
Abstract
Objectives
This study identifies differences in unmet mobility needs among older adults living in rural versus urban areas.
Methods
We used data from Round 9 of the National Health and Aging Trends Study (NHATS), limiting our analyses to respondents who had not moved since baseline (average housing tenure of 27 years; n = 3343). We conducted bivariate and multivariate analyses to detect rural/urban differences in unmet mobility needs, adjusting for socio-demographics, health status, and housing characteristics.
Results
Rural residence was associated with higher odds of any unmet mobility need
Discussion
Rural older adults aging in place have greater unmet need
Background
In policy and programming, there is a strong emphasis on supporting aging in place; that is, supporting older adults to remain in their home and community as they get older, even if their health and functional status changes. That emphasis accurately reflects older adults’ preferences: most older adults believe that the home setting is the optimal setting for receiving care if one needs it (Kasper et al., 2018). However, the home environment may not always be the optimal setting, especially if older adults’ social networks, health status, and functional status change while their physical environment remains the same. Indeed, some older adults may be “stuck in place” without financially feasible options for changing their current environment or moving to one that would offer a better fit (Erickson et al., 2012; Henning-Smith et al., 2017). Therefore, it is important to understand the extent to which older adults aging in place are able to get around their homes and immediate outdoor environment. This can be measured by examining mobility, defined as the ability to move around one’s home—inside and outside—with or without help (La Grow et al., 2013). Older adults who have mobility limitations and do not have the help they need to cope with them may experience poorer quality of life and poorer health outcomes as a result (La Grow et al., 2013; Musich et al., 2018).
Rural older adults may face particular challenges to aging in place (Bacsu et al., 2014; Henning-Smith, Lahr, & Tanem, 2021; Pruchno, 2018; Skinner & Winterton, 2018). Rural populations are, on average, older than urban populations (Cromartie, 2021; Tuttle et al., 2020). In some cases, this is because of out-migration of younger and middle-aged adults, which can lead to shortages of home health care workforce and informal caregivers to provide care and support if it is needed (Chapman et al, 2022; Cromartie, 2021). Rural older adults themselves differ from urban older adults in meaningful ways. On average, compared with urban older adults, rural older adults have poorer health, more chronic conditions, higher rates of disability, and fewer financial resources (Tuttle et al., 2020). Rural older adults also have barriers to accessing care and services within their local context. These include long-standing issues related to rural transportation (Park et al., 2010), ongoing rural hospital and nursing home closures (Healy, 2019; University of North Carolina Cecil G. Sheps Center for Health Services Research, 2022; Sharma et al., 2021), workforce shortages (Bureau of Health Workforce, 2021; MacDowell et al., 2010), and technological limitations, including limited access to broadband internet (Kozhimannil & Henning-Smith, 2021).
Rural areas also have considerable strengths that may promote positive experiences of aging in place for older adults, one being that rural adults perceive strong social cohesion in their communities (Henning-Smith et al., 2022; Pruchno, 2018). In fact, rural older adults report larger social networks and more tightly knit relationships with family members and friends than urban older adults (Henning-Smith, Moscovice, & Kozhimannil, 2019). Yet, research is limited on whether the experience of aging in place differs between rural and urban older adults.
Unmet needs for help with mobility limitations is one important measure of how well aging in place is working for older adults. If older adults have long-standing mobility limitations, or if they develop new functional impairments that limit mobility, they may still have a positive experience aging in place with the right housing environment and adequate physical and instrumental support (Henning-Smith et al., 2017). Yet, having an accessible housing environment and receiving adequate support depends on a number of factors, including housing characteristics, local environment, availability of caregivers, and access to financial and material resources. For example, previous research has shown that, for low-income older adults living alone, functional status worsens over time, while functional status can actually improve for high-income older adults living alone (Henning-Smith et al., 2017).
All of these concepts can be viewed through the conceptual framework of person-in-environment, widely used within the social work field to understand how someone’s broader position within their physical, social, political, and environmental context impacts their well-being and health outcomes (Kondrat, 2013). This approach simultaneously emphasizes individual outcomes and the array of supportive resources and barriers in one’s local environment affecting these outcomes (Sheafor & Horejsi, 2007: p. 9). Rather than simply investigating individual outcomes, we need to consider people as embedded within their homes and communities in order to understand the outcomes of aging in place. This includes the home environment (indoor and outdoor), neighborhood, and broader community, as well as local, state, and federal policy. This study applies a person-in-environment framework to understanding rural/urban differences in unmet mobility needs for older adults aging in place.
