
Abstract
Introduction
The Improving Medicare Post-Acute Care Transformation Act (the IMPACT Act) and other payment reforms (e.g. bundled and site-neutral payment programs) are changing how post-acute care (PAC) services are, and will be, received, delivered, and reimbursed (Centers for Medicare & Medicaid Services, 2017, 2018a, 2018b; The Lewin Group, 2018; The Urban Institute, 2014). PAC can be delivered in an inpatient rehabilitation facility, skilled nursing facility, home health agency, or long-term care hospital (Carter & Garrett, 2012; Mallinson, Deutsch, Bateman et al., 2014; Medicare Payment Advisory Commission, 2018). Each PAC setting provides different levels of rehabilitation. For example an inpatient rehabilitation facility offers acute care services for patients who need and can tolerate a greater degree of intervention following traumatic injuries and surgeries such as amputations. On the other hand, a skilled nursing facility offers subacute rehabilitation, which is similar to but less intensive than the interventions provided at an inpatient rehabilitation facility. Understanding how and why patients use additional PAC can help clinicians make important care transition choices or suggestions. However, limited data exist regarding the comparative effectiveness of health outcomes and services provided to patients across the PAC continuum.
Understanding the association between functional status and care transitions across PAC settings is crucial in the current healthcare landscape. Functional status is an important patient outcome. In particular, maintaining or improving functional ability (e.g., eating, dressing, and grooming) can optimize independence and quality of life, while also minimizing care costs for patients (Burke et al., 2016; Courtney et al., 2011; Covinsky et al., 2003; Middleton et al., 2017; Paterson & Warburton, 2010). Impaired function in PAC settings is a modifiable factor for subsequent hospital readmission and institutionalization (Burke et al., 2016; Fisher et al., 2013; Middleton et al., 2017). The relationship of functional status in different PAC settings and the sequence of PAC transitions, however, remain largely unknown.
To our knowledge this is the first study to examine co-calibrated functional scores across PAC settings and their associated PAC transitions for Medicare beneficiaries. This study examined self-care and mobility functional status for Medicare beneficiaries who initially transitioned to one of three PAC settings (inpatient rehabilitation facility, skilled nursing facility, and home health agency) after an acute hospitalization, and the association between functional status and subsequent PAC transition(s). Although the Centers for Medicare and Medicaid Services (CMS) started collecting standardized functional data (known as Section GG) at inpatient rehabilitation facilities in October 2015, the unified functional data are not currently available across all PAC settings (Centers for Medicare & Medicaid Services, 2018b). Using a co-calibration methodology allows us to compare functional status across PAC settings. This study provides a baseline of the associations between admission functional status (self-care and mobility) in the initial PAC setting and subsequent PAC transitions in the context of the current health-care policy. We hypothesized that higher functional scores at PAC admission would be associated with a lower likelihood of subsequent PAC transitions.
Methods
Data Source
We analyzed 100% of Medicare files covering 540,389 Medicare beneficiaries from January 2013 to August 2014. We identified index stays in acute hospitals for patients based on Medical Severity Diagnosis Related Groups and procedure codes. We used the Master Beneficiary Summary File, the Inpatient Rehabilitation Facility Patient Assessment Instrument (IRF-PAI) file, the Minimum Data Set (MDS 3.0) file, and the Home Health Outcome and Assessment Information Set (OASIS) file to obtain functional data. A Data Use Agreement was established following the CMS guidelines prior to any data analysis.
Cohort Selection
Online Appendix Table 1 illustrates the cohort selection process. Patients initially discharged home were excluded. The eligible cohort included Medicare beneficiaries aged 66 years or older enrolled in a Medicare fee-for-service plan, with one of the following impairments: stroke, lower extremity joint replacement, and hip/femur fracture. We chose these three impairments as they represent the largest users of PAC services and are also part of the impairment conditions CMS used to test episode-based payment models (e.g., the Bundled Payments for Care Improvement Initiative) (Medicare Payment Advisory Commission, 2018; The Lewin Group, 2018). We included beneficiaries initially discharged to one of the three abovementioned post-acute settings after an acute hospital stay. In the preliminary analyses, we found that less than 5% of Medicare beneficiaries initially discharged to home health agencies continued to use a second PAC service (Online Appendix Tables 2–4). Based on this finding, beneficiaries initially discharged to home health agencies were excluded in the subsequent logistic modeling (details described below).
Study Outcome
The primary outcome was one or more PAC transitions (yes/no), defined as using any subsequent PAC services (inpatient rehabilitation facilities, skilled nursing facilities, and home health agencies) in the follow-up period after a stay in the first PAC setting after an acute hospital stay.
