
Abstract
Effective and efficient staff scheduling has always been a challenging issue, especially in health service organisations. Both the extremes of staff shortage and overage have an adverse impact on the performance of healthcare organisations. In this case, an electronic and systematic staff scheduling (e-rostering) system is the often seen as the best solution. Unless an organisation has an effective implementation of such a system, possible cost savings, efficiency, and benefits could be minimal. This study is aimed to research key success factors for the successful effective implementation of an electronic rostering system, especially at healthcare organisations. A case study research method was used to evaluate critical success factors for effectively implementing an e-rostering system. The data were collected through interviews and observations. The findings indicate that technical support, an effective policy, leadership, clear goals and objectives, gradual change, evidence of the advantages of the new system, senior management support, and effective communication are the critical success factors in implementing an e-rostering system in healthcare organisations. Prior to this study, no such factors were grounded in the current context, so this research would help in bridging the gap towards effective implementation of an e-rostering system in the healthcare sector. This research also suggests future studies in different cultures and contexts.
Keywords
Introduction
The use of computer-based information systems has many advantages including quicker processing and cost-effectiveness. The health sectors, especially National Health Service (NHS) Trusts in UK, have reported significant budget deficits, with nearly half of the total budget being spent on staff payments, 1 so there is a need to effectively utilise staffing systems to minimise the use of agency staff. 2 Manual staff nurse rotation systems in the NHS, UK have led to overstaffing in some shifts and understaffing in others, which can lead to additional temporary staff resource being required to meet demand. The NHS is currently paying large sums annually to temporary staff as a result of rostering problems. In this regard, Dunn et al. 2 and Sprinks 3 suggest control over staff budgets, especially in regard to agency staff. E-rostering systems are an effective way to manage staff shifts efficiently, so the Medic Trust decided to implement an e-rostering system throughout the Medic Trust hospitals. In-depth research in this area, however, has not been carried out. This study aims to determine the critical success factors (CSFs) in the successful implementation of an e-rostering system in a healthcare setting.
A qualitative case study research approach was adopted and therefore semi-structured interviews and personal observation were used for data collection. Fifteen interviews were conducted with different respondents. Most of the respondents were the end-users of the new system, including ward managers, deputy ward managers, and staff nurses. One of the researchers was directly involved in the implementation process and therefore provided input from their personal observations.
Research problem
Prior to the implementation of the e-rostering system, the ward managers at Medic Trust produced staff rosters on paper. The manual rostering system allowed the ward managers to allocate unlimited shifts according to staff request and the work shift patterns that they preferred; however, the e-rostering system would prevent this from happening. The new electronic system would require the managers to follow the rules and procedures to create a staff roster. The system would also require agreed templates to be in place within the system that will need to be in line with Trust policy. Ward managers have the responsibility for producing staff rosters which result in the smooth running of services. If a ward manager ignores the system rules and assigns shifts that accommodate staff requests, this could leave mandatory shifts vacant which would require a temporary nursing cover. The Department of Health’s (DH) report was based on the fact that NHS Trusts were not efficiently controlling the expenditure on the temporary nursing cover. Therefore, to overcome the deficiencies of a manual rostering system, the case organisation introduced an e-rostering system. With the introduction of the e-rostering system, there was a big challenge regarding successful implementation of the system. Therefore, this research tries to address the questions: what are the CSFs in implementing an e-rostering system and how do these factors affect the success of implementing the system?
Literature review
Along with service quality as a vital focus, healthcare organisations pursue cost-effectiveness as an important organisational goal. Technology is becoming a key enabler for healthcare organisations to attain these goals but there are certain challenges in the adoption of new technologies related to change management. 4 Changing or replacing existing practices is often not easy.5–7 Therefore, management needs to adopt strategies to overcome such challenges to implement changes. 8 For effective strategies, management needs to be aware of key factors that lead to success in change management and these are often referred to as CSFs.
CSFs, as proposed by Rockart, 9 are a guiding approach for managers to define information needs in order to reach the goals of the organisation. Regarding CSF methodology, Boynton and Zmud 10 state that ‘The CSF methodology is a procedure that attempts to make explicit those few key areas that dictate managerial or organizational success.’ Boynton and Zmud 10 typically place emphasis on specific areas and actions which are critical to the success of specific programmes and change management. At the moment, literature has many studies focusing on CSFs in various fields and contexts. In each field, certain CSFs are recommended under which success is likely to occur.
