
Abstract
Research on governance often assumes that governance requires combinations of hierarchical, market and network co-ordination. However, governance versatility – understood as the existence of a repertoire of different modes of coordination – is not a characteristic of all instances of governance. The aim of this paper is to offer a more thorough analysis by exploring existing levels of governance versatility and how these are influenced by institutional profiles. Our comparative study of primary care performance across six jurisdictions suggests that higher levels of governance versatility can be shaped by very different institutional profiles. Our analysis raises important questions for future studies of governance versatility.
Introduction
Governance has emerged as a common conceptual perspective across a number of literatures for understanding changes in policies and delivery of public services. This rests on a more or less explicit assumption that governance typically requires combinations of hierarchical, market and network co-ordination (Bouckaert et al., 2010; Koppenjan et al., 2019). However, we should not assume governance versatility – understood as the use of different modes of coordination – is a characteristic of all instances of governance.
Against this background, this paper aims to explore existing levels of governance versatility and how these are influenced by institutional profiles. We develop an analytical framework designed to explore how political and administrative institutions at macro and meso levels shape the degree of governance versatility. We apply this framework to a cross-country comparative study of the governance of primary care performance across six jurisdictions. We chose this policy domain, as its governance has settled after a period of change and is subject to the influence of institutions at different levels. We conduct a small comparison as the in-depth understanding of cases can help conceptualise the relationship between governance versatility and institutions. We select six jurisdictions – Australia, Denmark, Germany, New Zealand, the Netherlands and Canada – based on an initial empirical puzzle and interesting variations in institutional profiles. Our study suggests that higher levels of governance versatility can reflect very different institutional profiles.
Understanding governance versatility and institutions
In the public policy, public management and organisational studies literatures over the past 20–30 years, research on “modes of coordination” has emerged as an important conceptual framework for understanding longer term trajectories of change (Powell, 1990; Pierre and Peters, 2020; Newman, 2001). We define governance as a process by which the activities of multiple actors (both state and non-state) are co-ordinated to collectively produce public policy “effects” (Lowndes and Skelcher, 1998; Rhodes, 1997). The multiple modes framework is centred on the distinction between ideal types of social co-ordination mechanisms. Scholars typically identify three modes of coordination, namely hierarchy, market and network (HMN) (Powell, 1990; Pierre and Peters, 2020).
Much of the recent literature on governance focuses on the development of “hybrid” forms of governance where governance involves combinations of markets, hierarchies and networks (Meuleman, 2008). Hybridity is not necessarily a new phenomenon but is increasing in prevalence and scale in public policy (Denis et al., 2015; Koppenjan et al., 2019). Hybridity has increasingly become associated with normative arguments that hybrid forms can result in more advanced, more robust or flexible and adaptable, or more effective governance (Leixnering et al., 2020; Pahl-Wostl, 2019). Meuleman (2008, 67) summarises the general advantages of hybridity as offering a richer tool box for public managers. Koppenjan and colleagues (2019, 137) specifically point to the possibilities of hybrid governance arrangements to help to complement, react to and compensate for the weaknesses of existing, single modes of coordination.
Hybridity presumes that multiple modes of coordination operate simultaneously. Hood (2000) shows that multiple modes of co-ordination may follow each other sequentially, rather than being present simultaneously as is implied by the term ‘hybridity’. Such moves are usually incomplete in that strong traces of previous modes often remain prominent (Newman, 2001). In line with the normative perspective, the literature focuses on the functionality of hybridity. Rather than promoting adaptable and resilient governance, potentially insurmountable tensions may emerge as a consequence of governance pulling into opposite directions, reflecting distinct, underlying logics (Bode and Firbank, 2009; Newman, 2001).
However, if the emergence of governance hybridity is a historical process, then this emergence is likely to be uneven. Therefore, there is no reason, ipso facto, to assume that multiple modes is a feature of all instances of governance. For any specific policy domain in a specific jurisdiction, we argue that the existence of multiple modes of coordination needs to be treated as an open, empirical question. This also draws attention to the specific institutional profiles that can support existing mode(s) of coordination. Examples of policy domains where there is an absence of governance resembling any mode (Burau and Clavier, 2018; Tenbensel et al., 2011) powerfully underline this point.
In this article, we adopt the term “governance versatility” to ask open questions about the use of multiple modes of coordination in a specific policy domain and how this relates to underlying institutional profiles. Governance versatility refers to the existence of a repertoire of different modes of coordination (Jessop, 2002, 2003; Tenbensel, 2008). Versatility can be a feature of how state agencies attempt to steer (cf. Jessop’s metagovernance), but it also includes the collective capacity of state and non-state actors to co-ordinate governance of a specific policy domain.
In any specific policy domain, governance resembling each of the ideal types may be present or absent. This raises important questions about what specific governance versatility there is and in what institutional profiles it exists. To our knowledge, these questions have only been addressed either in general terms, or by focusing on specific case studies where hybrid governance has already occurred. However, there has been little research that seeks to explore more thoroughly the extent to which specific policy domains are characterised by governance versatility and the relations to different institutional profiles.
These sorts of question are best approached through a comparative lens. One possibility is to compare different policy domains within the same jurisdiction. This approach would highlight the role of different contextual factors of specific policy domains, but it would be difficult to generalise findings beyond the country/jurisdiction of interest. The alternative approach, which we adopt, is to focus on a single specific policy domain and to compare governance versatility across multiple jurisdictions. Arguably, such an approach is capable of highlighting the role of national policy contexts (Bouckaert et al., 2010).
Institutional analysis provides a well-established toolbox for this comparative approach. The limited work that has been done comes from the historical institutionalist strand of comparative health policy research. Institutionalist approaches to analysing governance versatility include elements of “macro” and domain-specific (“meso”) institutions. In her influential work on health policy change, Tuohy (1999) sought to understand what shaped variations of governance mixes over time and between jurisdictions. She showed how macro-institutional conditions such as federal fragmentation and the rarity of single-party majority government meant that Canada exhibited less versatility compared to the US and the UK (Tuohy, 1999, 246). Tenbensel’s (2008) comparison of Canadian and New Zealand primary care reform and cost control, highlights the importance of meso-institutions. Corporatist bargaining between state and profession in Canadian provinces constrained the governance versatility in both these policy domains compared to New Zealand. In their comparative study of medical governance in four European countries, Burau and colleagues (2009; similarly Brunn, 2020; Kuhlmann and Allsop, 2008) identify different types of meso-institutions to explain different patterns of modes of coordination. This includes health care states (closely related to health care systems) and their degrees of decentralisation, together with medical authority as the relative strength of professional autonomy.
