
Abstract
Introduction
Physical inactivity is a leading risk factor for obesity and related comorbidities, including type 2 diabetes, coronary heart disease, and stroke (Reiner et al., 2013). Current guidelines for physical activity (PA) recommend that adults accumulate at least 150–300 minutes of moderate intensity or 75–150 minutes of vigorous-PA per week, in addition to at least 2 days per week of muscle-strengthening activities, to achieve health benefits (U.S. Department of Health and Human Services (HHS) & Office of Disease Prevention and Health Promotion, 2018). Yet, many adults are insufficiently active. Surveillance reports from the 2018 National Health Interview Survey indicated that 25.4% of adults engaged in no leisure-time PA, and only 24.0% of adults met both aerobic and muscle-strengthening activity recommendations (Centers for Disease Control and Prevention Centers for, 2013).
Habitual PA is associated with a more favorable body composition throughout the life course. Aging-related changes in body composition including increased fat mass and decreased skeletal muscle mass may be prevented or delayed with consistent engagement in PA (Cruz-Jentoft et al., 2014; Steffl et al., 2017). Sarcopenia and related decreases in muscle mass and strength are associated with poor lower-extremity physical functioning (PF) and mobility (Sowers et al., 2005, 2006). Thus, PA engagement, including regular exercise, is particularly important for midlife and older adults because it delays or mitigates age-related functional declines through maintenance of muscle mass and strength, gait speed, and balance. Once functional impairments begin, individuals may have physical difficulty with engaging in PA and thus become less active.
Paradoxically, however, the literature on PA and falls is somewhat mixed. Some work suggests that PA increases the risk of falls because PA participation increases the opportunity to fall (Bea et al., 2017). Individuals with high levels of PA but poor PF may be at high fall risk due to an increased opportunity to fall during activity coupled with poor compensatory mechanisms like strength and balance to navigate an environmental challenge. Conversely, a recent report from the Women’s Health Initiative (WHI) demonstrated increased fall risk in older ambulatory women (mean age 79 years ± 6.7) with low PA and low PF but not an increased fall risk for women with high PA (Buchner et al., 2017). This work supports the importance of PF and suggests that unique phenotypes of PA engagement and functional status (e.g., low PA and low PF; high PA and low PF) may be important indicators of fall risk. This work should be replicated in younger women as findings from the Behavioral Risk Factor Surveillance System indicate that women aged 55–64 years report more falls and injurious falls than either younger or older women and all men (Ylitalo & Karvonen-Gutierrez, 2016).
The purpose of this study is to identify PA and PF characteristic groups (i.e., “phenotypes”) and describe the relationship of phenotypes and falls among women in late midlife (60–65 years) or early late adulthood (65–70 years) in the Study of Women’s Health Across the Nation (SWAN). We hypothesized that we would observe a trend in the association between phenotypes and falls such that women classified as having both high PA and high PF would report the lowest fall incidence, with increasingly higher fall incidence for the low PA and high PF group, the high PA and low PF group, and finally the low PA and low PF group.
Methods
Study Population
The Study of Women’s Health Across the Nation is a prospective, multicenter, multiethnic study of the menopause transition and aging. Sampling and recruitment methods have been described previously (Sowers et al., 2000). Briefly, 3302 women who at the 1996 baseline were aged 42–52 years, premenopausal, and self-identified with site-designated race–ethnic groups were recruited from seven locations (Boston, Chicago, Detroit, Los Angeles, New Jersey, Oakland, and Pittsburgh) for a longitudinal study (Sowers et al., 2000). Near-annual study visits provided clinical and behavioral data. For this analysis, participants with complete questionnaire data for PF and PA at both visit 12 (V12, 2012–2013) and visit 15 (V15, 2016–2017) and fall data at V15 were included. The final analytic sample for the present article was n = 1597 (48.4% of baseline) participants with complete data. Compared with the analytic sample, excluded women were similar in age but more likely to be Hispanic or African American (p < .001) and have a high school education or less (p < .001).