E-rostering system adoption and implementation stages are affected by human-related issues irrespective of the nature of the organisation, so resistance at earlier stages can be reduced by effective change management practices such as policy enforcement, communication, training, and evaluation. 4 Paschou et al. 11 have a good insight into the issues of e-rostering systems. They studied the characteristics required in an effective e-rostering system but worked in a mathematical context and provided mathematical modelling for an effective e-rostering system for health organisations. Table 1 is a summary of literature on CSFs with regards to area of healthcare systems.
Summary of the key literature related to critical success factors in healthcare systems.
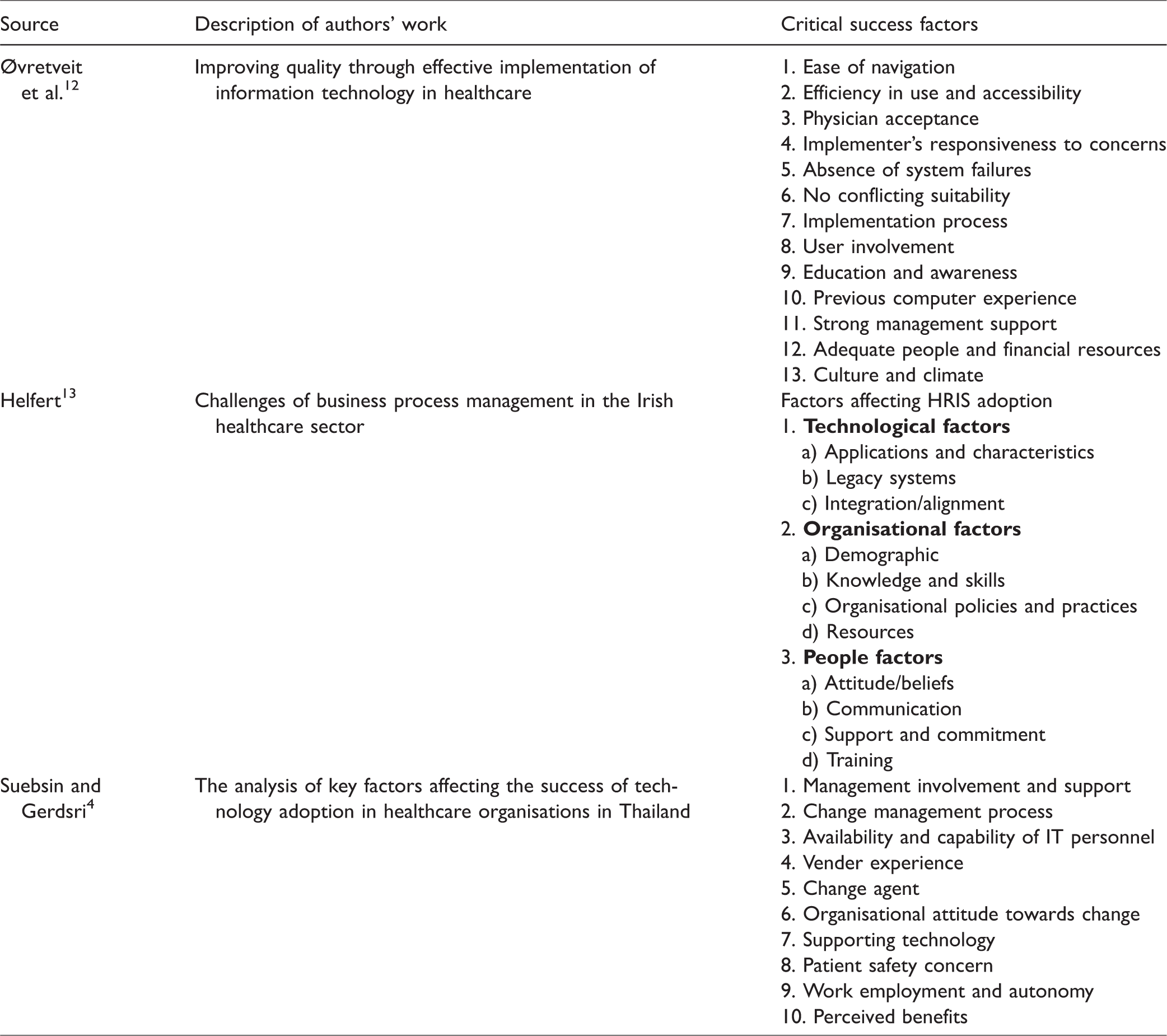
Table 1 mentions the CSFs for the implementation of information technology in health sector organisations. The research by Øvretveit et al. 12 is a good insight into CSFs for implementation of information technology in healthcare. They suggested 13 factors that have played a critical role in the implementation of electronic medical record (EMR) technology.