Primary Predictor Variable
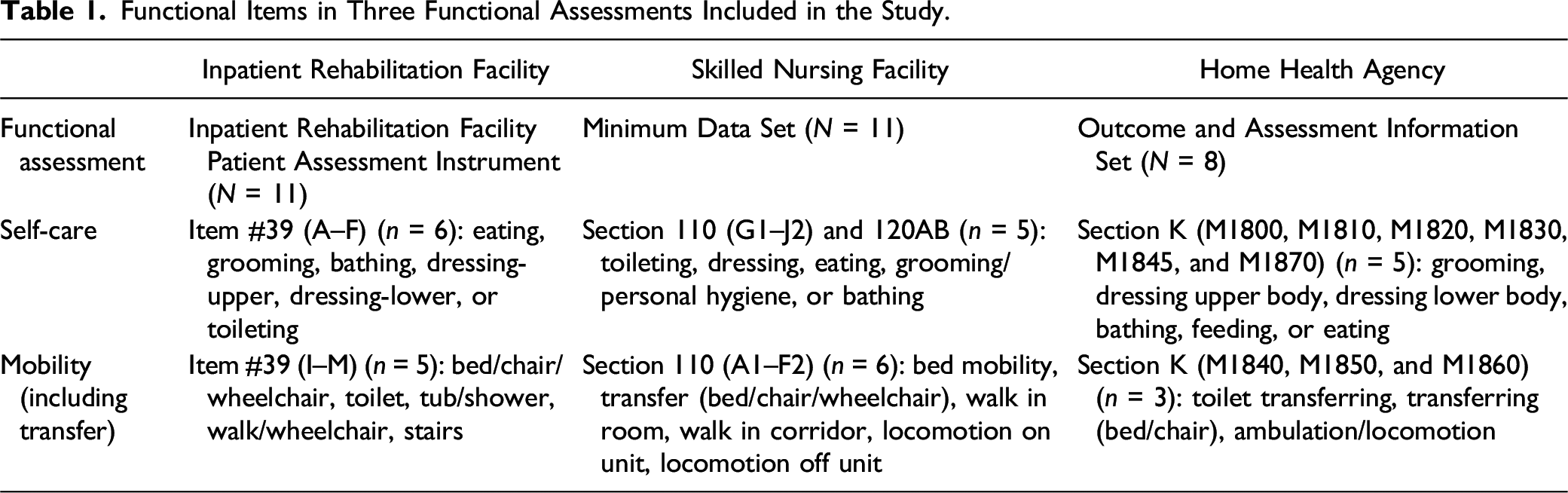
Functional Items in Three Functional Assessments Included in the Study.
Covariates
The analytical models were adjusted for available patient-level characteristics: (a) sociodemographic variables: age, gender, race/ethnicity, and original entitlement (original reason the patient received Medicare services, including age, disability, or end-stage renal disease) and (b) health-related factors: type of impairment (for stroke: ischemic stroke and hemorrhagic stroke; for lower extremity joint replacement: elective hip, nonelective hip, knee, and other joint replacement; and for hip/femur fracture: femur, femur neck, complications, and other fracture), Elixhauser comorbidities, length of hospital stay, length of PAC stay, and Medicare/Medicaid dual eligibility (yes/no).
Statistical Analyses
We conducted a total of six separate analyses: unadjusted models (n = 3) and models adjusted for all patient-level covariates (n = 3) for each impairment. A multilevel logistic regression model was used to examine the amount of variance (%) in the subsequent PAC transitions attributed to the functional score at admission in the initial PAC setting. In addition, the adjusted odds ratios of the probability of having one or more PAC transitions (yes/no) based on the co-calibrated functional score at admission to the initial PAC setting were estimated. Each model was stratified by impairment and adjusted for all the above-listed covariates. All analyses were performed with SAS 9.4 (Cary, NC).
Results
Patient Characteristics
Demographics of the Total Included Sample Cohort (N = 540,526).