Measures
Falls were measured at visit 15 by self-report: “During the past year, have you fallen and landed on the floor or ground (or fallen and hit an object like a table or stair)?” If affirmative, two follow-up questions were asked: “How many times have you fallen in the past year?” and “During the past year, were you injured in any of these falls?” Women who reported an injury were additionally asked about the type of injury (broken or fractured bone, head injury, sprain or strain, bruises, or bleeding). Recurrent falls were defined as ≥2 falls during the previous year.
PF was measured by self-report from the 10-item PF subscale of the Medical Outcomes Survey Short Form (SF-36) (Ware & Sherbourne, 1992). The PF subscale demonstrates two-week test–retest reliability (intraclass correlation coefficient = .81) and substantial construct validity (Brazier et al., 1992). Participants reported whether they were limited a lot, a little, or not limited at all in vigorous or moderate activities, lifting/carrying groceries, climbing stairs, bending/kneeling/stooping, walking, bathing, and dressing. Responses were scored and transformed to a normalized range of 0–100. High scores indicate better PF. Previously used cut points were used to define no limitations (scores 86–100), some limitations (51–85), or substantial limitations (0–50) (Rose et al., 1999; Ylitalo et al., 2013).
PA was measured by self-report using the Kaiser Physical Activity Survey (KPAS), an adaptation of the Baecke questionnaire designed specifically for women (Ainsworth et al., 2000). For the sports and exercise domain, participants were asked to report up to two sports or exercise activities performed most frequently over the previous 12 months. The KPAS sports and exercise domain demonstrates 1-month test–retest reliability (intraclass correlation coefficient = .84) and reasonable accuracy compared to O2 peak (Spearman correlation = .76; Ainsworth et al., 2000). Surveys obtained information about the activity type (open-ended), frequency (months in the previous 12 months), and duration (hours per week). Open-ended responses to primary and secondary sports/exercise activities were categorized into 65 groups and assigned a general metabolic equivalent of a task (MET) value using the Compendium of Physical Activities (Ainsworth et al., 2020). MET values were multiplied by frequency and duration to calculate average MET minutes per week. While the traditional KPAS scoring results in an index score ranging from 1 (low) to 5 (high), the sports and exercise domain was rescored and summarized as MET minutes per week in order to provide a more physiologically meaningful estimate.
High PA (≥450 MET minutes/week) and low PA (<450 MET minutes/week) were dichotomized based on the duration and intensity PA guidelines for adults in the United States (U.S. Department of Health and Human Services (HHS) & Office of Disease Prevention and Health Promotion, 2018). High PF (SF-12 scores ≥ 86, “no limitations”) and low PF (SF-12 scores < 86, “some or substantial limitations”) were dichotomized. We defined four “phenotypes,” or groups with similar characteristics, based on PF and PA clusters: (1) high PA and high PF, (2) high PA and low PF, (3) low PA and high PF, and (4) low PA and low PF.
Other covariates were intrinsic risk factors for falls (Institute of Medicine (US) Division of Health Promotion and Disease Prevention et al., 1992) and were selected a priori based on their known associations with falls. Covariates included age, race/ethnicity, educational attainment, marital status, socioeconomic status, body mass index (BMI), smoking status, alcohol consumption, depressive symptoms, osteoarthritis, and diabetes status. Height was measured without shoes in centimeters by a fixed stadiometer, and weight was measured in light clothing in kilograms by a balance beam scale. Body mass index was calculated as weight [kg]/height [m2] and categorized as underweight or normal weight (BMI ≤ 24.9 kg/m2), overweight (BMI 25–29.9 kg/m2), and obese (BMI ≥ 30 kg/m2) for non-Hispanic white, African American, and Hispanic women. We used Asian-specific cut points, categorized as underweight or normal weight (BMI < 23 kg/m2), overweight (BMI 23–24.9 kg/m2), and obese (BMI ≥ 25 kg/m2), for Japanese and Chinese women (Wee et al., 2010; WHO Expert Consultation, 2004; Woo et al., 2007). For all race–ethnic groups, the underweight/normal weight group was used as the reference. Diabetes status was defined using self-report of a physician diagnosis of diabetes, current use of diabetes medications, or, when available, a fasting blood glucose ≥126 mg/dL from visit 13. Smoking status was defined as current smoking (yes or no). Alcohol consumption was measured by self-report and categorized as none or ≤1 drink/month, >1 drink/month to <2 drinks/week, or ≥2 drinks/week. Depressive symptoms were ascertained using the Center for Epidemiological Studies Depression Scale (CES-D) and categorized as depressive symptoms (CES-D ≥16) or no depressive symptoms (CES-D <16) (Radloff, 1977).
