
Abstract
Introduction
The United States is facing a surge in demand for family and unpaid caregivers due to the aging demographics of its population and the subsequent growth in care needs induced by age-related health conditions (Wolff et al., 2016). While estimates of caregivers vary (ranging from 2.7 to 36.1 million), a recent National Academies of Sciences, Engineering, and Medicine (NASEM) report suggested that at least 17.7 million individuals in the United States are caregivers of an older adult living with health or functional limitations (National Academies of Sciences and Medicine, 2016).
The caregiver role is accompanied by complex costs and rewards (Raschick & Ingersoll-Dayton, 2004). While caregivers may develop a sense of personal achievement, mutuality, and purpose in life through constant interactions with their loved ones (Grant et al., 1998; Roth et al., 2015), they may also experience significant physical, emotional, and financial strains (Schulz et al., 2016; Schulz & Sherwood, 2008), especially when assisting care recipients who live with medical complexities. Chronic conditions such as dementia, cancer, and stroke are found to have detrimental effects on caregiver burden, as they could substantially undermine the independence of care recipients and generate additional care needs that require extensive caregiver involvement (Adelman et al., 2014).
Hearing loss is a highly prevalent health condition among older adults. In the United States, it is estimated that approximately two-thirds of adults aged 70 years and older experience clinically meaningful hearing loss (Lin et al., 2011; Lin & Ferrucci, 2012). Despite its association with multiple undesired health outcomes, such as social isolation, loneliness, cognitive decline, and falls (Livingston et al., 2020; Mick et al., 2014; Shukla et al., 2020), hearing loss has received less attention in the caregiving literature because it does not directly introduce care needs and is usually not the primary reason for which older adults receive care. However, hearing loss could negatively impact communication, a fundamental aspect of caregiving (World Health Organization, 2021; Polk, 2005), by interference with oral conversation, the most common form of interpersonal communication between caregivers and care recipients. As a direct result of communication breakdown, increased frustration, anxiety, and lethargy are observed among both parties of the caregiving relationship (Savundranayagam et al., 2005). Without proper intervention, the cumulation of unmet communication needs may prevent caregivers from fulfilling regular care needs, which could contribute to caregiver burden and harm the quality of caregiver-recipient relationships (Heine & Browning, 2002; Kamil & Lin, 2015).
Caregiving time is a key metric that has been widely used in the evaluation of informal family care (van den Berg & Spauwen, 2006). As compared to other measures of caregiver burden, time spent on care activities has several unique advantages. First, it is an objective metric that directly reflects aspects of the economic cost of care and may therefore be comparable across individuals. Second, it is sensitive to care needs as increased care needs may increase time spent providing care (Hajek et al., 2016), therefore, differences in time spent on care activities for those with similar conditions apart from hearing loss may capture the consequence of communication difficulties caused by hearing loss. Third, it is highly correlated to caregiver’s physical and emotional burden and is predictive of caregiver’s overall well-being (Novak & Guest, 1989). Lastly, studies that examined the association between other sensory loss and caregiver experiences also adopted caregiving time as a primary outcome (Varadaraj et al., 2021), supporting the continuation of our evidence base to improve care.
Caregiving research has traditionally relied on a dyadic approach that focuses on the experience of individual caregivers and their care recipients. However, recent work acknowledges the presence of caregiving networks, where multiple caregivers are involved in the assistance of a single care recipient and the delegation of shared care tasks and resources (Koehly et al., 2015; Spillman et al., 2020). Like other aspects of care, communication could be impacted by the presence of complex communication chains in caregiving networks, as a result, the association between hearing loss and caregiving time could be moderated by the presence of care networks.
Care recipient’s dementia status could be another potential moderator of the association between hearing loss and caregiving time. The concurrent presence of hearing loss and dementia is common—recent work suggests an overlap between the two conditions such that 6% of those with normal hearing have dementia while 9% and 16% of those with mild and moderate or greater hearing loss have dementia (Huang et al., 2023). Like hearing loss, dementia could exacerbate communication difficulties between caregivers and care recipients (Banovic et al., 2018). Moreover, caregivers assisting older adults with concurrent hearing loss and dementia are observed to be more actively engaged in care activities and have more frequent interaction with the medical system (Powell et al., 2023), making the association of hearing loss with caregiving time heterogeneous.
