
Abstract
Objectives
We examined the associations between state-level policies and the health of lesbian, gay, bisexual, and transgender (LGBT) older adults.
Keywords
The Healthy People 2020 report identified the health, safety, and well-being of lesbian, gay, bisexual, and transgender (LGBT) individuals as a public health priority in the United States, with a particular emphasis on national objectives aimed to improve the health of LGBT older adults (US Department of Health and Human Services, 2011). Research has found ample evidence that, compared to heterosexual and/or cisgender older adults, LGBT older adults are more likely to report poor general health (Conron et al., 2010; Dilley et al., 2010; Fredriksen-Goldsen et al., 2012; Fredriksen-Goldsen et al., 2017; Fredriksen-Goldsen, Kim, et al., 2013), functional limitations or disability (Blosnich et al., 2014; Conron et al., 2010; Fredriksen-Goldsen et al., 2012; Fredriksen-Goldsen et al., 2017; Fredriksen-Goldsen, Kim, et al., 2013), chronic conditions (Fredriksen-Goldsen et al., 2017; Hoy-Ellis & Fredriksen-Goldsen, 2016; Nelson & Andel, 2020), and poor mental health (Blosnich et al., 2014; Conron et al., 2010; Dilley et al., 2010; Fredriksen-Goldsen et al., 2017).
The minority stress theory posits that LGBT people face additional stressors that negatively impact their physical and mental health (Meyer, 2003). Anticipating or experiencing minority stressors such as stigma, prejudice, and discrimination have been found to be associated with increased risk of poor physical and mental health outcomes in LGBT older adults (Fredriksen-Goldsen, Emlet, et al., 2013; Fredriksen-Goldsen et al., 2015; Hoy-Ellis & Fredriksen-Goldsen, 2016; Valentine & Shipherd, 2018). However, most research has assessed the associations between individual-level minority stressors (e.g., internalized homonegativity, and microaggressions) and health in LGBT older adults; fewer studies have examined the associations between societal-level minority stressors (e.g., lack of legal protection against discrimination) and the health of LGBT older adults.
In the United States, there is currently no federal law that provides comprehensive legal protections against discrimination for LGBT people of any age. On June 15, 2020, the Supreme Court ruled that the Civil Rights Act includes protection from employment discrimination based on sexual orientation and gender identity. However, without a federal law (e.g., The Equality Act) that would extend protections to other areas such as federally funded programs, housing, education, and credit, LGBT individuals in the United States face varying degrees of structural discrimination from state-level laws and policies. This is a serious concern because it is well-documented that structural discrimination, defined as “societal-level conditions, cultural norms, and institutional policies that constrain the opportunities, resources, and well-being of the stigmatized” (Hatzenbuehler, 2014; Hatzenbuehler & Link, 2014), is associated with LGBT adults’ physical and mental health (Gonzales & Ehrenfeld, 2018; Hatzenbuehler et al., 2010, 2012; Perez-Brumer et al., 2015).
Research has found that living in states with protective LGBT-related policies (e.g., legal recognition of same-sex marriage and inclusive nondiscrimination laws) was associated with less minority stress and a more supportive environment for lesbian, gay, and bisexual (i.e., sexual minority) adults (Hasenbush et al., 2014; Riggle et al., 2010). In fact, state-level sexual minority climate index and subjective friendliness are positively associated with sexual minority adults’ health and routine health care utilization (Solazzo et al., 2018). Conversely, existing research has also found that sexual minority adults living in states with fewer protective policies were at greater risk of poor mental and physical health. For instance, Hatzenbuehler et al. (2010) found that sexual minority adults living in states that banned gay marriage between two waves of data collection experienced significant increases in rates of psychiatric disorders (e.g., anxiety, alcohol use). Another study found that disparities in self-rated health were particularly prominent between sexual minority adults and their heterosexual counterparts in states with limited protections against discrimination (Gonzales & Ehrenfeld, 2018).
Structural discrimination additionally impacts transgender adults’ health. Transgender adults are individuals whose gender identity does not correspond to their birth sex. Geographic differences in access to health care were found for transgender adults in the United States; a higher percentage of conservative voting practices was strongly associated with healthcare providers’ refusal to provide appropriate care to transgender adults (White Hughto et al., 2016). Moreover, lower structural discrimination has been found to be associated with fewer lifetime suicide attempts among transgender adults (Perez-Brumer et al., 2015). Together, laws and policies that address legal protections based on sexual orientation and gender identity can benefit the overall health of LGBT individuals and their broader communities.