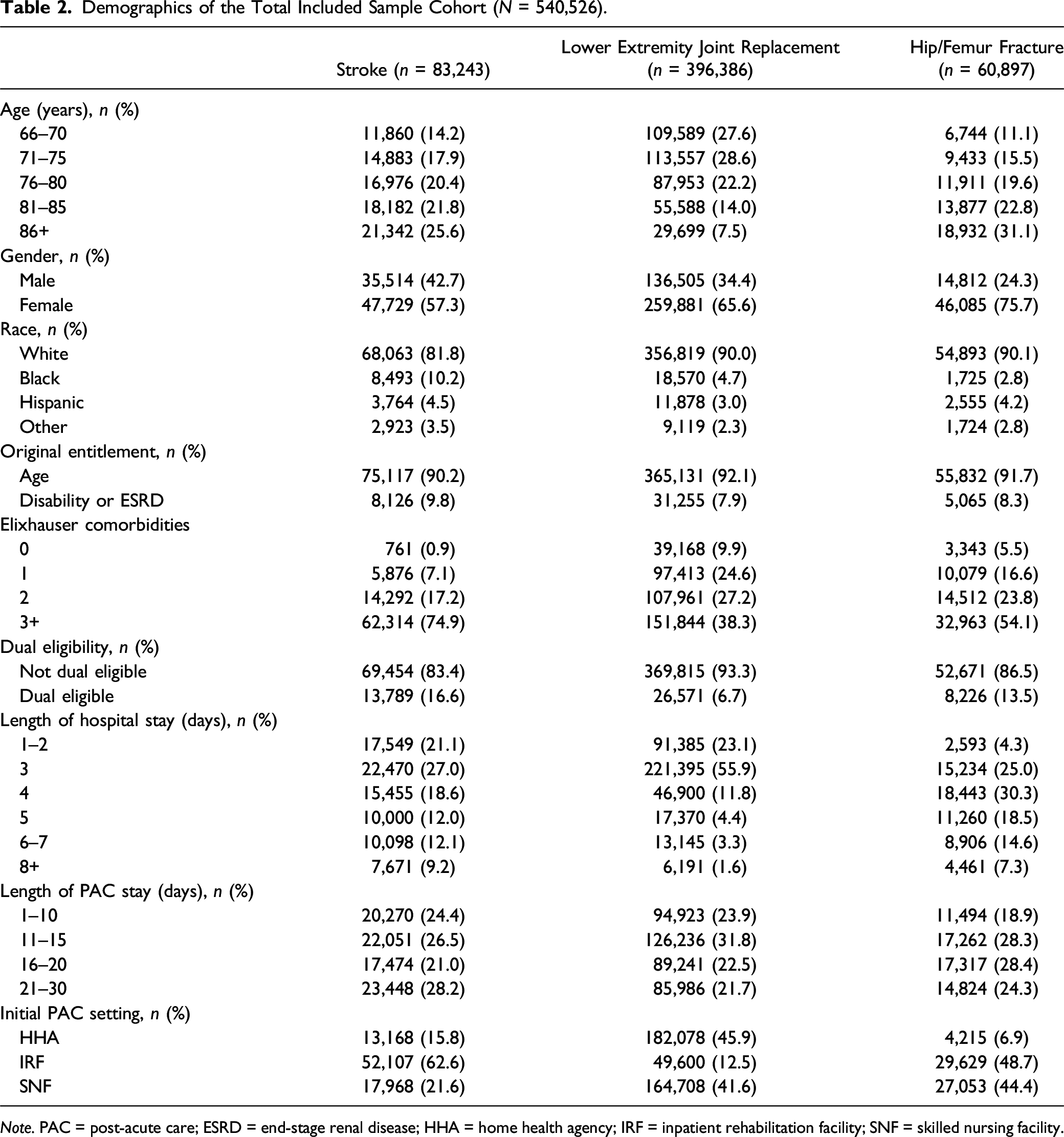
Note. PAC = post-acute care; ESRD = end-stage renal disease; HHA = home health agency; IRF = inpatient rehabilitation facility; SNF = skilled nursing facility.
Functional Scores across PAC Settings
Figure 1 provides detailed comparisons of the initial functional status (mobility and self-care) at the first PAC setting by impairment condition. Overall, for patients with stroke, the highest median functional scores in self-care occurred when the initial discharge was to home health agencies (56.5), followed by skilled nursing facilities (49.3) and inpatient rehabilitation facilities (48.5). For mobility in stroke, the highest median scores by PAC setting were for those discharged to home health agencies (51.3), then skilled nursing facilities (47.6) and inpatient rehabilitation facilities (47.0). For patients with lower extremity joint replacement, the highest median functional scores in self-care occurred when the initial discharge was to home health agencies (53.2), followed by inpatient rehabilitation facilities (51.8) and skilled nursing facilities (51.2). For mobility in lower extremity joint replacement, the highest median scores by PAC setting were for those discharged to skilled nursing facilities (48.8), followed by inpatient rehabilitation facilities (47.0) and home health agencies (46.3). For patients with hip/femur fracture, the highest median functional scores in self-care occurred when the initial discharge was to home health agencies (50.1), followed by inpatient rehabilitation facilities (48.5) and skilled nursing