We hypothesize that: (1) Among older adults aging in place, rural older adults will have fewer financial resources, less accessible housing, and more underlying health conditions than urban older adults. (2) Rural older adults aging in place will have greater unmet needs for help with mobility limitations than their urban counterparts, indicating a need for additional resources and support to ensure a good person-environment fit.
Methods
Data and Sample
For this study, we use data from Round 9 of National Health and Aging Trends Study (NHATS, 2022). The National Health and Aging Trends Study (NHATS) is a nationally representative survey of Medicare beneficiaries age 65 and older that has been fielded annually using in-person interviews since 2011. The sample was replenished in 2015 (Round 5), so that the sample again was nationally representative of Medicare beneficiaries age 65 and older (NHATS, 2022). NHATS follows respondents longitudinally to provide insight into changes in functional status, functional accommodations made through device use, home modifications, caregiving arrangements, and changes in residence including entry into institutional care. For this study, we limited our analysis to older adults who had not moved since baseline, meaning that they had been in the same home since their enrollment in the study (n = 3343).
Measures
The dependent variable for this study was unmet mobility needs. This was based on a composite of three different variables: unmet needs for help with outdoor mobility (did not go outside due to difficulty and a lack of help), unmet needs for help with indoor mobility (did not get around inside the home due to difficulty and a lack of help), and unmet needs for transferring (did not get out of bed due to difficulty and a lack of help). Any unmet need for help with mobility was assessed with an affirmative answer to one or more of those three variables. We analyzed each of the individual mobility needs questions separately, as well as in the composite variable.
Rurality was measured using the binary rural/urban variable included in the NHATS data. NHATS assigns a rural or urban designation to each respondent based on Office of Management and Budget classification of their county of residence as nonmetropolitan (rural) or metropolitan (urban) (Cromartie, 2019). Socio-demographic characteristics included living arrangement (living alone vs. with others); age; sex (female vs. male); race and ethnicity (non-Hispanic White, non-Hispanic Black, other); educational attainment (less than high school, high school degree, some college, college degree, graduate/professional degree); and household income. Housing characteristics included home ownership (own vs. rent home/apartment); housing type (single-family home, duplex, mobile home, or multi-unit building); and tenure in the home, measured in months. Housing characteristics also included measures of accessible housing: presence of stairs, presence of ramp, and presence of stairs with no ramp at the entry.
Health characteristics included self-rated health (good/very good/excellent vs. fair/poor) and diagnosis of the following chronic conditions: heart attack, heart disease, hypertension, arthritis, osteoporosis, diabetes, lung disease, stroke, probable dementia, cancer, hearing problems (based on not being able to use the phone), vision problems (based on not being able to read the newspaper), depression (based on the PHQ-2 score >2), and anxiety (based on GAD-2 score >2). These represent the available chronic conditions in Round 9 of the NHATS, and include the most common chronic conditions among older adults in the U.S. (Centers for Disease Control and Prevention, 2020). A count of chronic conditions tallied the number of diagnoses each respondent reported. We also included a measure of hip fracture and broken bone within the past year. Fall history included whether the respondent had a fall in the past year and whether they are worried about falling. Finally, to assess functional status, a composite measure was used to indicate that the respondent needed any help with activities of daily living (ADLs), including eating, bathing, dressing, or toileting, and a separate composite measure was used to indicate that the respondent needed any help with instrumental activities of daily living (IADLs), including laundry, shopping, meal preparation, banking, or medication management.
Analysis
We first conducted bivariate comparisons between rural and urban older adults on the dependent variable and all independent variables, using chi-squared tests for categorical variables and t-tests for continuous variables. Then, we conducted nested logistic regression models predicting unmet needs for help with mobility limitations, first adjusting for only rurality, then adding socio-demographic characteristics, housing characteristics, and health and functional status. In multivariable models, we included the overall count of chronic conditions, rather than each individual condition in order to avoid model overspecification.