Our study builds on previous literature linking structural stigma to LGBT health because most previous studies excluded transgender individuals from their samples and to our knowledge, only one study (Perez-Brumer et al., 2015) has examined the association between structural stigma and health in people who identify as transgender. It is critical to understand more about this association because transgender adults routinely face structural stigma through policies that restrict access to transgender-inclusive healthcare or insurance as well as through policies that do not allow the changing of gender markers on driver’s licenses or birth certificates (Hughto et al., 2015). Furthermore, our study builds on existing literature because previous studies focused primarily on younger adults (under 50 years old). Studies that did include older adults did not examine age-group differences (Gonzales & Ehrenfeld, 2018; Hatzenbuehler et al., 2010; Solazzo et al., 2018). Lesbian, gay, bisexual, and gay older adults aged 50 and older have experienced many LGBT-related policy changes throughout their lives and their health may be affected differently by structural discrimination than younger LGBT adults. Due to a lack of legal protections, LGBT middle-aged and older adults have expressed concerns about end-of-life preparations (de Vries et al., 2009) as well as fears of discrimination in healthcare and long-term care communities (Czaja et al., 2016; Putney et al., 2018), resulting in a reluctance to use health services and supports. Therefore, researching the effect of structural discrimination on the physical and mental health of older LGBT adults is crucial to fully understanding health disparities in older cohorts of LGBT adults.
The current study examined the associations between the amount of enacted state-level LGBT-related policies (e.g., religious exemption laws, hate crime laws, employment nondiscrimination policies, ability for transgender people to correct name, and gender markers on identity documents; see https://www.lgbtmap.org/equality-maps for full list of policies) and the health of LGBT older adults. Sexual orientation and gender identity are separate constructs with unique issues; therefore, cisgender sexual minority older adults and transgender non-sexual minority older adults were assessed separately in this study. This study had two aims: (1) to examine differences in the physical and mental health of sexual minority and transgender older adults by the percentage of enacted state-level LGBT-related policies in their state of residence, and (2) to examine differences in the physical and mental health of the propensity score matched heterosexual and cisgender groups as a comparison for the sexual minority and transgender groups, respectively.
Based on data from the Movement Advancement Project (2021), participants in this study were grouped based on the total amount of points earned for each enacted LGBT-related policy in the state in which they reside; protective policies earned a positive tally point and harmful policies earned a negative tally point. We hypothesized that sexual minority participants from low tally states (<0–49.9% of possible points for enacted LGBT-related policies) would report poorer health than sexual minority participants from high tally states (50–100% of possible points for enacted LGBT-related policies). Similarly, we hypothesized that transgender participants from low tally states would report poorer health than transgender participants from high tally states. Finally, we hypothesized that heterosexual and cisgender participants from low tally states would not report significantly poorer health than heterosexual and cisgender adults from high tally states.
Methods
We used data from the 2018, 2019, and 2020 Behavioral Risk Factor Surveillance System (BRFSS) annual surveys (Centers for Disease Control and Prevention, 2019). The BRFSS survey is conducted annually by the Center for Disease Control and Prevention (CDC) by telephone in all 50 states, completing more than 400,000 interviews with adults each year. For this study, participants 50 years or older from the states that used the Sexual Orientation and Gender Identity (SOGI) module were included in the analyses. In total, 41 states used the SOGI module during the 2018–2020 annual surveys, resulting in data from 10,032 sexual minority and 1,072 transgender participants. For the current study, we also created a 1:1 propensity matched heterosexual (n = 10,032) and a 1:1 propensity matched cisgender group (n = 1,072) for comparison with the sexual minority and transgender groups, respectively.
Measures
Outcome Measures
The dependent variables for this study were three health measures that assessed general health and the number of days when physical and mental health was not good in the past 30 days. Responses for self-rated general health were dichotomized into two groups by BRFSS coders: good or better (good, very good, and excellent) general health and fair or poor general health. For the physical and mental health measures, participants were asked how many days during the past 30 days their physical health (including physical illness and injury) was “not good” and how many days their mental health (including stress, depression, and problems with emotions) was “not good.” For both the physical and mental health measures, BRFSS coders categorized responses into three groups: zero days, 1–13 days, and 14 or more days when physical/mental health was not good.
Sexual Orientation
Participants were asked to select the sexual orientation that best represented how they thought of themselves: lesbian or gay, straight/not gay, bisexual, or something else. For this study, gay, lesbian, and bisexual men and women were combined into the sexual minority group. The sexual minority and heterosexual (i.e., straight/not gay) groups were limited to participants that identified as cisgender.