facilities (47.4). For mobility in hip/femur fracture, the highest median scores by PAC setting were for those discharged to home health agencies (46.3), inpatient rehabilitation facilities (44.7), and skilled nursing facilities (43.4). Representation of the co-calibrated functional score distribution (self-care and mobility) at the initial post-acute setting by impairment condition (n = 540,526). Note. IRF = inpatient rehabilitation facility; SNF = skilled nursing facility; HHA = home health agency.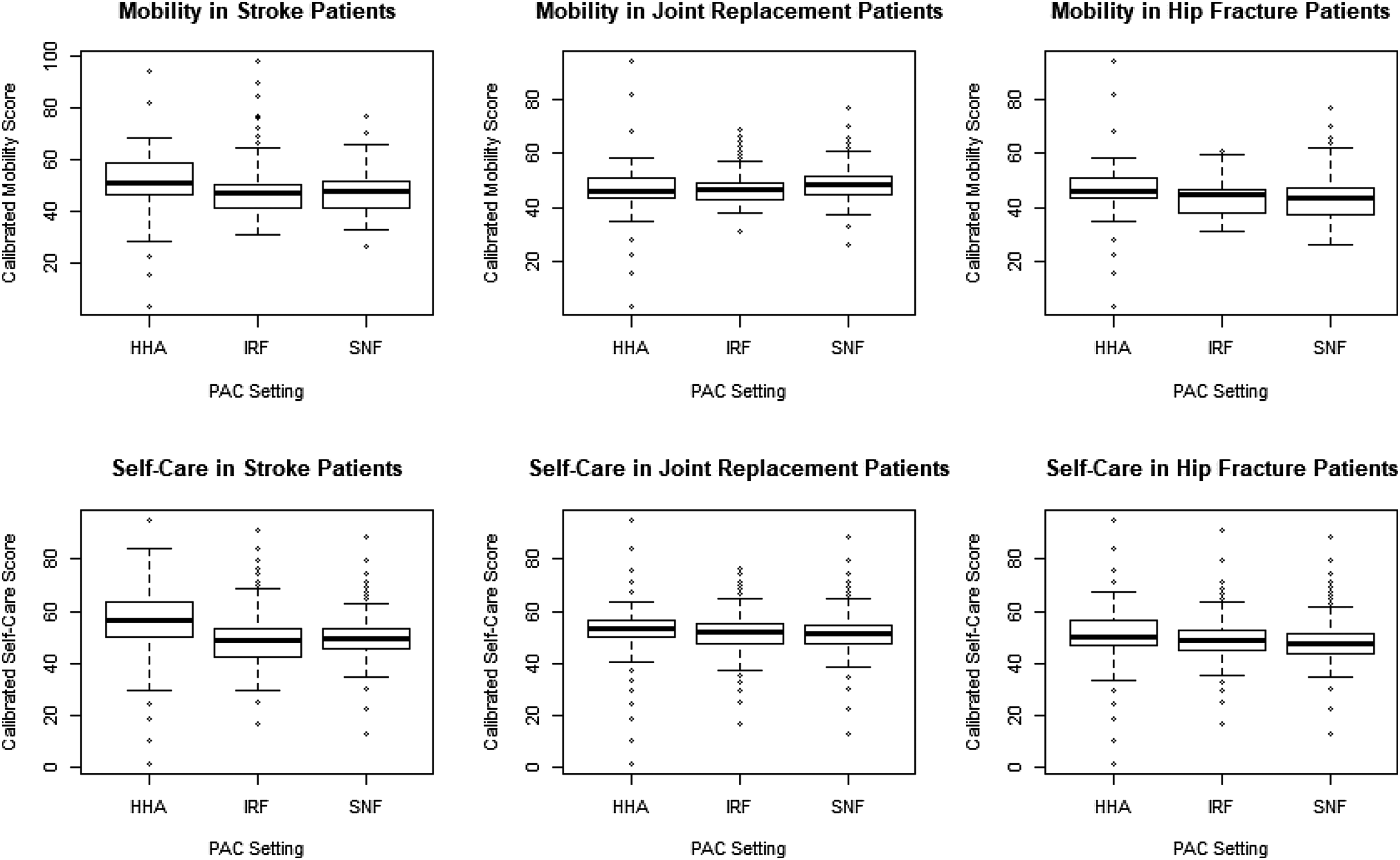
Initial and Subsequent PAC Service Use by Impairment
For the total sample, of those who used one PAC service (n = 540,526), 38.1% transitioned to a second PAC service (n = 205,774). Among those who transitioned to a second PAC service, 8.6% transitioned to a third PAC service (n = 17,697). Most patients used at least two PAC services if initially discharged to an inpatient rehabilitation facility (stroke (69.8%), lower extremity joint replacement (70.3%), and hip/femur fracture (84.8%)). The majority of patients with stroke were initially discharged to inpatient rehabilitation facilities (62.6%); those with lower extremity joint replacement were mainly discharged to home health agencies (46.0%); and those with hip/femur fracture were mainly discharged to inpatient rehabilitation facilities (48.7%) (Online Appendix Tables 2–4).
Association of Functional Score with Subsequent PAC Transitions
Proportion of Variance of Sequence of Post-Acute Care (PAC) Explained by Functional Status (Self-Care and Mobility) at Initial PAC Setting (n = 341,065).