Building on this, we use a more explicit framework for the comparative analysis of governance versatility. This allows for a deeper exploration of the extent of governance versatility and how this reflects the specific interplay between different types of institutions at different levels. We pose the following research questions: How does the level of governance versatility in a specific policy domain vary across different countries/jurisdictions, and how does this relate to differences in institutional profiles in these countries/jurisdictions?
Our analytical framework
Our analytical framework distinguishes between different modes of coordination and between various institutions. Existing institutional analyses stress the importance of institutions at different levels. Our overall focus is primary care, as this policy domain is characterised by strong meso-institutions. Modes of coordination can vary between different sub-domains. We chose the governance of primary care performance. This refers to efforts to govern the performance of primary care providers through the application, interpretation and response to measurable performance indicators. The most well-known example of the last 20 years is England’s Quality and Outcomes Framework (McDonald et al., 2008). In most high-income countries, governments have had little direct control over primary care services, which is generally delivered by sole practitioners or small provider organisations (Tenbensel and Burau, 2017). However, due to increasing availability of service-level data, along with health sector organisational reforms, a range of top-down and bottom-up processes have led to the introduction of performance frameworks in primary care in many countries.
Overview of analytical framework.
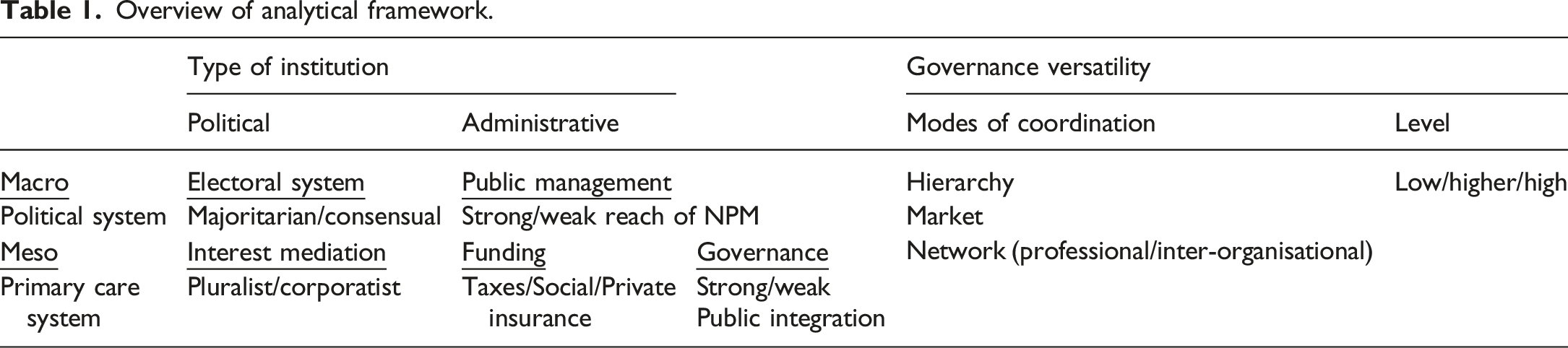
We use hierarchy, market, and network as ideal typical modes of coordination as the basis of our comparison of governance versatility in primary care performance. Hierarchical modes of coordination involve the direct use of state authority. For example, governmental funding of primary care services can be tied to satisfactory performance against defined criteria (Tenbensel and Burau, 2017). Stronger versions of hierarchy involve the use of sanctions for non-compliance, whereas “softer” hierarchical approaches are couched in terms of command and control, but compliance may be patchy or even non-existent (Jacobs et al., 2006). Market modes of coordination have generally been associated with “pay-for-performance” initiatives in primary care (Cashin, 2014). General practitioners are incentivised by the prospect of increased income and/or increased autonomy to meet specified performance requirements (McDonald et al., 2008). For network modes of coordination there are two varieties. Professional network modes of coordination involve collegial processes of developing relevant indicators, and feedback processes are institutionalised in different forms of professional self-regulation (Kringos et al., 2013). Inter-organisational network modes of coordination operationalise collective objectives of primary care performance through networks of provider organisations (Lewis, 2004).
Turning to institutions, we distinguish between political and administrative institutions at macro and meso levels. Relevant macro-political institutions concern the electoral system (Lijphart, 2012). The majoritarian variant gives governments solid electoral majorities that offers them greater capacity to devise more decisive substantive governance. Consensual electoral institutions rely on political compromise and limit this type of capacity. Based on this, we may expect that majoritarian electoral systems foster greater governance versatility compared to consensual systems (Weaver and Rockman, 1993). Alternatively, the greater capacity in majoritarian systems may include the wholesale introduction of one single mode, whereas consensual systems may support a more complex layering of modes (Van de Bovenkamp et al., 2013).
For macro-administrative institutions, the key distinction among high-income countries has been the reach of New Public Management (NPM)-related practices (Pollitt and Bouckaert, 2017). NPM is typically understood as a concerted attempt to introduce market mechanisms into the public sector, often in form of hierarchy/market combinations such as publicly regulated markets and competitive contracting. Our choice of NPM is shaped by the specific content of our chosen policy domain. The governance of performance emerged as a key feature of the NPM movement in the 1990s (Pollitt and Bouckaert, 2017). On this basis it is reasonable to assume that the strength of NPM is the key element of macro-administrative institutions that may have a significant influence on the nature of primary care performance management (Blank et al., 2018). One expectation may be that a higher degree of penetration of NPM principles and practices facilitates the use of market governance and therefore greater governance versatility. Alternatively, jurisdictions with high reach of NPM may be more prone to developing a governance “monoculture”, driving out alternative modes (Hood, 2000).