Using data from the linked National Health and Aging Trends Study (NHATS) and National Study of Caregiving (NSOC) covering the time period 2011–2015, we aimed to examine: (1) the association between care recipient’s hearing status and caregiving time; and (2) whether the association is moderated by the presence of caregiving networks and care recipient’s dementia status. Given prior evidence of greater care needs among older adults with hearing loss, we expect caregivers who assisted older adults with hearing loss to spend greater time providing care. This investigation seeks to improve the alignment of care recipients’ health needs with caregiver burdens, including time spent on care, to understand new avenues for future interventions to support the growing population of caregivers.
Methods
Study Population
We pooled cross-sectional data from the 2011 and 2015 rounds of the linked National Health and Aging Trends Study (NHATS) and National Study of Caregiving (NSOC). The NHATS is an ongoing panel cohort that is representative of Medicare beneficiaries aged 65 and older in the contiguous United States (Freedman et al., 2020). Via in-person interviews with the sampled persons or designated proxies (when the sampled person cannot respond independently), NHATS provides a general picture of the late-life health and functioning of older adults in the U.S.
The NSOC is a nationally representative survey of family and other unpaid caregivers who assist NHATS participants with aspects of health and function. NSOC rounds I and II were cross-sectional and were conducted in conjunction with NHATS at periodic intervals (rounds 2011 and 2015), and the NSOC sampling frame was developed using the list of helpers of NHATS participants (if more than five helpers were identified by one NHATS participant, five would be randomly sampled into the final NSOC population) (Freedman et al., 2020). Telephone interviews were scheduled to collect information on caregiving activities, duration and intensity of care, effects on caregivers’ well-being and participation, along with demographic factors.
Of the 4211 caregivers (linked to 2502 care recipients) surveyed (2007 from round 2011 and 2204 from round 2015), 1208 were excluded from the final analytic sample, leaving 3003 caregivers that were linked to 2055 care recipients. To maximize comparability across survey rounds and relevancy to our research question, we excluded NSOC caregivers assisting older adults who were not community-dwelling (n = 514). We also excluded caregivers who did not contribute to caregiving activities one month prior to the NSOC interview (n = 156), and whose care recipient self-identified as being Deaf (n = 32), since Deaf identity is highly correlated with the use of American Sign Language, a communication medium relies mainly on visual signals. Additionally, when creating the pooled sample, we excluded duplicated observations of caregivers who were sampled in both the 2011 and 2015 rounds of the NSOC survey (observations from the 2011 round were dropped, n = 506).
Multiple imputations by chained equations (MICE) were used to impute missing covariate values (Azur et al., 2011; Schafer, 1999). The imputation model included all the covariates in the final model plus care recipient’s marital status and presence of children under age 18 in the caregiver’s household. The imputation model included 20 sets of imputations and 20 iterations for the burn-in period (Detailed information can be found in Supplemental Material).
Both NHATS and NSOC were approved by the institutional review board (IRB) of Johns Hopkins Bloomberg School of Public Health. Signed informed consent was obtained from all participants or proxy respondents. All data used in this study were de-identified and publicly available; the study was considered not human subjects research by the IRB of Johns Hopkins Bloomberg School of Public Health and was exempted from IRB review.
Exposure
We identified care recipients’ functional hearing difficulty status to be our primary exposure. Hearing difficulty (1 = “yes,” 0 = “no”) was considered present if participants reported hearing aid use (1 = “yes,” 0 = “no”) or answered no to either of the following questions, “When using a hearing aid (if applicable), do you hear well enough to: (1) use the telephone; (2) carry on a conversation in a room with a radio or TV playing?”
Outcome
The primary outcome of this study was the hours of care provided by the caregivers in the past month (prior to the telephone interview). For those caregivers who helped regularly, days per week and hours per day (on days when help was provided) were collected; for those whose schedule varied, days in the last month and hours per day were collected. Although questions were identical across study visits, in the 2015 round of NSOC, respondents were allowed to report zero days of work in care activities. To create a valid and comparable count of hours of care per month across rounds, we adopted an imputation algorithm recommended by NHATS published methodology (Freedman et al., 2014).
