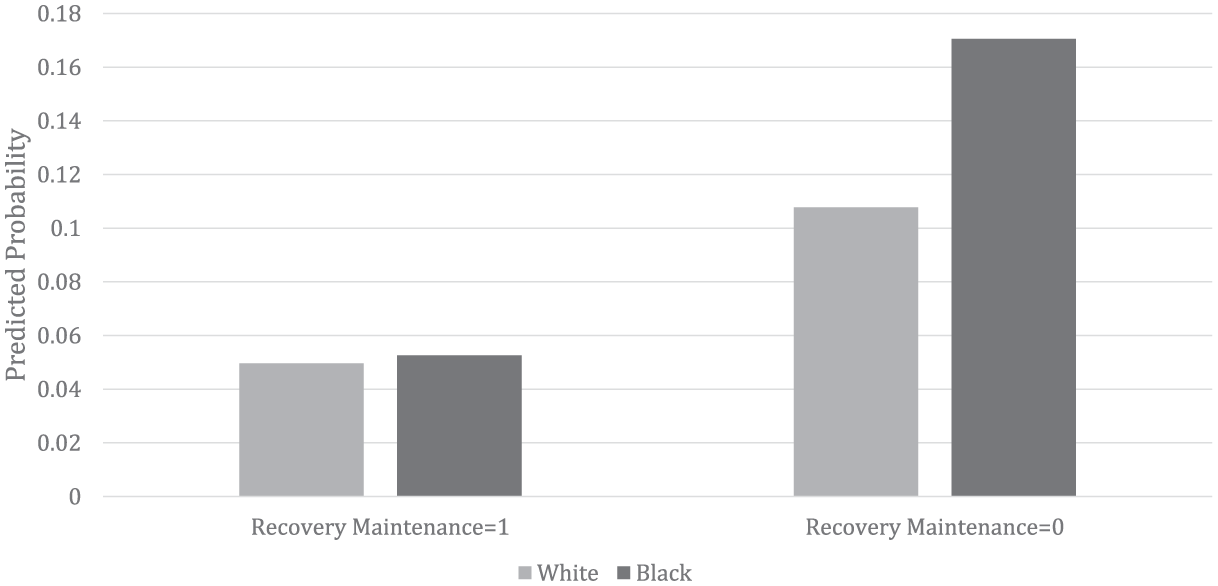
Predicted probabilities of disability onset among White and Black respondents who previously recovered from mobility limitation.
Among White and Black respondents who experienced recovery maintenance, the predicted probabilities for developing disability in the ensuing wave were quite similar (.050 and .053, respectively). However, among the respondents who did not experience recovery maintenance (i.e., had newly acquired mobility limitation after initial recovery), the predicted probabilities of disability onset diverged among White and Black respondents. Black respondents had a higher predicted probability of developing disability onset relative to White respondents.
Sensitivity Analyses
In addition to the focal analyses, supplemental analyses were completed to ensure robustness of these findings. Because this research assumed that racial and ethnic minorities had higher rates of recovery, supplemental analyses were completed to verify this claim. Supplemental Table 1 presents the odds ratio estimates of recovery versus persistent mobility limitation. These results document the increased odds of recovery among racial and ethnic minorities, net of sociodemographic characteristics and health risk factors, for the first episode of recovery. The results in Supplemental Table 1 use only one wave to establish the risk group (i.e., respondents with mobility limitation), and then assesses the odds of recovery in the following wave.
An additional set of sensitivity analyses examined the influence of the inclusion criteria for the main sample. The subsample used an additional risk group criterion (i.e., being free of ADL disability at baseline) so that disability onset could be established. Sensitivity analyses (not shown) were conducted using the same risk group criteria (i.e., having mobility limitation, but free of ADL disability) for the main sample. Findings from these sensitivity analyses (N = 8,262 person-intervals) generated analogous results. Furthermore, in supplemental analyses, the number of depressive symptoms was entered into the models as a health risk factor. With the introduction of depressive symptoms, the substantive findings were not altered. Finally, to assess whether recovery maintenance varied by age, a formal test of moderation was conducted using an age interaction term in the main sample. There were no significant differences in recovery maintenance status by age. In addition, a three-way interaction was explored among recovery maintenance, race/ethnicity, and age in the ADL disability subsample. Again, age was not a significant moderator.
Discussion
The purpose of this research was to examine whether racial and ethnic minorities had lower odds of recovery maintenance, compared with their White peers. After adjusting for socioeconomic status, there were no significant differences in recovery maintenance among older White and minority adults—suggesting that following an episode of recovery, the risk of acquiring a new onset or being free of mobility limitation in the subsequent wave does not vary by race or ethnicity. It is yet to be seen whether a longer observation period would reveal differences in onset and recovery patterns by race and ethnicity; however, this research provides evidence that the higher rates of recovery among minorities is a form of physical resilience.