Gender Identity
Participants were asked if they considered themselves to be transgender. All transgender participants (male-to-female, female-to-male, and gender non-conforming) were combined into one group. Those who responded “no” to this question were grouped into the cisgender category. Participants that identified as a sexual minority were excluded from the transgender and cisgender groups to avoid confounding effects.
State-Level LGBT-Related Policy Tally
We used data from the Movement Advancement Project (MAP), specifically The Equality Maps (Movement Advancement Project, 2021) to create policy tally categories based on the amount of enacted state-level LGBT-related policies. The Equality Maps tallied the number of LGBT-related laws and policies that help drive equality (out of nearly 40 as of January 1, 2020) within each state. Each law or policy earned a tally point, ranging from −1 to 1. Laws and policies that are protective for LGBT people received a positive tally. Laws and policies that are harmful to LGBT people received a negative tally. Some laws apply only to sexual orientation (e.g., marriage for same-sex couples) or gender identity (e.g., changing gender markers on identity documents) while others apply to both sexual orientation and gender identity (e.g., housing nondiscrimination laws). Laws that apply to both sexual orientation and gender identity received separate tallies as some states may have protections for sexual minority people but not for transgender people. The total possible points were 42.5 points, 20.5 for sexual orientation-related policies, and 22 for gender identity-related policies.
Forty-one states in the 2018, 2019, and 2020 BRFSS annual surveys included the Sexual Orientation and Gender Identity module. For this study, these 41 states were grouped according to the number of enacted LGBT-related laws and policies. The Movement Advancement Project categorized the states based on the tally scores. States with scores equivalent to 75–100% of the possible points were categorized as “high.” States earning 50–74.9% of the points possible were categorized as “medium.” States with tallies equivalent to 25–49.9% of points possible were categorized as “fair.” States categorized as “low” scored 0–24.9% of points possible and states categorized as “negative” had scores of less than zero. For this study, two groups were created; the medium and high categories were combined into the high policy tally group (50–100% of points possible), and the fair, low, and negative groups were combined into a low policy tally group (<0–49.9% of points possible). The decision to combine the groups as stated above was based on achieving roughly equal sample sizes in the groups and simplifying analyses. MAP updates the Equality Maps in real-time. This study accessed the policy data on September 14, 2021.
Covariates
The covariates for this study included the variables used for propensity score matching (age, sex, education, race, income, and state of residence) as well as variables that were found to differ significantly between groups (marital status, health insurance coverage, and employment status). The covariates were age (grouped in five-year intervals from 50 to 80 and older), sex (male or female), education (high school graduate or less, some college, college graduate/graduate school), race (white, black, Hispanic, other), income (categories ranging from less than $15,000 to $50,000 or more), marital status (married/unmarried couple, single/never married, separated/divorced, widowed), health insurance coverage (yes/no), and employment status (employed, retired, other). This study used the imputed race variable provided by BRFSS; race/ethnicity was imputed for those who refused to respond based on the most common race/ethnicity for the region of the state.
Statistical Analyses
All statistical analyses for this study were performed using SAS, version 9.4. Propensity score matching was used to create a heterosexual group and a cisgender group for comparison with the sexual minority group and the transgender group, respectively. Propensity score matching improves the accuracy of inferences made based on the results of the analyses and reduces the effects of confounding in nonrandomized studies (Austin, 2011; Haukoos & Lewis, 2015). The purpose of using propensity score matching in this study was to create comparison groups that are balanced with the sexual minority and transgender groups on several covariates. To create the matched groups, we used a propensity score matching add-on macro in SAS (Parsons, 2004). First, propensity scores (i.e., the predicted probability of identifying as a sexual minority) were estimated using logistic regression analyses adjusted for the matching covariates. Next, each sexual minority participant was matched with one heterosexual participant based on the calculated propensity score. Specifically, one heterosexual participant was matched with each of the sexual minority participants based on age, sex, education, race, income, state of residence, and state policy tally category. The propensity score matching process was repeated to create the cisgender comparison group for the transgender participants. Specifically, one cisgender participant was matched with each of the transgender participants based on age, race, education, income, state of residence, and state policy tally category. For the 1:1 cisgender to transgender propensity matching, participants were not matched based on sex due to the incongruence between sex assigned at birth and the gender identity of transgender people (Cicero et al., 2020; Pharr & Batra, 2021). Chi-square analyses were conducted to confirm the balance between the sexual minority and heterosexual groups as well as between the transgender and cisgender groups on the matching covariates.