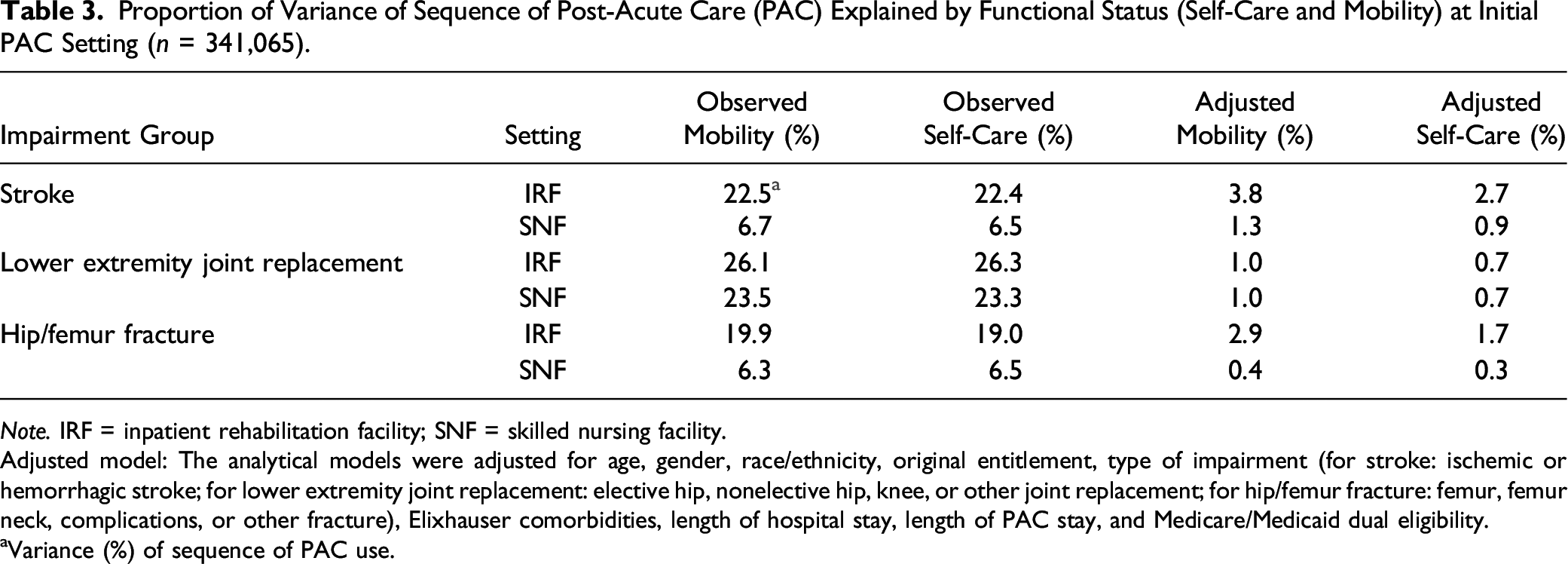
Note. IRF = inpatient rehabilitation facility; SNF = skilled nursing facility.
Adjusted model: The analytical models were adjusted for age, gender, race/ethnicity, original entitlement, type of impairment (for stroke: ischemic or hemorrhagic stroke; for lower extremity joint replacement: elective hip, nonelective hip, knee, or other joint replacement; for hip/femur fracture: femur, femur neck, complications, or other fracture), Elixhauser comorbidities, length of hospital stay, length of PAC stay, and Medicare/Medicaid dual eligibility.
Variance (%) of sequence of PAC use.
Detailed Estimates and Level of Significance of Included Variables in Explaining Sequence of Post-Acute Care Transitions (n = 341,065).
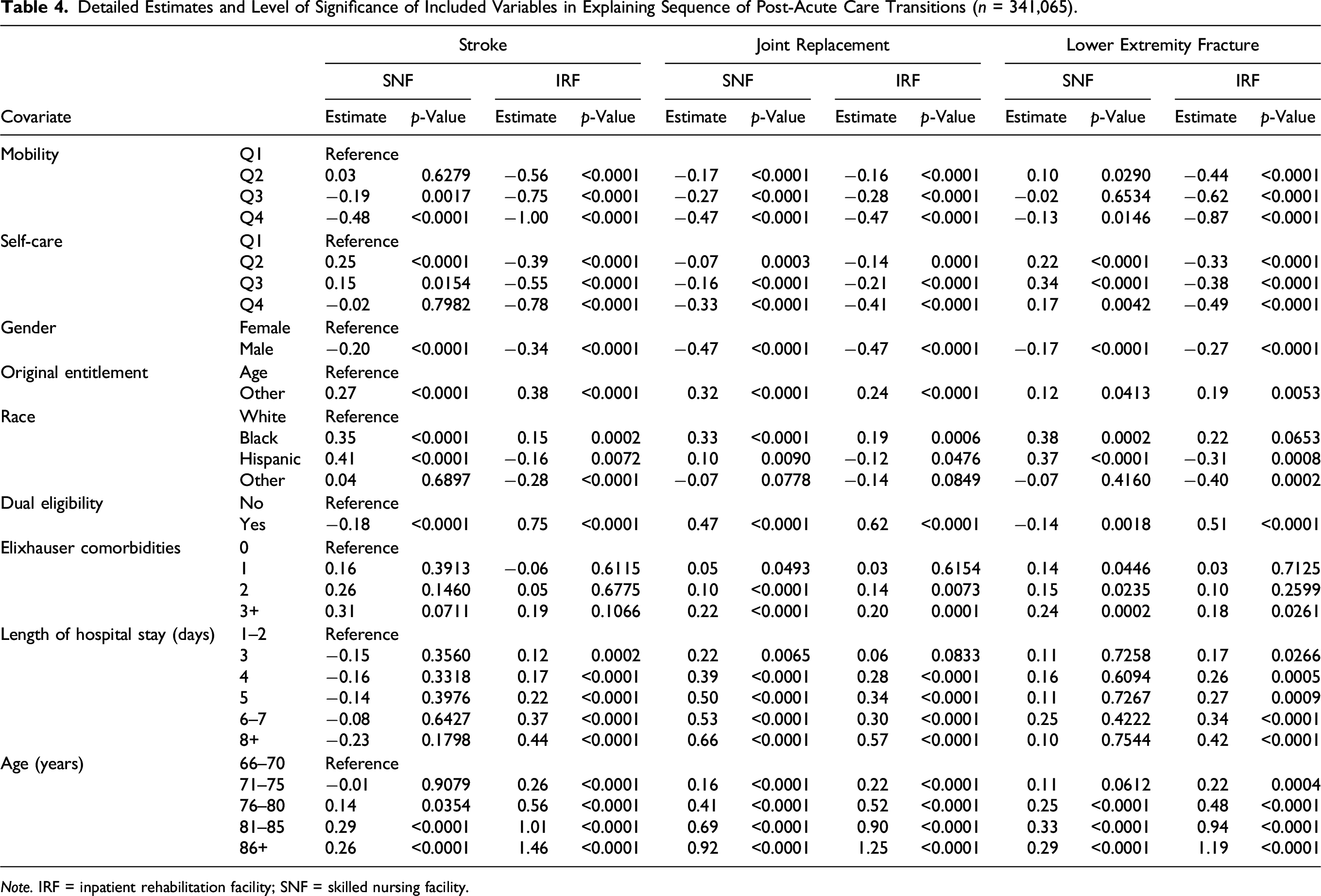
Note. IRF = inpatient rehabilitation facility; SNF = skilled nursing facility.
After adjusting for all patient-level covariates, the proportion of variance (%) decreased significantly across impairments. In the adjusted model for stroke, for patients who received their initial PAC in an inpatient rehabilitation facility, mobility explained 3.8% and self-care explained 2.7% of the variance in the sequence of PAC use; for those who initially received care at a skilled nursing facility, mobility explained 1.3% and self-care explained 0.9% of the variance (Table 3). In the adjusted model, for lower extremity joint replacement, mobility at both the initial inpatient rehabilitation facility and the initial skilled nursing facility explained 1.0% of the variance in the sequence of PAC use; self-care at both the initial inpatient rehabilitation facility and the initial skilled nursing facility explained 0.7% of the variance (Table 3). In the adjusted model, for hip/femur fracture, mobility at the initial inpatient rehabilitation facility explained 2.9% of the variance and self-care explained 1.7% of the variance in the sequence of PAC use, whereas mobility at the initial skilled nursing facility explained 0.4% and self-care explained 0.3% of the variance in the sequence of PAC use (Table 3).