Nonetheless, there may be a few similarities in the implementation of the projects such as efficiency in use and access, an absence of system failure, education and awareness, and implementation process, which are common to in the implementation of any information technology. But the nature and implications of both projects vary as EMR is related to patient information while e-rostering is related to staff and their scheduling, therefore the CSFs of implementing EMR may not be same for an e-rostering system implementation; as a result, outcomes of this research are novel as no such study has been carried out previously. Helfert 13 has considered the standardisation of healthcare human resources and payroll in Ireland. He devised technological, organisational, and human factors affecting the implementation of healthcare human resources and payroll management systems. This was a national-level study involving a variety of staff involved in healthcare, whereas the current study focuses only on nursing staff, so the size of the organisation, the nature of the staff under study, and the objectives of both studies have differences.
The study by Suebsin and Gerdsri 4 also includes a number of CSFs in the adoption of ERP systems in healthcare organisations in Thailand. They suggested 10 CSFs (see Table 1), in the adoption of a new enterprise resource planning (ERP) system to order medicines from the supplier. Although these factors are significant for the adoption of technology related to ERP, the nature of the technology in the current study is different and therefore will have varying success factors. So far, the extant literature has no such study devising the CSFs in the implementation of e-rostering systems in the healthcare context. Therefore, this study helps to bridge this gap in existing research.
Research methods
This research is aimed at identifying the CSFs in the successful implementation of e-rostering systems in an NHS Trust. The case study approach was adopted using semi-structured interviews and personal observations were also used as one of the researchers was directly involved in the process of e-rostering system implementation.
The case study – Medic Trust
For the purpose of this research, the case study explores the CSFs in the implementation of the e-rostering system at a healthcare organisation which has been named as Medic Trust (a code name given to preserve the confidentiality of the participating organisation). The case study approach helps to investigate in-depth insights relating to issues in a real-world setting 14 and explains the elements behind management actions. It also reveals the organisational culture and human resource utilisation, and provides information about the activities, culture, and norms of the organisation. 15 According to Gibbert et al., 16 case studies are carried out in close interaction with practitioners who deal with managerial situations because this approach is suited to informing managerially relevant knowledge. The major factor in choosing this organisation was the direct involvement of one of the researchers in the implementation phase of the system which helped in the collection of data through participant observation and also provided easy access to the respondents.
The semi-structured interviews were conducted with end-users of the system and a total of 15 participants were interviewed. A semi-structured questionnaire was developed and refined to make the data reliable. The principal purpose of the interviews was to gain insight into the system implementation process and highlight the CSFs. The questionnaire contained basic questions on the impact of the system, potential resistances, motivators, and policy and compliance. Further in-depth questions were asked relating to the roles of the interviewees. With respect to nurses, additional questions were asked related to their knowledge on the functionality of the system, the fear of using the system, and the benefits of the system. The end-users were further engaged regarding the ease of use, training, support, and potential obstacles in the implementation. The managers were asked about the benefits of the system, control arrangements in the new system, policy compliance obstacles and countermeasures, other potential obstacles, and role of management in the effective implementation of the system.
The participants were randomly chosen to include the respondents involved in the implementation phase and were the core end-users of the system. The participants also included the ward manager and the deputy ward managers, as they are the main end-users of the system. An interview was also conducted with a matron to gain the views of senior management as they approve the work of the ward managers. To get a multidimensional result from this exercise, staff from different directorates in the organisation were invited for participation. All the participants were contacted personally, by telephone and through email, to get their prior consent. The participants were briefed about the project and process, and a consent form was signed by the participants accordingly. The interviews were conducted after the successful implementation of the project; therefore, the outcomes of the project were apparent and the interviewees deemed it as a successful project. The interviews were recorded through an audio recording tool and were stored and transcribed in full privacy. For participants’ privacy purposes, personal questions related to their names and other identifications were not included in the questionnaire.
One of the authors had held a post as a Rostering Administration Manager, prior to the old system being rolled out. Training on how to administrate the system and how to train the end-users was given to this author. The project team, along with one of the authors, included two other Rostering Administration Managers and a Project Manager. The plan we were to follow was to implement the system initially across five wards, and then the month after, extend the system to a further five wards. After the first two months, the system was extended to batches of two to three wards a month until fully implemented in all the nursing areas at the Trust. The experiences that the author had throughout the period as an implementation team member gave them valuable insight into the system implementation process.