Moderator
For the stratified analysis, we created two binary indicators of the presence of caregiving networks (0 = “no,” 1 = “yes”) and care recipient’s dementia status. Specifically, if an NSOC caregiver worked independently and served as the only source of assistance to an NHATS participant, the caregiver was regarded as having no caregiving network; otherwise, if the caregiver worked with other NSOC caregiver(s) to assist an NHATS participant, the caregiver was coded as having existing caregiving networks; the construction of caregiving networks is based on previous NSOC literature (Spillman et al., 2020).
Classification of dementia followed NHATS published methodology (Kasper et al., 2013). Based on physicians’ diagnosis, the eight-item informant interview to differentiate aging and dementia (AD8 criteria) (Galvin et al., 2005) and cognitive test scores (in domains of orientation, memory, and executive functioning), NHATS participants were classified into three groups regarding their dementia status—probable dementia, possible dementia, and no dementia. To stay consistent with previous research in NHATS, we coded dementia as a binary variable (0 = “possible/no dementia,” 1 = “probable dementia”) (Kasper et al., 2015).
Covariates
Caregiver’s characteristics include age (in years), sex (0 = “male,” 1 = “female”), relationship to the care recipients (1 = “spouse,” 2 = “adult children,” 3 = “other relatives,” 4 = “non-relatives”), educational attainment (1 = “high school or less,” 2 = “some college,” 3 = “college degree or above”), annual household income (adjusted for inflation), living arrangement (0 = “co-reside with the care recipients,” 1 = “other living arrangements”), presence of children under age 18 in the household (0 = “no,” 1 = “yes”), and self-reported health status (1 = “poor/fair,” 2 = “good,” 3 = “very good/excellent”).
Care recipient’s characteristics include age (in years), sex, race/ethnicity (1 = “Non-Hispanic White,” 2 = “Non-Hispanic Black,” 3 = “Hispanic,” 4 = “other”), marital status (0 = “married or partnered,” 1 = “other”), self-reported health status (1 = “poor/fair,” 2 = “good,” 3 = “very good/excellent”), number of comorbidities (1 = “0,” 2 = “1–2,” 3 = “3–5,” 4 = “6 or more”; comorbidity count includes arthritis, cancer, diabetes, heart attack, heart disease, hypertension, lung disease, osteoporosis, and stroke), ownership of hearing devices (0 = “no,” 1 = “yes”), and the number of caregivers.
Data Analysis
We summarized caregivers’ and care recipients’ demographic and socioeconomic characteristics, caregiving hours, and other attributes of care, stratified by care recipients’ hearing difficulty status. Multivariable linear regression models, clustered at NHATS participant ID, were used to estimate the association between care recipient’s hearing difficulty status and caregiving hours in the past month. We used natural-log-transformed caregiving time as the dependent variable, as the distribution of caregiving time was highly right-skewed (skewness = 2.4). Two stratified analyses were then conducted by re-fitting the model on subgroups of the analytical sample according to the presence of caregiving networks and care recipient’s dementia status. In sensitivity analyses, we examined whether adopting a more sensitive dementia definition (probable/possible dementia vs. no dementia) is going to influence the estimated association, and whether hearing aid use is associated with reduced caregiving time among those with hearing difficulty. Results of sensitivity analyses were presented in Supplemental Material.
All models were adjusted for NHATS participants’ age, race/ethnicity, sex, number of comorbidities, dementia status, NSOC caregivers’ age, sex, education, income, self-reported health, relationship to care recipient, and living arrangement. Covariates were selected based on clinical relevance and prior research (Varadaraj et al., 2020). NHATS and NSOC complex survey weights were applied to all analyses as instructed by published NHATS methodology (Freedman et al., 2020). All tests were based on a statistically significant level as defined by two-sided p < .05. Data management and analysis were conducted using Stata 17.0 (Stata Corp, College Station, TX).
Results
Characteristics of Caregiving Dyads and Attributes of Care
Caregivers’ Characteristics, Stratified by Care Recipients’ Functional Hearing Status, Using Pooled 2011 & 2015 National Study of Caregiving (NSOC) Data.