Odds Ratios of One or More Post-Acute Care (PAC) Transitions Based on Functional Status at Initial PAC Setting (n = 341,065).
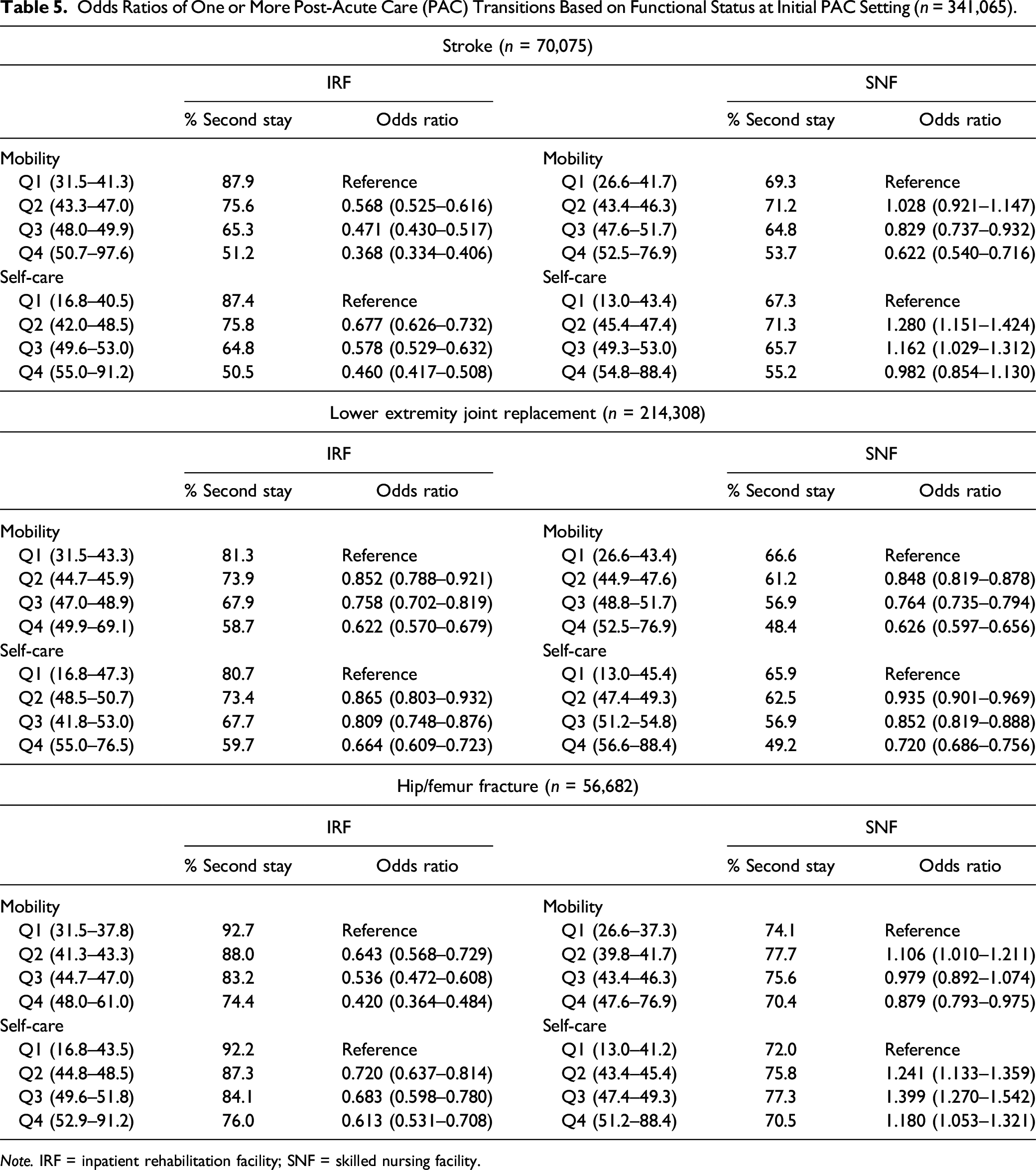
Note. IRF = inpatient rehabilitation facility; SNF = skilled nursing facility.
Discussion
Our study represents an early attempt to identify the role of function in the sequence of PAC transitions. This is the first study using co-calibrated functional scores across PAC settings to simulate the use of forthcoming standardized functional assessment (e.g. Section GG) across the PAC continuum. Our findings expand the current understanding of functional status and post-acute transitions. The findings show that Medicare beneficiaries are more independent in self-care than in mobility across three PAC settings and three impairments. Medicare beneficiaries discharged from acute care to a home health agency were overall the most independent in self-care and mobility, except for those with lower extremity joint replacement who were first discharged to a skilled nursing facility. The findings partially supported our original hypothesis, as higher functional scores at admission were associated with a lower likelihood of subsequent PAC transitions, but only for those who first went to an inpatient rehabilitation facility. Our study provides critical information for clinicians to optimize the provision of care and patients’ recovery during PAC stays and transitions.