Chi-square analyses were conducted to examine differences in demographic characteristics by state policy tally category for each of the four groups (sexual minority, heterosexual, transgender, and cisgender). Logistic regression and multinomial logistic regression analyses were conducted to assess the association between the policy tally category and the three health outcome variables, adjusted for covariates (age, sex, education, race, income, marital status, health insurance, and employment status). Though sex was not a matching variable for the transgender and cisgender groups, sex was controlled for in the analyses for consistency in the covariates across all logistic regressions. Four sets of logistic regression analyses were conducted to obtain adjusted odds ratios (AOR) and 95% confidence intervals (CI) for each of the health outcomes, one for each of the four groups. Additional logistic regression analyses were conducted to examine differences in sexual orientation subgroups (i.e., gay men, bisexual men, lesbian women, bisexual women) as well as separate logistic regression analyses for heterosexual men and women for comparison.
Results
Demographic Differences Between Propensity Score Matched Groups From 2018–2020 BRFSS

Sexual Minority and Heterosexual Participants
Demographic Characteristics by State Policy Tally Category for Sexual Minority and Heterosexual Participants From 2018–2020 BRFSS
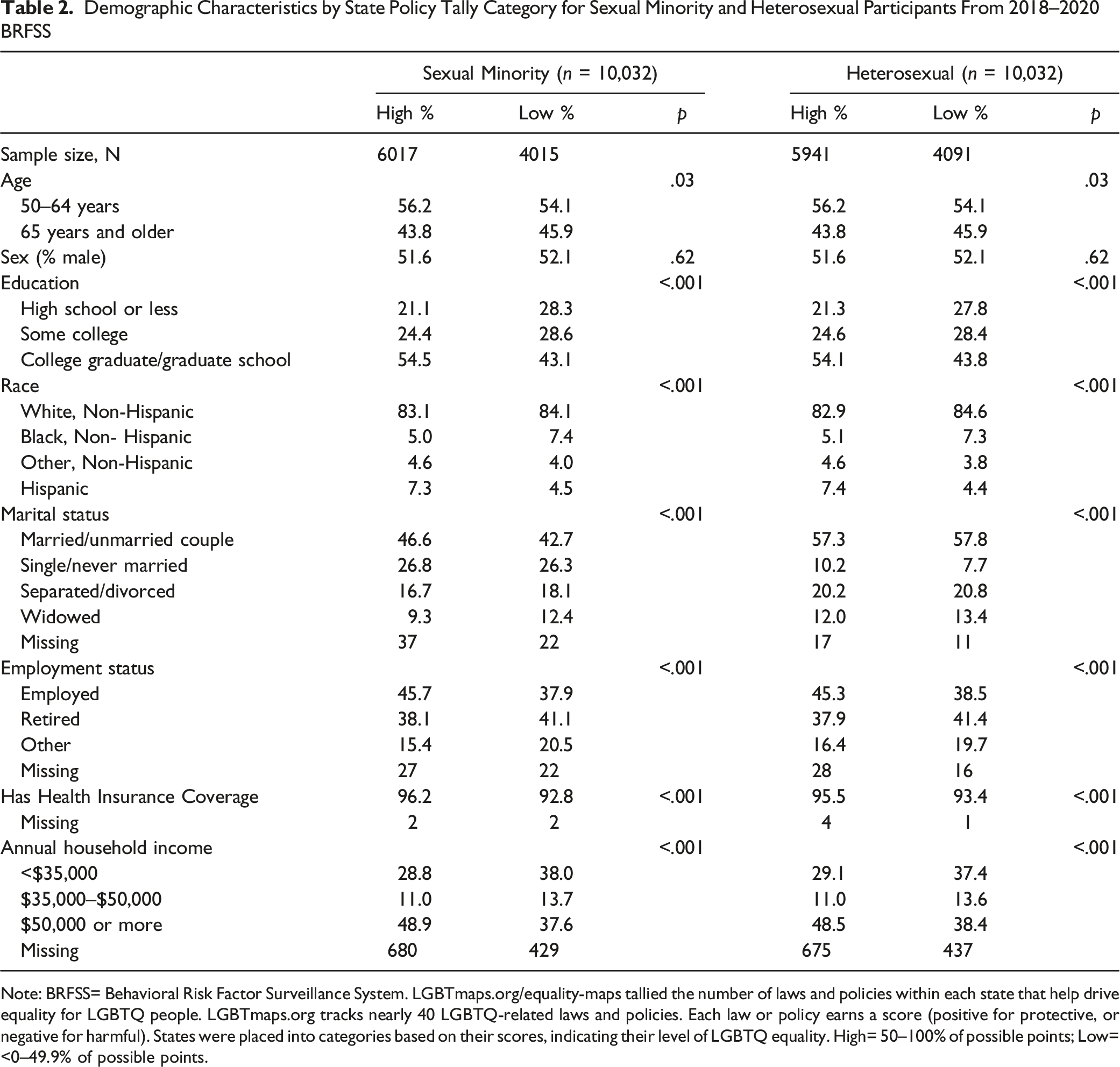
Note: BRFSS= Behavioral Risk Factor Surveillance System. LGBTmaps.org/equality-maps tallied the number of laws and policies within each state that help drive equality for LGBTQ people. LGBTmaps.org tracks nearly 40 LGBTQ-related laws and policies. Each law or policy earns a score (positive for protective, or negative for harmful). States were placed into categories based on their scores, indicating their level of LGBTQ equality. High= 50–100% of possible points; Low= <0–49.9% of possible points.