Notes: Unweighted frequencies and weighted percentages were displayed for categorical variables; weighted mean and standard deviation were calculated for continuous variables, using pooled NSOC analytical weights. Five exhaustive and mutually exclusive categories of caregivers’ age were created to compare its distribution by hearing status. Descriptive statistics are based on complete cases only, missing observations will be imputed when doing regression analysis.
Care Recipients’ Characteristics, Stratified by Their Functional Hearing Difficulty Status, Using Pooled 2011 & 2015 National Health and Aging Trends Study (NHATS) Data.

Notes: Unweighted frequencies and weighted percentages were displayed for categorical variables; weighted mean and standard deviation were calculated for continuous variables, using pooled NHATS analytical weights. Six exhaustive and mutually exclusive categories of care recipients’ age were created to compare its distribution by hearing status. Comorbidity count included arthritis, cancer, diabetes, heart attack, heart disease, hypertension, lung disease, osteoporosis, and stroke. Descriptive statistics are based on complete cases only.
The majority of care recipients were non-Hispanic White (75%) females (64%) with an average age of 79. Of all care recipients (N = 2055), 660 lived with hearing difficulty. Care recipients with hearing difficulty tended to be older (mean age: 82) and consisted of more males (43%) and non-Hispanic Whites (79%) relative to those without hearing difficulty (mean age: 78; male: 33%; non-Hispanic Whites: 73%); they were also less likely to be married or partnered (50% vs. 55%). Care recipients with and without hearing difficulty were similar regarding their health status, with approximately 50% reporting good or better health and 70% having more than two comorbid conditions. The average number of caregivers per care recipient in the total study population was 1.4, and among those with hearing difficulty, 44% reported hearing aid use.
Attributes of Care Provided by Caregivers from the Pooled 2011 & 2015 National Study of Caregiving (NSOC) Data, Stratified by Care Recipients’ Functional Hearing Difficulty Status.
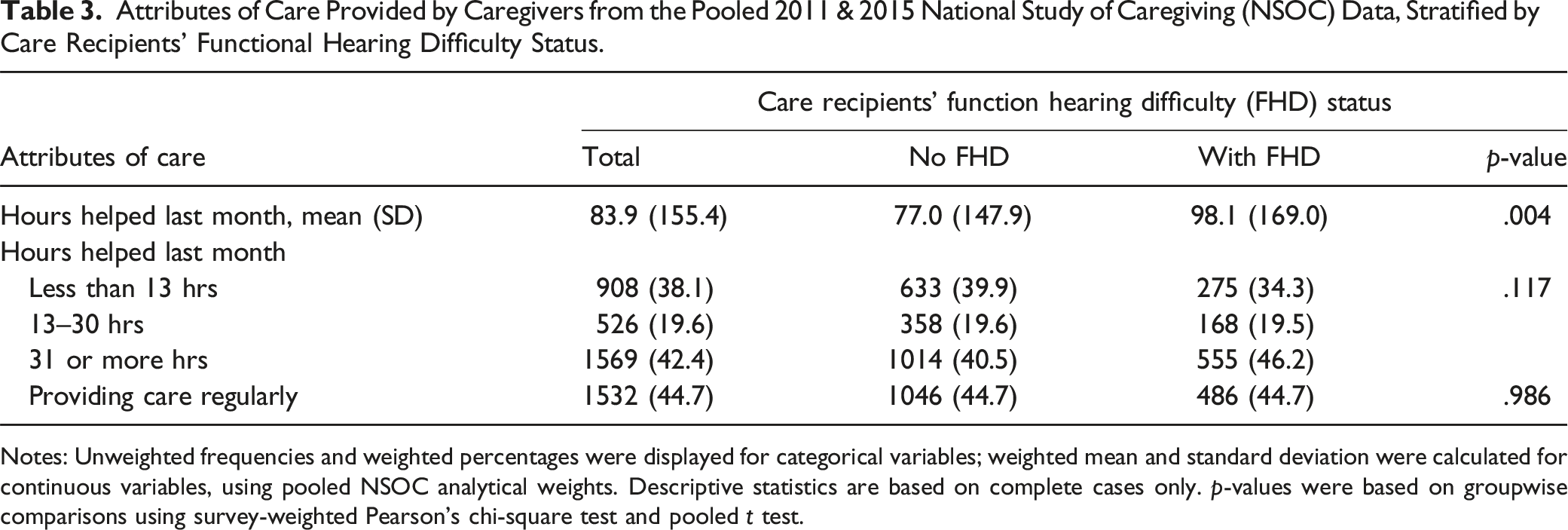
Notes: Unweighted frequencies and weighted percentages were displayed for categorical variables; weighted mean and standard deviation were calculated for continuous variables, using pooled NSOC analytical weights. Descriptive statistics are based on complete cases only. p-values were based on groupwise comparisons using survey-weighted Pearson’s chi-square test and pooled t test.