Personal biasedness or subjectivity is a critical issue in case study data collection using participant observation. To minimise the possible personal bias and to enhance the methodological rigour, suggestions by Iacono et al. 17 were acted upon. The suggestion included: (a) let the facts speak for themselves; (b) analyse the evidence objectively through more than one source of data; and (c) distinguish as appropriate, facts from personal reflections. Thus, the methodological rigour was achieved and personal bias was minimised using these techniques.
The qualitative data were analysed with the help of NVivo software which helped to classify and code the data accordingly into the nodes. A thematic analysis approach was adopted and CSFs were inferred from the data as themes. Interview text was thoroughly reviewed to infer any CSFs, and statements that referred to the same factor were categorised into the same node. Finally, a list of all CSFs mentioned in the interviews was developed for discussion.
Results and discussions
The Medic Trust chose to implement an e-rostering system following the research carried out by the DH. In 2005, the DH had concerns that NHS Trusts were failing to control their expenditure on temporary nursing staff effectively. The National Audit Office 18 found that £8.3 billion were spent on nursing staff between 2004 and 2005 and £790 million were spent on the temporary nursing cover. The report stated that one of the ways to improve the use of temporary nursing cover was to introduce more effective staff rostering which could result in savings of between £25 and £50 million for the NHS. Therefore, the Medic Trust decided to implement an e-rostering system at their hospitals and this study is designed to investigate the CSFs in the implementation of the project.
The Medic Trust purchased the e-rostering system (called HealthRoster) from Manpower Software PLC. The system was purchased in 2008 and was fully implemented in 2009; it took about 12 months to carry out the full implementation. Once fully implemented, 93 nursing wards and units became live on the HealthRoster system. Prior to the e-rostering system, staff rosters were produced manually on paper. The e-rostering system helped to improve the productivity of the NHS workforce and aided effective healthcare. The Medic Trust stated key objectives of the system such as the achievement of potential savings, placing less dependency on agency nurses, and having a transparent rostering system. It was imperative that the system was fully utilised to achieve these objectives, requiring staff to adopt the system and take into account the skills and knowledge they had been given during the initial training on how to use the system.
At the outset, motivational factors, such as encouraging acceptance of the system, were observed, which paved the way for the initial success of the implementation phase. The other factors that made the implementation successful were technical support, committed leadership, having evidence of the advantages of the new system, clear goals and objectives, gradual change, senior management support, effective communication, and monitoring and reporting.
Policy and compliance
Having a rostering policy in place that staff adhere to was an objective that the Trust measured the success of with respect to the implementation of the system. Observations during the implementation phase highlighted the fact that with a manual rostering system, nursing wards were not following the policies and procedures strictly. In that situation, ward managers were creating rosters to satisfy the staff rather than actual demand. The monitoring of the manual rosters was also difficult and time consuming, which sometimes resulted in overstaffing in less busy times and understaffing in busy hours. This was the basic reason for increased wage expenses and dependency on agency nurses, which also affected the quality of service.
Although the staff were clear on the policy regarding the rostering system, lack of compliance was a major obstacle to achieve the objectives. In the e-rostering system, compliance monitoring became easier, which motivated the rostering staff to fully comply with it. So detailing a policy and having an easy compliance monitoring process are CSFs in the implementation of the e-rostering system. Siponen et al. 19 also support the notion that a policy and its compliance has a positive impact on the behaviour of employees.
Technical support
It was observed during the training sessions that end-users found the system difficult on the account of close monitoring of the system to ensure compliance with rostering policy. Therefore, the project team spent more time in supporting the end-users to help and motivate them to overcome this issue, which proved to be helpful in complying with the rostering policy. Regarding the support received, a ward manager also mentioned that, ‘The e-rostering team from the start have been fantastic. The team is always available and the service has been excellent and in my opinion that is why this has been successful.’
It was therefore evident that the technical support received from the project team helped the rostering managers in the effective compliance of the policy. Thus, the project team’s technical support became a success factor for the effective implementation of the e-rostering system.