In relation to meso-political institutions, we focus on interest mediation in the primary care system, drawing on the distinction between pluralism and corporatism (Blank et al., 2018). The key questions are how primary care interests (generally medical practitioners) are organised and how their organisations are incorporated into policy processes. In relation to governance versatility, one expectation is that state actors may have more room for devising governance in pluralist processes, whereas in corporatist processes, the power of other parties may limit experimentation and by extension governance versatility (Tenbensel and Burau, 2017). Alternatively, corporatism may foster versatility because it encompasses pragmatic compromises between state-driven hierarchical and sector-driven network logics (Vrangbæk, 2009).
Finally, in terms of meso-administrative institutions, we include institutions related to the funding and governance of primary care (Blank et al., 2018). Funding rests on a balance between taxes, social insurance, private insurance and direct payments. Governance relates to the degree largely private medical practices are incorporated into a primary health care system that is predominantly publicly funded and regulated. Together, these institutions influence the relative public control over primary care and one expectation maybe that public control is conducive to a greater governance versatility. Alternatively, when public integration is weak, this might provide conducive conditions for a range of governance types to emerge in a bottom-up way (Tenbensel and Burau, 2017).
Methods
In this paper, we apply the analytical framework to a comparison across selected jurisdictions. This based on a qualitative, multiple-case design, where the jurisdictions are the individual cases (Yin, 2018). Our case selection is inspired by an abductive logic (Yanow, 2014). Initially, we were puzzled that there seemed so little governance of primary care performance, considering our prior knowledge from comparative health policy about the great variation among health systems. Because we are interested in the relationship between institutions and modes of co-ordination in primary care performance management, we adopted a method that focused on ‘institutional profiles’. We selected jurisdictions that show interesting variation in terms of combinations of institutional characteristics as identified in our analytical framework. However, we treat the influence of institutions as an open question. Our jurisdictions are Australia, Denmark, Germany, New Zealand, the Netherlands and Québec. In the initial analysis, novel patterns of institutional variations emerged. We grouped our cases in three pairs of institutional profiles, where each pair shares a very similar profile of institutional characteristics, but with significant variety across the three pairs.
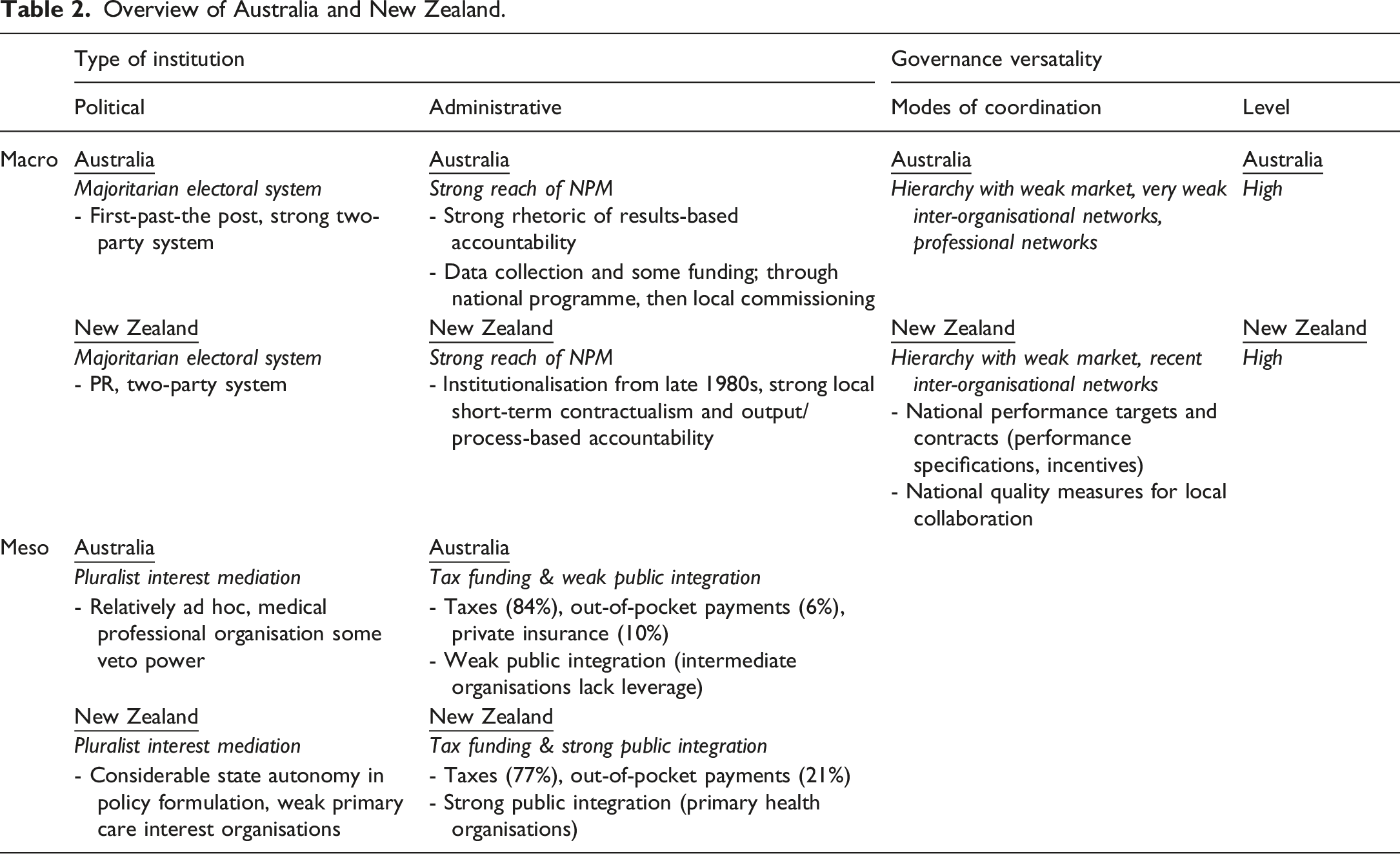
In terms of meso-institutions, Australia and New Zealand are characterised by tax funding as the main source of primary care funding, but private funding remains significant. This is coupled with predominantly pluralist interest mediation, which allows for degrees of state autonomy. At the macro-level, this is embedded in electoral and party systems that continue to manifest majoritarian patterns, and a strong reach of NPM, which has had an influence on primary care in terms of both ideas and policy programmes. The institutional conditions are very different in Germany and the Netherlands, where social insurance funding co-exists with corporatist interest mediation. Funding arrangements mitigate against government control and put third-party payers in an influential position. Together with the medical profession, insurance funders are key players in national arenas for policy making. Both countries are characterised by a consensual electoral system and a relatively weak reach of NPM at the macro-level. Denmark and Québec offer yet another combination of institutional conditions, with some similarities to each of the other pairs. Here, tax funding is coupled with corporatist interest mediation at the meso-level. The existence of de facto third-party payers and the close involvement of the medical profession mitigates the increasing political control typically associated with tax funding. At the macro-level, the reach of NPM is weak in both jurisdictions. This pair differs only in terms of macro political institutions, with Denmark a consensualist democracy and Québec more majoritarian.