Association Between Care Recipients’ Hearing Difficulty Status With Caregiving Time
Based on weighted, fully adjusted linear regression models (Figure 1), caregivers of older adults with hearing difficulty were observed to spend 18% (95% Confidence Interval [CI]: 1.04, 1.32) more time on care activities than caregivers who assisted older adults without hearing difficulty. Results were similar in sensitivity analysis where dementia was reclassified, no significant association was observed between hearing aid use and caregiving time among caregivers assisting older adults with hearing difficulty (see Supplement Material). Multivariable-adjusted associations between care recipient’s functional hearing difficulty status and caregiving time, stratified by presence of caregiving networks and care recipient’s dementia status, using linked National Health and Aging Trends Study (NHATS) and National Study of Caregiving (NSOC), Round 2011 & 2015. Note: CN = Caregiving Network; CR = Care Recipient. Models were adjusted for caregivers’ characteristics (age, education, relationship to CR, health status, annual household income, and living arrangement) and care recipients’ characteristics (age, female sex, race/ethnicity, dementia status [not included in the second stratified analysis], and the number of chronic conditions). Pooled NSOC complex analytical weights were applied. Multiple Imputations by Chained Equations (MICE) approach was adopted to impute the missing values of covariates.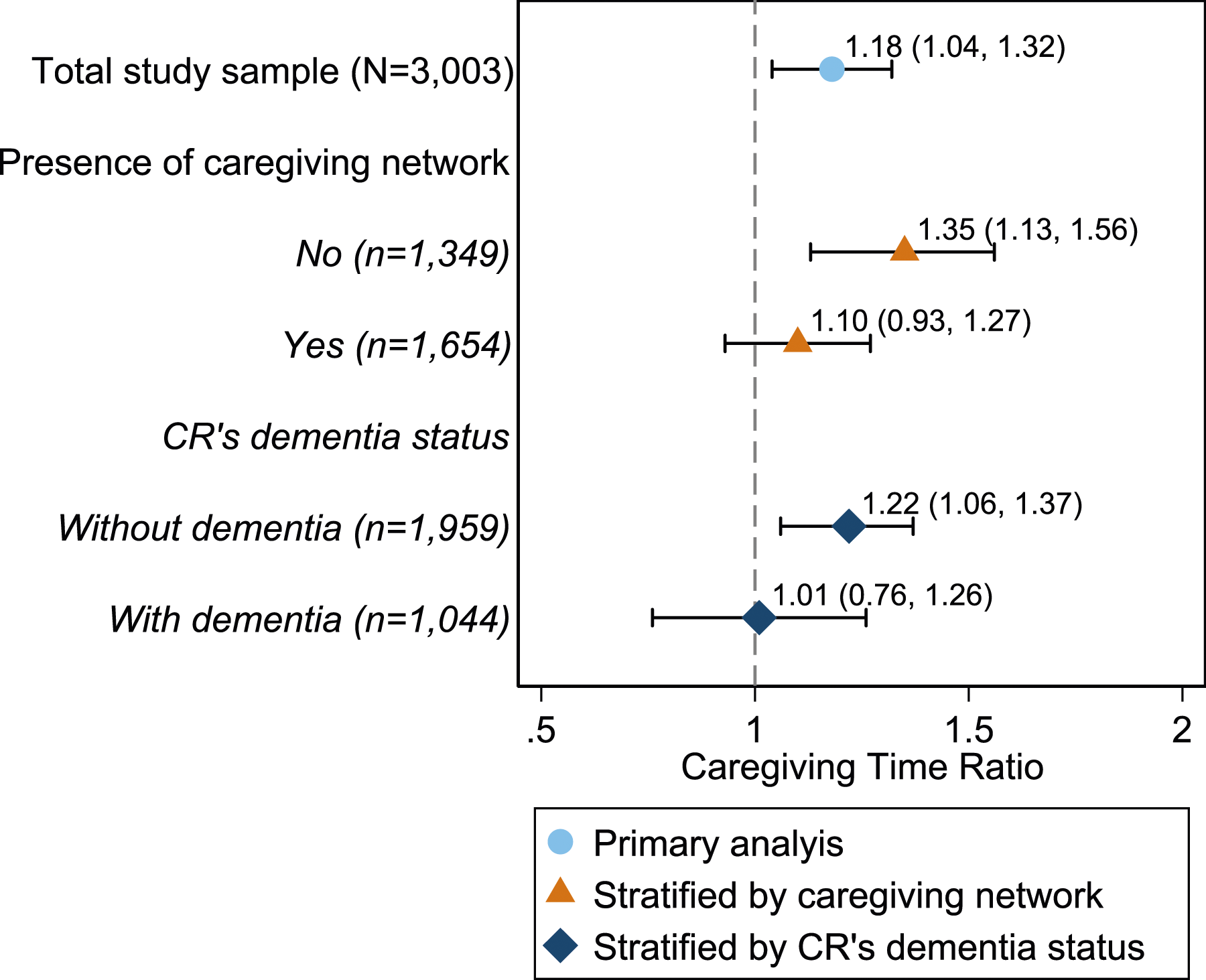
In models stratified by the presence of caregiving networks, associations between hearing difficulty and caregiving time were stronger among caregivers who assisted older adults without existing caregiving networks, among those, who assisted older adults with hearing difficulty were observed to spend 35% (95% CI: 1.13, 1.56) more time providing care, relative to those assisting older adults without the condition. With the presence of caregiving networks, however, the association between care recipient’s hearing status and the caregiving time of each caregiver was no longer statistically significant (β = 1.10; 95% CI = .93, 1.27).