Leadership
The leadership of the project has a significant impact on the successful implementation of the e-rostering system. 20 The project leaders had a clear vision, which gave inspiration to the staff. The project leaders also motivated the end-users and related staff through effective communication, which turned the barriers into success factors. Prompt feedback was given and the efforts of the staff were valued towards the accomplishment of the project, which also encouraged the end-users to strive towards the achievement of the project objectives. So it can be argued that effective leadership has a significant impact on project implementation.
Clear goals and objectives
At the initial stage, ward managers were confused with the new system; however, during the training sessions, they were provided with the goals and objectives of the project and any concerns raised were responded to in a satisfactory manner. Once the ward managers were clear about the goals and objectives of the project, their intentions focused towards the achievement of these. Such a notion is also supported by Costantino et al. 21 and Mathrani and Viehland, 22 who argue that clarity on project goals and objectives is an essential ingredient for achieving the benefits and the overall success of projects. Consequently, clarity in goals and objectives of the project proved to be a CSF for the project.23–25
Gradual change
During the interviews, all the participants agreed that the implementation schedule was gradual and they had experienced no material issues as the project was implemented according to a pre-planned schedule.21,26 Initially, the manual rostering processes were carried out in parallel to the electronic system and once end-users, managers, and matrons were satisfied with the accuracy of the system, the manual processes were no longer carried out. On the other hand, the system was implemented in phases, five wards a month. Regarding this implementation strategy, a ward manger stated that: ‘The system could have failed if it was to be implemented suddenly throughout the Trust.’
So, the gradual implementation phase helped the end-users and other stakeholders to understand the project, not only with help from the project team but also from colleagues in other wards who had experience of the system. So gradual change became significant to the successful embedding of the system, as too much haste at the implementation stage may well have led to premature results and project failure.22,27
Having evidence of the advantages of the new system
As already mentioned, the manual rostering system processes were carried out in parallel to the e-rostering system. The advantages of the new system such as time and cost saving, effectiveness and efficiency, close monitoring, easy compliance of the rostering policy, and accuracy of the system motivated the staff and the managers in terms of the effective implementation of the e-rostering system. In this regard, one of the ward managers mentioned that: ‘I actually thought that paper was more flexible, but e-rostering makes you put the times in, accurately.’
The statement shows that the staff realised the advantages of the new system, which was a motivation factor for the successful implementation of the system. Thus, evidence of the advantages of the new system became a CSF in the effective implementation of the system.
Senior management support
Support from senior management helped in making the project implementation possible.22,23 The senior managers provided guidance, resources, and feedback to the field managers 28 while the project team helped with troubleshooting. Regarding the support received from senior and project managers, staff confirmed that it was motivating to adopt the new system.
Thus, management support proved to be a factor for success in the e-rostering system implementation. Management support is also considered critical in project implementation in various other studies such as Anjum et al., 29 Bhatti, 30 Costantino et al., 21 Garg and Agarwal, 26 Mathrani and Viehland, 22 and Ravesteyn and Baterburg. 31
Effective communication
A strong communication link between all levels of staff proved helpful in overcoming resistance. Such results also validate the argument of Mullins 32 that effective communication at all levels is a better tool to overcome the resistance to change. With effective communication, the Medic Trust increased the acceptance level of the end-users and ward managers, which in result motivated them with regards to successful implementation. So effective communication has a critical role in the successful implementation of projects.26,27,30,31
Monitoring and reporting
Monitoring and reporting are critical aspects to keep the activities of employees aligned with the overall organisational strategy for project implementation.25,33 To ensure this, the supervising staff had responsibility for close monitoring and reporting, in order to address any problem in time and to ensure the successful implementation of the project. So the strategy of close monitoring and reporting played a critical role in successful implementation of the e-rostering system at the Medic Trust. The results of the identification of CSFs at the Medic Trust, construed from the observations and interviews, have been summarised in Table 2.
Summary of the research results with reported data collection method.