The following analysis is based on six case studies prepared by authors with specific expertise in their jurisdiction. Each case study followed the analytical framework presented above and collected material on modes of coordination and institutional profiles. In line with our cross-sectional approach, the country case studies analyse the governance of primary care performance in its present form (2022). We assume that governance arrangements have settled after different processes of introducing more explicit governance of primary care performance over the past two decades. The material included secondary sources (research articles and grey literature reports) and primary sources (policy documents). The authors also drew on their expert knowledge honed in through many years of research in health policy in their respective jurisdictions.
Analysis
In this section, we explore the level of governance versatility in primary care performance across the six jurisdictions. Our aim is to explore the institutional profiles that underpin particular patterns of governance versatility. By and large, these patterns revealed important differences between the three pairs of jurisdictions, and notable similarities within each of our pairs.
Australia and New Zealand
Overview of Australia and New Zealand.
The Australian story is one of experimentation with the full range of coordination modes. Hierarchical governance of primary care performance in relation to data collection and some funding began in the early 2000s, although it has never been strongly tied to sanctions. The National Quality Performance System (NQPS) in 2003 (Sibthorpe and Gardner, 2007) and the National Performance Authority (NPA) in 2011–12 are examples of well-developed policy designs for hierarchical governance. The NQPS was also a nationally co-ordinated attempt to develop a system of performance management (Foster et al., 2016) that was influenced by the English Quality-and-Outcomes-Framework. The NQPS also incorporated professional networks and built on existing quality improvement approaches. Initially, indicators were devised, but specific mechanisms for funding performance were not developed.
Since 2013, the onus of developing performance frameworks has been devolved to 31 Primary Health Networks (PHNs), although the Commonwealth Department of Health plays a facilitative role. In theory, PHNs are responsible for commissioning services in their local area (Australian Department of Health, 2019). The federal government envisaged that commissioning could incorporate both competitive contracting (market) and collaborative, inter-organisational modes for governing performance. However, few extensive examples of either market or network governance arrangements have emerged beyond small-scale pilots of incentive-based funding for quality improvement.
New Zealand has also developed the full range of hierarchical, market, and inter-organisational network modes of governing primary care performance over the past 20 years. Starting around 2005, a small proportion of funding for Primary Health Organisations and their general practices utilised pay for performance (market governance). From around 2010, these P4P mechanisms worked in tandem with hierarchical performance targets and national contracts embedded in the Primary Health Organisation Performance Programme (PPP) that included performance specifications (Smith, 2015). Examples of performance indicators included the percentage of two-year-old children who are fully immunised and the percentage of smokers given smoking cessation advice by their primary care doctor (Ashton, 2015).
Since 2016, the emphasis on hierarchical and market governance in New Zealand has been overlaid with, and partially superseded by, collaborative, inter-organisational network governance in the form of the System Level Measures Framework (Chalmers et al., 2017; Tenbensel et al., 2021). The most recent policy iteration, the Health System Indicators framework has confirmed this move towards inter-organisational network governance, while downplaying of targets and pay for performance (Little, 2021). The appearance of network governance is largely a consequence of frustration within government and provider groups with the limitations and unintended consequences of market and hierarchical governance, but vestiges of hierarchical and market approaches persist.
We suggest that this pattern of governance versatility is strongly related to the institutions that the two countries share. At the centre of the institutional profile are tax funding and pluralist interest mediation. Tax funding makes for high government control and in combination with high reach of NPM creates a policy environment in which hierarchical and market, and more recently network governance in primary care have been prominent in each government’s toolbox. New Zealand entrenched a strong contractualist NPM regime across the whole public sector in the 1990s, with hard-wired new accountability instruments focused on outputs and processes. In Australia, NPM has had a deep impact on social, employment, and not-for-profit health services (Dwyer et al., 2011), but to date, mainstream primary care has largely been beyond its reach. Nevertheless, the ideas regarding performance management of primary care strongly reflect this NPM heritage.
The capacity of governments to develop hierarchical, market and network governance in primary care is also reinforced by traditions of pluralist interest mediation in which primary care providers are not formally integrated into policymaking processes. In Australia, provider involvement in primary care policy decision-making is relatively ad hoc, despite a reasonably strong veto power by the medical profession. In New Zealand, the state has more autonomy in policy formulation, and the organisations representing primary care interests are also fragmented. This makes for a centralised form of fluid pluralism that only involves general practitioners on an ad hoc basis in policy formulation. Veto power, where exercised, tends to be manifest in implementation processes (Tenbensel and Ashton, 2020). Both countries also have a history of predominantly majoritarian electoral systems that produce alternating majority governing coalitions. This history has tended to foster more pluralist forms of interest mediation Lijphart (2012).