Statistical Analysis
Data management and analyses were conducted using SAS v9.4 (SAS Institute, Inc, Cary, NC). Means (SD) or frequencies and proportions were reported for all variables of interest. Sociodemographic and health-related characteristics were compared by fall status using Student t-tests for continuous variables and chi-square tests for categorical variables. We identified four mutually exclusive PA–PF phenotypes at visit 12. Sociodemographic and health-related characteristics were also compared across phenotypes using generalized linear models for continuous variables and chi-square tests for categorical variables. Unadjusted and adjusted Poisson regression was performed using PROC GENMOD to generate risk ratios (RRs) and corresponding 95% confidence intervals (CIs) for binary fall outcomes. We evaluated the association of visit 12 phenotypes with visit 15 falls and visit 12 to visit 15 PA or PF change with visit 15 falls.
Results
Sociodemographic and health-related characteristics at visit 15 in total sample and by any fall status.
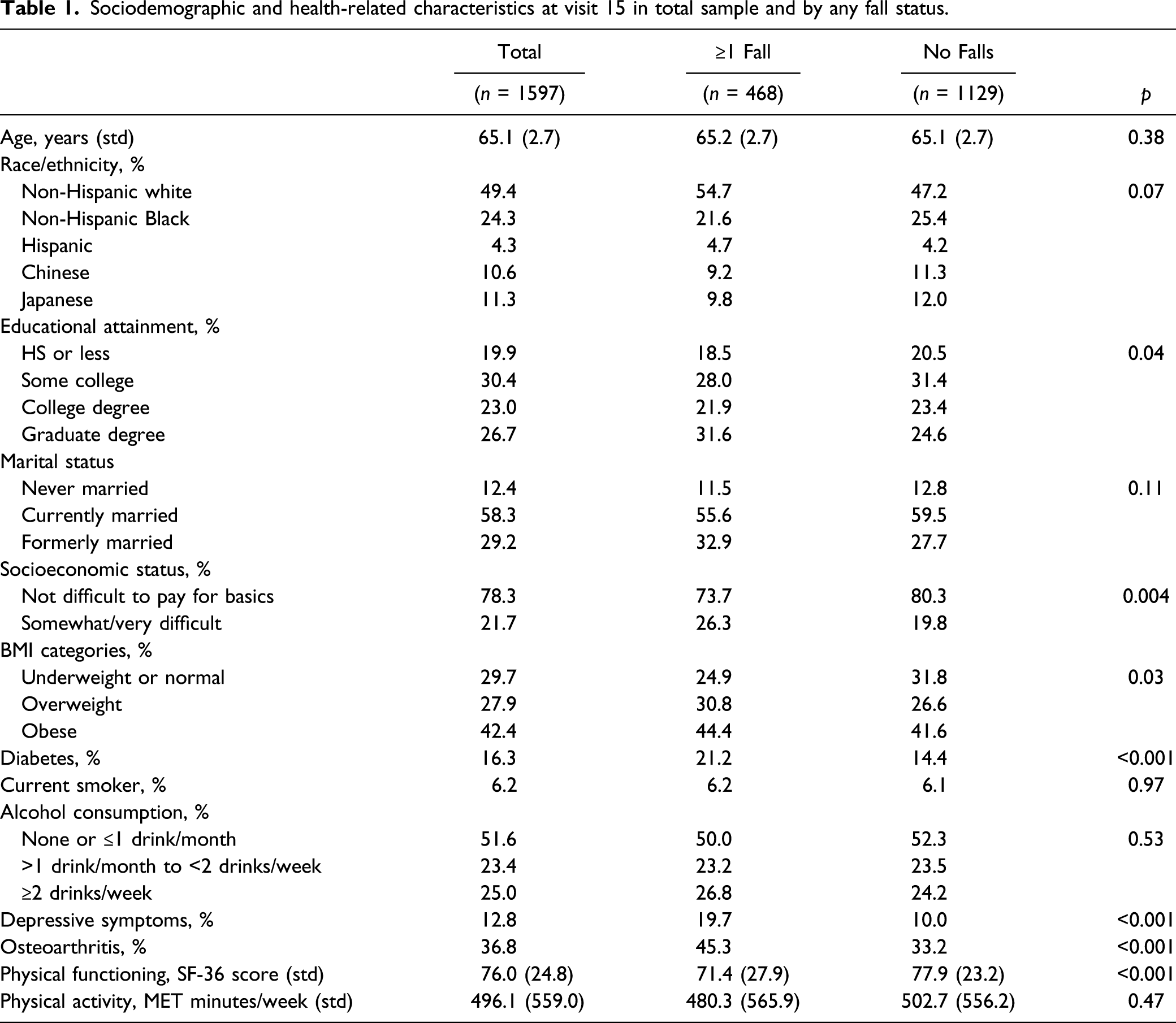
At study visit 15, 29.3% (n = 468) of participants reported ≥1 fall in the previous year, 12.2% (n = 195) reported ≥2 falls (i.e., “recurrent falls”), and 8.0% (n = 128) reported recurrent falls with at least one injury. Among participants with recurrent falls, 17 reported a broken or fractured bone. Non-fracture fall injuries were common among the 128 women with recurrent injurious falls: 46 reported sprain/strain, 109 reported bruise, and 37 reported bleeding.