Health Outcomes by State Policy Tally Category for Sexual Minority and Heterosexual Participants From 2018–2020 BRFSS

Note: AOR= adjusted Odds Ratio. CI= Confidence Intervals. BRFSS= Behavioral Risk Factor Surveillance System. LGBTmaps.org/equality-maps tallied the number of laws and policies within each state that help drive equality for LGBTQ people. LGBTmaps.org tracks nearly 40 LGBTQ-related laws and policies. Each law or policy earns a score (positive for protective, or negative for harmful). States were placed into categories based on their scores, indicating their level of LGBTQ equality. High= 50–100% of possible points; Low= <0–49.9% of possible points. Logistic regression analyses controlled for age, sex, education, income, employment status, health insurance, race, marital status, and state of residence.
Health Outcomes by State Policy Tally Category for Sexual Orientation and Gender Subgroups From 2018–2020 BRFSS
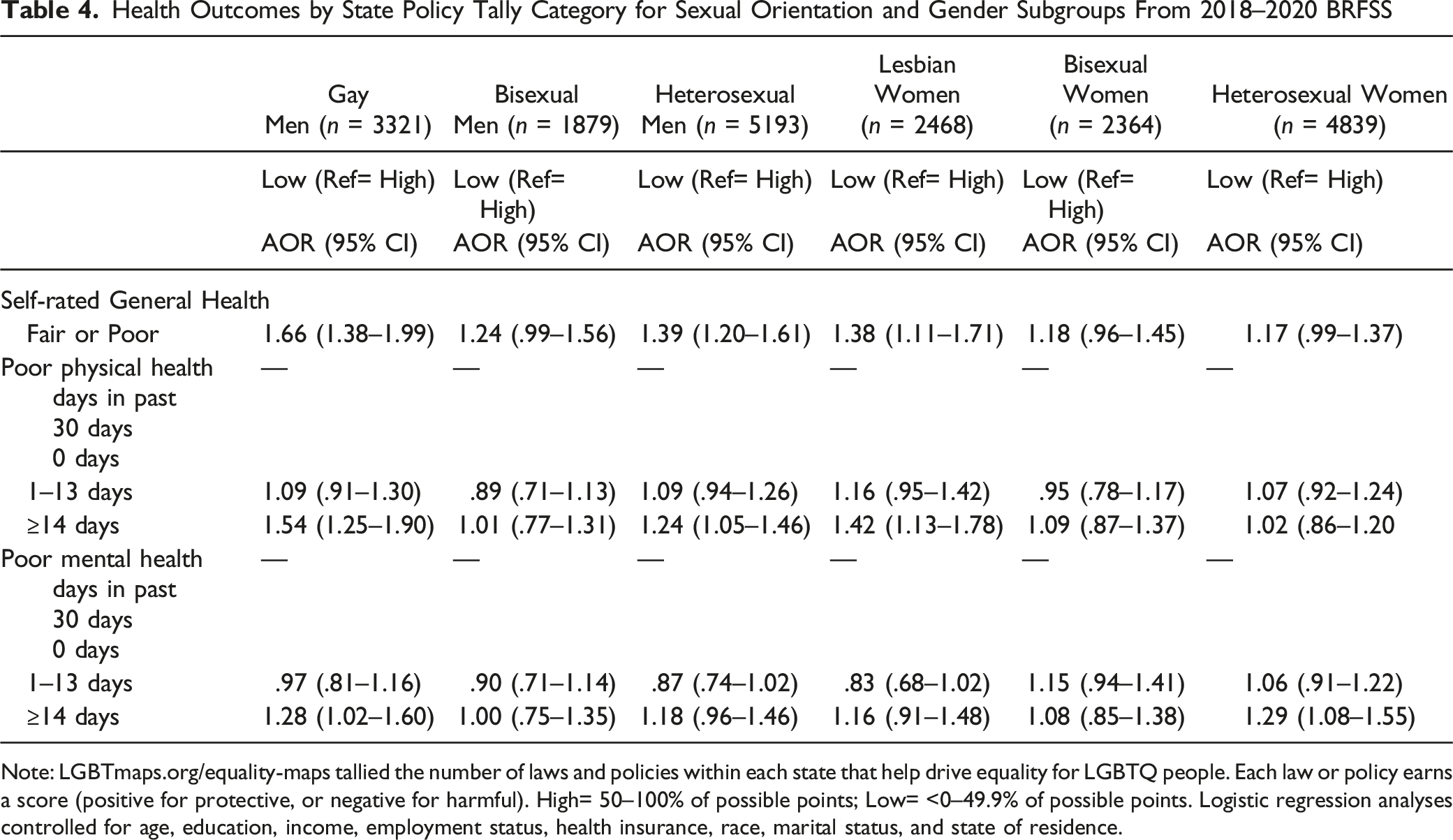
Note: LGBTmaps.org/equality-maps tallied the number of laws and policies within each state that help drive equality for LGBTQ people. Each law or policy earns a score (positive for protective, or negative for harmful). High= 50–100% of possible points; Low= <0–49.9% of possible points. Logistic regression analyses controlled for age, education, income, employment status, health insurance, race, marital status, and state of residence.
Lesbian women in low tally states had 38% higher odds of reporting fair or poor general health and 42% higher odds of reporting 14 or more days of poor physical health in the past 30 days compared to lesbian women in high tally states. Heterosexual women in low tally states had 29% higher odds of reporting 14 or more days of poor mental health than heterosexual women in high tally states. There were no significant differences in health by state policy tally category found for bisexual women.
Transgender and Cisgender Participants
Demographic Characteristics by State Policy Tally Category for Transgender and Cisgender Participants From 2018–2020 BRFSS