The reinforcing dynamics between tax funding, high reach of NPM and pluralist interest mediation is attenuated in both countries. The main source of primary care funding is taxation, but significant degrees of private funding somewhat dilute the level of state influence. Out-of-pocket payments make up around 20% of primary care funding. Further, the overall reinforcing dynamics is more attenuated in Australia than in New Zealand, reflecting different degrees of public integration of primary care (meso-administrative). In New Zealand, there has been comparatively strong public integration of primary care through PHOs as intermediate organisations. By comparison, the development and influence of intermediate primary care organisations (e.g., Medicare Locals, PHNs) in Australia have been weak and subject to regular restructuring since 2000. Most Australian primary care funding is distributed through a reimbursement model (Medicare) that bypasses these intermediate organisations, and this institutional feature significantly limits the reach of the governance of primary care performance in Australia.
Germany and the Netherlands
Overview of Germany and the Netherlands.
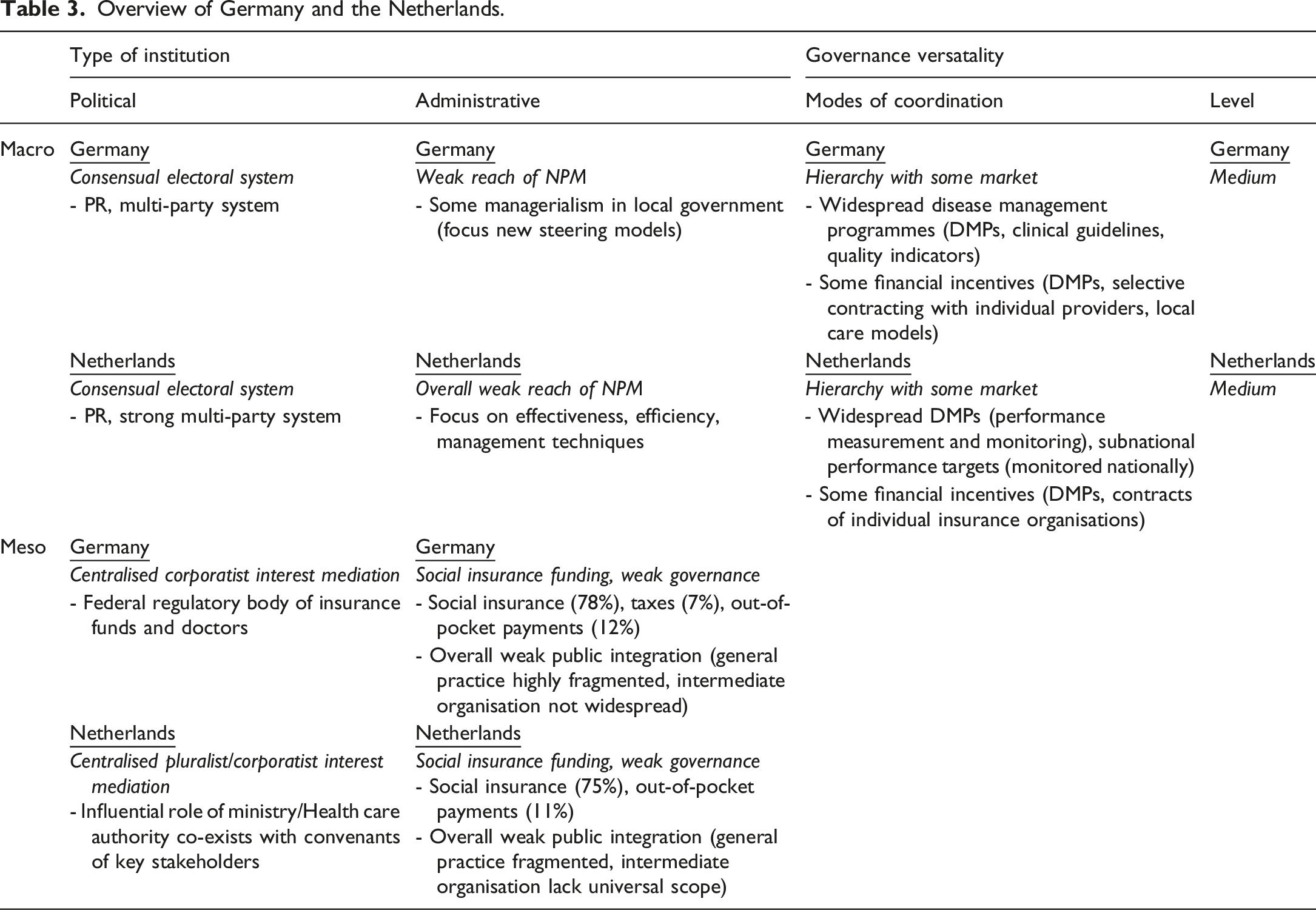
In Germany, Disease Management Programmes for major chronic illnesses are widespread although they are voluntary. The programmes are administered by the Joint Self-Administration of insurance funds and doctors as the central, quasi-public health authority. They include clinical guidelines and quality indicators as well as moderate financial incentives (Busse et al., 2017). For nearly a decade, the programmes have coexisted with more bottom-up initiatives, supported by selective contracting with some financial incentives with individual providers (introduced in 2011) and financial support earmarked for innovative local care models (introduced in 2015). This has encouraged the development of Medical Care Centres and integrated care networks (Müller et al., 2016). The picture is somewhat similar in the Netherlands. Disease Management Programmes have been part of the general practice contract since 2010 and combine financial incentives (bundled payments) with performance measurement (treatment and outcomes) and monitoring (Kroneman et al., 2016). Contracts of individual insurance organisations can also include elements of pay for performance. Additional subnational performance targets exist based on the policy goals formulated by the National Convenant on General Practice Care and which the Dutch Health Care Authority monitors.
Compared to Australia and New Zealand, governance versatility in the two jurisdictions is only medium, drawing primarily on hierarchy and markets, whereas network governance is more situated. However, the existence of market governance is interesting for two reasons. Firstly, NPM is comparatively weak in both countries. In Germany, Weberian bureaucracy and hierarchy continue to be the dominant structural principles for public management (Hammerschmid and Oprisor, 2016). In the Netherlands, NPM does have some influence but is limited to management techniques designed to address organisational efficiency and effectiveness (Jilke et al., 2016).