Participants who reported ≥1 fall were statistically significantly more likely to report difficulty paying for basics; be overweight or obese; and have diabetes, depressive symptoms, and poor PF. There were no statistically significant differences in fall status by age, race/ethnicity, marital status, smoking or alcohol consumption, or self-reported PA (Table 1).
Sociodemographic and health-related characteristics by phenotypes at visit 12.
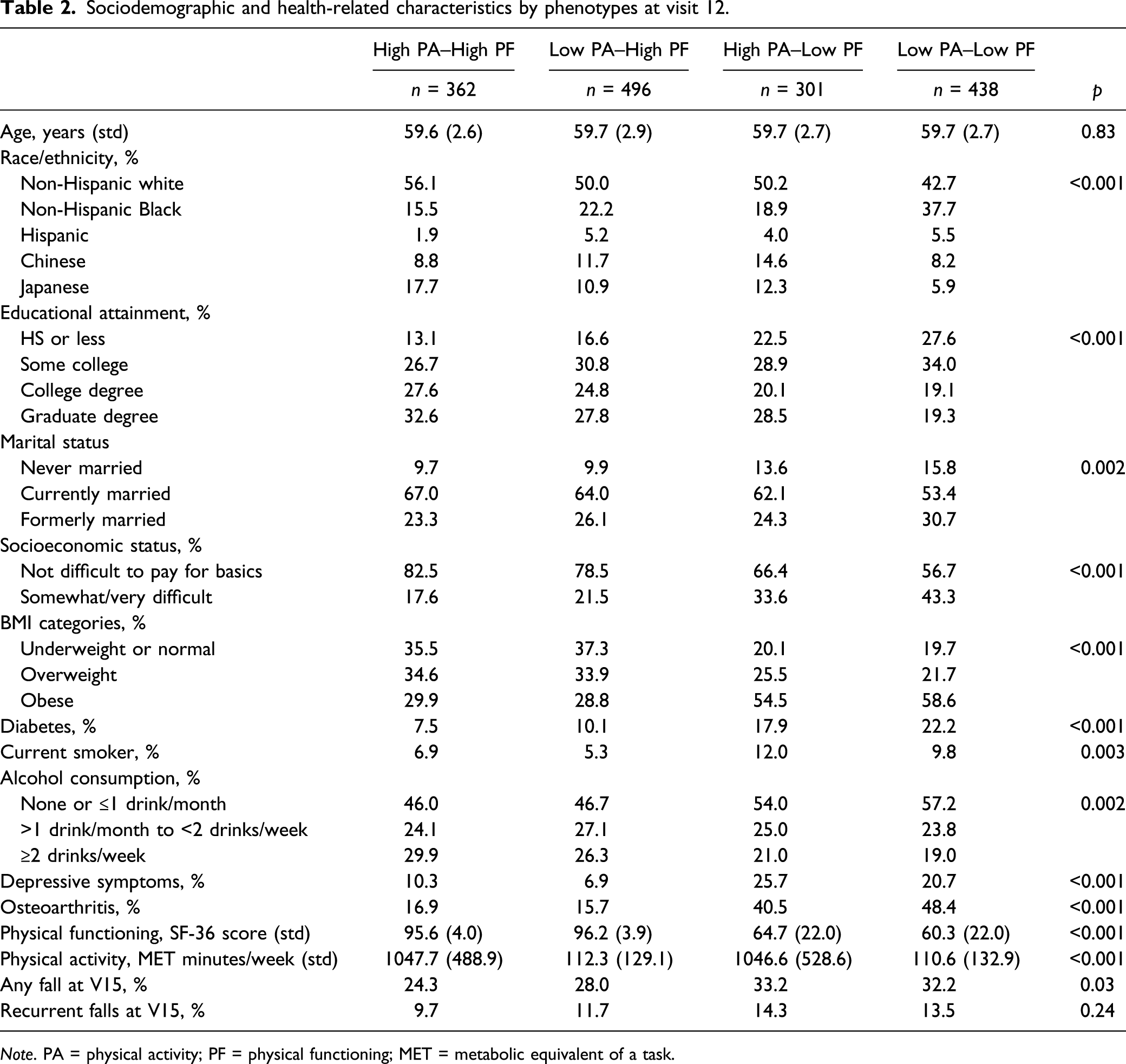
Note. PA = physical activity; PF = physical functioning; MET = metabolic equivalent of a task.
Relationship of physical activity and physical functioning phenotypes with fall outcomes at visit 15.
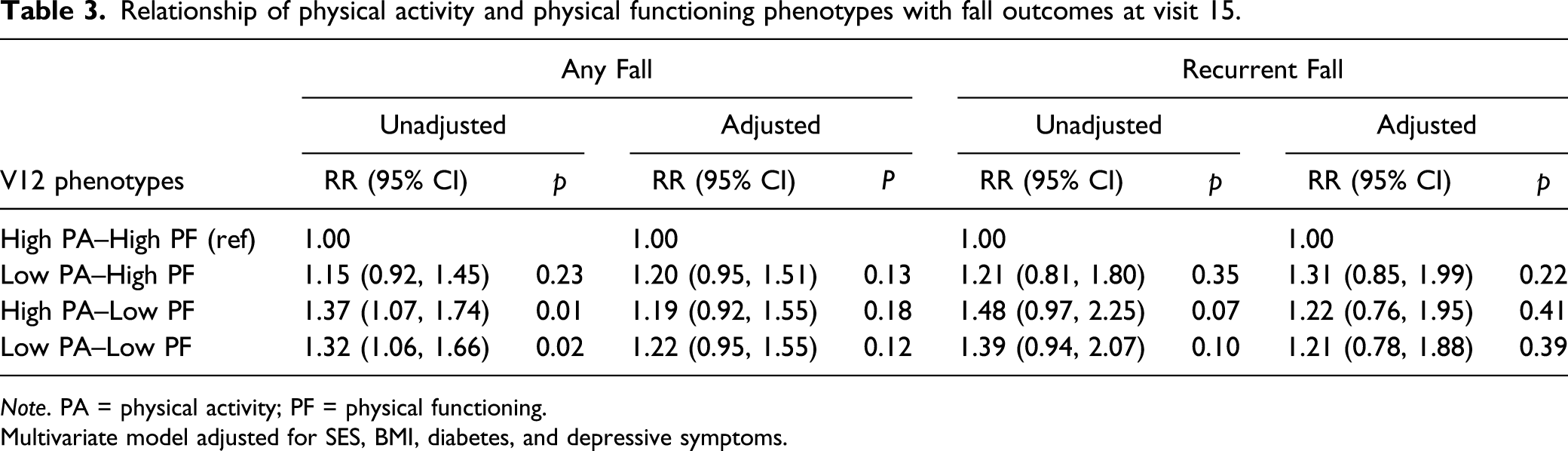
Note. PA = physical activity; PF = physical functioning.
Multivariate model adjusted for SES, BMI, diabetes, and depressive symptoms.