Note: BRFSS= Behavioral Risk Factor Surveillance System. LGBTmaps.org/equality-maps tallied the number of laws and policies within each state that help drive equality for LGBTQ people. tracks nearly 40 LGBTQ-related laws and policies. Each law or policy earns a score (positive for protective, or negative for harmful). States were placed into categories based on their scores, indicating their level of LGBTQ equality. High= 50–100% of possible points; Low= <0–49.9% of possible points.
Health Outcomes by State Policy Tally Category for Transgender and Cisgender Participants From 2018–2020 BRFSS

Note: AOR= adjusted Odds Ratio. CI= Confidence Intervals.
LGBTmaps.org/equality-maps tallied the number of laws and policies within each state that help drive equality for LGBTQ people. LGBTmaps.org tracks nearly 40 LGBTQ-related laws and policies. Each law or policy earns a score (positive for protective, or negative for harmful). High= 50–100% of possible points; Low= <0–49.9% of possible points. Logistic regression analyses controlled for age, sex, education, income, employment status, health insurance, race, marital status, and state of residence.
Discussion
To our knowledge, this is the first study to examine within-group differences in the association between state-level LGBT-related policies and the health of LGBT older adults. We found that sexual minority and transgender older adults had greater odds of poor physical health if they lived in a state that had a low state-level policy tally (i.e., <0–49.9% of possible tally points) than sexual minority and transgender older adults in states with a high policy tally (i.e., 50–100% of possible tally points). Our results also suggest that heterosexual participants in low tally states have higher odds of poor health than heterosexual participants living in high tally states. However, the percentage of sexual minority older adults in low tally states (26.8%) reporting fair or poor general health was greater than the percentage of heterosexual older adults in low policy tally states (23.5%) that reported fair or poor general health, a difference between the two groups that is statistically significant. Similar to the findings of a previous study (Gonzales & Ehrenfeld, 2018), these results suggest that sexual minority and transgender older adults have greater odds than heterosexual/cisgender older adults of being in poor physical health when they reside in states with limited or no LGBT protections.