Secondly, low levels of public integration further shield primary care from potential incursions from management. In the two jurisdictions, primary care is fragmented; doctors work as private practitioners, and the organisational size of practices is not necessarily large. Single-handed practices continue to prevail in Germany, and in terms of the number of general practitioners, the practice size in the Netherlands is also comparatively small (Groenewegen et al., 2015). Although intermediate primary care organisations exist, they are fragmented by specific purpose (as the organisations of Community Health Centres, Chronic Care Groups and Out-of-hours Cooperatives in the Netherlands) or they do not exist across the healthcare system as a whole (as the Medical Care Centres in Germany).
This suggests that there must be other institutions that support the inclusion of market governance. Here, funding from social insurance emerges as key. The predominance of this type of funding in both jurisdictions puts third-party payers in an influential position, and this further mitigates against government control over selection of modes of coordination. Yet, the principle of social insurance builds on a separation of purchaser and provider functions; this offers a natural lever for market governance.
Corporatist interest mediation is prominent in the two jurisdictions and this relates to an electoral system based on proportional representation and strong multi-party systems. Importantly, corporatism can offer an arena to negotiate the specific nature of the purchaser-provider split and the extent to which it embraces competition. Here, the medical profession plays an influential role across the two jurisdictions. The respective arenas of the Federal Joint Committee of insurance funds and doctors as the main platform in Germany (Busse and Blümel, 2014) and the national-level convenant in the Netherlands both include the peak organisations of professions in addition to the insurance funds, the Ministry of Health, and the National Patient Federation (Kroneman et al., 2016).
There are also important differences between the two jurisdictions. In Germany, an increasingly centralised corporatism at the federal level co-exists with sub-central corporatisms that are based on more or less ad hoc alliances between healthcare providers and insurance funds (Busse et al., 2017). The institutions of interest mediation in the primary care system in the Netherlands are more hybrid, and centralised corporatism co-exists with centralised pluralism. The latter also gives the Ministry of Health and the Health Care Authority some influence over doctors’ interests (Meloen et al., 2001).
Denmark and Québec
Overview of Denmark and Québec.
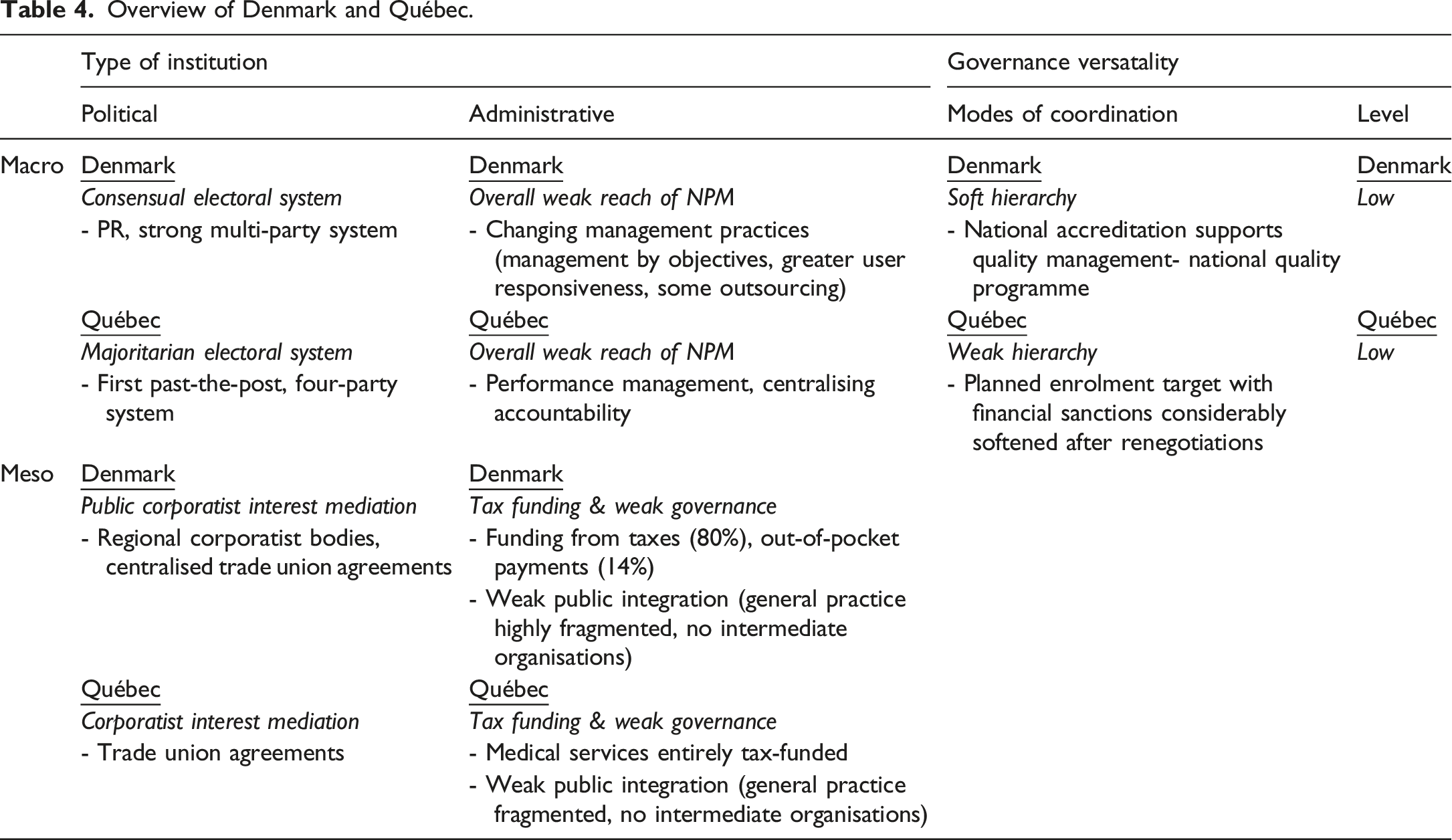
In the two jurisdictions, the state makes some performance demands on the primary care sector but demands lack teeth in terms of monitoring and sanctions and are limited in scope. In Denmark, hierarchy is soft, sanctions are few, and the primary focus is on developing quality management (Vrangbæk, 2009). A major element of performance management is mandatory accreditation, drawing on standards developed with general practice and including ongoing quality assessment (Forde et al., 2016). The initial idea was to connect accreditation to a system for collecting data about services provided by general practice. However, this was abandoned as sharing data with regions (as funders) proved highly controversial (Deloitte, 2014). Since 2018, a new quality programme has gradually replaced accreditation (RLTN, 2017). It is based on voluntary “quality cooperatives”, which bring together local practices to engage in systematic quality development. The programme combines hierarchy with some elements of professional network governance. The programme has also initiated the development of quality indicators for general practice and a corresponding database, but again lacks sanctions.