When stratifying by care recipient’s dementia status, a stronger association between hearing difficulty and caregiving time was observed among caregivers assisting older adults without dementia (β = 1.22; 95% CI = 1.06, 1.37). For those whose care recipients lived with dementia, the association between hearing difficulty and caregiving time was no longer statistically significant (β = 1.01; 95% CI = .76, 1.26).
Discussion
Using nationally representative datasets of family caregiving, we found that caregivers of individuals with functional hearing difficulty spent more time providing care. Considering the amount of time on an absolute scale and the long-term commitment of family care, the elevated caregiving time associated with hearing difficulty (around 16 hours per month) likely has a meaningful impact on the well-being of caregivers. Results from stratified analysis suggested that the association between hearing difficulty and caregiving time might be heterogeneous across subgroups of caregivers, among those assisting older adults with existing caregiving networks or dementia, minimal association between hearing difficulty and caregiving time was observed. To our knowledge, few studies have characterized how the presence of hearing difficulty among care recipients affects caregivers’ experience, and this study is the first to quantitatively examine the associations of older adults’ hearing difficulty status with caregiving time. Despite a paucity of existing literature, findings from our study closely mirror some previous research on family care for older adults with other sensory or cognitive impairments that may impact communication: using data from the linked NHATS/NSOC study, an association was found between care recipients’ vision impairment and dementia status with increased caregiving hours (relative to caregivers assisting older adults with neither condition; those who assisted older adults with vision impairment or dementia, spent 1.3 times more hours on caregiving activities in the past month, while those who assisted older adults with concurrent vision impairment and dementia spent 1.7 times more hours), as well as restricted participation in valued social activities (Varadaraj et al., 2020, 2021).