The purpose of the nested models is to see the separate, but compounding, impact of different aspects of the person’s environment. By understanding compounding environmental factors, we situate individual outcomes in environmental context (Sheafor & Horejsi, 2007). For all analyses, we used survey weights and design variables to account for the complex sampling and to approximate national estimates.
Results
Sample Characteristics by Rural and Urban Location.

Data are from Round 9 of the National Health and Aging Trends Study (NHATS) and include respondents who had not moved since baseline (n = 3343). Numbers in the table represent weighted proportions of the study sample.
Rural older adults aging in place were more likely than urban older adults to own their home (88% vs. 82%, p < .05) and were more likely to live in single-family homes or mobile homes (p < .001). Rural older adults aging in place were also more likely than urban older adults to have stairs (84% vs. 76%, p < .01) or a ramp (14% vs. 8%, p < .01) at their entrance, again supporting Hypothesis 1 (rural older adults aging in place have less accessible housing than urban older adults aging in place). Contrary to Hypothesis 1, rural and urban older adults aging in place did not differ in terms of having stairs, but no ramp, at the entrance.
Health Characteristics, Fall History, and Unmet Needs for Care by Rural and Urban Location.

Data are from Round 9 of the National Health and Aging Trends Study (NHATS) and include respondents who had not moved since baseline (n = 3343). ADL = activity of daily living; IADL = instrumental activity of daily living. Numbers in the table represent weighted proportions of the study sample.