Relationship of physical activity and physical functioning change (V12 to V15) with fall outcomes at visit 15.
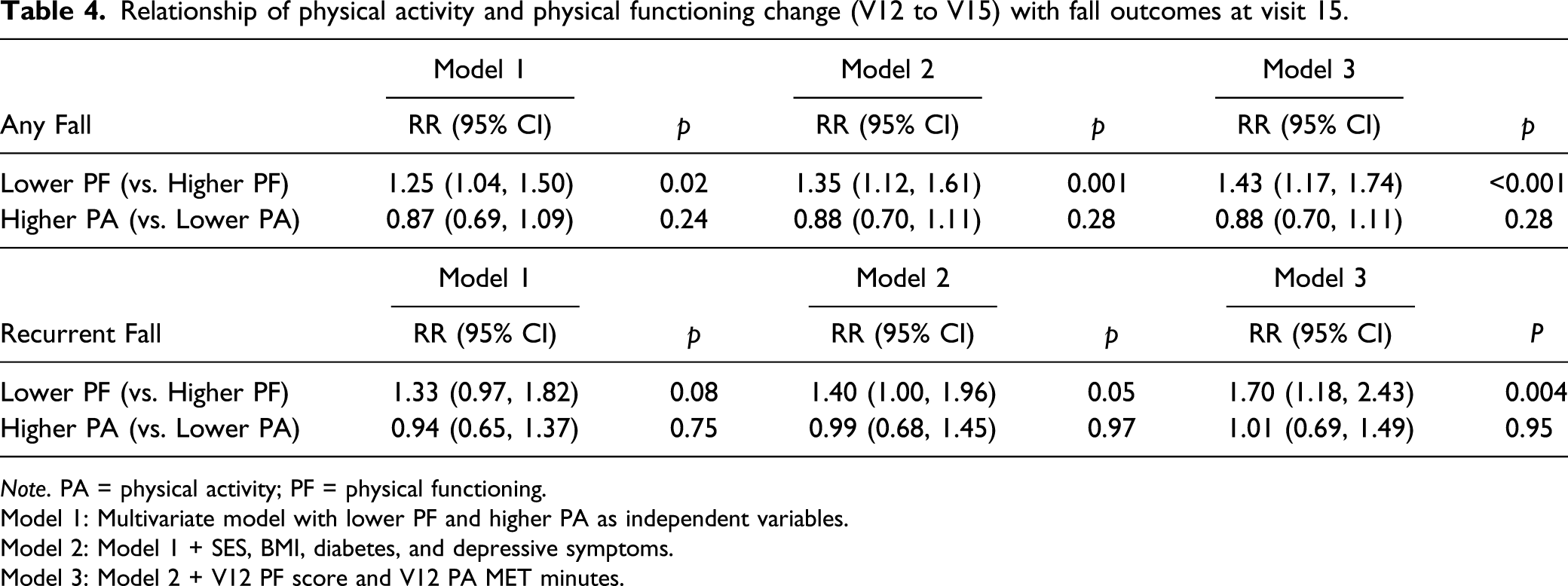
Note. PA = physical activity; PF = physical functioning.
Model 1: Multivariate model with lower PF and higher PA as independent variables.
Model 2: Model 1 + SES, BMI, diabetes, and depressive symptoms.
Model 3: Model 2 + V12 PF score and V12 PA MET minutes.
Discussion
The purpose of this study was to identify PA and PF phenotypes and describe the relationship of phenotypes and fall outcomes in late midlife and early old age women. Although we expected a large proportion of women to be classified as highly active without functional limitations or highly inactive with functional limitations, we also observed that approximately half of our sample had discordant levels of PA and PF. We hypothesized that discordant phenotypes (e.g., low PA high PF; high PA low PF) would be at greater fall risk than women with high PA and high PF. However, we observed that only the low PF groups were associated with falls, and this association was mitigated after adjustment for covariates. Nevertheless, the four PA and PF phenotypes appeared to identify important patterns in health profiles, particularly for cardiometabolic factors like BMI and diabetes status. Over time, women who experienced declines in PF phenotype categories had a significantly increased risk of falls, but women who increased PA phenotype categories did not have increased risk of falls. These findings suggest that women can engage in PA to the extent they are able without increasing fall risk, even for women with functional limitations.