Caregiving is often a shared experience—with care tasks borne by multiple individuals, caregiving networks are naturally formed when caregivers work collaboratively to support each other and the care recipients. Previous studies have suggested that the types and amounts of help provided by caregivers differ substantially with and without existing caregiving networks (Barbosa et al., 2011). In our analysis, we also found the associations between hearing difficulty and caregiving time to be attenuated with the presence of caregiving networks. This may be partially explained by the presence of caregivers who helped with less communication-intensive activities (e.g., shopping, transportation, and home repairs) and devoted shorter time (around 65% less) to care activities (Tennstedt et al., 1989).
Considering dementia’s detrimental effect on communication, the minimal association of hearing difficulty with caregiving time among caregivers assisting older adults with dementia could likely be explained by shared pathways, as both hearing difficulty and dementia contribute to caregiving time via communication breakdowns (Watson et al., 2012). However, it is worth noting that the validity of hearing difficulty measures might be threatened by the presence of dementia, as prior methodological work suggested, both self- and proxy-reported hearing measures have low sensitivity (less than 65%) among older adults with cognitive impairments (Choi et al., 2016; Kim et al., 2022). It is reasonable to assume the underlying association between clinically diagnosed hearing loss and caregiving time to be stronger than the observed association in our analysis.
There are several limitations of our study. Firstly, in NHATS, hearing was subjectively measured through self-evaluation, which may fail to capture clinically meaningful hearing loss that has insidious onsets (Nondahl et al., 1998). Secondly, although the NSOC sampling design aimed to capture a nationally representative caregiver population, some key caregiver characteristics, including race and ethnicity, were not available at its first survey round. By assuming that caregivers and care recipients were from the same racial/ethnical background, we acknowledge that our study population predominantly consists of non-Hispanic White females with college degrees, which prevented us from further exploring the potential moderation effects of culture and other indicators of socioeconomic positions.
The strength of our study lies in the representativeness of the study population. The linked NHATS/NSOC datasets provide comprehensive information on the caregiving aspects and characteristics of the caregiving networks, enabling us to be among the first to examine hearing-related caregiving effects quantitatively and make inferences on a national level. With newly released NHATS/NSOC data, future work should consider adopting clinical measurements of hearing loss that would allow for a deeper understanding of the dose-response of hearing loss on caregiving outcomes.
Findings from our study have important implications. Current caregiver support programs have primarily targeted older adults with dementia, cancer, or other critical health conditions. Despite its high prevalence, however, hearing loss has rarely been the primary focus of these programs. Emerging evidence from pilot trials has suggested that hearing care intervention can improve communication between older adults and their care partners and has the potential to reduce caregiver burden and promote quality of life for both parties (Mamo et al., 2017). Moreover, with FDA’s new regulations on over-the-counter (OTC) hearing aids, the potential is high that caregivers in the U.S. who assist older adults with mild-to-moderate hearing loss can benefit from more accessible and affordable hearing devices.
Standing at the intersection of family care and hearing care, our study provides evidence of hearing difficulty as a source of caregiver burden in the form of greater time input. Considering the modifiable nature of hearing difficulty, older adults who live with the condition, as well as their caregivers, could benefit from accessible, person-centered hearing rehabilitation; with increased public awareness, tailored intervention strategies can be developed to support caregivers and equip them with toolsets to address communication problems raised by hearing loss.
Footnotes
Author’s Note
The paper was presented as a poster at the 49th Annual Scientific and Technology Conference of the American Auditory Society.
Author Contributions
NSR, WZ, and DSP were responsible for the concept and design of this study. WZ and EEG were responsible for conducting statistical analysis and interpretation of study findings. WZ took the lead in drafting the manuscript while NSR, DSP, and JAD made critical revisions. NSR and WZ prepared the final version of the manuscript with approval from all other co-authors.
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NSR reports sitting on the scientific advisory board of Neosensory.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DSP is supported by NIH/NIA T32AG066576 and the Hopkins’ Economics of Alzheimer’s Disease and Services (HEADS) Center of the National Institute on Aging (NIA) award number P30AG066587. JAD is supported by NIA Grant K01AG054693. NSR is supported by NIA Grant K23AG065443 and reports sitting on the scientific advisory board of Neosensory.