In Québec, prior to 2015 governance of primary care performance was hierarchical, but also lacked teeth. There were some examples of performance targets relating to access to care, continuity of care, and equity that applied to Family Medicine Groups, but participation in these groups was voluntary (Pomey et al., 2009). This changed after 2015 with the attempt to impose hierarchical governance in the form of enrolment rates, productivity targets, which were accompanied by sanctions for non-compliance (Pineault et al., 2016). Pressures by the trade union of general practitioners led to renegotiations, whereby government temporarily dropped sanctions in return for doctors accepting targets and their responsibility for achieving them (Denis et al., 2017).
In terms of funding, taxes are the main source in both jurisdictions, typically increasing political control and facilitating greater governance versatility. However, the existence of de facto third-party payers has a mitigating effect as it introduces an intermediate level that lacks teeth. In Denmark, these are the regions that have traditionally acted as payers, transferring funds for services delivered, rather than purchasers, defining services and monitoring their delivery (Hansen et al., 2010). The regions are thus very similar to the Health Insurance Plan (RAMQ) in Québec, which is responsible for the day-to-day administration of payments of general practitioners (Gagné and Sirois, 2016). This includes implementing any new agreements between government and the trade union of general practitioners and dealing with cases of suspected fraud.
In contrast to Australia and New Zealand, there is a different influence on versatility when tax-funding is combined with corporatist interest mediation. The close involvement of the medical profession is likely to smooth any sharp corners that hierarchical modes of coordination may have. Denmark has a form of public corporatism that operates through regional corporatist bodies and national trade union agreements (Forde et al., 2016; Vrangbæk, 2009). Negotiations have to tread carefully because of low trust between the parties and the weak support by rank-and-file general practitioners over the past years (Hougaard, 2013). In Québec, interest mediation in the primary care system has traditionally been highly corporatist and overshadows any influence of the majoritarian electoral system. The introduction of family medicine groups has allowed government to make demands beyond agreements over pay, although the trade union of general practitioners has won a number of concessions in relation to performance management (Denis et al., 2017; Pomey et al., 2009).
In both jurisdictions, third-party payers dilute the public control of tax funding and the inclusion of organised medicine in corporatist interest mediation weakens support for the introduction of market governance. This combination of meso-institutional conditions serves to filter the potential impact of NPM and existing elements have emphasised hierarchical components. In Denmark, NPM has been embedded in a modernising agenda, and the focus has been on changing management practices through management by objectives, greater user responsiveness, and some outsourcing (Greve and Ejersbo, 2016). NPM in Québec has taken the form of an expansion of performance management, such as lean management, and attempts to reinforce the accountability of health managers and providers to central authority (Quesnel-Vallée and Carter, 2018). This has been coupled with growing centralisation and massive restructuring.
The relative absence of both market and network governance, and the limited teeth of hierarchical governance, are reinforced by weak levels of public integration as there are no intermediary organisations connecting individual practices to sub-central administrative levels. This is significant as primary care is also fragmented, although to slightly different degrees. In Denmark, only 26% of practices have four or more general practitioners (PLO, 2017), while in Québec Family Medicine Groups with 6–10 physicians have become the norm. Taken together, general practice emerges as a satellite service separate from hospitals and other primary care (and social care) services at the local level. This is surprising particularly in the case of Québec, which is otherwise characterised by a highly integrated system structurally of health and social care services (Tenbensel et al., 2017). In both jurisdictions, this low level of public integration has served to shield primary care from managerial reforms in the wider healthcare system and in public services at large. Due to this weak public integration, there are few viable channels for network approaches to performance management to emerge from the bottom up, and limited motivation amongst providers to develop them.
Macro-political institutions are less influential in shaping the versatility of the governance of primary care performance. In Denmark the consensual electoral system with elections based on proportional representation and a strong multi-party system reinforces corporatist interest mediation (Lijphart, 2012), but Québec provides a good example of highly developed corporatist institutions that flourish in a majoritarian context because of the specific evolution of health system institutions.
Discussion
Levels of governance versatility and underlying institutional profiles
Overview of findings.