Supporting Hypothesis 2, rural older adults aging in place reported greater unmet mobility needs overall (11% vs. 7%, p < .05), as well as within specific outdoor (7% vs. 4%, p < .05) and indoor (5% vs. 3%, p < .05) categories, compared with urban older adults aging in place. Rural and urban older adults aging in place did not differ in terms of unmet needs for transferring in and out of bed (see Figure 1). Unmet needs for help with mobility limitations by rural and urban location. Data are from Round 9 of the NHATS and include respondents who had not moved since baseline (n = 3343). Difference between rural and urban significant at *p < .05.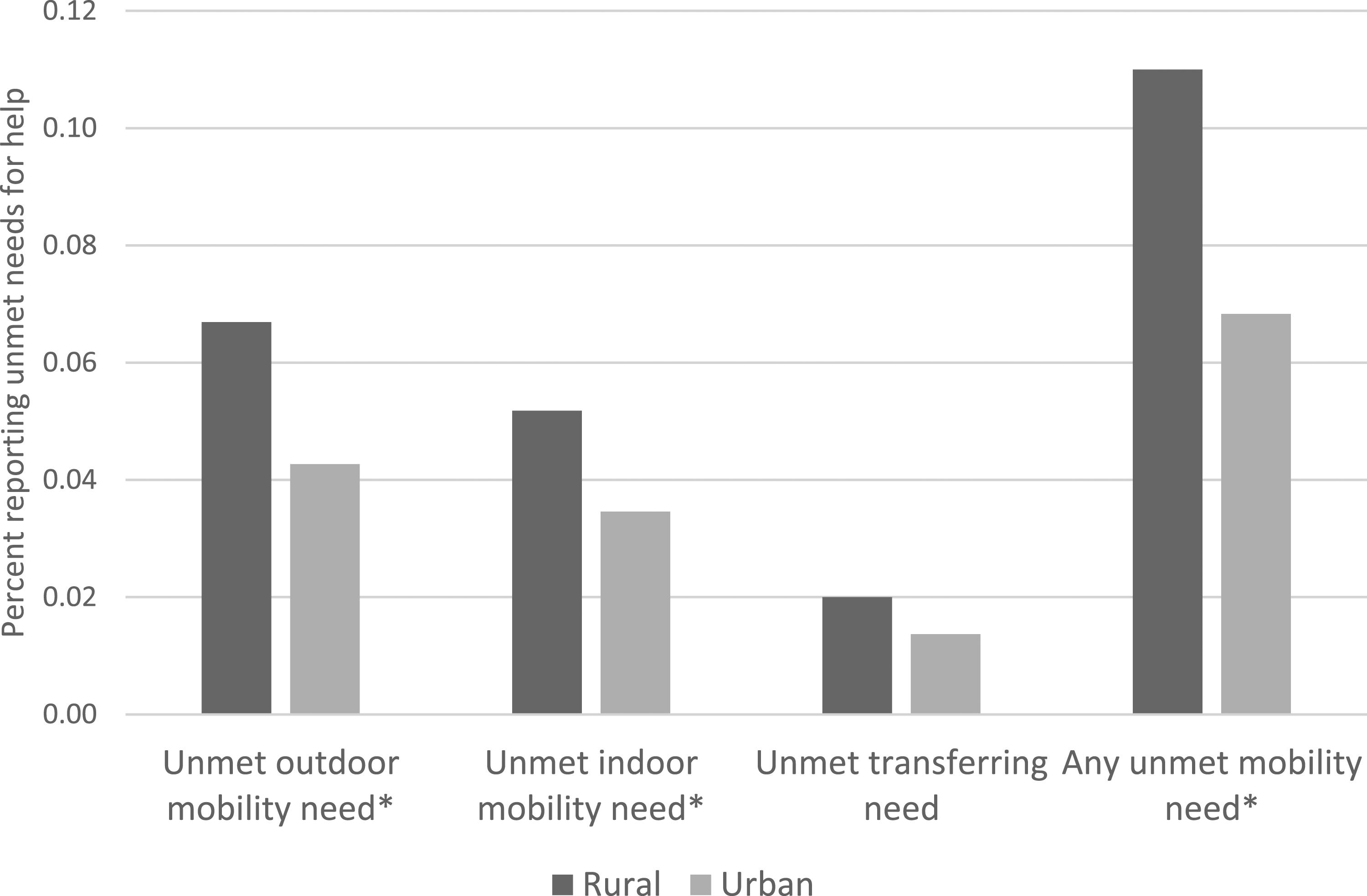
Nested Logistic Regression Models Assessing Odds of Unmet Mobility Needs.
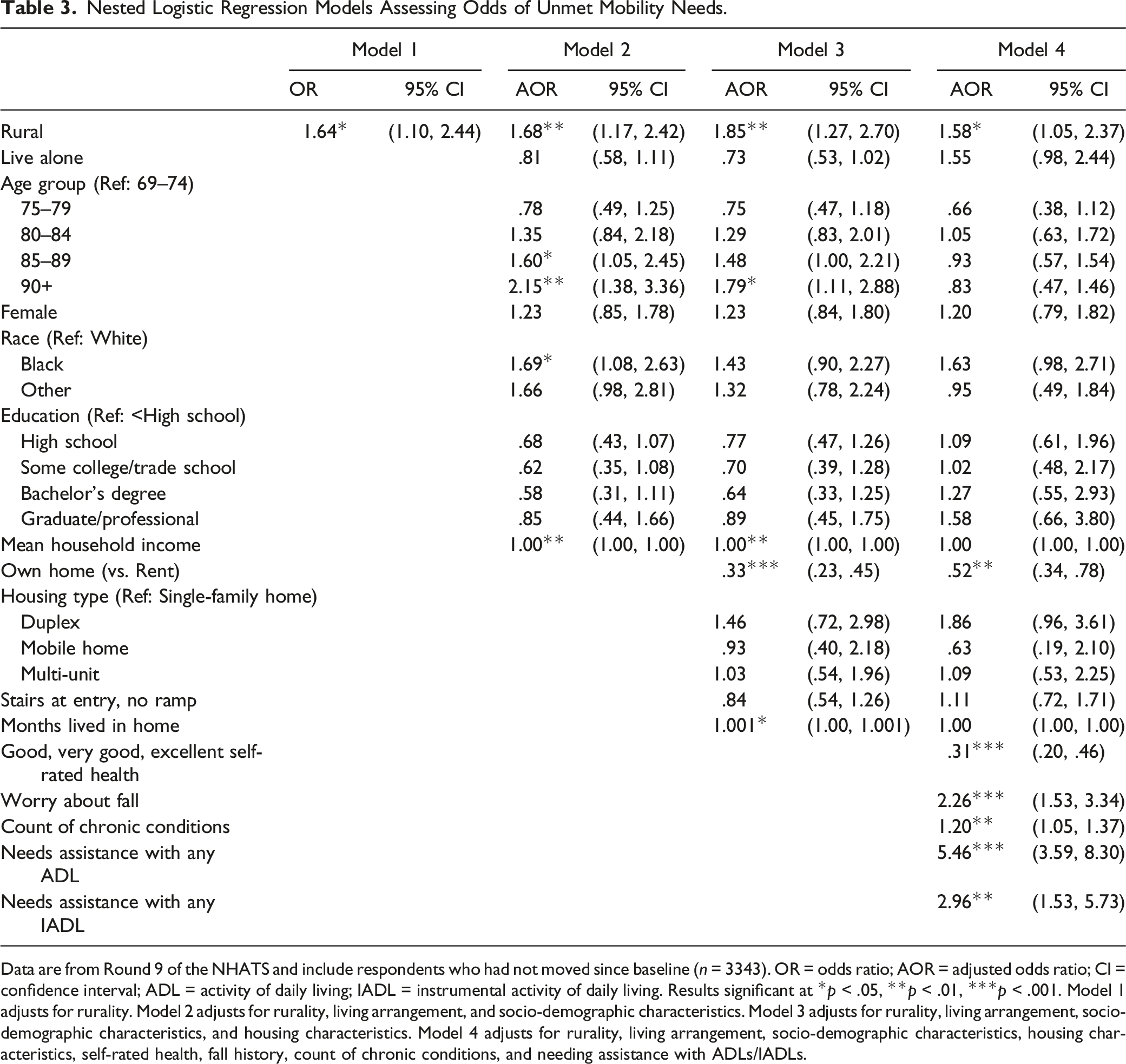
Data are from Round 9 of the NHATS and include respondents who had not moved since baseline (n = 3343). OR = odds ratio; AOR = adjusted odds ratio; CI = confidence interval; ADL = activity of daily living; IADL = instrumental activity of daily living. Results significant at *p < .05, **p < .01, ***p < .001. Model 1 adjusts for rurality. Model 2 adjusts for rurality, living arrangement, and socio-demographic characteristics. Model 3 adjusts for rurality, living arrangement, socio-demographic characteristics, and housing characteristics. Model 4 adjusts for rurality, living arrangement, socio-demographic characteristics, housing characteristics, self-rated health, fall history, count of chronic conditions, and needing assistance with ADLs/IADLs.
Discussion
In this study, we found that rural older adults aging in place report more unmet needs for mobility assistance than their urban counterparts. This means that they are more likely than urban older adults aging in place to have difficulty getting around their home environment, both indoors and outdoors. This could have large implications on quality of life. Having trouble navigating one’s home and neighborhood