Current guidelines for PA engagement recommend that adults accumulate at least 150–300 minutes a week of moderate intensity or 75–150 minutes of vigorous intensity aerobic activity each week; adults with chronic conditions or disabilities should meet these recommendations as they are able to “avoid inactivity” (U.S. Department of Health and Human Services (HHS) & Office of Disease Prevention and Health Promotion, 2018). Although current guidelines state that PA benefits for older adults include reduced risk of fall-related injuries, the literature suggests a somewhat more complicated relationship (U.S. Department of Health and Human Services (HHS) & Office of Disease Prevention and Health Promotion, 2018). In the Osteoporotic Fractures in Men Study, age modified the association between PA and falls (Cauley et al., 2013). In men <80 years, those with the lowest energy expenditure had a lower risk of falling; in men >80 years, those with the lowest energy expenditure had a higher risk of falling (Cauley et al., 2013). Absolute differences in PA by fall status, while statistically significant, were small (Cauley et al., 2013). In the Baltimore Longitudinal Study of Aging, there were no differences in total daily PA between fallers and nonfallers (Nastasi et al., 2018). “Risky” fallers, defined as participants who fell while riding a bike, hiking, doing yard work, etc., had higher PA, better balance, and better PF than “normal” fallers, which emphasizes the importance of functional limitations (Nastasi et al., 2018). In the WHI observational study, increases in PA over time were associated with increased fall risks among women aged 50–79 years (Bea et al., 2017). Likewise, in the Hispanic Established Populations for Epidemiologic Study of the Elderly study, high levels of PA with low levels of PF were associated with increased fall risk among older (mean age 82.3 years ± 4.6) Mexican American adults over time (Lewis et al., 2016). In our study of adult women (65.1 years ± 2.7), poor PF increased the risk of falls for women. Women who increased PA participation over time did not have increased fall risk, even when adjusting for PF. Our work is consistent with more recent work from the WHI that suggests falls are not more common for older adult women who participate in higher levels of moderate- to vigorous-intensity PA (Buchner et al., 2017). These findings underscore the importance of PA engagement throughout the life course, even for women with PF limitations.
PA has numerous health benefits, including the slowing of aging-related declines in PF (Dugan et al., 2018; Manini & Pahor, 2008). Women report more disability than men at every age, but women who maintain at least moderate PA engagement demonstrate better PF than those who maintain low PA (Freedman et al., 2016; Gabriel et al., 2017). PF maintenance throughout the life course is important, particularly for women. In our study, phenotypes with low PF, regardless of PA level, had poorer health than phenotypes with high PF. Women in both the high PA and low PF and the low PA and low PF groups had disproportionately higher obesity, diabetes, depressive symptoms, and osteoarthritis at both time points.
PF limitations are dynamic, and the critical midlife period for women is characterized by changes in functional limitations, suggesting that adults can experience both improvement and worsening of functional status (Ylitalo et al., 2013). PF has been posited as the “sixth vital sign” and easy-to-use assessments like the self-reported SF-12 may be useful in the clinical setting to identify older adults at high fall risk (Bierman, 2001; Richardson et al., 2012). Our findings suggest that declines in PF—and specifically, a categorical change from no limitations in PF to some or substantial limitations in PF on the SF-12 questionnaire—are significantly associated with fall risk, regardless of PA engagement. This finding provides further support for evaluation of PF to identify those at higher risk of falls. Based on our results, poor PF, even if coupled by high PA engagement, increases risk of falls. Thus, while PA is beneficial and should continue to be encouraged, consideration of both PA and PF is critical among aging populations. Furthermore, we observed that women who increase PA over time—for example, begin to meet PA guidelines—do not have a greater fall risk in early old age women, even after accounting for PF limitations. Our findings are consistent with Buchner et al. which demonstrated that women with high PA were not more likely to fall (Buchner et al., 2017). Thus, even in individuals with PF limitations, PA should be encouraged, consistent with recommendations to participate in activities according to abilities and to limit inactivity (U.S. Department of Health and Human Services (HHS) & Office of Disease Prevention and Health Promotion, 2018).