Although the results suggest that sexual minority older adults living in states with less legal protections have greater odds of poor physical health, there is also evidence that the matched heterosexual older adults living in the same states also experience poorer health than their counterparts in states with more enacted LGBT-related policies. There are likely some underlying differences between the states that have more legal protections for LGBT people and the states with fewer protections. For instance, states with more LGBT protective policies are likely more progressive in other (non-LGBT specific) ways that benefit health, such as more labor protections, flexibility in Medicaid eligibility, and strict housing rules (e.g., rent control; Montez et al., 2020). Social determinants of health that have a major impact on the health and well-being of all people include barriers to accessing health care services (e.g., lack of insurance coverage), social contexts (e.g., social norms such as discrimination, socioeconomic conditions such as poverty), physical environment (e.g., safety), and education (US Department of Health and Human Services, n.d). Though we controlled for these covariates, participants in low tally states were more likely to have a lower income, less education, and were less likely to have health insurance coverage compared to participants in high tally states.
Additionally, states that have fewer enacted LGBT-related protective policies have more conservative voting practices (i.e., more likely to be Republican). A quick comparison between the equality map on the Movement Advancement Project website (Movement Advancement Project, 2021) and a recent election map will show similar trends. As mentioned in the introduction, one study found that conservative voting practices were associated with higher rates of experiences of discrimination in health care for transgender people (White Hughto et al., 2016). Other research has also found associations between Republican/conservative voting and poorer health (Kannan & Veazie, 2018; Pabayo et al., 2015; Shin & McCarthy, 2013; Wasfy et al., 2020). This suggests that anyone who lives in a state with more progressive policies likely benefits from better health regardless of sexual orientation or gender identity; however, living in a state with more progressive policies is more important for sexual minority and transgender individuals because they are at greater risk of experiencing health problems and have a history of health disparities compared to their heterosexual/cisgender counterparts.
For the number of days of poor mental health, heterosexual older adults in low tally states had significantly higher odds of reporting fourteen or more days of poor mental health than their counterparts in high tally states. There was no significant difference in the number of days of poor mental health for sexual minority older adults by state tally category. However, an examination of the percentages in Table 3 shows that 40% of sexual minority participants in both high and low tally states reported at least one day of poor mental health while only 30% of heterosexual participants in both high and low tally states reported at least one day of poor mental health. Exploratory analyses found this difference in the number of days of poor mental health between sexual minority and heterosexual participants to be statistically significant. Together, these findings suggest that sexual minority older adults experience poorer mental health than their heterosexual counterparts regardless of the number of protective policies in their state of residence. Poorer mental health in sexual minority participants may be the result of individual-level minority stressors such as microaggressions, internalized homonegativity, or victimization (Balsam et al., 2011; Feinstein et al., 2012; Lee et al., 2016; Lehavot & Simoni, 2011).
The subgroup analyses revealed significant differences between the sexual minority subgroups. Gay men and lesbian women in low tally states had greater odds of poor physical health compared to their counterparts in high tally states. Gay men additionally had greater odds of poor mental health if they lived in states with fewer protections. These results may be indicative of living in states that are not LGBT-friendly which may result in more exposure to minority stressors that have a deleterious effect on health and well-being. Additionally, the subgroup analyses for the heterosexual group found that, when analyzed by gender, heterosexual women in low tally states had greater odds of poor mental health, but the association was not significant for heterosexual men. This may suggest that the conservative voting practices in the low tally states may also create a more mentally stressful environment for heterosexual women.
Bisexual men and women did not experience differences in the physical and mental health outcomes by state policy tally. One possible explanation is that bisexual men and women in states with fewer protections may be less affected by the lack of LGBT-related policies than their gay and lesbian counterparts. Another possible explanation is that bisexual people in states with fewer protections may be less inclined to disclose their sexual identity, resulting in less exposure to external minority stressors. Finally, bisexual people may experience similar odds of poor physical and mental health regardless of where they live. Existing research has found that bisexual older adults were at greater risk of poor health outcomes than gay and lesbian older adults (Conron et al., 2010; Dilley et al., 2010; Fredriksen-Goldsen et al., 2017; Wardecker et al., 2019). More research is necessary to understand how LGBT-related laws and policies affect the health and well-being of bisexual people.