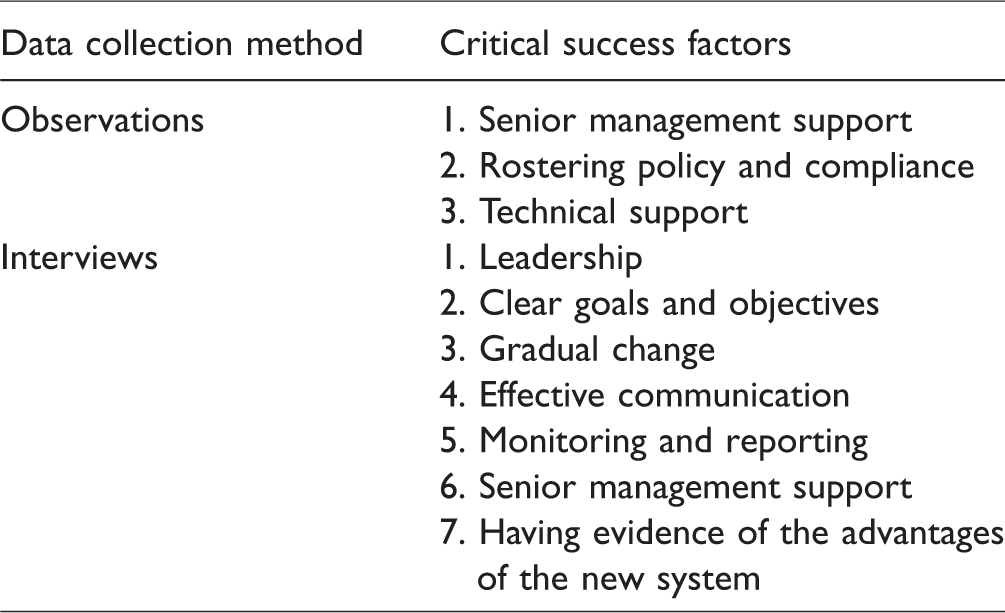
The observational research was significant as resistance was witnessed on a first-hand basis during the training sessions. End-user training sessions helped them overcome this resistance and fear of the unknown. Ward managers, deputy ward managers, and nurses were the end-users of the system, so they were provided training, but the matrons (their supervisors) were not provided with such training which created problems in the approval of rosters produced by the end-users on the system. In this instance, support from senior management helped matrons and end-users deal with any issues faced. The existence of the related policy and technical support was also a critical factor motivating the adoption of the e-rostering system. The interviews revealed similar barriers but also added more success factors. The respondents stated that effective leadership, clear objective, and gradual change were helpful in the effective implementation of the system. The respondents also revealed that effective communication, monitoring, and senior management support were also critical to this.
Along with the support for CSFs from many authors, there are also some criticisms. For example, Berg 34 is of the view that the same factors and management strategies that were successful in one organisation may not be similarly successful in other organisation. Berg 34 further argues that different organisations with varying sizes, different leadership and management styles, different cultures, different financial situations, and different environments may react differently with similar technological innovations or to similar implementation strategies. So, for effective implementation, organisational and environmental aspects should be considered and certain changes must be made in respect of implementation policies and strategies to best fit with organisational factors.
Conclusions
Staff scheduling has always been a critical problem, especially in healthcare organisations, as an overage or shortage of nursing staff adversely affects the objectives of healthcare organisations. In the absence of an e-rostering system, the Medic Trust was spending heavily on the temporary nursing cover. Implementation of information technology, especially at healthcare organisations, has always been a critical issue in terms of adoption and implementation.5–7 This study was aimed at exploring the CSFs for successful implementation of the e-rostering system at the Medic Trust. The CSFs for effective implementation were investigated and analysed in detail to discern their impact on the implementation process of e-rostering systems in health sector organisations.
For data collection, a case study method was adopted, and a qualitative approach was utilised to gain an in-depth insight into the facts. In our qualitative approach with respect to data collection, semi-structured interviews were conducted with 15 members of staff concerned with the project implementation. Personal observations were also part of data collection as one of the researchers was personally involved in the project implementation.
This study explores some key factors which were critical for the implementation of the e-rostering system at a healthcare organisation. These include senior management support, technical support, effective leadership, clear goals and objectives, gradual change, effective communication, and monitoring and reporting. This set of factors has not been explored in the current context, which is the novel contribution of this research. In the real-world setting, this study would be helpful to managers for the successful implementation of e-rostering, especially in a healthcare setting.
Like other studies, this research also has some limitations. As the study was conducted at an NHS healthcare organisation in the UK, there may cultural differences in other countries which are not addressed here. So it may be possible that studies in countries with different cultures may have different outcomes. Also, this study was limited to an NHS Trust so there may be a possibility of varying results in a private healthcare setting. As mentioned previously, one of the authors was involved in the implementation of the project, so there may be personal bias in the data in spite of taking measures to minimise this. Therefore, the authors suggest future studies with a quantitative data collection approach, in different cultures and private healthcare organisations. These CSFs can also be analysed for their application in contexts other than healthcare, so future studies will also be helpful in generalising the outcomes of this study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.