Functional scores for patients using inpatient rehabilitation facilities explained more variance in subsequent PAC transitions than did those of the patients using skilled nursing facilities. CMS reported that 39% of Medicare beneficiaries in skilled nursing facilities were not cognitively impaired and 20% could function independently (Centers for Medicare & Medicaid Services, 2015), suggesting that high-functioning patients may be placed in the institutional setting rather than the home setting. Determining the underuse or overuse of post-acute resources is complicated and beyond the scope of this study. However, it is important to understand that proper post-acute placement may maximize patient outcomes such as self-care and mobility. Patients should receive the necessary care and services that meet with their needs across the post-acute continuum of care.
Our findings did not show that inpatient rehabilitation facilities had better functional outcomes than skilled nursing facilities for patients with joint replacement procedures, as did by DeJong et al. (2009). However, we found variation in transitions after the initial PAC setting was associated more with functional status in patients discharged from acute care to inpatient rehabilitation facilities than to skilled nursing facilities. The difference in findings could be due to variations in the use of functional scores, risk adjustment methods, patient characteristics, or study design, as well as the 10-year gap in data between studies. Our study also failed to find lower self-care function at inpatient rehabilitation facilities and home health agencies than skilled nursing facilities for patients with hip fracture (Mallinson, Deutsch, Bateman et al., 2014). This difference in findings may be due to the fact that we adjusted for length of hospital stays and length of post-acute stays (dominating factors in services use), and to the different study design of patient recruitment. In addition, we used co-calibrated scores from different functional assessments, and our patient characteristics also differed from those in the previous study (Mallinson, Deutsch, Bateman et al., 2014).