Mobility limitation is thought to be an impetus for the disablement process (Lawrence & Jette, 1996); however, recovery from mobility limitation is associated with lower odds of ADL disability. Coupled with living in more demanding, hazardous environments and having considerable barriers to health care services, the increased odds of recovery from mobility limitation and lack of significant variation in recovery maintenance, among older minorities, are particularly remarkable. The link between chronic conditions and functional health is well understood with access to high quality health care serving as an important avenue of intervention (Bowen & González, 2008). Although health insurance coverage was not associated with recovery maintenance, this research suggests that more targeted efforts to increase recovery from mobility limitation such as better access to health care services (inside and outside health care settings) could capitalize on the existing physical resilience among older minorities—ultimately reducing racial and ethnic disparities in disability.
This research also investigated whether recovery maintenance predicted onset of ADL disability. Respondents who reported recovery maintenance had remarkably lower odds of subsequent ADL disability onset; however, racial and ethnic minorities had higher odds of ADL disability onset, net of recovery maintenance. There was suggestive evidence that the effect of recovery maintenance on ADL disability onset varied by race. Black and White respondents who reported recovery maintenance had similar predicted probabilities of ADL disability onset, yet among those without recovery maintenance, Black respondents had a higher predicted probability of ADL disability onset. Reacquiring mobility limitation appeared to be particularly detrimental to Black respondents, relative to Whites.
Taken together, this set of results suggests that recovery maintenance is an effective strategy for preventing subsequent ADL disability among racial and ethnic minorities. Conversely, one episode of recovery did not appear to be enough to stave off ADL disability onset among older racial and ethnic minorities. These findings may help illuminate the contradictory findings regarding higher prevalence rates of functional limitations and disability among racial and ethnic minorities, yet increased recovery rates. Older racial and ethnic minorities may experience more recovery, but unless that recovery is accompanied with recovery maintenance, they are still at risk of worsening functional health.
Racial and ethnic minorities face unique challenges to optimal aging because of systemic racism and discrimination. Within the United States, racial and ethnic minorities have fewer economic opportunities, live in environments that are more harmful, have less access to health care, and are exposed to more psychosocial stressors (Williams, 2005), yet many embody physical resilience. For older minorities who experience recovery maintenance, we can expect similar health outcomes compared with their White peers, despite a lifetime of exposure to discrimination. There is much insight to be gained by understanding physical resilience among older minorities.
Although this research provides evidence that recovery maintenance is a salient predictor ADL disability, there are important limitations that must be noted. First, this research examines recovery from mobility limitation among older adults (i.e., 50+ years), which is subject to selective mortality. Because of differences in social and economic resources, racial minorities have lower life expectancies; therefore, older minorities may represent a healthier or hardy population (Beckett, 2000). However, as an attempt to minimize this concern, death and attrition were explicitly measured as an outcome over the observation period. Second, the length of time between each wave was approximately 2 years. I cannot determine whether respondents experience onset and recovery between waves. It is possible that respondents moved in and out of mobility limitation multiple times between waves. Future research should explore recovery maintenance using shorter intervals to address this concern.
Mobility limitation was measured using self-reports and did not take into account whether recovery was due to increased physical functioning or modifications to the environment (e.g., lowering environmental demands). Access to high quality health services is thought to contribute to the management of chronic conditions and progression of disability, yet health insurance coverage was not significantly associated with recovery maintenance in this sample. Although health insurance coverage may provide some insight into access to health care, it does not fully describe the barriers to care experienced by racial and ethnic minorities. Future research should explore the relationship between health care services/treatment and recovery maintenance. Despite these important limitations, I contend that these analyses provide evidence that recovery maintenance is useful for understanding physical resilience and the disablement process—particularly among racial and ethnic minorities.
Conclusion
As the U.S. population continues to age and diversify, many older adults will experience mobility limitation. Structural inequalities ensure that older minorities will experience an excess of mobility limitation and disability compared with their White peers. However, if we are able to prevent subsequent declines in functional health by encouraging recovery maintenance among older adults, we may see increases in active life expectancy. Examining facilitators of recovery is an important first step to identifying meaningful community and clinical interventions. Specifically, targeted interventions that address inequalities in both access and quality of health care services may benefit racial and ethnic minorities with mobility limitation (Penner et al., 2014; Purnell et al., 2016).
In the face of structural barriers, many minority older adults are exhibiting resilience with regard to their functional health. Qualitative research suggests that this resilience is best understood within the context of systemic racism and discrimination. Experiences of past adversity and hardships may undergird current approaches to disease and impairment management among older minorities (Felten, 2000). Structural inequalities may “override” the benefits of temporary or episodic recovery, but for those who are able to maintain their improved mobility, they may also prevent disability onset. Yet, we must recognize that physical resilience and recovery require access to resources such as health care, social support, health-promoting environments, and much more (Behel, Shamaskin, Guequierre, Emery, & Rybarczyk, 2012; Latham, 2018). Future research should strive to understand the larger facilitators of recovery maintenance so that older racial and ethnic minorities may have more opportunities to be resilient and experience optimal aging.
Supplemental Material
Supplemental_Table_1 – Supplemental material for Exploring Racial and Ethnic Differences in Recovery Maintenance From Mobility Limitation
Supplemental material, Supplemental_Table_1 for Exploring Racial and Ethnic Differences in Recovery Maintenance From Mobility Limitation by Kenzie Latham-Mintus in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.