environment, and not receiving adequate assistance with that navigation, may limit one’s daily activities, including participation in social events, physical activities, hobbies and leisure, household chores, work, and civic engagement. Moreover, the measure of unmet needs for mobility assistance in this study assessed whether older adults could not easily move around their home environment, which may signal larger issues with meeting one’s daily needs (e.g., food preparation, bathing, toileting, home maintenance) and should raise concerns about safety and health. This is reflected in our findings that limitations in ADLs and IADLs were more strongly correlated with unmet needs for mobility help than any other variable we assessed. Clearly, some older adults aging in place—especially those living in rural areas—have limitations in mobility and daily activities that are not being sufficiently addressed and supported.
For the 11% of rural older adults and 7% of urban older adults aging in place who do have unmet mobility needs; however, our findings may reflect being stuck in place, rather than aging in place because of preference. Policy and programs need to become more attuned to that nuance (Chen et al., 2019; Friedman et al., 2019; Gorges et al., 2019; Wang et al., 2021). This means that, while substantial gains have been made in ensuring that older adults are able to remain in their homes and communities, effort still needs to be put into ensuring high-quality alternatives to aging in place, especially in rural areas (Henning-Smith, Mulcahy, et al., 2021). This is complicated by the fact that rural long-term care facilities have been closing at a faster rate than urban long-term care facilities, and rural areas have greater health care workforce shortages (Bureau of Health Workforce, 2021; Sharma et al., 2021).