Our findings indicate that functional scores explain only a small portion of variation in one or more PAC transitions, after adjusting for the included covariates. In addition to the variation in functional status, many other factors may influence the selection and use of PAC services: the preferences of practitioners, patients, or caregivers; the local need and availability of certain types of care; the degree of family or social support; severity of the impairment; insurance coverage; hospital or provider characteristics; and the changing health-care practice landscape (Comondore et al., 2009; Dartmouth Atlas of Health Care, 2017; Graham et al., 2016; Horwitz et al., 2017; Li et al., 2017; Rahman et al., 2013). It is likely that patient transitions across care settings are mainly due to health reasons rather than functional reasons. We suggest that future studies compare how the above-listed additional factors influence PAC transitions. In addition, policy makers and practitioners need to be aware of and address barriers to care transition, such as poor quality discharge communication and inaccurate information exchange, to enhance the effectiveness of care transitions (King et al., 2013). We also suggest that future studies examine whether differences in functional scores across settings are clinically meaningful, as we found that co-calibrated functional scores at admission were relatively similar across PAC settings.
Changes in the health-care system (e.g., bundled, site-neutral, and value-based care and payments) are influencing how continuous care is delivered and what services patients will receive after discharge from the acute hospital. Choosing an efficient PAC service can help patients receive effective care planning (Leland et al., 2015). For clinicians, changes in the reimbursement system and health-care policy increase the importance of selecting the most appropriate PAC services for patients. Our findings serve as a baseline to understanding the continuous PAC experience in the context of the current health-care policy. Our findings provide guidelines to enable stakeholders (e.g., patients, clinicians, and policy makers) to optimize the recovery process of each patient across the continuum of care and inform the implementation of future policies.
Study Limitations
Our study has limitations associated with using claims data. The level of detail related to patient case-mix and condition severity may be limited (Cheng & Phillips, 2014). Our results are not applicable to persons younger than 66 years, those enrolled in managed care or private insurance plans, those admitted from a nursing facility, and those who did not use more than one PAC service. We are also aware that transitions between institutional settings (e.g. inpatient rehabilitation facilities to skilled nursing facilities) may differ as do those between an institution and home with home healthcare. In addition, we did not include cognitive function in our study. We were unable to develop a measure of cognition with adequate precision using our co-calibration approach. Future investigations should also examine longitudinal trends and include information on geographic and facility characteristics to improve the generalizability of our findings. We are also aware that we did not include other social determinants that may potentially affect the use of care, such as family support, social network, and personal finances. Finally, using functional scores at admission may correlate less with the second PAC setting than scores at discharge. However, a large proportion of patients with missing functional data (∼20%) at discharge limited the use of functional scores at discharge.
Conclusion
We examined the association between functional scores (self-care and mobility) at admission to the first PAC setting and the subsequent PAC transitions. Our study found that patients’ functional scores at admission to an inpatient rehabilitation facility explained more variance in subsequent PAC transitions than functional scores at admission to a skilled nursing facility. Identifying factors (facilitators and barriers) affecting functional status across PAC transitions could potentially improve recovery, stability of reimbursement, and the quality of health outcomes for the patients we serve.
Supplemental Material
SupplementaryFiles_2020_04_14 – Supplemental Material for Impact of Self-Care and Mobility on One or More Post-Acute Care Transitions
Supplemental Material, SupplementaryFiles_2020_04_14 for Impact of Self-Care and Mobility on One or More Post-Acute Care Transitions by Chih-Ying Li, Amol Karmarkar, Yong-Fang Kuo, Allen Haas and Kenneth J. Ottenbacher in Journal of Aging and Health
Footnotes
Appendix 1
Acknowledgments
The authors would like to acknowledge Trudy Mallinson, PhD, OTR, for her assistance to the research team in applying her developed crosswalk. The authors would also like to thank Sarah Toombs Smith, PhD, a board-certified editor in the Life Sciences (bels.org), at the Sealy Center on Aging, University of Texas Medical Branch, for her assistance in reviewing and editing the manuscript prior to submission.
Declaration of Conflicting Interests
All authors declare that they follow the International Committee of Medical Journal Editors (ICMJE) authorship guidelines and have no potential conflicts of interest with respect to the publication of this paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Ottenbacher is currently receiving grants (P2C HD065702, R01 MD010355 and K07-AG064031) from the National Center for Medical Rehabilitation Research (NICHD) and the National Institute on Minority Health and Health Disparities (NIMHD), National Institutes of Health (NIH) and National Institute of Aging (NIA). Dr Karmarkar is currently receiving a grant (K01HD086290) from the NICHD, NIH. Dr Li is currently receiving a grant (K01HD101589) from the NICHD, NIH. Dr Li received a pilot grant (P30-AG024832, PI: Dr Volpi) to conduct this study from the Claude D. Pepper Older Americans Independence Centers Award at the University of Texas Medical Branch, funded by the National Institute on Aging. For the remaining authors, none were declared.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.