This study has several limitations. First, although short-term recall of fall events is moderately accurate, our use of a 12-month recall period may underestimate the incidence of falls. Future work should consider more frequent fall calendars to increase the recall of fall events. We focused our work on intrinsic risk factors for falls, yet a fall is the result of intrinsic and extrinsic factors (Institute of Medicine, 1992). Accordingly, future work should consider fear of falling and fall circumstances to measure situational and/or environmental hazards. We have a robust set of covariates, but we may have unmeasured confounding. Although we included several measures of fall outcomes including recurrent falls, we were limited in our statistical power to detect differences in recurrent falls across the four phenotypes. Our main analyses used self-reported PA because only self-reported data were available at both time points of interest. Although we used meaningful categorizations, we also conducted a sensitivity analysis with PA and PF as continuous variables and found similar results. Compared to the original baseline cohort, participants excluded from our analytic sample were more likely to be Hispanic or African American and have a high school education or less. Finally, future work should include a closer examination of device-based PA, specifically because devices can distinguish intensity level of activity.
Conclusion
PA, including regular exercise, delays or mitigates age-related functional declines. Even among women with poor PF, increasing PA does not appear to increase the risk of falls among late-midlife and early old-age women, suggesting that women can engage in PA to the extent they are able. Falls are a major public health concern, particularly for older adult women. Given the widely appreciated benefits of PA on many age-related health domains, including long-term benefits for physical function, women should be encouraged to engage in PA throughout the life course.
Supplemental Material
sj-pdf-1-jah-10.1177_0898264320988405 – Supplemental Material for Association of Physical Activity and Physical Functioning Phenotypes With Fall Risk Among Women
Supplemental Material, sj-pdf-1-jah-10.1177_0898264320988405 for Association of Physical Activity and Physical Functioning Phenotypes With Fall Risk Among Women by Kelly R. Ylitalo, Carrie A. Karvonen-Gutierrez, Barbara Sternfeld and Kelley Pettee Gabriel in Journal of Aging and Health
Footnotes
Acknowledgments
Clinical Centers: University of Michigan, Ann Arbor – Siobán Harlow, PI 2011 – present, MaryFran Sowers, PI 1994–2011; Massachusetts General Hospital, Boston, MA – Joel Finkelstein, PI 1999 – present; Robert Neer, PI 1994–1999; Rush University, Rush University Medical Center, Chicago, IL – Howard Kravitz, PI 2009 – present; Lynda Powell, PI 1994–2009; University of California, Davis/Kaiser – Ellen Gold, PI; University of California, Los Angeles – Gail Greendale, PI; Albert Einstein College of Medicine, Bronx, NY – Carol Derby, PI 2011 – present, Rachel Wildman, PI 2010–2011; Nanette Santoro, PI 2004–2010; University of Medicine and Dentistry – New Jersey Medical School, Newark – Gerson Weiss, PI 1994–2004, and the University of Pittsburgh, Pittsburgh, PA – Karen Matthews, PI.
NIH Program Office: National Institute on Aging, Bethesda, MD – Chhanda Dutta 2016 – present; Winifred Rossi 2012–2016; Sherry Sherman 1994–2012; Marcia Ory 1994–2001; National Institute of Nursing Research, Bethesda, MD – Program Officers.
Central Laboratory: University of Michigan, Ann Arbor – Daniel McConnell (Central Ligand Assay Satellite Services).
Coordinating Center: University of Pittsburgh, Pittsburgh, PA – Maria Mori Brooks, PI 2012 – present; Kim Sutton-Tyrrell, PI 2001–2012; New England Research Institutes, Watertown, MA - Sonja McKinlay, PI 1995–2001.
Steering Committee: Susan Johnson, Current Chair; Chris Gallagher, Former Chair.
We thank the study staff at each site and all the women who participated in SWAN.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Study of Women’s Health Across the Nation (SWAN) has grant support from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR), and the NIH Office of Research on Women’s Health (ORWH) (Grants U01NR004061; U01AG012505, U01AG012535, U01AG012531, U01AG012539, U01AG012546, U01AG012553, U01AG012554, U01AG012495). The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the NIA, NINR, ORWH, or NIH. K.R.Y. is supported by NIA under Award Number K01AG058754. C.K.G. is supported by NIA under Award Number K01AG054615.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.