We also found that rural older adults are more likely to own their homes. This could be good, indicating more financial security and lower housing costs. However, that also means that they are more solely responsible for home maintenance, upkeep, modifications, and accessibility. Currently, there are limited policies and programs available to support older adults with housing modifications and accessibility in both rural and urban areas. However, rural housing is older and in poorer quality to begin with (“Barriers to Affordable Rural Housing, 2018; Housing Assistance Council, 2008; White, 2015”) and rural older adults aging in place may be living in less accessible and appropriate settings than their urban counterparts. For example, we find that rural older adults aging in place are nearly 10% points more likely to have stairs at the entrance to their home compared with urban older adults aging in place. They are also more likely to have a ramp at their entrance, but still three-quarters of rural older adults aging in place have stairs with no ramp at the entrance to their home. The presence of these housing characteristics has implications for exercise, socialization, and ability to attend appointments. This is especially true in under-resourced rural communities, where access to home and community based services and home health care workforce may be more limited (Chapman et al, 2022), and for low-income older adults in both rural and urban settings who may not be able to access or afford home modifications (Henning-Smith et al., 2017). Additionally, given that rural older adults aging in place were also more likely to be worried about falling and to have unmet needs for help with mobility limitations, such differences in housing characteristics likely have serious implications for their experience of aging in place because the home environment may not be sufficiently safe or accessible. These issues are exasperated by the fact that rural older adults have fewer financial resources (Tuttle et al., 2020) and that rural areas have older, poorer-quality housing stock (“Barriers to Affordable Rural Housing,” 2018; Housing Assistance Council, 2008; White, 2015). As a result, rural residents may find that home modifications are more difficult to complete, both because of limited financial resources and because of the underlying condition of their home.
Despite the aforementioned issues, older adults aging in place who owned their home were less likely than older adults aging in place who rented to have unmet needs for help with mobility limitations, above and beyond rural/urban location. Given that we were looking at a subset of older adults who had not moved since their enrollment in the survey, these findings point to the particular risk faced by older adults aging in place in rental housing. Those older adults may be even more susceptible to inappropriate living environments and may have less agency in making modifications to their homes. Because this study captures older adults aging in place, rather than older adults who may have moved to a rental unit for accessibility reasons, we are likely detecting the particular vulnerability of older adults in rental housing. On average, across the U.S., renters have significantly fewer financial resources than homeowners (U.S. Federal Reserve, 2020), and prior research has shown that lower-income older adults are more likely to develop functional limitations while aging in place (Henning-Smith et al., 2017).
Our findings also indicated that difficulties with ADLs and IADLs were relatively common among older adults aging in place in both rural and urban areas. More than 10% of all older adults aging in place reported needing help with an ADL, and nearly three-quarters reported needing help with an IADL. Needing help with ADLs and IADLs were both associated with higher odds of having an unmet needs for help with mobility limitations, above and beyond location, socio-demographic characteristics, and health. While not surprising, these findings emphasize the importance of assessing for limitations related to ADLs and IADLs among older adults aging in the community, especially because of their close association with unmet needs for help with mobility limitations. Such assessments could occur in routine clinical settings, and may result in referrals to home health and/or occupational or physical therapy. For rural older adults aging in place, there may be additional barriers to overcoming those limitations, including transportation, lack of caregivers and providers, and longer distances to services (Henning-Smith, Mulcahy, et al., 2021; Henning-Smith, Wu, & Lahr, 2019), but addressing them may help older adults with mobility limitations to remain in their homes longer and more comfortably.
Limitations
As with any study, our findings should be considered in light of their potential limitations. First, we use a binary measure of rural/urban location. While this is useful for shedding light on rural/urban differences and disparities, it is less useful for understanding regional variation and differences by degree of rurality. Further, counties are a blunt measure of rurality and counties can contain both urban and rural areas (Bennett et al., 2019). Next, given the relatively small sample size of rural older adults aging in place in the NHATS, it is not possible to look in adequate detail at inequities by race and ethnicity. This is an important omission, as structural racism impacts access to housing and health outcomes among older adults. Finally, we present information on housing characteristics, but not housing quality, in this study. More research is needed on all of these dimensions, especially given the growing population of older adults in rural areas amid increasing housing and health care challenges.
Implications
Given that most older adults would prefer to age in place in both rural and urban areas, more efforts are required to ensure that they can do so safely and comfortably. Our findings show that older adults aging in place experience unmet need
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Federal Office of Rural Health Policy (FORHP), Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) under PHS Grant No. U1CRH03717-13-00. This research was also supported by the NIH National Center for Advancing Translational Sciences, grant UL1TR002494.The information, conclusions and opinions expressed in this manuscript are those of the authors and no endorsement by FORHP, HRSA, NIH, or HHS is intended or should be inferred.