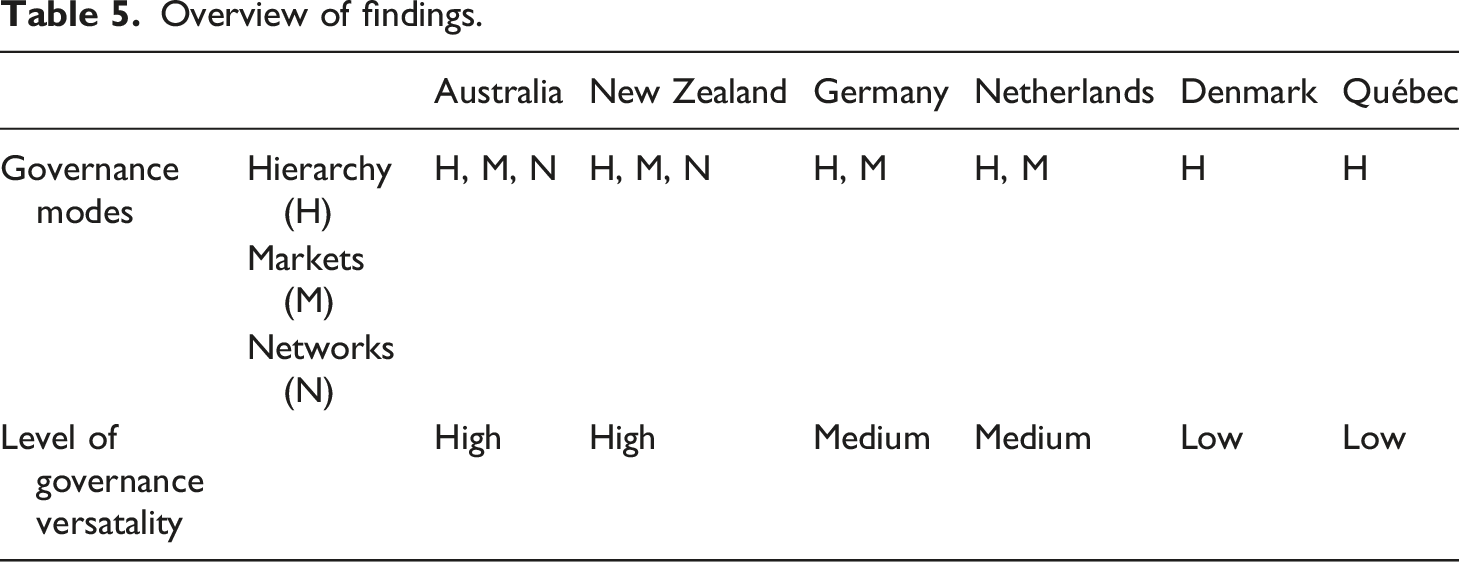
Our analysis identifies three levels of governance versatility. The level of governance versatility is high in Australia and New Zealand with a combination of hierarchy, market and network governance, medium in Germany and the Netherlands with a co-existence of primarily hierarchy and market governance, and low in Denmark and Québec, where soft forms of hierarchy prevail. Given that the levels match our three pairs, this provides evidence supporting the contention that some institutional conditions shape governance versatility.
Macro- and meso-political and administrative institutions relate to the level of governance versatility in the form of three distinct sets of institutional profiles where individual institutions relate to each other in specific ways. There are two very distinct (and contrasting) profiles underpinning high/moderate levels of versatility. Profile one is Tax Funding + High Reach of NPM + Pluralist Interest Mediation, and profile two is Social Insurance Funding +(Centralised) Corporatist Interest Mediation + Consensual Electoral System. Conversely, Profile three of Tax Funding + Corporatist Interest Mediation + Low Degree of Public Integration is associated with a low level of versatility. Our analysis suggests that the low level of versatility in Denmark and Québec reflects a combination of institutions, whereby the state has the incentive to attempt some form of performance management but can only do so as far as the capacities of third-party payers can reach and as the medical profession is willing to go. The high/medium level in the other pairs points to the common presence of a purchaser-provider split, although institutional origins vary. In Germany and the Netherlands, this is related to funding based on social insurance and more centralised corporatist interest mediation supported by a consensual electoral system. In Australia and New Zealand, the purchaser-provider split is shaped by pluralist interest mediation in a tax-funded system, and this dynamic is amplified by the institutional logics of a strong reach of NPM.
Implications for studying varieties of governance versatility
Our analysis suggests a number of questions for future research. A first question concerns the most appropriate level for studying governance versatility. Across our cases, meso-institutions always matter, whereas macro-institutions matter sometimes and whether they do or not is highly contextual. This may reflect the specific meso-institutions of primary care, which build on the deep-seated concordat between primary care doctors and the state in a context in which universalist services are provided by private, for-profit small businesses (Burau, 2016). Not surprisingly, we only have one case out of six where there is strong public integration (New Zealand) and that differs from its partner. Alternatively, the relative importance of meso-institutions in the governance of primary care performance may in fact be an indication of the broader relevance of policy domains as the most appropriate level for studying governance versatility. This resonates with Lowi’s (1972) observation that policy problems determine policy making and Richardson’s (2012) point about the sectorisation of policy-making in the co-existence of different policy styles. One avenue for future research could be to study governance versatility in “families of policy domains”, which share central characteristics. Examples are the influence of professional expertise (such as in healthcare) or the prominent role played by civil society organisations (such as in international development) or the importance of private industry (such as in utilities).
Secondly, our analysis raises questions about the importance of considering time when studying governance versatility. For example, in Australia and New Zealand, the introduction of network governance was meant to compensate for the deficiencies of existing hierarchy and market governance. Future research needs to treat governance versatility as a complex phenomenon that can vary not only across jurisdictions, but also over time. Newman (2001) and others acknowledge the importance of time when they stress the non-linearity of governance change. However, their view of time emerges as rather functional, whereby time leads to different modes of coordination by default. We advocate a different understanding of time, namely as a more contingent force, which defies generalised predictions of how it influences governance versatility.
Time also seems to be an important factor when understanding the institutional profiles underpinning specific levels of governance versatility. Our analysis stresses the interplay between different macro- and meso-political and administrative institutions is complex, not least also, because it involves a great deal of layering over time. For example, in Germany and the Netherlands, the layering of funding from social insurance and corporatist interest mediation develops over time to enable greater governance versatility and the introduction of market governance. In the other pairs, the macro-administrative institutions of public management interact with meso level institutions to reinforce high or low versatility. Future research needs to make a greater effort to better understanding the institutional origins of governance versatility by studying the specific ways in which different institutions evolve over time. Here, the literature on historical institutionalism offers a variety of relevant conceptual tools (Mahoney and Thelen, 2010).
Thirdly, our analysis brings to the fore questions about the sustainability of governance versatility (Koppenjan et al., 2019). Differences in governance versatility have significant consequences for the ability of governments to govern public services. For example, in Demark and Québec the sole use of soft hierarchy clearly limits the prospects of reaching performance management in primary care. However, higher governance versatility may not necessarily lead to more effective governance, contra the arguments made by advocates of hybrid governance. For example, the emergence of greater versatility encompassing hierarchy, market and network governance in Australia and New Zealand resembles a process of cycling from one mode of coordination to the next. As a result, it is difficult for individual modes to take root and it is indicative that in both countries, policy implementation often remains patchy. Taken together, this calls for future research to set focus on the material consequences of different varieties of governance versatility, for example by studying these consequences over a long period of time (Koppenjan et al., 2019, 148). This would offer a stepping-stone for formulating conditions for sustainable versatility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.