This study provides evidence that structural stigma is associated with poorer physical health for LGBT older adults. Structural stigma was also associated with poorer mental health for older gay men. The cumulative effect of the chronic stress from structural stigma over time may contribute to the increased risk of poor physical and mental health in older LGBT adults (Ferraro & Shippee, 2009). Older LGBT adults have experienced tremendous social and political change during their lifetime (Fredriksen-Goldsen, 2016) and may be more cognizant of changes in LGBT-related laws and policies, resulting in chronic stress that negatively influences their health and well-being. For LGBT older adults, a lack of legal protection against discrimination in long-term care settings may result in feeling the need to “go back into the closet” or conceal their sexual or gender identity in these settings (Furlotte et al., 2016; Putney et al., 2018; Stein et al., 2010). Furthermore, chronic exposure to stress is a risk factor for cognitive decline. Research has found that LGBT older adults have unique risk factors for cognitive decline, including a greater risk of social isolation due to identity concealment and discrimination (Fredriksen-Goldsen et al., 2018; Kim & Fredriksen-Goldsen, 2016; Kuyper & Fokkema, 2010).
This study built on previous research and has several strengths. First, we examined state-level legal protections for LGBT people by using data that tallies the number of enacted policies in 41 states out of nearly 40 sexual orientation- and gender identity-related policies. Second, we examined within-group differences in physical and mental health outcomes between sexual minority adults as well as differences between transgender adults from states with 50% or more of the LGBT-related policy points (i.e., medium or high tally states) compared to their sexual minority and transgender counterparts in states that had less than 50% of possible policy points (i.e., fair, low, or negative tally states). Third, we included propensity matched heterosexual and cisgender groups for comparison with the sexual minority and transgender groups, respectively, to see if the differences in health are unique to LGBT individuals. Lesbian, gay, bisexual, and transgender participants had greater odds of reporting fair or poor general health if they lived in a state with less than 50% of possible points for enacted LGBT-related policies.
Despite the strengths of this study, there are some limitations to note. First, this study is cross-sectional; therefore, we cannot infer causality between the implementation of state-level LGBT-related policies and the health of LGBT adults. Second, only data from 41 states were included in the analyses. The states that did not have data were primarily in the low or negative tally categories, especially when looking at gender identity-related policies; the inclusion of these states may have differently influenced the results of the study. Third, the state-level policy data from MAP is continuously updated as policies change, and year-to-year data is not available. Therefore, we used policy data from 2021 but used health data from the 2018–2020 BRFSS surveys. However, we believe it is unlikely that this significantly influenced the results of this study. Additionally, this study excluded participants that identified as both a sexual minority and as transgender. The transgender participants included in this study identified as a non-sexual minority (i.e., heterosexual) which may have contributed to the lack of significant differences in physical and mental health. The small group of excluded participants who identified as transgender and as a sexual minority may be at even greater risk of poor health outcomes due to a combination of stressors from both their sexual orientation and gender identity. Finally, while several covariates were controlled for, the only independent variable assessed in this study was LGBT-related policy tally. Future research should fully examine the differences in social determinants of health between the states that have more legal protections for LGBT people compared to those that have fewer protections as well as the associations with the health of residents in those states.
Conclusions
This study examined whether state-level policies regarding sexual orientation and gender identity were associated with physical and mental health in older LGBT adults. We found that LGBT older adults were more likely to report poorer physical health if they lived in a state that had less than 50% of the possible points from nearly 40 LGBT-related laws and policies. This suggests that differences in LGBT-related policies at the state level are an important factor to consider when examining health disparities in LGBT adults. As of this writing, LGBT-related laws and policies are enacted by the state-level government. Not having federal protections allows states to enact or remove protections against discrimination for LGBT people. For example, in 2022, the Florida state government passed a “don’t say gay” law that bans the discussion of LGBT-related issues in schools and the Texas state government attempted to restrict medical care for transgender youth. A federal law like The Equality Act would provide consistent protections against discrimination for LGBT people and result in less variation by state. This study provides more evidence that structural discrimination or policies that constrain opportunities, resources, and well-being of LGBT people are associated with poorer physical and mental health in this growing subpopulation. Since health disparities are costly to society, policymakers should consider the physical and mental health benefits of implementing protective LGBT-related policies at the state or federal level.
Supplemental Material
Supplemental Material - Sexual Orientation and Gender Identity-Related State-Level Policies and Perceived Health Among Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults in the United States
Supplemental Material for Sexual Orientation and Gender Identity-Related State-Level Policies and Perceived Health Among Lesbian, Gay, Bisexual, and Transgender (LGBT) Older Adults in the United States by Christi L. Nelson, Britney M. Wardecker, and Ross Andel in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.